http://jdr.sagepub.com/
Journal of Dental Research
http://jdr.sagepub.com/content/91/1/39
The online version of this article can be found at:
DOI: 10.1177/0022034511423396
2012 91: 39 originally published online 27 September 2011
J DENT RES
M.A. Awad, J.A. Morais, S. Wollin, A. Khalil, K. Gray-Donald and J.S. Feine
Implant Overdentures and Nutrition: A Randomized Controlled Trial
Published by:
http://www.sagepublications.com
On behalf of:
International and American Associations for Dental Research
can be found at: Journal of Dental Research
Additional services and information for
http://jdr.sagepub.com/cgi/alerts
Email Alerts:
http://jdr.sagepub.com/subscriptions
Subscriptions:
http://www.sagepub.com/journalsReprints.nav
Reprints:
http://www.sagepub.com/journalsPermissions.nav
Permissions:
What is This?
- Sep 27, 2011
OnlineFirst Version of Record
- Dec 6, 2011
Version of Record
39 Clinical
DOI: 10.1177/0022034511423396
Received June 13, 2011; Last revision August 16, 2011; Accepted August 17, 2011
A supplemental appendix to this article is published elec-tronically only at http://jdr.sagepub.com/supplemental.
© International & American Associations for Dental Research
M.A. Awad
1*, J.A. Morais
2, S. Wollin
3,
A. Khalil
4, K. Gray-Donald
5,
and J.S. Feine
3,61Department of General & Specialist Dental Practice, College of Dentistry, University of Sharjah, Sharjah, United Arab Emirates; 2Division of Geriatric Medicine, McGill University, MUHC Royal Victoria Hospital, Montreal, Canada; 3Oral Health and Society Research Division, Faculty of Dentistry, McGill University, Montreal, Canada; 4Research Center on Aging, Health and Social Services Center-University Institute of Geriatrics of Sherbrooke, Sherbrooke, Quebec, Canada; 5School of Dietetics and Human Nutrition, McGill University, Montreal, Canada; and 6Department of Epidemiology and Biostatistics and Department of Oncology, Faculty of Medicine, McGill University, Montreal, Canada; *correspond-ing author, [email protected]
J Dent Res 91(1):39-46, 2012
AbstrAct
We conducted a randomized clinical trial to deter-mine whether providing simple mandibular implant overdentures (IODs) to elderly individuals would give them a significantly better nutritional profile than those who receive complete dentures (CDs). Two hundred fifty-five edentate patients > 65 yrs were randomly assigned to receive maxillary CDs and mandibular IODs (n = 128) or CDs (n = 127). Six-month and one-year post-treatment outcomes were blood plasma levels of homocysteine (tHcy), vitamin B12, vitamin B6, albumin, serum folate, and C-reactive protein concentrations, as well as dietary intake. The association between treatment and tHcy levels was not statistically significant. A decline of folate from baseline values in both study groups, as well as those of vitamins B6 and B12 and albumin, was observed. Significant between-group differences were detected in food preparation and in the individu-als’ ability to chew a variety of foods. This study suggests that implant overdentures do not have a more positive effect on the nutritional state of elderly edentate individuals at 6 and 12 mos post-treatment than new complete dentures. However, those wearing IODs are significantly more likely to take in their nutrients through fresh, whole fruits and vegeta-bles. (International Clinical Trial Registration#: ISRCTN24273915)
KEY WOrDs:
implant overdentures, complete dentures, nutrition, diet, elderly, clinical trial.IntrODuctIOn
t
ooth loss has a negative impact on diet; as teeth are lost, masticatory efficiency declines (Wayler and Chauncey, 1983; Wayler et al., 1984; Leake, 1988). Low levels of vitamins C, A, calcium, protein, and fiber have been frequently reported in edentate individuals (Wayler et al., 1984; Greksa et al., 1995). These deficien-cies coincide with alterations in intake of vegetables, meat, nuts, dairy products, and cereals. Furthermore, low vitamin B6 and folate levels are observed in eden-tate persons (Joshipura et al., 1996; Krall et al., 1998).The concentration of plasma homocysteine [tHcy] is inversely related to plasma concentrations of water-soluble vitamins B12, B6, and folate and depends on dietary intake of these vitamins (Selhub, 2002). Studies have linked higher [tHcy] with cardiovascular disease and cognitive dysfunction in elders (Seshadri and Robinson, 2000).
Mandibular implant overdentures (IODs) have been shown to be highly satis-factory to patients, providing significantly improved function and comfort (Feine
et al., 1994; Bouma et al., 1997; Awad and Feine, 1998). Patients wearing IODs find it easier to chew than those wearing complete dentures (CDs); consequently, they may change their diets to include foods that they could not previously eat.
A few studies have investigated the effects of IODs on dietary intake (Sandstrom and Lindquist, 1987; Hamada et al., 2001; Allen and McMillan, 2002). These had several limitations, such as the use of small sample sizes (Sandstrom and Lindquist, 1987; Allen and McMillan, 2002) or having been conducted with male diabetic patients (Hamada et al., 2001). Thus, a study that is specifically designed to assess the impact of IODs on health parameters associ-ated with improved nutritional status in an edentate general population is needed. Therefore, the main objective of this RCT was to assess the effects of mandibular IODs on the nutritional status of an edentate elderly population. We hypothesized that patients who received mandibular IODs would have significantly lower blood serum concentration of homocysteine [tHcy] than those who received CDs at 6 and 12 mos post-treatment.
MAtErIAls & MEthODs
Advertisements were placed in local French and English newspapers for edentate individuals willing to participate in a study of mandibular CDs or
Implant Overdentures and
40 Awad et al. J Dent Res 91(1) 2012
IODs with 2 implants. Respondents were invited to an informa-tion session. The inclusion criteria were: (a) males and females, (b) 65+ yrs of age, (c) edentate for a minimum of 5 yrs, (d) wish to replace their existing CDs, (e) adequate understanding of written and spoken English or French, and (f) willing and able to understand the protocol and give informed consent. Exclusion criteria were: (a) insufficient bone for placement of 2 implants in the anterior mandible, (b) acute or chronic symptoms of TMDs, (c) systemic or neurologic disease that contraindicates implant surgery, (d) any neoplasia diagnosed < 5 yrs previously, (e) body mass index (BMI) less than 20 or more than 32 kg/m2,
and (f) taking dietary supplements, anti-neoplastic medication, phenytoin, or corticosteroids. Ethical approval was granted from the McGill University Institutional Review Board (IRB) (International Clinical Trial Registration #ISRCTN24273915), and all provided written informed consent to participate. Using a computer-generated permuted block scheme, we stratified participants by sex and type 2 diabetes and randomly assigned them to receive mandibular CDs or IODs, both opposed by new maxillary CDs. All patients received financial compensation to participate in the investigation (Fig.).
Intervention
Experimental Group
Participants randomized to the experimental group received max-illary CDs and mandibular IODs on 2 implants with ball attach-ments (ITI, Straumann-048.242/243, Waldenburg, Switzerland) implanted into the canine region of the anterior mandible. After healing for 3 mos, the participants received new dentures in both jaws, a maxillary CD and a mandibular IOD.
control Group
Patients randomized to the control group received maxillary and mandibular CDs fabricated in a standard manner.
Outcome Measures
The primary outcome was blood serum concentration of homo-cysteine [tHcy]. This marker of general health is sensitive to changes in dietary intake of fresh fruits, vegetables, and meats. Secondary outcomes were blood concentrations of folate, vita-min B6, vitavita-min B12, C-reactive protein (CRP), and albuvita-min. All nutritional assessments were conducted at baseline, 6 mos, and 12 mos post-treatment, at the MUHC-Royal Victoria Hospital (RVH) Clinical Investigation Unit (Montreal, Canada). For each assessment, participants arrived in a fasted state. A venous blood sample was drawn from an antecubital vein and was sent to the biochemistry laboratory of MUHC-RVH for analysis of plasma vitamin B12 and serum concentrations of albumin, hypersensitivity CRP (lower range, 0.02 mg), and folate. Laboratory measurements were made with automated or commercial immunoplates. Venous blood not immediately ana-lyzed was centrifuged at -4°C for 10 min, and the supernatant was aliquoted and kept frozen at -80°C. From these, vitamin B6 (pyridoxal 5-phosphate) was measured within 1 mo by radioen-zymatic assay. [tHcy] was measured with an ADVIA Centaur®
System competitive immunoassay (Bayer HealthCare LLC, Berkeley, CA, USA) in single runs and with the human homo-cysteine control Liquicheck™ (Bio-Rad Laboratories, Irvine, CA, USA). The coefficients of variation (CVs) of the low and high controls were 9.2% and 6.6%, respectively. When values of [tHcy] were above 25 μmol/L, samples were re-measured by high-performance liquid chromatography (HPLC) with fluoro-metric detection (Araki and Sako, 1987). The correlation coef-ficient (r) of the ADVIA Centaur® System with HPLC is
reported by the manufacturer to be 0.945. BMI (kg/m2) was
calculated from each participant’s weight and height.
Participants completed a Likert scale questionnaire at base-line, 6 mos, and 12 mos post-treatment to rate level of difficulty associated with chewing foods of various textures, such as meat,
fruits, and vegetables over the preceding 2 wks, for which “very much” was coded as “5” and “without difficulty” was coded as “1”. They were also asked to rate the frequencies of habits, such as food avoidance and dipping food in liquids to facilitate chew-ing and swallowchew-ing, for which “never” was coded as “1” and “always” was coded as “5”.
All were provided with literature outlining healthy lifestyle guidelines (Canada’s Food Guide for Healthy Eating, Katamay
et al., 2007).
sample size Estimation
A sample size of 208 patients (104 IOD, 104 CD) was deter-mined to be sufficient to observe a difference of 1g/L in [tHcy] (SD: 2.0), associated with a 10% reduction in the risk of cardio-vascular disease (Boushey et al., 1995). We sought 95% power, using a two-sided test at an alpha of 0.05, with the primary out-come assessed at 6 mos post-treatment. An anticipated 18% loss to follow-up increased the sample size, totaling 254 individuals (complete denture group, N = 128; implant group, N = 127).
statistical Analysis
Baseline and within-group differences at 6 and 12 mos post-treatment were assessed by paired and independent t tests.
Multivariable regression was used to assess the association among homocysteine, serum folate, vitamins B6 and B12, and BMI, adjusted for confounding variables: baseline values, age, sex, and season. Bonferroni adjustment was applied to blood serum concentration variables and BMI to correct for multiple testing, resulting in a significance level of p < 0.05 divided by 14 (p < 0.0035). For ratings of habits and chewing capacities, this adjustment resulted in a significance level of p < 0.05 divided by 58 (p < 0.0008).
Missing data were replaced with multiple imputation to pri-mary and secondary outcome variables (PASW version 18.0, SPSS Inc., Somers, NJ, USA). This is associated with a greater degree of uncertainty than if the imputed values had actually been observed.
rEsults
Of 255 participants randomized to the IOD (N = 127) and CD groups (N = 128), the cumulative loss to follow-up from the beginning of the study to the 12-month post-treatment assess-ment was 15% in the IOD group (N = 17) and 14% (N = 19) in the CD group. Reasons for withdrawal included fear of surgery, illness, or lack of interest.
The groups were similar (CD, mean 69.7, SD 4.6; IOD, mean 70.5, SD 5.03) and gender distribution [CD, males N = 57
table 1. Within-group* and Between-group** Differences in Outcomes in Complete and Implant Groups at Baseline, 6, and 12 Months Post-treatment
Variable Average Values for Healthy Elderly*** Mean ± SDBaseline Mean ± SD6 Months Mean ± SD12 Months Homocysteine (µmol/L)
Complete denture Implant overdenture
>14 µmol/L
14.2 ± 3.7
15.3 ± 11.9 14.7 ± 4.0
a
5.2 ± 8.4 14.2 ± 3.815.2 ± 7.5 Serum Folate (nmol/L)
Complete denture Implant overdenture
>40 nmol/L
37.6 ± 11.9
37.2 ± 12.6 32.6 ± 13.0
a,c
28.8 ± 10.1a, 29.1 ± 11.1 b,d
25.8 ± 9.7b,d
Vitamin B12 (pmol/L) Complete denture Implant overdenture
<230 pmol/L
259.9 ± 123.1
238.1 ± 105.1 231.7 ± 104.1
a,c
193.2 ± 65.1a,c 207.3 ± 82.2 b,d
194.0 ± 63.2.b,d
Vitamin B6 (nmol/L) Complete denture
Implant overdenture 73.6 ± 62.768.7 ± 51.2 33.8 ± 26.3
a
35.8 ± 26.1a 34.1 ± 28.3 b
30.0 ± 26.0 Albumin (g/L)
Complete denture Implant overdenture
>40 g/L
41.3 ± 2.9
41.4 ± 2.6 40.5 ± 2.6
a
40.3 ± 2.3a 40.5 ± 2.8 b
40.1 ± 2.58b
C-Reactive Protein (mg/L) Complete denture Implant overdenture
>5.0 mg/L
5.5 ± 10.5
5.3 ± 15.5 5.0 ± 7.44.9 ± 8.8 4.9 ± 7.63.8 ± 3.6 Body Mass Index
Complete denture Implant overdenture
28-34
28.7 ± 5.7
28.5 ± 5.4 28.5 ± 5.528.0 ± 4.5 29.0 ± 6.128.1 ± 4.7 *Based on paired t test.
**Based on independent t test. ***Selhub et al., 1999.
aSignificant within-group difference between baseline and 6 mos. bSignificant within-group difference between baseline and 12 mos. cSignificant between-group difference at 6 mos.
42 Awad et al. J Dent Res 91(1) 2012
(44.5%), females N = 71 (55.5%); IOD, males N = 57 (44.9%), females N = 70 (55.1%); p = 0.95]; 41 patients (16%) had type 2 diabetes. Both groups were similar on baseline values of homocysteine, serum folate, albumin, vitamin B6, vitamin B12, CRP, and BMI (Table 1).
Statistically, but not clinically, significant within-group dif-ferences from baseline to 6 mos post-treatment were observed in [tHcy] (CD group only), serum folate, vitamin B12 , vitamin B6, and albumin (p < 0.0035). At 12 mos post-treatment, no within-group differences from baseline were observed in [tHcy] (p > 0.0035). However, serum folate, vitamins B12 and B6, and albumin concentrations dropped from baseline to 6 and 12 mos post-treatment in both groups (p < 0.0035).
The between-group means for [tHy] were not different at 6 or 12 mos post-treatment (p > 0.0035). Unexpectedly, folate and vitamin B12 values were higher in the CD than in the IOD group at 6 and 12 mos (p < 0.0035).
Half of the participants had [tHcy] in the fourth quartile (> 16.50 μmol/L). Further, the percentage of participants with
serum folate levels in the 4th quartile was higher in the CD than in the IOD group at 6 (31% vs. 15%) and 12 mos (27% vs. 19%) post-treatment.
A non-significant association was observed with [tHcy] at 6 and 12 mos and treatment received (p = 0.20 and p = 0.53, respectively; Table 2). A tendency for higher serum folate and vitamin B12 (at 6 mos) among individuals with CD was also observed after adjustment for age, sex, baseline values, and season (Table 2).
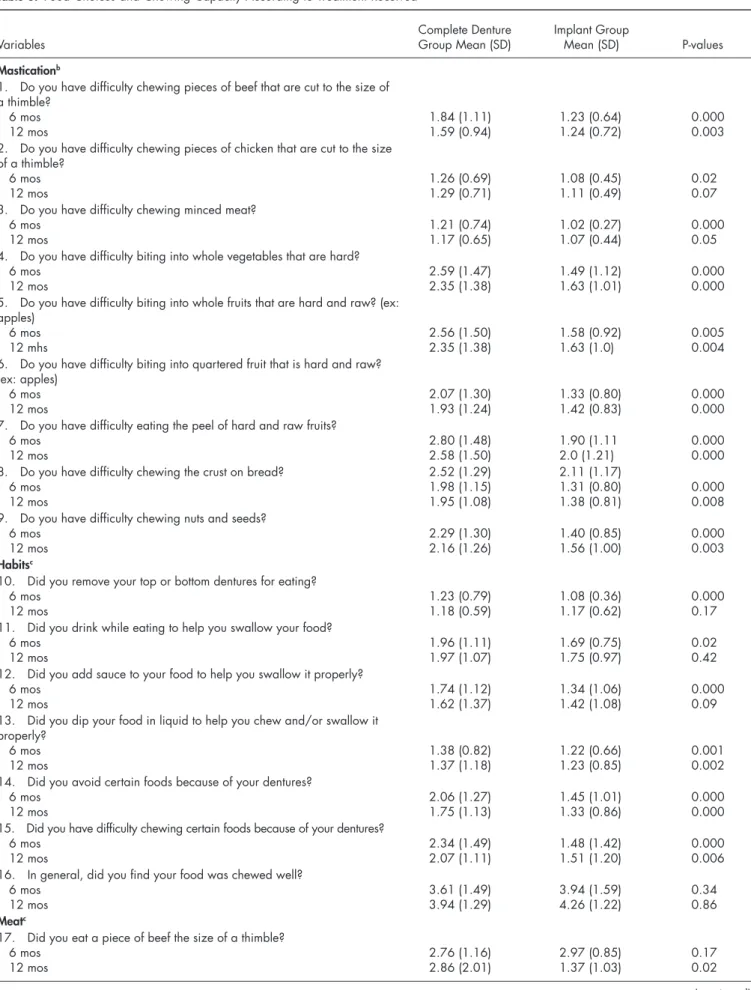
Within-group analysis showed that the IOD group had sig-nificantly more improvements than the CD group from baseline to 12 mos post-treatment in chewing ability and food habits (Appendix Table). IOD group participants reported fewer diffi-culties chewing pieces of beef, vegetables, fruits, bread crust, and nuts than did those in the CD group (p < 0.0008; Table 3). Compared with those who received CDs, IOD participants were less likely to avoid certain foods because of their dentures [6-month post-treatment mean, 2.06 (SD 1.27) vs. 1.45 (1.01), P < 0.0001; 12-month post-treatment mean, 1.75 (1.13) vs. 1.33
table 2. Linear Regression Models* for the Association between 6 and 12 Months Homocysteine, Serum Folate, Vitamin B12, Vitamin B6, Albumin, C-reactive Protein, and Body Mass Index According to Treatment Received
6 Months 12 Months
Variables Standardized B 95% CI Standardized B 95% CI Homocysteine (µmol/L)
Implant –0.02 –0.08, 0.04 –0.03 –0.04, 0.07 Baseline value** 0.89 0.83, 0.95 0.92 0.58, 0.87 Season*** 0.005 –0.07, 0.05 –0.04 –0.08, 0.01 Serum Folate (nmol/L)
Implant –0.15 –0.26, –0.03 –0.15 –0.28, –0.02 Baseline value 0.46 0.34, 0.58 0.41 0.30, 0.52 Season –0.02 –0.13, 0.10 –0.13 –0.25, –0.009 Vitamin B12 (pmol/L)
Implant –0.14 –0.23, 0.05 –0.12 –0.10, 0.08 Baseline value 0.63 0.53, 0.72 0.69 0.60, 0.78 Season –0.06 –0.16, 0.04 0.04 –0.06, 0.13 Vitamin B6 (nmol/L)
Implant 0.04 –0.09, 0.17 –0.08 –0.21, 0.05 Baseline value –0.22 –0.35, –0.09 –0.07 –0.13, 0.15 Season –0.03 –0.16, 0.09 –0.13 –0.26, –0.008 Albumin (g/L)
Implant –0.02 –0.12, 0.10 –0.07 –0.18, 0.04 Baseline value 0.55 0.45, 0.65 0.53 0.42, 0.64 Season –0.11 –0.22, –0.01 –0.13 –0.24, –0.006 C-reactive Protein (mg/L)
Implant –0.03 –0.15, 0.10 –0.11 –0.24, 0.02 Baseline value 0.08 –0.04, 0.20 0.07 –0.06, 0.20 Season 0.11 –0.01, 0.24 –0.10 –0.24, 0.06 Body Mass Index
Implant –0.03 –0.10, 0.04 –0.07 –0.17, 0.02 Baseline value 0.84 0.77, 0.91 0.74 0.59, 0.89 Season 0.04 –0.11, 0.03 –0.05 –0.03, 0.14 *All models adjusted for age and sex.
**Reference category.
table 3. Food Choices and Chewing Capacity According to Treatment Received
Variables Complete DentureGroup Mean (SD) Implant GroupMean (SD) P-values
Masticationb
1. Do you have difficulty chewing pieces of beef that are cut to the size of a thimble?
6 mos
12 mos 1.84 (1.11)1.59 (0.94) 1.23 (0.64)1.24 (0.72) 0.0000.003 2. Do you have difficulty chewing pieces of chicken that are cut to the size
of a thimble? 6 mos
12 mos 1.26 (0.69)1.29 (0.71) 1.08 (0.45)1.11 (0.49) 0.020.07 3. Do you have difficulty chewing minced meat?
6 mos
12 mos 1.21 (0.74)1.17 (0.65) 1.02 (0.27)1.07 (0.44) 0.0000.05 4. Do you have difficulty biting into whole vegetables that are hard?
6 mos
12 mos 2.59 (1.47)2.35 (1.38) 1.49 (1.12)1.63 (1.01) 0.0000.000 5. Do you have difficulty biting into whole fruits that are hard and raw? (ex:
apples) 6 mos
12 mhs 2.56 (1.50)2.35 (1.38) 1.58 (0.92)1.63 (1.0) 0.0050.004 6. Do you have difficulty biting into quartered fruit that is hard and raw?
(ex: apples) 6 mos
12 mos 2.07 (1.30)1.93 (1.24) 1.33 (0.80)1.42 (0.83) 0.0000.000 7. Do you have difficulty eating the peel of hard and raw fruits?
6 mos
12 mos 2.80 (1.48)2.58 (1.50) 1.90 (1.112.0 (1.21) 0.0000.000 8. Do you have difficulty chewing the crust on bread?
6 mos 12 mos
2.52 (1.29) 1.98 (1.15) 1.95 (1.08)
2.11 (1.17) 1.31 (0.80)
1.38 (0.81) 0.0000.008 9. Do you have difficulty chewing nuts and seeds?
6 mos
12 mos 2.29 (1.30)2.16 (1.26) 1.40 (0.85)1.56 (1.00) 0.0000.003
habitsc
10. Did you remove your top or bottom dentures for eating? 6 mos
12 mos 1.23 (0.79)1.18 (0.59) 1.08 (0.36)1.17 (0.62) 0.0000.17 11. Did you drink while eating to help you swallow your food?
6 mos
12 mos 1.96 (1.11)1.97 (1.07) 1.69 (0.75)1.75 (0.97) 0.020.42 12. Did you add sauce to your food to help you swallow it properly?
6 mos
12 mos 1.74 (1.12)1.62 (1.37) 1.34 (1.06)1.42 (1.08) 0.0000.09 13. Did you dip your food in liquid to help you chew and/or swallow it
properly? 6 mos
12 mos 1.38 (0.82)1.37 (1.18) 1.22 (0.66)1.23 (0.85) 0.0010.002 14. Did you avoid certain foods because of your dentures?
6 mos
12 mos 2.06 (1.27)1.75 (1.13) 1.45 (1.01)1.33 (0.86) 0.0000.000 15. Did you have difficulty chewing certain foods because of your dentures?
6 mos
12 mos 2.34 (1.49)2.07 (1.11) 1.48 (1.42)1.51 (1.20) 0.0000.006 16. In general, did you find your food was chewed well?
6 mos
12 mos 3.61 (1.49)3.94 (1.29) 3.94 (1.59)4.26 (1.22) 0.340.86
Meatc
17. Did you eat a piece of beef the size of a thimble? 6 mos
12 mos 2.76 (1.16)2.86 (2.01) 2.97 (0.85)1.37 (1.03) 0.170.02
44 Awad et al. J Dent Res 91(1) 2012
(0.86), p < 0.0008]. IOD participants were less likely to cut fruits and vegetables into small pieces for chewing (Table 3).
DIscussIOn
To our knowledge, this is the first RCT specifically designed to answer the question of whether simple mandibular IODs improve the nutritional state of independently living edentate elders. It was postulated that replacing CDs with IODs in patients with functional problems should favor the consumption of more raw foods rich in nutrients like B vitamins, leading to a reduction in [tHcy], a known marker of cardiovascular disease
risk. In this study, providing mandibular IODs and maxillary CDs to edentate elders did not corroborate this hypothesis.
It was also expected that changes would occur in plasma levels of the most important B vitamins. Contrary to expecta-tions, the levels of folate and vitamins B6 and B12 decreased from baseline to 6 and 12 mos, more so for folate and vitamin B12 in the IOD than the CD group (Tables 1 and 3). These find-ings contradict preliminary results by the authors (Morais et al., 2003), in which an increase in vitamin B12 in the implant group was observed at 6 mos post-treatment. In this study, IOD inter-vention appeared to have a negative impact on plasma folate and serum vitamin B12 concentrations, with the effect persisting in
Variables Complete DentureGroup Mean (SD) Implant GroupMean (SD) P-values 18. Did you find it necessary to mince the beef before eating it?
6 mos
12 mos 1.74 (1.11)1.63 (1.59) 1.24 (0.86)1.37 (1.27) 0.080.10 19. Did you eat a piece of chicken the size of a thimble?
6 mos
12 mos 3.17 (1.13)3.17 (1.31) 3.33 (1.31)3.24 (1.33) 0.100.21 20. Did you find it necessary to mince the chicken before eating it?
6 mos
12 mos 1.36 (0.85)1.28 (0.70) 1.11 (0.44)1.16 (0.57) 0.060.03 21. Did you find it necessary to puree the meat before eating it?
6 mos
12 mos 1.12 (0.51)1.14 (0.58) 1.03 (0.20)1.08 (0.44) 0.0000.01
Fruitsc
22. Did you eat a whole apple that was hard and raw? 6 mos
12 mos 2.15 (1.69)2.65 (1.53) 3.17 (1.68)3.06 (1.30) 0.070.06 23. Did you find it necessary to remove the skin before eating the apple?
6 mos
12 mos 3.18 (1.94)3.44 (2.22) 2.65 (1.81)2.67 (1.86) 0.040.09 24. Was it necessary to cut the apple into quarters to chew it properly?
6 mos
12 mos 3.65 (2.05)3.52 (2.48) 2.67 (1.50)2.67 (1.73) 0.080.07 25. Was it necessary to cut the apple into pieces the size of a quarter to
chew it properly? 6 mos
12 mos 2.33 (1.63)2.14 (1.59) 1.41 (1.33)1.62 (1.46) 0.0000.03 26. Was it necessary to puree hard and raw fruits in order to eat them?
6 mos
12 mos 1.57 (1.0)1.62 (1.11) 1.12 (0.46)1.21 (0.80) 0.0000.000
Vegetablesc
27. Did you eat a whole and raw carrot? 6 mos
12 mos 2.68 (1.13)2.28 (2.1) 3.21 (1.30)2.97 (1.68) 0.0030.008 28. Was it necessary to cut the carrot into quarters in order to chew it
properly? 6 mos
12 mos 2.52 (2.07)3.28 (2.02) 1.89 (1.74)1.97 (1.57) 0.020.003 29. Was it necessary for you to puree the raw vegetables in order to eat
them? 6 mos
12 mos 1.70 (1.38)1.48 (1.33) 1.20 (0.69)1.39 (0.99) 0.0000.005
aAnalysis was based on independent t test.
bResponse codes: 1, without difficulty; 2, a little difficulty; 3, enough difficulty; 4, much difficulty; 5, very much difficulty. cResponse codes: 1, never; 2, rarely; 3, occasionally; 4, often; 5, always.
folate up to 12 mos post-treatment. Plasma folate has a short half-life; thus, its decline in the IOD group by the 6th and 12th mos should not have been influenced by the surgical procedure that may have temporarily reduced food intake. However, sea-son can affect the accessibility of folate-rich foods, which might have contributed to this unexpected result. Regardless, it is unlikely that implants would cause folate alone to decrease while other nutrients remain unaffected. It is more plausible to consider shifts in food patterns, since patients with IODs report that they can chew better (Awad et al., 2003). Perhaps partici-pants in the implant group switched from drinking beverages fortified with folic acid to fresh fruits and raw vegetables whose folate content is less. Of interest is that folate values are in the high range, a reflection of the enrichment of flour in Canada. However, the decline of folate and vitamins B6 and B12 from baseline values in both groups may have been caused by par-ticipants who did not refrain from taking vitamins as requested prior to baseline data gathering, which is reflected in the rela-tively high standard deviation at baseline in vitamin B6 and B12 values (Table 2). A decline from baseline was also significant for albumin, a strong marker of mortality and disability in the elderly (Corti et al., 1994); however, it remained above 40 g/L (associated with good health) for most participants.
BMI remained stable over time and at healthy levels in both groups (Janssen et al., 2005).
Of interest is that CRP, a marker of inflammation associated with CVD (He et al., 2010), remained stable over time, but at levels associated with an increased risk above 2 mg/L (Ridker
et al., 2005). A trend toward lower values in the IOD group was observed at 12 mos (p = 0.09), suggesting that IOD patients have improved inflammatory status over those who wear CDs. In the implant group, this decrease reached a value considered to be clinically significant (1.3 mg/L; Cushman et al., 2005).
The provision of IODs versus CDs was associated with fewer difficulties chewing fruits, vegetables, meats, and avoidance of certain foods. These findings substantiate previous research by this group (Feine et al., 1994; Awad et al., 2003; Thomason et al., 2003) and others (Geertman et al., 1996; Assunção et al., 2007) on the positive impact of IODs on chewing ability. Additionally, food preparation was easier for the IOD group. Arguably, if IODs reduce the need for special food preparation, such as peeling hard or raw fruits and adding sauce to assist in swallowing, then eating is a much more enjoyable experience. This is reflected in our findings that those in the IOD group reported improvements in oral-health-related quality of life (Emami et al., 2010).
This trial has several strengths. First, random assignment of participants ensured equivalence of both groups at baseline. Second, assessments were conducted at 6 and 12 mos post-treatment, pro-viding ample time for participants to get accustomed to their new prostheses and to feel comfortable enough to attempt eating a vari-ety of foods. Third, attrition was relatively low and taken into consideration in the design and statistical analysis phases.
There were some study limitations: A follow-up period lon-ger than 12 mos might be needed to observe a reduction in homocysteine and CRP, both associated with a clinically impor-tant change in risk of cardiovascular disease. Alternatively,
changing eating habits or increasing the frequency of eating specific foods may be more complex than simply providing an efficient prosthesis. Instead, eating habits and food preferences could be influenced by a variety of factors, including socio-economic and behavioral (Schlettwein-Gsell, 1992). In addition, nutritional counseling could be provided, which may allow for change to occur in eating habits (Bradbury et al., 2008; Ellis
et al., 2010). We also recommend that future studies consider the inclusion of an age-matched dentate group and should focus on edentate populations whose diet is compromised. Thus, there will be room and opportunity for dietary improvement.
In summary, these findings show that, although patients who received IODs had significant improvement in ability to chew and food habits, clinically important differences in blood nutri-ents and health parameters were not observed.
AcKnOWlEDGMEnts
This study was funded by the Canadian Institutes of Health Research and Straumann Canada Ltd. The authors are grateful to Nicolas Drolet and Dr. Louise Johnson-Down. The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
rEFErEncEs
Allen F, McMillan A (2002). Food selection and perceptions of chewing ability following provision of implant and complete prostheses in com-plete denture wearers. Clin Oral Implants Res 13:320-326.
Araki A, Sako Y (1987). Determination of free and total homocysteine in human plasma by high-performance liquid chromatography with fluo-rescence detection. J Chromatogr 422:43-52.
Assunção WG, Zardo GG, Delben JA, Barão VA (2007). Comparing the efficacy of mandibular implant-retained overdentures and complete dentures among elderly edentulous patients: satisfaction and quality of life. Gerodontology 24:235-238.
Awad MA, Feine JS (1998). Measuring patient satisfaction with mandibular prostheses. Community Dent Oral Epidemiol 26:400-405.
Awad M, Lund J, Shapiro S, Locker D, Klemetti E, Chehade A (2003). Oral health status and treatment satisfaction with mandibular implant over-dentures and complete over-dentures: a randomized clinical trial in a senior population. Int J Prosthodont 16:390-396.
Bouma J, Boerrigter LM, Van Oort RP, van Sonderen E, Boering G (1997). Psychosocial effects of implant-retained overdentures. Int J Oral Maxillofac Implants 12:515-522.
Boushey CJ, Beresford SA, Omenn GS, Motulsky AG (1995). A quantitative assessment of plasma homocysteine as a risk factor for vascular dis-ease. Probable benefits of increasing folic acid intake. J Am Med Assoc
274:1049-1053.
Bradbury J, Thomason JM, Jepson NJ, Walls AW, Mulvaney CE, Allen PF,
et al. (2008). Perceived chewing ability and intake of fruit and vegeta-bles. J Dent Res 87:720-725.
Corti MC, Guralnik JM, Salive ME, Sorkin JD (1994). Serum albumin level and physical disability as predictors of mortality in older persons. J Am Med Assoc 272:1036-1042.
Cushman M, Arnold AM, Psaty BM, Manolio TA, Kuller LH, Burke GL,
et al. (2005). C-Reactive protein and the 10-year incidence of coronary heart disease in older men and women. The Cardiovascular Health Study. Circulation 112:25-31.
46 Awad et al. J Dent Res 91(1) 2012
Emami E, Allison PJ, de Grandmont P, Rompré PH, Feine JS (2010). Better oral-health-related quality of life: type of prosthesis or psychological robustness? J Dent 38:232-236.
Feine JS, Maskawi K, de Grandmont P, Donohue WB, Tanguay R, Lund JP (1994). Within-subject comparison of implant-supported mandibular pros-theses. Evaluation of masticatory function. J Dent Res 73:1645-1656. Geertman ME, van Waas MA, van’t Hof MA, Kalk W (1996). Denture
sat-isfaction in a comparative study of implant-retained mandibular over-dentures: a randomized clinical trial. Int J Oral Maxillofac Implants
11:194-200.
Greksa LP, Parraga IM, Clark CA (1995). The dietary adequacy of edentu-lous older adults. J Prosthet Dent 73:142-145.
Hamada MO, Garret NR, Roumanas ED, Kapur KK, Han T, Chen T, et al. (2001). A randomized clinical trial comparing the efficacy of mandibu-lar implant-supported overdentures and complete dentures in diabetic patients. Part IV: comparison of dietary intake. J Prosthet Dent 85: 53-60.
He L, Tang X, Ling W, Chen W, Chen Y (2010). Early C-reactive protein in the prediction of long-term outcomes after acute coronary syndromes: a meta-analysis of longitudinal studies. Heart 96:339-346.
Janssen I, Katzmarzyk PT, Ross R (2005). Body mass index is inversely related to mortality in older people after adjustment for waist circum-ference. J Am Geriatr Soc 53:2112-2118.
Joshipura KJ, Willett WC, Douglass CW (1996). The impact of edentulous-ness on food and nutrient intake. J Am Dent Assoc 127:459-467. Katamay SW, Esslinger KA, Vigneault M, et al. (2007). Eating well with
Canada’s Food Guide: Development of the food intake pattern.
Nutrition Reviews 65:155-166.
Krall E, Hayes C, Garcia R (1998). How dentition status and masticatory function affect nutrient intake. J Am Dent Assoc 129:1261-1269. Leake JL (1988). A review of regional studies on the dental health of older
Canadians. Gerodontology 7:11-19.
Morais JA, Heydecke G, Pawliuk J, Lund JP, Feine JS (2003). The effects of mandibular two-implant overdentures on nutrition in elderly edentu-lous individuals. J Dent Res 82:53-58.
Ridker PM, Cannon CP, Morrow D, Rifai N, Rose LM, McCabe CH, et al. (2005). C-reactive protein levels and outcomes after statin therapy. N Engl J Med 352:20-28.
Sandström B, Lindquist LW (1987). The effect of different prosthetic resto-rations on the dietary selection in edentulous patients. A longitudinal study of patients initially treated with optimal complete dentures and finally with tissue-integrated prostheses. Acta Odontol Scand 45:423-428.
Schlettwein-Gsell D (1992). Nutrition and the quality of life: a measure for the outcome of nutritional intervention? Am J Clin Nutr 55(6 Suppl):1263S-1266S.
Selhub J (2002). Folate, vitamin B12 and vitamin B6 and one carbon metabolism. J Nutr Health Aging 6:39-42.
Selhub J, Jacques PF, Rosenberg IH, Rogers G, et al. (1999). Serum total homocysteine concentration in the third National Health and Nutrition Examination Survey (1991-1994) population reference ranges and con-tribution of vitamin status to high serum concentrations. Ann Intern Med 131:331-339.
Seshadri N, Robinson K (2000). Homocysteine, B vitamins, and coronary artery disease. Med Clin North Am 84:215-237.
Thomason JM, Lund JP, Chehade A, Feine JS (2003). Patient satisfaction with mandibular implant overdentures and complete dentures 6 months after delivery. Int J Prosthodont 16:467-473.
Wayler AH, Chauncey HH (1983). Impact of complete dentures and impaired natural dentition on masticatory performance and food choice in healthy aging men. J Prosthet Dent 49:427-433.