A. R. Ness
A. K. Wills
A. Waylen
R. Al-Ghatam
T. E. M. Jones
R. Preston
A. J. Ireland
M. Persson
J. Smallridge
A. J. Hall
D. Sell
J. R. Sandy
Centralization of cleft care in the
UK. Part 6: a tale of two studies
Authors' affiliations:
A. R. Ness, D. Sell, National Institute for Health Research (NIHR) Biomedical Research Unit in Nutrition, Diet and Life-style at the University Hospitals Bristol NHS Foundation Trust and the University of Bristol, Bristol, UK
A. R. Ness, A. K. Wills, A. Waylen, R. Al-Ghatam, T. E. M. Jones, A. J. Ireland, J. R. Sandy, School of Oral and Dental Sciences, University of Bristol, Bristol, UK T. E. M. Jones, Musgrove Park Hospital, Taunton, UK
R. Preston, Cleft Lip and Palate Associa-tion, London, UK
M. Persson, Centre for Appearance Research, University of the West of England, Bristol, UK
J. Smallridge, South Thames’ Cleft Unit, Guy’s and St Thomas Hospital, London, UK
J. Smallridge, Cleft Net East Cleft Network, Addenbrooke’s Hospital, Cambridge, UK
A. J. Hall, Children’s Hearing Centre, University Hospitals Bristol NHS Founda-tion Trust, Bristol, UK
Ness A. R., Wills A. K., Waylen A., Al-Ghatam R., Jones T. E. M., Preston R., Ireland A. J., Persson M., Smallridge J., Hall A. J., Sell D., Sandy J. R. Centralization of cleft care in the UK. Part 6: a tale of two studies.
Orthod Craniofac Res2015;18(Suppl. 2): 56–62.©2015 The Authors.
Orthodontics & Craniofacial ResearchPublished by John Wiley & Sons Ltd
Structured Abstract
Objectives –We summarize and critique the methodology and outcomes from a substantial study which has investigated the impact of reconfig-ured cleft care in the United Kingdom (UK) 15 years after the UK govern-ment started to implegovern-ment the centralization of cleft care in response to an earlier survey in 1998, the Clinical Standards Advisory Group (CSAG).
Setting and Sample Population – A UK multicentre cross-sectional study of 5-year-olds born with non-syndromic unilateral cleft lip and palate. Data were collected from children born in the UK with a unilateral cleft lip and palate between 1 April 2005 and 31 March 2007.
Materials and Methods – We discuss and contextualize the outcomes from speech recordings, hearing, photographs, models, oral health and psychosocial factors in the current study. We refer to the earlier survey and other relevant studies.
Results –We present arguments for centralization of cleft care in health-care systems, and we evidence this with improvements seen over a per-iod of 15 years in the UK. We also make recommendations on how future audit and research may configure.
Conclusions –Outcomes for children with a unilateral cleft lip and palate have improved after the introduction of a centralized multidisciplinary Date:
Accepted 5 September 2015
DOI: 10.1111/ocr.12111
©2015 The Authors.
A. J. Hall, Centre for Child and Adolescent Health, School of Social and Community Medicine, University of Bristol, Bristol, UK
D. Sell, Speech and Language Therapy Department and Centre for Outcomes and Experience Research in Children’s Health, Illness and Disability (ORCHID), Great Ormond Street Hospital NHS Foun-dation Trust, London, UK
Correspondence to: Professor J. R. Sandy
School of Oral and Dental Sciences University of Bristol
Lower Maudlin Street Bristol, BS1 2LY, UK
E-mail: [email protected]
service, and other countries may benefit from this model. Predictors of early outcomes are still needed, and repeated cross-sectional studies, larger longitudinal studies and adequately powered trials are required to create a research-led evidence-based (centralized) service.
Key words: Cleft Lip; Cleft Palate; Cross-Sectional Studies
Introduction
In this supplement, we report on the results of a UK-wide cross-sectional survey of 5-year-old children with unilateral cleft lip and palate con-ducted between January 2011 and December 2012 – Cleft Care UK (CCUK) (1–5). We attempted as far as possible to follow the design of a previous survey conducted fifteen years ago that recruited from a similar target population of children with unilateral cleft lip and palate– the Clinical Standards Advisory Group (CSAG) study (6–11). Much has changed since this first survey was conducted. The 57 centres providing care for children with cleft lip and palate have reduced to 11 centres or managed clinical net-works. Care in these centres is provided by mul-tidisciplinary teams, and the surgeons in these teams operate on at least 35 cases each year (12–14). Preliminary studies suggest that out-comes have improved but these reports either were regional (rather than national), were speci-fic to a single outcome or had incomplete data (15–17). We report here the results of a compre-hensive nationwide survey and directly compare these results with those prior to centralization.
A tale of two studies
We were not able to replicate the previous sur-vey exactly. We used the same inclusion criteria
and measured the same attributes in the study children. But the children we studied fifteen years later were younger (despite using the same target age range), and some of the approaches to mea-surement have changed. Orthodontists now sometimes use photographs in place of study models, speech and language therapists assess speech using a modified protocol, and psycholo-gists have changed the questions they ask. The similarities and differences between the two stud-ies are summarized in Table 1 and described in detail in the first paper in this supplement (1). Despite these differences, we believe that these studies are similar enough to allow us to describe changes in care and outcome over this time frame and thus to evaluate the impact of the move to a centralized multidisciplinary service.
Summary of findings
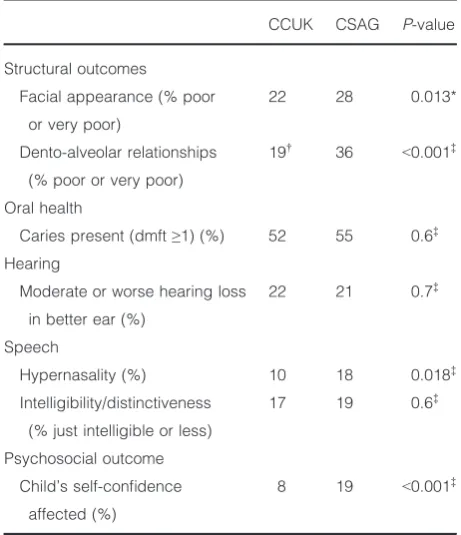
supple-ment (2–5). Though much improved, compara-tive data from other centres on dento-alveolar arch relationships and speech outcomes suggest these are still not as good as those achieved in the best centres in Europe (18–20). Further, there are still a proportion of children who do badly with up to 20% having poor results for important outcomes such as dento-alveolar arch relationships and intelligibility/distinc-tiveness of speech. The numbers with poor outcomes are summarized in Table 3 and described in more detail in the results papers in this supplement (2–5).
Other benefits of this programme of
cleft research
This second cross-sectional survey was part of a larger programme of work funded by the UK
[image:3.595.64.542.79.434.2]National Institute for Health Research (NIHR). We ran a series of research workshops to design the study that also triggered a James Lind Alli-ance initiative (21) and a health talk project (22) in children with cleft lip and palate. We com-pleted several systematic reviews on treatment for children with cleft lip and palate (23–25). We conducted a survey of cleft centres that has described the service provision (12, 13) and the process of centralization (26). We have been able to offer training opportunities. Three students have already completed taught doctorates using data collected as part of this cross-sectional sur-vey and the sursur-vey of the centres. We have strengthened patient and public involvement among people with cleft by disseminating our work through the Cleft Lip and Palate Associa-tion and by running a workshop focussing on patient involvement. Our study (and pro-gramme) has thus paved the way for future Table 1. Comparison of methods and demographics between the Cleft Care UK (CCUK) study and the Clinical Standards Advisory Group (CSAG) study
CCUK 2012 CSAG 1998
Methods
Type of activity Research Audit
People collecting key outcomes Mainly local teams Study team
Measures
Appearance Better quality digital images Photographs
Dento-alveolar arch relationships Study models and photographs Study models
Oral health British Association for the Study of Community
Dentistry (BASCD) calibrated dental
examination by consultant paediatric dentist
BASCD calibrated dental
examination by an orthodontist
Hearing Pure tone audiometry, tympanometry and
otology assessment
Pure tone audiometry and otology
assessment
Speech assessment Cleft Audit Protocol for Speech–Augmented
(CAPS-A)
Cleft Audit Protocol for Speech
(CAPS)
Psychology assessment Modified psychosocial questionnaire, 8 items;
self-confidence response was 0–10 (0=very
negative effect; 5=no difference; 10=very
positive effect)
Psychosocial questionnaire, 18
items; self-confidence response
was yes/no
Demographics
Year of birth 2005–2007 1989–1991
Eligible 359 326
Number recruited and response rate 268 (75%) 239 (73%)
Age (median and interquartile range) 5.5 (5.4–5.7) 6.4 (5.9–6.9)
randomized trials and observation studies by reviewing the evidence and building research capacity in cleft centres in the UK.
Implications for practice
Our data show that a centralized multidisci-plinary service improves outcomes albeit that some areas of cleft care still require improve-ment. This study will provide evidence for cleft teams to argue with commissioners for increased resource. In our view, centralized multidisci-plinary services should be introduced in all countries. Local comprehensive surveys are not required to justify or guide this change. Earlier UK outcomes described in the original CSAG study were poor, and it was argued that this was because there was no centralized service. This does not prove at all that small centres with a low case load but very well-organized care are
[image:4.595.303.534.93.361.2]likely to have poor outcomes. The issue is that these small centres will have great difficulty in proving the quality of their outcomes because of a lack of statistical power. These arguments have been well rehearsed elsewhere with strong evi-dence to counter the continuation of low volume operating (10). However, it is not clear what the key component (or components) of centraliza-tion is. Is it the improvements in surgical train-ing? Is it the increase in number of operations? Is it the implementation of multidisciplinary team working? Is it the creation of an audit cul-ture that encourages reflective practice? Further analyses of the data in these two cross-sectional studies and future studies may refine our under-standing, but this should not delay plans to rationalize services. It is also unclear how we should monitor outcome post-centralization. It would be useful to have process measures that predict outcome at age five, or earlier outcome measures that can be used before the age of Table 2. Comparison of good outcomes between the Cleft
Care UK (CCUK) study and the Clinical Standards Advisory Group (CSAG) study
CCUK CSAG P-value
Structural outcomes
Facial appearance (% good
or excellent)
36 32 0.107*
Dento-alveolar relationships
(% good or excellent)
53† 30 <0.001‡
Oral health
Caries-free (dmft=0) (%) 48 45 0.6‡
Hearing
None or mild hearing loss in
better ear (%)
78 79 0.7‡
Speech
No hypernasality (%) 90 82 0.018‡
Intelligibility/distinctiveness
(% normal)
56 20 <0.001‡
Psychosocial outcome
Child’s self-confidence
not affected (%)
92 81 <0.001‡
*Mixed effects logistic regression to account for the non-inde-pendence of observations from multiple observers.
†This is based on the 198 children with models as the 49
[image:4.595.53.283.93.364.2]chil-dren with photographs were excluded. ‡Chi-squared test.
Table 3. Comparison of poor outcomes between the Cleft Care UK (CCUK) study and the Clinical Standards Advisory Group (CSAG) study
CCUK CSAG P-value
Structural outcomes
Facial appearance (% poor
or very poor)
22 28 0.013*
Dento-alveolar relationships
(% poor or very poor)
19† 36 <0.001‡
Oral health
Caries present (dmft≥1) (%) 52 55 0.6‡
Hearing
Moderate or worse hearing loss
in better ear (%)
22 21 0.7‡
Speech
Hypernasality (%) 10 18 0.018‡
Intelligibility/distinctiveness
(% just intelligible or less)
17 19 0.6‡
Psychosocial outcome
Child’s self-confidence
affected (%)
8 19 <0.001‡
*Mixed effects logistic regression to account for the non-inde-pendence of observations from multiple observers.
†This is based on the 198 children with models as the 49
5 years or both. In the UK, we rely on data col-lected at audit clinics when the child is 5 years old. These data therefore reflect outcome some-time after the primary surgery, and the numbers treated in any one centre are small. Obtaining standardized measures from all centres routinely is challenging and expensive (17). In our view, the best approach is to encourage audit clinics locally (where these do not already happen) that provide training and encourage review of per-sonal practice – this will certainly be able to detect extreme variations in outcome – and to carry out intermittent comprehensive surveys nationally that describe care and outcomes. It is essential to continue to participate in interna-tional comparative studies and to be mindful of the better European centres where care is still being delivered at higher standards with better outcomes.
Implications for research
We plan to conduct further analyses of these data to look at the impact of centre characteris-tics such as size, time to centralization, surgical throughput and multidisciplinary working on outcome. We also intend to look at predictors of specific outcomes in an attempt to quantify the role of individual and treatment factors that pre-dict both good and poor outcomes. We will also describe the costs incurred by families and peo-ple’s choice preferences. This cross-sectional study is a resource, and we are trying to encour-age future collaborations to ensure it is fully exploited. We are currently creating a detailed data dictionary and formalizing access arrange-ments. A further national cross-sectional survey should be considered in 5–10 years to confirm that there have been further improvements in service provision and outcome such that cleft care in the UK is the best in Europe. Longitudi-nal studies to describe trajectories of children with cleft and to identify early outcome mea-sures or predictors of outcome would be valu-able. Well-designed adequately powered trials informed by the priorities identified through the recent James Lind Alliance initiative should be
conducted (21). There is also now an opportu-nity for the cleft teams in the UK to participate in larger international studies of outcomes and to participate in clinical trials. These collabora-tions are key with a low incidence anomaly as all aspects of aetiology and care will benefit from increasing sample sizes. The diversity of genetic and environmental factors in the causation of clefting will only be explored through multicen-tre collaborations and international epidemio-logical approaches.
The challenges of clinical research in
cleft
conduct multicentre clinical research but that there is room for improvement. Future research projects need to consider strategies to reach and study socially disadvantaged groups who are less likely to come to clinics and complete question-naires (28). The challenge is to build research understanding, expertise and capacity in teams. If this challenge is met, there is an opportunity to strengthen the evidence base to inform treat-ment decisions for children with cleft lip and palate (29).
Conclusions
Outcomes for children with a unilateral cleft lip and palate have improved after the introduction of a centralized multidisciplinary service. This process of centralization should be introduced in other countries with a less centralized service for children with clefts. Further analyses will be
conducted to explore centre-level effects and individual and treatment factors that influence outcome. There is a need for earlier outcome measures or predictors of outcome that could be used to audit practice and monitor service qual-ity in a more timely fashion. Repeated cross-sec-tional studies, larger longitudinal studies and adequately powered trials are required to create the research-led evidence-based (centralized) service that children born with cleft lip and palate deserve.
Acknowledgements: We would like to thank the fami-lies that took part in this study. We would also like to thank the clinicians and staff in the cleft centres who supported this project. This publication presents inde-pendent research commissioned by the National Insti-tute for Health Research (NIHR) under its Programme Grants for Applied Research scheme (RP-PG-0707-10034). The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
References
1. Persson M, Sandy JR, Waylen A, Wills AK, Al-Ghatam R, Hall A et al. A cross-sectional survey of five-year old children with non-syndromic unilat-eral cleft lip and palate: cleft Care UK. Orthod Craniofac Res2015;18(S2): 1–13.
2. Al-Ghatam R, Jones TEM, Ireland AJ, Atack NE, Chawla O, Deacon S et al. Structural outcomes in the cleft care UK study–dentofacial outcomes. Orthod Craniofac Res2015;18 (S2):14–24.
3. Smallridge J, Hall AJ, Chorbaki R, Parfect V, Persson M, Ireland A et al. Functional outcomes in the Cleft Care UK study: oral health and audi-ology.Orthod Craniofac Res2015;18 (S2):25–35.
4. Sell DA, Mildinhall S, Albery L, Wills AK, Sandy JR, Ness AR. Perceptual speech outcomes in the Cleft Care UK study.Orthod Craniofac Res 2015;18(S2):36–46.
5. Waylen A, Ness AR, Wills AK, Pers-son M, Rumsey N, Sandy JR. Child psychosocial outcomes and satisfac-tion with cleft services in the Cleft Care UK study.Orthod Craniofac Res 2015;18(S2):47–55.
6. Clinical Standards Advisory Group. Cleft Lip and/or Palate, HSMO, ISBN 0-11-322103-7 London, 1998. 7. Sandy JR, Williams AC, Bearn D,
Mildinhall S, Murphy T, Sell D et al. Cleft lip and palate care in the Uni-ted Kingdom–the Clinical Standards Advisory Group (CSAG) Study. Part 1: background and methodology. Cleft Palate Craniofac J2001;38:20–3. 8. Williams AC, Bearn D, Mildinhall S,
Murphy T, Sell D, Shaw WC et al. Cleft lip and palate care in the Uni-ted Kingdom–the Clinical Standards Advisory Group (CSAG) Study. Part 2: dentofacial outcomes and patient satisfaction.Cleft Palate Craniofac J 2001;38:24–9.
9. Sell D, Grunwell P, Mildinhall S, Murphy T, Cornish TA, Bearn D et al. Cleft lip and palate care in the United Kingdom-the Clinical Stan-dards Advisory Group (CSAG) Study. Part 3: speech outcomes.Cleft Palate Craniofac J2001;38:30–7.
10. Bearn D, Mildinhall S, Murphy T, Murray JJ, Sell D, Shaw WC et al. Cleft lip and palate care in the Uni-ted Kingdom–the Clinical Standards Advisory Group (CSAG) Study. Part 4: outcome comparisons, training,
and conclusions.Cleft Palate Cran-iofac J2001;38:38–43.
11. Williams AC, Sandy JR, Thomas S, Sell D, Sterne JA. Influence of surgeon’s experience on speech out-come in cleft lip and palate.Lancet 1999;354:1697–8.
12. Scott JK, Leary SD, Ness A, Sandy J, Persson M, Kilpatrick N et al. Cen-tralisation of services for children born with orofacial clefts in the Uni-ted Kingdom: a cross sectional sur-vey.Cleft Palate Craniofac J2014;51: e102–9.
13. Scott JK, Leary SD, Ness AR, Sandy JR, Persson M, Kilpatrick N et al. Perceptions of team members work-ing in cleft services in the United Kingdom: a pilot study.Cleft Palate Craniofac J2015;52:e1–7.
14. Fitzsimons KJ, Mukarram S, Copley LP, Deacon SA, van der Meulen JH. Centralisation of services for children with cleft lip or palate in England: a study of hospital episode statistics. BMC Health Serv Res2012;12:148. 15. Hathorn IS, Atack NE, Butcher G,
16. Revington PJ, McNamara C, Mukar-ram S, Perera E, Shah HV, Deacon SA. Alveolar bone grafting: results of a national outcome study.Ann R Coll Surg Engl2010;92:643–6. 17. Fitzsimons K, Deacon S, Copley L,
van der Meulen J.CRANE Database: Annual Report on cleft lip and/or palate 2013. www.crane-database.or-g.uk.
18. Sinko K, Caacbay E, Jagsch R, Tur-hani D, Baumann A, Mars M. The GOSLON yardstick in patients with unilateral cleft lip and palate: review of a Vienna sample.Cleft Palate Craniofac J2008;45:87–92.
19. Lilja J, Mars M, Elander A, Enocson L, Hagberg C, Worrell E et al. Analy-sis of dental arch relationships in Swedish unilateral cleft lip and palate subjects: 20-year longitudinal consecutive series treated with delayed hard palate closure.Cleft Palate Craniofac J2006;43:606–11. 20. Lohmander A. Surgical intervention
and speech outcomes in cleft lip and palate. In: Howard S, Lohman-der A, editors.Cleft Palate Speech. Chichester: John Wiley & sons; 2011. pp. 55–85.
21. Petit-Zeman S, Cowan K. Patients/ carers and clinicians can set joint priorities for research in cleft lip and palate.Int J Paediatr Otorhinolaryn-gol2013;77:309–10.
22. Healthtalk.org. Cleft lip and palate. [Online] Available from: http:// www.healthtalk.org/peoples-experi- ences/pregnancy-children/cleft-lip-and-palate/topics [Accessed Febru-ary 2015].
23. Bessell A, Sell D, Whiting P, Roul-stone S, Albery L, Persson M et al. Speech and language therapy interventions for children with cleft palate: a systematic review. Cleft Palate Craniofac J2013;50: e1–17.
24. Norman A, Persson M, Stock N, Rumsey N, Sandy J, Waylen A et al. The effectiveness of psy-chosocial intervention for individu-als with cleft lip and/or palate and their parents: a systematic review. Cleft Palate Craniofac J2015;52: 301–10.
25. Pepper H, Perry R, Ness A, Sandy J, Thomas S. A Systematic review of skin closure techniques in primary
cleft lip surgery.Oral Surgery 2015;8:10–7.
26. Searle A, Scott J, Sandy J, Ness AR, Waylen A. Clinical directors’ views of centralisation and commissioning of cleft services in the UK.BMC Oral Health2015;22:12.
27. Sandy J, Kilpatrick N, Persson M, Bessel A, Waylen A, Ness A et al. Why are multi-centre clinical obser-vational studies still so difficult to run?Br Dent J2011;211:59–61. 28. Bonevski B, Randell M, Paul C,
Chapman K, Twyman L, Bryant J et al. Reaching the hard-to-reach: a systematic review of strategies for improving health and medical research with socially disadvantaged groups.BMC Med Res Methodol 2014;14:42.