CHRONIC ESCALATING HEROIN WITHDRAWAL LEADS TO FUTURE ENHANCED FEAR LEARNING
Shveta V. Parekh
A thesis submitted to the faculty at the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Master of Psychology and Neuroscience in the
Behavioral Neuroscience program in the College of Arts and Sciences.
Chapel Hill 2020
Approved by:
Donald T. Lysle
Regina M. Carelli
ii
iii
ABSTRACT
Shveta V. Parekh: Chronic escalating heroin withdrawal leads to future enhanced fear learning (Under the direction of Donald T. Lysle)
Converging evidence suggests opioid abuse can increase the incidence and severity of
post-traumatic stress disorder (PTSD) in clinical populations. Interestingly, opioid withdrawal
alone can produce symptoms similar to those of PTSD. Despite this association, the neural
mechanisms underlying the relationship of opioid abuse, withdrawal, and PTSD is poorly
understood. The present experiments investigate whether the heroin withdrawal may induce a
PTSD-like phenotype. Therefore, we developed an animal model of heroin withdrawal which
consists of a chronic escalating heroin administration paradigm. This paradigm reliably produces
withdrawal behaviors in rodents. We tested the effect of chronic escalating heroin administration
and withdrawal regimen on fear learning, and found it acts as a severe stressor to produce
enhanced fear learning. These data provide further evidence that heroin withdrawal is sufficient
to produce enhanced fear learning, and suggests a common underlying mechanism between
iv
To my parents:
v
ACKNOWLEDGEMENTS
Many thanks to the Lysle Laboratory, Christina L. Lebonville, Jacqueline E. Paniccia,
Gillian A. Barkell and to my advisor, Donald T. Lysle, whose guidance, support, and editing
vi
TABLE OF CONTENTS
LIST OF FIGURES...vii
LIST OF ABBREVIATIONS...viii
CHAPTER 1: CHRONIC ESCALATING HEROIN WITHDRAWAL LEADS TO FUTURE ENHANCED FEAR LEARNING...1
Introduction...1
Materials and Methods...4
Animals...4
Experiment 1: Effect of Chronic Escalating Heroin Administration on Withdrawal Behaviors...4
Experiment 2: Effect of Heroin Withdrawal on Fear Learning...6
Statistical Analysis...7
Results...7
Experiment 1: Chronic Escalating Heroin Administration Produces a Reliable Withdrawal ……...7
Experiment 2: Heroin Withdrawal Produces Enhanced Fear Learning...9
Discussion...10
Funding and Disclosure……...13
vii
LIST OF FIGURES
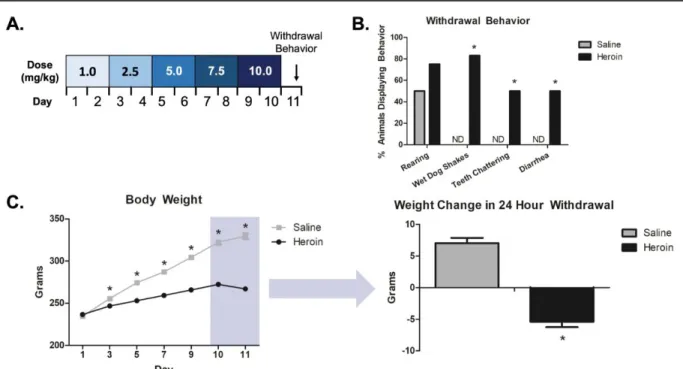
Figure 1 – Chronic escalating heroin administration produces withdrawal...8
Figure 2 – Chronic escalating heroin administration produces a similar range of withdrawal.…..9
viii
LIST OF ABBREVIATIONS
DH dorsal hippocampal
HPA axis hypothalamic pituitary adrenal axis
HW-EFL heroin withdrawal-enhanced fear learning
IL-1RA IL-1 receptor antagonism
IL-1β interleukin-1β
mRNA messenger RNA
NIDA National Institute on Drug Abuse
NIMH National Institute of Mental Health
OUD opioid use disorder
PTSD post-traumatic stress disorder
SC subcutaneously
1
CHAPTER 1: CHRONIC ESCALATING HEROIN WITHDRAWAL LEADS TO FUTURE ENHANCED FEAR LEARNING
INTRODUCTION
One of the most severe psychological disorders induced by stress is post-traumatic stress
disorder (PTSD), a chronic and debilitating disorder characterized by exaggerated fear and anxiety
that results from a traumatic experience. PTSD includes a myriad of psychological and
physiological consequences, some of which include re-experiencing the fear through flashbacks
or nightmares, avoiding the fear by staying away from places, events, or objects that are reminders
of the traumatic experience, arousal and reactivity symptoms such as being easily startled or
feeling tense or stressed and cognition and mood symptoms such as negative thoughts and distorted
feelings (Rubin, Berntsen et al. 2008, Gill, Saligan et al. 2009, Xia, Zhai et al. 2013, Reardon,
Chappelle et al. 2016). Importantly, PTSD affects 7.7 million Americans (NIMH), with the major
at-risk population being active military personnel, first responders, emergency responders, and
abused individuals (Bowler, Han et al. 2010, Thomas, Wilk et al. 2010). While up to 17% of
combat veterans are diagnosed with PTSD (Richardson, Frueh et al. 2010), well over 30% of
veterans meet the criteria for a possible PTSD diagnosis.
To further exacerbate the consequences of PTSD, multiple lines of evidence indicates
significant comorbidity between PTSD and opioid use disorders (OUD). For example, heroin use
disorder is associated with increased anxiety diagnoses (McHugh, Votaw et al. 2017) and can
increase severity of PTSD symptoms in clinical populations (Jacobsen, Southwick et al. 2001,
2
Heroin misuse leads to adverse consequences that persist long after cessation of drug use. The
stress of withdrawal has been implicated in drug relapse (Koob and Volkow 2010), but may also
increase vulnerability to other disorders such PTSD. Moreover, there is often a shared
symptomology between opioid withdrawal and PTSD (Patel, Elmaadawi et al. 2017). While it is
generally thought that PTSD precedes, and therefore is a risk factor, for substance use disorders,
there is also evidence that a prior history of substance use exacerbates the development and
symptoms of PTSD (Saladin, Brady et al. 1995, Bremner, Southwick et al. 1996, Jacobsen,
Southwick et al. 2001, Holmes, Fitzgerald et al. 2012, McCauley, Killeen et al. 2012, Meier,
Lambert-Harris et al. 2014, Patel, Elmaadawi et al. 2017). Consistent with this view, this
suggests that the adverse symptoms that arise from substance use disorders, such as anxiety,
depression, and poor coping skills, leave individuals biologically more vulnerable to the impact
of severe stress and are thus more likely to develop PTSD (Jacobsen, Southwick et al. 2001,
McCauley, Killeen et al. 2012).
There are several animal models of PTSD (Yamamoto, Morinobu et al. 2009, Kaouane,
Porte et al. 2012), and stress enhanced fear learning (SEFL) (Rau, DeCola et al. 2005), is an
excellent model that effectively demonstrates hyperreactivity to future fear learning. In this model,
animals are exposed to 15 foot shocks, characterized as severe foot shock stress, in one context
(Context A). One-week later animals are exposed to a single, more mild foot shock in a distinctly
different context, (Context B). Severe stress in Context A significantly enhances fear learning to
Context B. It is believed that neuroplastic changes occur following severe stress that lead to
long-term alterations of fear learning and changes how the animal processes subsequent fear challenges.
This model is pronounced, robust, and reliable (Szczytkowski-Thomson, Lebonville et al. 2013,
3
human PTSD. Although several animal models to study PTSD have been developed, the animal
models needed to study heroin withdrawal are lacking.
Few models of heroin withdrawal such as self-administration (Towers, Tunstall et al.
2019, Gipson, Dunn et al. 2020) and precipitated withdrawal (Liu, Coller et al. 2011, Fatahi,
Zeinaddini-Meymand et al. 2020) have been developed, however these models do not capture the
clinical implications of heroin use disorder and withdrawal. The self-administration model,
where a rodent is trained to press a lever to obtain self-administered intravenous injections of
drug, has many advantages (Kmiotek, Baimel et al. 2012); however, the focus of our work is to
examine the effects of heroin withdrawal, not the motivational aspects of heroin which requires
self-administration. Furthermore, this model involves the animal receiving small doses of drug
over a span of time. In order to reach a dependence level enough to produce a spontaneous
opioid withdrawal, rodents must undergo ‘long-access’ self-administration cycles, often for 6 –
24 hours (Shaham, Rajabi et al. 1996, Edwards, Graham et al. 2009). These small doses of opioid
administration are not indicative of a clinical heroin addiction. On the other hand, a precipitated
withdrawal involves the administration of an opioid antagonist, such as naloxone, which results
in an immediate withdrawal. Our work is aimed at studying a spontaneous withdrawal to better
understand the clinical consequences of opioid use disorder. In humans, heroin addiction is
characterized by multiple phases of chronic drug use, spontaneous withdrawal, and relapse to
drug-seeking behavior (Seip, Reed et al. 2012). Although the drug-seeking behavior of heroin is
well characterized through the use of self-administration (De Vries, Schoffelmeer et al. 1998,
Highfield, Yap et al. 2001, Leri and Stewart 2001, Kuntz, Patel et al. 2008, Zhou and Kalivas
2008), little is known about heroin withdrawal. Neither the self-administration model nor the
4
spontaneous withdrawal. Therefore, one of the goals of the present study was to test whether a
chronic, escalating heroin administration and spontaneous withdrawal paradigm would produce a
reliable heroin withdrawal animal model.
Given that heroin withdrawal can produce similar physiological responses as those
induced by stress, the second goal of the present study was to test whether heroin withdrawal
may enhance fear learning in the same way as a severe stressor. The current studies test the
overarching hypothesis that heroin withdrawal substitutes for a severe stressor in the SEFL
model to produce enhanced fear learning. To this end, Experiment 1 tested whether a chronic,
escalating heroin administration and spontaneous withdrawal would produce withdrawal
behaviors, and in turn a novel animal model of heroin withdrawal. Subsequently, Experiment 2
determined whether heroin withdrawal can produce enhanced fear learning. Collectively, these
experiments are the first to test whether chronic escalating heroin administration and
spontaneous withdrawal can sensitize future fear learning.
MATERIALS AND METHODS
Animals
Adult male Sprague Dawley rats (225-250g, Charles River Laboratories, Raleigh, NC)
were individually housed under a reversed 12-hour light-dark cycle, given ad libitum access to
food and water, and handled regularly throughout experimentation. All procedures were
conducted in accordance with federal guidelines and with approval from the University of North
Carolina at Chapel Hill Institutional Animal Care and Use Committee.
Experiment 1: Effect of Chronic Escalating Heroin Administration on Withdrawal Behaviors
5
[diacetylmorphine hydrochloride, National Institute on Drug Abuse (NIDA) Drug Supply
Program, Bethesda, MD, USA] was dissolved in sterile 0.9% saline to final concentrations of
1.0, 2.5, 5.0, 7.5, and 10.0 mg/mL, and stored at 4°C until time of injection. Injections were
administered subcutaneously (SC). The administration schedule of chronic escalating heroin
(adapted from (Zhou, Bendor et al. 2006, Seip, Reed et al. 2012, Zhou, Leri et al. 2013))
consisted of 10-days of three injections over 24-hour periods (at 15:00, 21:00, and 9:00 the next
day, UTC-05:00) and a dose increase every other day: 3.0 (3 x 1.0) mg/kg/day on days 1-2, 7.5
(3 x 2.5) mg/kg/day on days 3-4, 15.0 (3 x 5.0) mg/kg/day on days 5-6, 22.5 (3 x 7.5) mg/kg/day
on days 7-8, and 30 (3 x 10) mg/kg/day on days 9-10 (Figure 1a). Animal weight change, a quantifiable and reliable measure of opioid withdrawal (Gellert and Holtzman 1978), was
measured at every dose increase and subsequent withdrawal time point.
Procedure Rodent withdrawal behaviors were quantified following the chronic
escalating heroin administration. Animals were randomly assigned to receive heroin (n=12) or
saline (n=8) throughout the procedure. Twenty-four hours into withdrawal, animals were placed
into open-field Plexiglas boxes (42cm x 42cm x 30cm). Withdrawal behaviors (rearing, wet dog
shakes, teeth chattering, and diarrhea) were video-recorded for 30 min. Experimenters were
trained on withdrawal behaviors, until there was 98% agreement in observation scores.
Experimenters scored behaviors blind to treatment condition. Positive withdrawal behavior was
recorded if the behavior occurred at least once in the 30 min observation period. A heroin
withdrawal score was calculated for each behavior based on the number of behaviors observed
during the 30 min observation period, and these individual behavior scores were summed to
6
Experiment 2: Effect of Heroin Withdrawal on Fear Learning
Heroin Withdrawal-Enhanced Fear Learning (HW-EFL): We used a modified version of the SEFL model previously described (Rau, DeCola et al. 2005,
Szczytkowski-Thomson, Lebonville et al. 2013, Jones, Lebonville et al. 2015, Jones, Lebonville et al. 2017).
Rather than a severe foot shock, animals underwent heroin withdrawal in their home cage.
Control animals received saline administration and were kept in the home cage. Seven days after
the start of withdrawal, animals were placed into a novel context for 15 min and video recorded
for baseline activity (Test Day B). The novel context (Med Associates, St. Albans, VT) was
housed in a separate room and had a distinct textile, olfactory, and auditory characteristics, as
previously described (Szczytkowski-Thomson, Lebonville et al. 2013). On Day 8, animals were
placed into the same context for a single scrambled foot shock (1mA, 1s) at 3 min, 12 s. On days
9, 10, 15, 22 (Test Days 1, 2, 7, and 14) animals are placed into the same context for 8 min, 32 s
and were video recorded to measure freezing behavior, a measure of learned fear. Automated
video tracking and analysis software was used to quantify percent freezing behavior in all
sessions (Ethovision XT, Activity Analysis Feature with Threshold=10, Noldus Information
Technology Inc., Netherlands).
Procedure: The effect of heroin withdrawal was examined on enhanced fear learning. Animals were randomly assigned to receive heroin (n=15), or saline (n=16) and underwent the
chronic escalating heroin administration and subsequently exposed to heroin
withdrawal-enhanced fear learning.
Statistical Analysis
For Experiment 1, withdrawal behaviors were analyzed using a χ2 test. Body weight on
7
(Drug Treatment) x 6 (Day) repeated measures ANOVA. Weight change and composite
withdrawal scores were analyzed using an unpaired, two-tailed Student’s t-test. For Experiment
2, a one-way (Heroin, Saline) ANOVA was used to analyze baseline freezing data. A 2 (Heroin,
Saline) x 4 (Test Day) repeated measures ANOVA was used to analyze freezing behavior across
test days.
RESULTS
Experiment 1: Chronic Escalating Heroin Administration Produces a Reliable Withdrawal
Thechronic escalating heroin administration (Figure 1A) produced withdrawal behaviors 24 hours after the last heroin dose. χ2 analysis revealed no difference between the heroin
withdrawal and saline controls for rearing behavior (χ2(1,n=20)=1.319, p=.251). Importantly, χ2
analysis revealed significant increases in withdrawal behaviors between the heroin withdrawal
and saline controls for wet dog shakes (χ2(1,n=20)=13.333, p<.001), teeth chattering
(χ2(1,n=20)=5.714, p=.017), and diarrhea (χ2(1,n=20)=5.714, p=.017) (Figure 1b). A one-way
ANOVA revealed no significant differences between heroin and saline animal weights on Day 1,
(F(1,29)=.645, p=.428), indicating no pre-existing weight differences between groups. Importantly,
a repeated measures ANOVA revealed a significant main effect of drug-treatment on weight
between days 3-10, (F(1,29)=127.937, p<.001), indicating that heroin-treated animals have
decreased weight compared to saline-treated controls. There was also a significant main effect
across days (F(5,145)=705.236, p<.001) and significant day by drug treatment interaction
8
10 and Day 11 (first 24 hours of withdrawal) revealed that heroin-treated animals lost
significantly more weight than saline-treated animals (t(29)=10.666, p<.001) (Figure 1c).
Student’s t-test comparing composite withdrawal scores between heroin-treated animals
and saline-treated animals revealed that heroin-treated animals had a significantly higher
composite withdrawal score than saline-treated animals (t(18)=-9.754, p<.001) (Figure 2b). Furthermore, the range of heroin withdrawal scores was between 6 and 14, with no outliers,
suggesting that all animals experienced a relatively similar range of withdrawal after the chronic
escalating heroin administration.
9
Experiment 2: Heroin Withdrawal Produces Enhanced Fear Learning
Heroin withdrawal substituted for the severe stressor in the SEFL model, and produced
subsequent enhanced fear learning. There was no effect of drug treatment on baseline freezing to
the context, (F(1,16)=1.209, p=.288). Importantly, a 2 x 4 repeated measures ANOVA revealed a
significant main effect of drug treatment, (F(1,16)=7.389, p=.015), indicating the exciting finding
that a history of heroin withdrawal enhances fear learning to a single shock experience. There
was also a significant main effect of day, (F(3,48)=14.222, p<.001), indicating that indicating that
conditioned freezing behavior diminished over time. (Figure 2).
Figure 2. Chronic escalating heroin administration produces a similar range of withdrawal
10
DISCUSSION
The current studies demonstrate for the first time that exposure to chronic escalating
heroin administration produces heroin withdrawal in a rat. Previously our laboratory and others
have established that the severe stress of inescapable foot shock causes the development of
enhanced fear learning (Rau, DeCola et al. 2005, Szczytkowski-Thomson, Lebonville et al.
2013). Here, we show that the chronic heroin administration and spontaneous withdrawal is
capable of producing a PTSD-like phenotype in a rodent model. These studies suggest that
severe foot shock stress and heroin withdrawal may act similarly to alter enhanced fear learning.
Collectively, these findings provide new evidence that heroin withdrawal, similar to a severe
stressor, can lead to the development of future enhanced fear learning.
11
In the present study, exposure to chronic escalating heroin administration produces a
reliable withdrawal in rats. The focus of the present work was to examine the effects of heroin
withdrawal, not the motivational aspects of heroin, and therefore we chose to develop an
experimenter-administration of heroin versus a self-administration of heroin. The chronic,
escalating doses of experimenter-administered heroin reliably result in the development of
spontaneous withdrawal upon cessation of drug administration (Zhou, Leri et al. 2013), which is
not reliably achieved with self-administration. Importantly, the chronic, escalating dosing
regimen and spontaneous withdrawal is in fact reflective of the human condition of heroin
misuse (Seip, Reed et al. 2012, Zhou, Leri et al. 2013). This model mimics the multiple and
escalating doses that are taken by heroin-dependent individuals to prevent symptoms of
withdrawal (Kreek, L et al. 2002). Furthermore, Kreek and colleagues have also shown that the
spontaneous withdrawal produced by a similar model induces the expression of genes in the
brain that are associated with stress responses (Zhou, Leri et al. 2013). We believe that this
approach, while not encapsulating drug motivation per se, offers a strength over
self-administration, with greater face, construct and predictive validity as a means to examine the
neural consequences of heroin withdrawal on stress-enhanced fear learning.
Opioid withdrawal is often associated with increased stress-sensitivity, and therefore
managing stress and anxiety becomes a major focus of treatment in clinical populations
(Carcoba, Contreras et al. 2011). There have been various studies that have shown a connection
between morphine withdrawal and increased anxiety in both humans and animals (Bhattacharya,
Chakrabarti et al. 1995, Schulteis and Koob 1996, Koob and Le Moal 1997, Koob 2008). This
suggests that withdrawal states can lead to a stress response and that opioid withdrawal may
12
morphine withdrawal results in the activation of the HPA axis, specifically,
corticotropin-releasing hormone mRNA is increased following a precipitated morphine withdrawal (McNally
and Akil 2002, Houshyar, Gomez et al. 2003, Nunez, Foldes et al. 2007). This long-lasting
activation within the HPA axis and stress response leads us to believe that an individual may be
more susceptible to develop anxiety-like disorders such as PTSD.
Here, we demonstrate that exposure to heroin withdrawal is shown to produce a
PTSD-like phenotype in a rodent model. PTSD, alone, is a severe psychological disorder, and to further
exacerbate the consequences of PTSD, multiple lines of evidence indicate that opiate misuse
leads to increased incidence and severity of PTSD. Consistently, opiate use disorder has emerged
as a significant issue in clinical populations with PTSD due to prolonged pain treatments with
opiates following active duty (Bennett, Elliott et al. 2017, Finley, Schneegans et al. 2018). The
current findings provide strong and novel evidence that heroin use and withdrawal can lead to an
exacerbated PTSD-like phenotype.
Our studies suggests that severe foot shock stress and heroin withdrawal may act through
similar mechanisms to produce altered enhanced fear learning, however, the mechanism through
which heroin withdrawal induces alterations in future fear learning is not known. We have
previously shown that the severe stressor in SEFL induces a time-dependent, region-specific
increase in dorsal hippocampal (DH) interleukin-1β (IL-1β), a cytokine responsible for learning
and memory, and subsequent fear learning is blocked by DH IL-1 receptor antagonism (IL-1RA)
(Jones, Lebonville et al. 2015, Jones, Lebonville et al. 2017, Jones, Paniccia et al. 2018). This
suggests that stress-induced dorsal hippocampal interleukin-1β signaling is critical to the
development of SEFL. Future studies could investigate whether the same neurobiological
13
In summary, our findings demonstrate that exposure to chronic escalating heroin
administration produces a heroin withdrawal animal model. Furthermore, exposure to chronic
heroin administration and spontaneous withdrawal is capable of producing a PTSD-like
phenotype in rats. Collectively, these data provide important new evidence that chronic heroin
administration and withdrawal can alter learning and memory processes. These data may lead to
future experiments that may provide a possible mechanism that contributes to the similarities in
symptomology and overwhelming comorbidity of opiate use disorders and PTSD.
FUNDING AND DISCLOSURE
This research was supported by National Institute on Drug Abuse (NIDA) grants R01
DA034721, T32 DA007244, andF31 DA047054, a National Science Foundation grant
DGE-1144081, a Richard A. King Research Excellence Award, and a Behavioral Neuroscience
14
REFERENCES
Bennett, A. S., L. Elliott, A. Golub, B. Wolfson-Stofko and H. Guarino (2017). "Opioid-Involved Overdose Among Male Afghanistan/Iraq-Era U.S. Military Veterans: A Multidimensional Perspective." Subst Use Misuse 52(13): 1701-1711.
Bhattacharya, S. K., A. Chakrabarti, M. Sandler and V. Glover (1995). "Rat brain monoamine oxidase A and B inhibitory (tribulin) activity during drug withdrawal anxiety." Neurosci Lett 199(2): 103-106.
Bowler, R. M., H. Han, V. Gocheva, S. Nakagawa, H. Alper, L. DiGrande and J. E. Cone (2010). "Gender differences in probable posttraumatic stress disorder among police responders to the 2001 World Trade Center terrorist attack." Am J Ind Med 53(12): 1186-1196.
Bremner, J. D., S. M. Southwick, A. Darnell and D. S. Charney (1996). "Chronic PTSD in Vietnam combat veterans: course of illness and substance abuse." Am J Psychiatry 153(3): 369-375.
Carcoba, L. M., A. E. Contreras, A. Cepeda-Benito and M. W. Meagher (2011). "Negative affect heightens opiate withdrawal-induced hyperalgesia in heroin dependent individuals." J Addict Dis 30(3): 258-270.
De Vries, T. J., A. N. Schoffelmeer, R. Binnekade, A. H. Mulder and L. J. Vanderschuren (1998). "Drug-induced reinstatement of heroin- and cocaine-seeking behaviour following long-term extinction is associated with expression of behavioural sensitization." Eur J Neurosci 10(11): 3565-3571.
Edwards, S., D. L. Graham, K. N. Whisler and D. W. Self (2009). "Phosphorylation of GluR1, ERK, and CREB during spontaneous withdrawal from chronic heroin self-administration." Synapse 63(3): 224-235.
Fatahi, Z., A. Zeinaddini-Meymand, S. Karimi-Haghighi, M. Moradi, F. Khodagholi and A. Haghparast (2020). "Naloxone-precipitated withdrawal ameliorates impairment of cost-benefit decision making in morphine-treated rats: Involvement of BDNF, p-GSK3-beta, and p-CREB in the amygdala." Neurobiol Learn Mem 167: 107138.
Finley, E. P., S. Schneegans, C. Tami, M. J. Pugh, D. McGeary, L. Penney and J. Sharpe Potter (2018). "Implementing prescription drug monitoring and other clinical decision support for opioid risk mitigation in a military health care setting: a qualitative feasibility study." J Am Med Inform Assoc 25(5): 515-522.
Gellert, V. F. and S. G. Holtzman (1978). "Development and maintenance of morphine tolerance and dependence in the rat by scheduled access to morphine drinking solutions." J Pharmacol Exp Ther 205(3): 536-546.
15
Gipson, C. D., K. E. Dunn, A. Bull, H. Ulangkaya and A. Hossain (2020). "Establishing
preclinical withdrawal syndrome symptomatology following heroin self-administration in male and female rats." Exp Clin Psychopharmacol.
Highfield, D., J. Yap, J. W. Grimm, U. Shalev and Y. Shaham (2001). "Repeated lofexidine treatment attenuates stress-induced, but not drug cues-induced reinstatement of a heroin-cocaine mixture (speedball) seeking in rats." Neuropsychopharmacology 25(3): 320-331.
Holmes, A., P. J. Fitzgerald, K. P. MacPherson, L. DeBrouse, G. Colacicco, S. M. Flynn, S. Masneuf, K. E. Pleil, C. Li, C. A. Marcinkiewcz, T. L. Kash, O. Gunduz-Cinar and M. Camp (2012). "Chronic alcohol remodels prefrontal neurons and disrupts NMDAR-mediated fear extinction encoding." Nat Neurosci 15(10): 1359-1361.
Houshyar, H., F. Gomez, S. Manalo, A. Bhargava and M. F. Dallman (2003). "Intermittent morphine administration induces dependence and is a chronic stressor in rats."
Neuropsychopharmacology 28(11): 1960-1972.
Jacobsen, L. K., S. M. Southwick and T. R. Kosten (2001). "Substance use disorders in patients with posttraumatic stress disorder: a review of the literature." Am J Psychiatry 158(8): 1184-1190.
Jones, M. E., C. L. Lebonville, D. Barrus and D. T. Lysle (2015). "The role of brain interleukin-1 in stress-enhanced fear learning." Neuropsychopharmacology 40(5): 1289-1296.
Jones, M. E., C. L. Lebonville, J. E. Paniccia, M. E. Balentine, K. J. Reissner and D. T. Lysle (2017). "Hippocampal interleukin-1 mediates stress-enhanced fear learning: A potential role for astrocyte-derived interleukin-1β." Brain, Behavior, and Immunity.
Jones, M. E., J. E. Paniccia, C. L. Lebonville, K. J. Reissner and D. T. Lysle (2018).
"Chemogenetic manipulation of dorsal hippocampal astrocytes protects against the development of stress-enhanced fear learning." Neuroscience.
Kaouane, N., Y. Porte, M. Vallee, L. Brayda-Bruno, N. Mons, L. Calandreau, A. Marighetto, P. V. Piazza and A. Desmedt (2012). "Glucocorticoids can induce PTSD-like memory impairments in mice." Science 335(6075): 1510-1513.
Kmiotek, E. K., C. Baimel and K. J. Gill (2012). "Methods for intravenous self administration in a mouse model." J Vis Exp(70): e3739.
Koob, G. F. (2008). "A role for brain stress systems in addiction." Neuron 59(1): 11-34.
Koob, G. F. and M. Le Moal (1997). "Drug abuse: hedonic homeostatic dysregulation." Science 278(5335): 52-58.
16
Kreek, M. J., B. L, Z. Y and S. J (2002). Relationships between endocrine functions and
substance abuse syndromes: heroin and related short-acting opiates in addiction contrasted with methadone and other long-acting opioid agonists used in pharmacotherapy of addiction.
Hormones, Brain and Behavior. San Diego, Academic Press: 781-830.
Kuntz, K. L., K. M. Patel, P. S. Grigson, W. M. Freeman and K. E. Vrana (2008). "Heroin self-administration: II. CNS gene expression following withdrawal and cue-induced drug-seeking behavior." Pharmacol Biochem Behav 90(3): 349-356.
Leri, F. and J. Stewart (2001). "Drug-induced reinstatement to heroin and cocaine seeking: a rodent model of relapse in polydrug use." Exp Clin Psychopharmacol 9(3): 297-306.
Liu, L., J. K. Coller, L. R. Watkins, A. A. Somogyi and M. R. Hutchinson (2011). "Naloxone-precipitated morphine withdrawal behavior and brain IL-1beta expression: comparison of different mouse strains." Brain Behav Immun 25(6): 1223-1232.
McCauley, J. L., T. Killeen, D. F. Gros, K. T. Brady and S. E. Back (2012). "Posttraumatic Stress Disorder and Co-Occurring Substance Use Disorders: Advances in Assessment and Treatment." Clin Psychol (New York) 19(3).
McHugh, R. K., V. R. Votaw, D. H. Barlow, G. M. Fitzmaurice, S. F. Greenfield and R. D. Weiss (2017). "Development of an integrated cognitive behavioral therapy for anxiety and opioid use disorder: Study protocol and methods." Contemp Clin Trials 60: 105-112.
McNally, G. P. and H. Akil (2002). "Role of corticotropin-releasing hormone in the amygdala and bed nucleus of the stria terminalis in the behavioral, pain modulatory, and endocrine consequences of opiate withdrawal." Neuroscience 112(3): 605-617.
Meier, A., C. Lambert-Harris, M. P. McGovern, H. Xie, M. An and B. McLeman (2014). "Co-occurring prescription opioid use problems and posttraumatic stress disorder symptom severity." Am J Drug Alcohol Abuse 40(4): 304-311.
Nunez, C., A. Foldes, M. L. Laorden, M. V. Milanes and K. J. Kovacs (2007). "Activation of stress-related hypothalamic neuropeptide gene expression during morphine withdrawal." J Neurochem 101(4): 1060-1071.
Patel, R. S., A. Elmaadawi, S. Nasr and J. Haskin (2017). "Comorbid Post-Traumatic Stress Disorder and Opioid Dependence." Cureus 9(9): e1647.
17
Rubin, D. C., D. Berntsen and M. K. Bohni (2008). "A memory-based model of posttraumatic stress disorder: evaluating basic assumptions underlying the PTSD diagnosis." Psychol Rev 115(4): 985-1011.
Saladin, M. E., K. T. Brady, B. S. Dansky and D. G. Kilpatrick (1995). "Understanding
comorbidity between PTSD and substance use disorders: two preliminary investigations." Addict Behav 20(5): 643-655.
Schulteis, G. and G. F. Koob (1996). "Reinforcement processes in opiate addiction: a homeostatic model." Neurochem Res 21(11): 1437-1454.
Seip, K. M., B. Reed, A. Ho and M. J. Kreek (2012). "Measuring the incentive value of escalating doses of heroin in heroin-dependent Fischer rats during acute spontaneous withdrawal." Psychopharmacology (Berl) 219(1): 59-72.
Shaham, Y., H. Rajabi and J. Stewart (1996). "Relapse to heroin-seeking in rats under opioid maintenance: the effects of stress, heroin priming, and withdrawal." J Neurosci 16(5): 1957-1963.
Szczytkowski-Thomson, J. L., C. L. Lebonville and D. T. Lysle (2013). "Morphine prevents the development of stress-enhanced fear learning." Pharmacol Biochem Behav 103(3): 672-677. Thomas, J. L., J. E. Wilk, L. A. Riviere, D. McGurk, C. A. Castro and C. W. Hoge (2010). "Prevalence of mental health problems and functional impairment among active component and National Guard soldiers 3 and 12 months following combat in Iraq." Arch Gen Psychiatry 67(6): 614-623.
Towers, E. B., B. J. Tunstall, M. L. McCracken, L. F. Vendruscolo and G. F. Koob (2019). "Male and female mice develop escalation of heroin intake and dependence following extended access." Neuropharmacology 151: 189-194.
Xia, L., M. Zhai, L. Wang, D. Miao, X. Zhu and W. Wang (2013). "FGF2 blocks PTSD symptoms via an astrocyte-based mechanism." Behav Brain Res 256: 472-480.
Yamamoto, S., S. Morinobu, S. Takei, M. Fuchikami, A. Matsuki, S. Yamawaki and I. Liberzon (2009). "Single prolonged stress: toward an animal model of posttraumatic stress disorder." Depress Anxiety 26(12): 1110-1117.
Zhou, W. and P. W. Kalivas (2008). "N-acetylcysteine reduces extinction responding and induces enduring reductions in cue- and heroin-induced drug-seeking." Biol Psychiatry 63(3): 338-340.
18