Research Article
Emotional, physical and sexual abuse and its psychological impact
in children
Sameh Saad
1*, Rania K. H. Hashish
2, Rehab I. Abdel-Karim
2, Ghada F. Mohammed
3INTRODUCTION
Child abuse was defined by World Health Organization (WHO) as all forms of physical and/or emotional ill-treatment, sexual abuse, neglect or negligent ill-treatment, commercial or other exploitation, resulting in actual or potential harm to the child’s health, survival, development or dignity in the context of a relationship of responsibility, trust or power.1 Several studies have been undertaken to explore the risk factors regarding child abuse. In this regard, poverty, lower level of parental education, large families, young parental age and low family income have been suggested as plausible risks or eliciting factors.2,3
Various studies have addressed the problem of child abuse in Suez Canal area, however they either depended on cases reported from autopsy reports or did not study all types of abuse, especially sexual abuse which might lead to underestimation of the size of the problem.4 The present study supposes also that there is increasing level of abuse as there is increase in social violence. Hence, this study was conducted to identify the pattern of different types of child abuse, risk factors and psychological consequences in children attending Suez Canal University Hospital (emergency department and dermatology clinic) in Ismailia city, Egypt.
ABSTRACT
Background: To date, there are no accurate Egyptian epidemiologic studies evaluating the magnitude of the problem
of child abuse and its psychological impact. This study was conducted to the pattern of child abuse, its risk factors and its psychological impact in children attending Suez Canal University Hospital.
Methods: This cross sectional study involved 735 child and their guardians, they completed questionnaires and Arabic version of Brief Symptom Inventory (BSI) checklist through a structured personal interview. They had undergone full history-taking; general examination for signs of violence.
Results: All participating children were exposed to violence. Out of the 735 participating children; 53 (7.2%) were exposed to all types of abuse (emotional/physical/sexual). The study shows statistically significant relationships between the type of abuse and each of child's age, residence, father and mother educational levels, family structure, and family history of psychopathology/substance abuse. It also has a significant effect on anxiety, depression, phobia, somatization and obsessive-compulsive disorders
Conclusions: Child abuse is still prevalent in our culture. It is imperative to support the activities of child abuse prevention in order to decrease its psychological consequence in the community.
Keywords: Child abuse, Emotional abuse, Physical abuse, Sexual abuse
1Department ofEmergency Medicine, Faculty of Medicine, Suez Canal University, Ismailia, Egypt
2Department of Forensic Medicine and Clinical Toxicology, Faculty of Medicine, Suez Canal University, Ismailia,
Egypt
3
Department ofDermatology and Venereology, Faculty of Medicine, Suez Canal University, Ismailia, Egypt
Received: 10 May 2016
Accepted: 10 June 2016
*Correspondence:
Dr. Sameh Saad,
E-mail: sameh_er2005@hotmail.com
Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
METHODS
This is a cross sectional descriptive study was conducted between March 2013 and August 2013. (The chronological steps appear in Figure 1). It was conducted in accordance with the guidelines of the Helsinki Declaration and performed after obtaining written informed consent from all children's guardians; Confidentiality regarding children's and their families' identities was maintained as the used questionnaire was anonymous.
Participants
Children [child is an individual less than 18 years] were recruited from those attending emergency department/dermatology clinic, Suez Canal University hospital, Ismailia, Egypt. The study included any child lives in Ismailia city, aged up to 18 years; attending the Emergency department/Dermatology clinic in the period between March 2013 and August 2013. Children whose guardians refused to participate or to give informed consent were excluded from the study (Figure 1).
Tools
Finally, 735 children were enrolled. All participants (children and their guardians) through a structured personal interview - completed a questionnaire included demographic data and data related to suspected risk factors of child abuse. The questionnaire was predesigned by researchers based on and modified from tools used in other studies.5 Arabic version of brief symptom inventory (BSI) checklist - a 53 item checklist - was used to assess psychological distress in children more than 13 years old.6 BSI was designed to evaluate a broad range of symptoms and psychological problems.7
It was used as it is a practical and concise screening tool; and it can be used by non-experts.It is scored in terms of nine subscales covering nine forms of symptom dimensions such as somatization, obsessive-compulsive, interpersonal sensitivity, depression, anxiety, hostility, phobia, anxiety, paranoid ideation, and psychoticism.8 Participants rank each item on a 5 degree scale range from 0 (not at all) to 4 (extremely), this ranking describes the intensity of distress.8 BSI reliability ranges from 0.71-0.85, its internal consistency is α=0.96.8 Each child was examined carefully for signs of general violence. For ethical considerations, anal and genital examinations were performed only upon children presented to the dermatology clinic complaining from itching, discharge, anal lesions and seeking medical consultation. This intimate examination was performed by the dermatologist researcher and their data were included in the study after obtaining their guardians' informed consent.
Statistical analysis
Statistical analysis was performed using SPSS version 20.0 (SPSS, Inc, an IBM Company, Chicago, Illinois). Categorical variables were presented as frequencies and
percentages. Chi-square test was used to test significance of difference for qualitative variables. One-way ANOVA test was used for correlations between the type of child abuse and BSI subscales. Statistical significance was defined as P <0.05.
RESULTS
Out of 735 children, 398 (54.1%) of them were males and 337 (45.9%) were females. Their mean age was 13±7.8 years, ranging from 1.2 to 18 years. All the participating children were exposed to both emotional and physical abuse (Table 1); the patterns of their exposure to emotional and physical abuse are shown in Tables 2 and 3. Out of the 735 participant children 53 (7.2%) were exposed to all types of abuse (Table 4). The current study demonstrates that emotional and physical abuses were mainly perpetrated by mothers, followed by fathers and teachers sexual abuse was higher with non-relative perpetrators (p < 0.005) (Table 5).
Most of the participated children didn't show any abnormal finding on general body examination, with some exceptions (Table 6), the commonest sign of child abuse that was detected among the study group is body bruises with a percent 12.4%. Out of 735 children, 278 children aged 13 years and above, BSI was used for their psychological assessment. ANOVA showed a high significant effect of exposure to various types of child abuse on obsessive-compulsive disorder, anxiety and phobia (p <0.05). Significant effect was also noticed on somatization and depression (p <0.05), while there is no significant effect on interpersonal sensitivity, hostility, paranoia and psychoticism (p ˃0.05) (Table 7).
DISCUSSION
Child abuse is a recognized problem in communities of low- and middle-income countries. The current study was conducted to identify the pattern of different types of child abuse, risk factors and its psychological impact in children attending Suez Canal University Hospital (emergency department and dermatology clinic) in Ismailia city, Egypt. This study revealed that all children had experienced both physical and emotional abuse, however only 7.2% of them had experienced at least one form of sexual abuse.
Those results were higher than those of Hassan, and his colleagues.4 This result was not surprising knowing that in the Arab world parents and educators tend to support the use of corporal punishment for discipline and education, they can also be related to the increased social stressors and violence noticed recently in the community.9
Physical and emotional abuses were practiced more on young children (6 to 12 years) in this study. Young children are helpless, can't defend themselves and can be easily frightened.4
that88.3% of sexually abused children were between 10 and 18 years old.10
Table 1:Relationship between different types of child abuse and the characteristics of the participant children attended Suez Canal University hospitals.
Variable Type of child abuse
Emotional abuse N =735
Physical abuse N =735
Sexual abuse
N = 53 X
2 test P value
N (%) N (%) N (%)
Age (years)
0 up to 6 6 up to 12 12 up to 18
103 (14) 354 (48.2) 278 (37.8)
103 (14) 354 (48.2) 278 (37.8)
6 (11.3) 15(28.3) 32(58.4)
11.2575 0.023817*
Gender
Male Female
398 (54.1) 337 (45.9)
398(54.1) 337 (45.9)
31(58.5) 22(41.5)
0.3885 0.823471
Father's level of education
Illiterate
Primary education Less than high school High school
Bachelor’s degree or higher
208 (28.3) 191(26.4) 80 (10.9) 155 (21.1) 101 (13.7)
208 (28.3) 191 (26.4) 80 (10.9) 155 (21.1) 101 (13.7)
19(35.8) 13(24.5) 17(32.1) 2 ( 3.8) 2 (3.8)
32.1103 0.000215*
Mother's level of education
Illiterate
Primary education Less than high school High school
Bachelor’s degree or higher
328 (44.7) 211(28.7) 79 (10.7) 22 (3) 95 (12.9)
328 (44.7) 211(28.7) 79 (10.7) 22 (3) 95 (12.9)
16(30.2) 14(26.4) 19(35.8) 2(3.8) 2(3.8)
24.6622 0.001773*
Residence
Rural Urban
189 (25.7) 546(74.3)
189 (25.7) 546 (74.3)
2(3.8)
51(96.2) 13.1512 0.001394*
Religion
Muslim Non-Muslim
502 (68.3) 233 (31.7)
502 (68.3) 233 (31.7)
40(75.5) 13(24.5)
1.2206 0.54318
Family structure
Together Separated Widow
509 (69.3) 206 (28) 20 (2.7)
509 (69.3) 206 (28) 20 (2.7)
13(24.5) 40(75.5) 0 (0)
55.3566 <0.00001*
If cases not together, Who do the child live with (n=226)
Father Mother Stepfather Stepmother Others
72 (31.9) 89 (39.4) 1 (0.14) 3 (0.41) 61(8.3)
72 (31.9) 89 (39.4) 1 (0.14) 3 (0.41) 61 (8.3)
15(28.3) 4 (7.5) 1 (1.9) 1 (1.9) 19(35.8)
17.237 0.027734*
Family history of psychopathology
Yes No
256(34.9) 479(65.1)
256(34.9) 479(65.1)
35 (66) 18 (34)
21.6462 0.000383*
Family history of substance abuse
Yes No
569(77.4) 166(22.6)
569(77.4) 166(22.6)
53(100) 0 (0)
15.3068 0.000474*
X 2: Chi-square test; *Statistically significant (p < 0.05).
However, Elgendy and Hassan reported that the higher rates of sexual abuse cases were found in the age group 6 to 12 years.11 Low rates of abuse among younger children
agreement with those of Afifi et al who reported that the rate sexual abuse increase with age, while that of physical abuse decrease with age.12
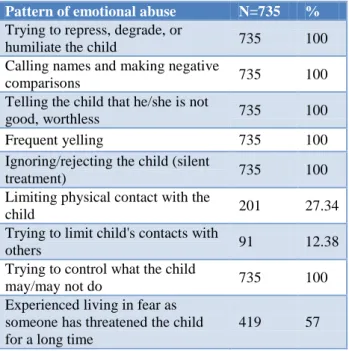
Table 2: Pattern of emotional abuse among the participating children attended Suez Canal University
hospitals.
Pattern of emotional abuse N=735 %
Trying to repress, degrade, or
humiliate the child 735 100 Calling names and making negative
comparisons 735 100 Telling the child that he/she is not
good, worthless 735 100 Frequent yelling 735 100 Ignoring/rejecting the child (silent
treatment) 735 100
Limiting physical contact with the
child 201 27.34
Trying to limit child's contacts with
others 91 12.38
Trying to control what the child
may/may not do 735 100 Experienced living in fear as
someone has threatened the child for a long time
419 57
The current study reported no gender difference for any type of abuse as was reported by Hassan et al.4 On the other hand; Al-Eissa et al found that females were at greater risk of victimization for physical and psychological abuse.13 No gender difference regarding sexual abuse was detected by other studies.11,13 Al Eissa et al and Afifi et al, referred that to the social norms that protect girls and keep their proximity to caregivers, at the same time they provide boys with more freedom thus predisposing them to a greater risk of sexual victimization producing similar rates of sexual victimization by gender or even increasing sexual victimization in males.12,13 However, other studies detect that girls are more sexually victimized than boys.10,14 This also might be explained by the fact that male victims might refuse to admit being exposed to sexual abuse.15 In this study, most of abused children were resident in urban areas; however this is not a community based study and the results can't be generalized, furthermore, all cases were collected from a university hospital in an urban region (Ismailia) and those living in urban region outnumbered those in rural regions who come to that hospital mostly for serious conditions. These results agree with those of Hagras who found that sexually assaulted victims were more common in urban areas, but disagree with, Aboul-Hagag and Hamed who reported that the prevalence of sexual abuse was more in rural area.10,16 The difference in results might also be due to the characteristics of the collected sample as they investigated university students and the university
community includes students from both rural and urban region.
Table 3: Pattern of physical abuse upon the participating children attended Suez Canal University
hospitals.
Pattern of emotional abuse N=735 %
Hitting the child 735 100 Smacking child's face 735 100 Holding child firmly against his/her
will
735 100
Hitting the child with his/her fist(s) 501 68.2 Hitting the child with a hard object 735 100 Kicking the child 523 71.2 Pushing the child violently 222 30.2 Beating the child 735 100 Burning with cigarette puts 23 3.12 Trying to strangle the child 12 1.63
Table 4: Pattern of sexual abuse upon the participating children attended Suez Canal University
hospitals.
Pattern of sexual abuse N=53 %
Look at child's genitals 53 100 Touched parts of child's body other
than the genitals in a sexual way
53 100
Forced the child to touch parts of his/her body in a sexual way
53 100
Forced the child to watch a pornographic movie/photos
26 49.05
Forced the child to participate in a pornographic movie/photos
0 0
Forced to child to watch him masturbate
3 5.66
Show child's body naked 49 92.45 Touched child's genitals 53 100 Used child's body to satisfy him/her
sexually
31 58.49
Forced the child to touch someone else’s genitals
12 1.63
Tried to or put his penis into child's mouth or rectum
5.66 3
Tried to or put an object into child's mouth or rectum.
7.54 4
Have full sexual intercourse with penetration
35.84 19
poverty, alcohol/drug use and a rapidly-changing system of norms. Disclosure and asking help after abuse was
hindered by structural barriers and stigmatization.4
Table 5:Relationship between the perpetrator and different types of child abuse among the participating children attended Suez Canal University hospitals.
Type of abuse Emotional abuse
N =735
Physical abuse N =735
Sexual abuse
N =53 X
2
test p value
Perpetrator(relative) N (%) N (%) N (%)
Father 599 (81.5 ) 695 (94.6 ) 9 (17)
280.6969 < 0.00001** Mother 679 (92.4 ) 735(100) 0 (0)
Older sister/brother 512(69.7) 221(30.1) 10(18.9) Uncle/aunt 381(51.8 ) 139( 18.9) 16(30.2) Grandmother 439(59.7 ) 241(32.8 ) 0 (0)
Perpetrator(non-relative)
Teacher 616(83.1) 563(76.6 ) 9 (17)
210.6367 < 0.00001** Boss 58 (7.9) 27 (3.7) 22 (41.1)
Stranger 41(5.6 ) 32 (4.4 ) 21(39.7)
** Highly statistically significant (p < 0.005) X 2: Chi- square
Table 6: Finding of general body examination of the abused children attended Suez Canal University
hospitals.
% N (735) Signs of abuse
1.22 9
Traction alopecia
2 15
Cigarette burn
12.4 91
29 17 33 3 9
Body bruises (n=91)
Head Arm Legs Back Abdomen
4.1 30
29 15 1 27 27
Body petichias (n=30)
Head Arm Legs Back Abdomen
0.7 5
Fracture bone
2 15
Oral wart
0.7 5
Anal wart
0.27 2
Anal tear
1.63 12
Anal molluscum
Various studies concluded that the parents' level of education is considered an important risk factor for child abuse. Abusing parents tend to be illiterate or less educated in agreement with the present study which might be due to lack of parenting skills.18 On the other hand, Jaudes et al observed a higher risk of both neglect and abuseamong children of mothers who had graduated from high school or had some college education; they related that to the family level of frustration of not being able to live with their full potentials.19
BSI: Brief symptom inventory.
Figure 1: Study flow chart.
Culture helps form parental attitudes about how children should be disciplined.20 Beliefs, religion and attitudes towards child upbringing among other things vary between different societies. In some communities, striking, slapping or shouting at children is a societal norm, so such practices usually occur, irrespective of parental education, age, or social status. The Egyptian culture values child's power assertive discipline and obedience, hence, corporal maltreatment and punishment are expected to be a common practice.4 Divorce/separation was negatively associated with experienced psychological aggression/sexual coercion in this study. A 75% of sexually abused children were from families with separated parents in current study. Several studies reported that parental divorce increased odds of all types of child abuse when compared to intact families.21 Living away from the family is considered as a risk factor in child abuse which might be due to lacking of parental care, supervision, protection and love.
The study was conducted between March 2013 and August 2013 according to the guidelines of
the Helsinki Declaration
1012 Children were recruited from those attending Emergency department and Dermatology clinic, Suez Canal University
hospital, Ismailia, Egypt
277 Children were excluded as their guardians refused to participate or to give informed
consent.
735 (children and their guardians) - through a structured personal interview - completed a questionnaire, 278 filled the Arabic version of
BSI.
Furthermore, it exposes the child to persons who may try to take advantage of him/her which might explain increased sexual abuse in children living with other persons outside family.12 The current study revealed that 69% of abused children are from families where parents are living together, but we didn't study the relationship between parents in details. Domestic violence between parents, quarrels or other marital problems may increase social stressors, hence creates unhealthy child rearing environment and may increase the risk of abuse. Parents who have problems or are the victims of violence are
more likely to have difficulty in being emotionally available for their children.12 The current study found that 66% of sexually abused children had family history of psychopathology, while it represented only 34.9% for both physical and emotional abuse. Family history of psychopathology and substance abuse are important risk factors which increase stress in the family and are associated with parental abuse of their children as parents become less emotionally involved with their children and show poor parenting skills.22,23
Table 7:Relationship between the type of child abuse and the psychiatric diagnosis according to the Brief Symptom Inventory (BSI) scale among the participating children attended Suez Canal University hospitals.
p value ANOVA-test
Type of child abuse
Sexual abuse N = 32 Physical abuse
N =278 Emotional abuse
N = 278 Scales of the BSI
Mean±SD Mean±SD
Mean±SD
0.023* 4.018
1.1±1.1 8.2±4.3
8.2±4.3 Somatization
0.000** 14.931
1.2±1.3 7.1±1.5
7.1±1.5 Obsessive-Compulsive
0.914 0.091
3.2±2.3 4.3±5.6
4.3±5.6 Interpersonal Sensitivity
0.026* 3.818
4.3±5.6 9.5±5.3
9.5±5.3 Depression
0.000** 9.760
3.2±5.3 8.5±3.4
8.5±3.4 Anxiety
0.371 1.004
0 3.7±4.3
3.7±4.3 Hostility
0.000* 11.743
1.2±1.3 9.2±2.3
9.2±2.3 Phobia
0.454 0.410
0 7.2±4.8
7.2±4.8 Paranoia
0.489 1.434
0 5.3±3.3
5.3±3.3 Psychoticism
SD: standard deviation; BSI: Brief Symptom Inventory; * Statistically significant (p < 0.05); ** Highly statistically significant (p <0.005).
Corporal punishment and physical abuse are more likely to be adopted in families where parents smoked and used alcohol or psychoactive drugs.12,18 In consistence with those studies, the present study revealed that a higher percentage of child abuse in families with a history of substance abuse. During the interviews with children's guardians, they considered that using emotional and physical violence was a way of correcting behavior of children. Regarding parents; it may reflect the difficulties of parenting and the variety of techniques that parents use to modify child behavior. Several studies addressed the problem of violence against children in Arab countries.13,18 What really worsen the problem in Arab World is the support of parents and educators to the use of physical punishment as an educational and disciplinary tool.9Violence against children was accepted as a method of disciplinarians with children aged 13-17.24In a study in Alexandria, Egypt, 80% of boys and 60% of girls had been physically abused for the purpose of discipline.18
It is a common sense that parents start with threatening before physical punishment, so verbal punishment and physical abuses are commonly used together.18,25 This explains the result in the current study as well as in other studies as it was noticed that the prevalence of both physical and emotional abuses are closely related.17 Violence may escalate gradually starting by threatening, yelling and humiliation by calling names, and then
develops into smacking the face, firm holding and hitting which represent the most common experiences in the current study. Then violence may progress to more dangerous practices as showing weapons to the child, burning with cigarette butts and trying to strangle the child. This gradual escalation was also noticed in other studies.13,17 Regarding sexual abuse, it might be underestimated in many studies, as these studies depended on maternal reporting of sexual victimization of their children where many mothers may not be aware of their children victimization.26 Sexual abuse is often hidden within families, it may not be known until the victim disclose it later in life, furthermore, many children refrain from admitting exposure to it.12
staff were the most common perpetrators of physical abuse or emotional and combined abused (49.3% and 44.2%).12
However parents are most common perpetrators of child physical abuse, the case is different for child sexual abuse.30 The current study revealed that the most common perpetrators of sexual abuse were from outside the family as the boss of the working child or strangers, followed by uncles, older brothers, fathers and teachers. Several studies reported that strangers were the most common perpetrators of sexual abuse.10,16 In cases where Sexual perpetrator is known by the victim child abuse reporting becomes problematic.28 General body examination in the present study was mostly normal. Bruises represented the most common type of injury which is consistent with another study which found that bruises were the most common and the second common type of injury.12 However, it should be noticed that this study was conducted in a sample attending the hospital for different clinical indications and not attending for management of acute injuries due to recent abusive assaults, so injuries are less than expected. Some of children of this study had oral, anal warts and anal molluscum contagiosum. This might be due to sexual cause or non-sexual causes, but in the present study sexual cause was approved by history.31 The impact of child abuse on child's psychiatric status raises many legal and psychological issues; as exposure to child abuse may be associated with several psychiatric disorders. For this reason, psychiatric assessment of the participating children is of prime importance.
The increasing risk of psychiatric disorder after emotional and physical abuse was revealed in present study; children had depression, anxiety, somatization and obsessive-compulsive disorders On the other hand; the most common psychiatric disorders among sexually abused children are anxiety, depression followed by inter-personal sensitivity disorders. These findings are supported by those of other studies.32,33 The present study shows that the type child abuse has a significant effect on anxiety, depression, obsessive-compulsive disorder, phobia and somatization disorders and non-significant effect on interpersonal sensitivity, hostility, paranoia and psychoticism. These results are in agreement with Neumann et al who determined the significant effect of abuse on anxiety, depression, obsessions and somatization disorders.34
These results can be explained by that children exposure to high degrees of trauma as physical or sexual abuse may leads to over activation of the brain neurological pathways which are responsible for “fight or flight” response, frequent exposure for prolonged times - especially at periods of critical brain development - makes the brain chemically organized in a dysfunctional manner, which appears in the form of poor mental and physical state as well as maladaptive behaviors (aggression); mood disorders (anxiety, depression); somatization and posttraumatic stress disorder.35 The current study concluded that child abuse is a serious
problem in our culture and is associated with later psychological disorders. These results can support the concept that the activities of child abuse prevention can play a role in decreasing the rate of psychological disorder in the community. Further studies are recommended to examine the characteristics and risk factors of all types of abuse. Psychological support programs should be directed towards abused children. The limitations of the study were that the sample is convenience; it may not be representative of the community. Lack of the control of the confounding factors with child abuse, as the psychological outcome may be the product of social or personal factors. Mood congruency can constitute a potential bias; as depressed individuals can recall negative experiences and exaggerate childhood adversity. Memory recall can be considered as a bias as this study depends on the recall of abused children and their mothers.
For ethical considerations; anal and genital examination was not performed upon all cases and was done only for those presented seeking medical consultation, so other cases of sexual abuse might have been missed. No clear distinction was made between corporal punishment and physical abuse. In the present study; repeated acts of physical violence (more than three times per month) is considered as physical abuse.
Funding: No funding sources Conflict of interest: None declared
Ethical approval: The study was approved by the Institutional Ethics Committee
REFERENCES
1. World Health Organization. Report of the Consultation on Child Abuse Prevention, 29-31 March 1999. Geneva, Switzerland: World Health Organization (WHO/HSC/PVI/99.1).
2. Straus M, Gelles R, Steinmetz S. Physical violence in the American family. Beverly Hills, CA: Sage Publications. 1990.
3. Bethea L. Primary prevention of child abuse. American Family Physician. 1999;59(6):1577-85. 4. Hassan F, Refaat A, El-Sayed H, El-Defrawi MH.
Disciplinary Practices and Child Maltreatment among Egyptian Families in an Urban Area in Ismailia. Egyptian J Psyc. 1999;22:177-93.
5. Kooiman CG, Ouwehand AW. The Sexual and Physical Abuse Questionnaire (SPAQ). A screening instrument for adults to assess past and current experiences of abuse. Child Abuse Neglect. 2002;26:939-53.
6. Al-Krenawi A, Lev-Wiesel R, Sehwail MA. Psychological symptomatology among Palestinian male and female adolescents living under political violence 2004-2005. Community Ment. Health J. 2007;43(1):49-56.
assessment in primary care settings. Mahwah, NJ: Lawrence Erlbaum Associates; 2000:297-334. 8. Derogatis LR. BSI Brief Symptom Inventory:
Administration, Scoring, and Procedures Manual (4th Ed). Minneapolis, MN: National Computer Systems. 1993.
9. Alyahri A, Goodman R. Harsh corporal punishment of Yemeni children: occurrence, type and associations. Child Abuse Neglect. 2008;32:766-73. 10. Hagras AM, Moustafa SM, Barakat HN, El-Elemi
AH. Medico-legal evaluation of child sexual abuse over a six-year period from 2004 to 2009 in the Suez Canal area, Egypt. Egyptian Journal of Forensic Sciences. 2011;1:58-66.
11. Elgendy IS, Hassan NA. Medicolegal Study of Child Sexual Abuse in Greater Cairo, Egypt, During a 7-Year Period 2005-2011. American journal of Forensic Medicine and Pathology. 2013;34:335-41. 12. Afifi ZEM, El-Lawindi IMI, Ahmed ISA, Basily
WW. Adolescent abuse in a community sample in Beni Suef, Egypt: prevalence and risk factors. Eastern Mediter Health J. 2003;9:1003-17.
13. Al-Eissa MA, AlBuhairan FS, Qayad M, Saleheen H, Runyan D, Almuneef M. Determining child maltreatment incidence in Saudi Arabia using the ICAST-CH: A pilot study. Child Abuse Neglect. 2015;42:174-82.
14. MacMillan HL, Tanaka M, Duku E, Vaillancourt T. Child physical and sexual abuse in a community sample of young adults: Results from the Ontario Child Health Study. Child Abuse Neglect. 2013;37:14-21.
15. Holmes WC, Slap GB. Sexual abuse of boys: definition, prevalence, correlates, sequeale, and management. The J American Medi Associ. 1998;280:1855-62.
16. Aboul-Hagag KE, Hamed AF. Prevalence and pattern of child sexual abuse reported by cross sectional study among the university students, Sohag University, Egypt. Egyptian J Foren Scie. 2012;2:89-96.
17. Christoffersen MN, Armour C, Lasgaard M, Andersen TE, Elklit A. The prevalence of four types of childhood maltreatment in Denmark. Clin Pract Epid Mental Health. 2013;9:149-56.
18. Youssef RM, Attia MS, Kamel MI. Children experiencing violence: parental use of corporal punishment. Child Abuse Neglect.1998;22:959-73. 19. Jaudes PK, Ekwo A, Voorhis JV. Association of
drug abuse and child abuse. Child Abuse Neglect. 1995;19:1065-75.
20. Wamoyi JM, Wight D, Plummer M, Mshana GM, Ross D. Transactional sex amongst young people in rural northern Tanzania: An ethnography of young women’s motivations and negotiation. Reprod Health. 2010;7:2.
21. Afifi TO, Boman J, Fleisher W, Sareen J. The relationship between child abuse, parental divorce,
and lifetime mental disorders and suicidality in a nationally representative adult sample. Child Abuse Neglect. 2009;33:139-47.
22. Walsh C, MacMillan H, Jamieson E. The relationship between parental psychiatric disorder and child physical and sexual abuse: Findings from the Ontario Health Supplement. Child Abuse Neglect. 2002;26:11-22.
23. Walsh C, MacMillan HL, Jamieson E. The relationship between parental substance abuse and child maltreatment: Findings from the Ontario Health Supplement. Child Abuse Neglect. 2003;27:1409-25. 24. Egypt UNICEF. Egypt Programme Profile: Child Protection. Situation in Egypt. Retrieved in December, 2014. Available at http: // www. unicef. org/egypt/protection.html. Accessed on 21 December 2016.
25. Hemenway D, Solnick S, Carter J. Child- rearing violence. Child Abuse Neglect. 1994;18:1011-20. 26. Theodore AD, Chang JJ, Runyan DK, Hunter WM,
Bangdiwala SI, Agans R. Epidemiologic Features of the physical and sexual maltreatment of children in the Carolinas. Pediatrics. 2005;115:e331-7.
27. Goldman JDG, Padayachi UK. The prevalence and nature of child sexual abuse in Queensland, Australia. Child abuse Neglect. 1997;21:489-98. 28. Feng JY, Chang YT, Chang, HY, Fetzer S, Wang JD.
Prevalence of different forms of child maltreatment among Taiwanese adolescents: A population-based study. Child Abuse Neglect. 2015;42:10-9.
29. Machado C, Goncalves M, Matos M, Dias AR. Child and partner abuse: Self-reported prevalence and attitudes in the north of Portugal. Child Abuse Neglect. 2007;31:657-70.
30. Gilbert R, Widom CS, Brown K, Fergusson D. Burden and consequences of child maltreatment in high-income countries. Lancet. 2009;373:68-81. 31. Sinclair KA, Woods CR, Sinal SH. Venereal warts in
children. Pediatr Rev. 2011;32:115-21.
32. Fergusson DM, Horwood LJ, Lynskey MT. Childhood sexual abuse and psychiatric disorder in young adulthood: II. Psychiatric outcomes of childhood sexual abuse. Journal of the American Academy of Child Adolescent Psychiatry. 1996;35(10):1365-74.
33. Briere J, Elliott DM. Prevalence and psychological sequelae of self-reported childhood physical and sexual abuse in a general population sample of men and women. Child Abuse Neglect. 2003;27:1205-22. 34. Neumann DA, Houskamp BM, Pollock VE, Briere J.
The long-term sequelae of childhood sexual abuse in women: a meta-analytic review. Child Maltreatment. 1996;1:6-16.
35. Leeb RT, Lewis T, Zolotor AJ. A review of physical and mental health consequences of child abuse and neglect and implications for practice. American J Lifest Medi. 2011;5:454-68.