Mediators ofInflammation3, 57-60(1994)
THElocalproductionoftumournecrosisfactor-0t(TNF0t)
wasevaluated inthe cerebrospinal fluid (CSF) from ten
patientswithtuberculous meningitis(TBM).Thedegree of intrathecal immune activation was also studied by assessingthe CSF levels of2-microglobulin (2-M) and adenosine deaminaseactivity(ADA).Resultsindicatethat elevated CSF concentrations of TNF0t,
12-M
and ADAwere found in all TBM patients. Moreover, TNF0t is
producedandselectivelyconcentrated foralong periodof time,while
2-M
and ADAvalues progressively declineduringthe course ofTBM. Our findings suggest thatin
TBMpatients, after an early activationofimmune cells, thereisanenhanced andcontinuousproductionof TNF0t atthe site of infection.
Key words: Adenosine deaminase, fl2-microglobulin,
Cere-brospinal fluid, Immune activation, Tuberculous meningitis,
Tumournecrosis factor-cz
Tumour
necrosis factor-=
production
and
immune
cell
activation
in
tuberculous
meningitis
C. M. Mastroianni,cA F. Paoletti, C. Valenti, A. P. Massetti, V. Vullo and
S.
DeliaInstitute of Infectious Diseases, University
’La
Sapienza’, Policlinico Umberto I, Viale Regina Elena 331, 00161 Rome, Italy
CACorresponding Author
Introduction
Tumour
necrosis factor-o(TNFo
0
is a cytokinemainly
releasedby
cells of themonocyte-macrophage lineage
inresponse
to lipopolysacchar-ide(LPS)
and other immune and inflammatorystimuli. It has been
recognized
as a primarymediator in the
pathogenesis
of infection, injuryand
inflammation andin the beneficialprocesses
ofhost
response.
Inparticular, TNFe
isanimportantmacrophage-activating
factor for antibacterial re-sistance against infections causedby
facultative intracellular organisms, such as mycobacteria.2In
experimentalmodels ithas beenreported
thatTNF
enhancesmacrophage
phagocitic capacity andmycobacterial killing by
humanmacrophages.
In
addition, recent lines ofevidence indicated thatTNF
issynthesizedinlarge
amountsinpulmonary
tuberculosis andit is
locally
concentratedat thesiteofdiseaseactivity.4,s
To
date, little is known aboutthe intrathecal
production
ofTNF
during
thecourse of tuberculous meningitis
(TBM).
6There-fore,it
appears
tobe ofinteresttoevaluate the localproduction
and release ofTNFo
in thecere-brospinal
fluid(CSF)
ofpatientswithTBM.
In
the presentstudy, TNFo
concentrations weremeasuredin CSF specimens obtained from
hospital
patients
on admission andduring
the course ofTBM.
In order to determine the extent to whichcell-mediated immunity is involved in the disease,
the CSF levels of two markers of immune
activation, such as
fl2-microglobulin
(/2-M)
andadenosine deaminase activity
(ADA),
were alsomeasured.
Materials and Methods
Patients:
Ten
patients withTBM (five
males, fivefemales)
admitted to the Institute of InfectiousDiseases of the University ofRome
’La Sapienza’,
wereenrolled in this
study.
Themeanagewas 34.4years (range,
12-55years). TBM
wasdiagnosed
on the basis offindings
in the CSF. In six cases CSFsmears werepositive
by
acid-fast staining and fluid culturesgrew
Mycobacterium tuberculosis; in theremaining patients, diagnosis was made
by
compatible cytological
and biochemicalfindings,
supported by
clinical features andsymptomatic
improvement with antituberculoustherapy.
Allpatients were sero-negative for human
immuno-deficiency virus
(HIV)
and did not have other disturbances ofimmunity.A
total of 66CSF samples
was collected fromTBM
patients before starting treatment andsubsequently
atvariousintervals oftimeduringthe course of infection.CSF specimens were also obtained from 15
patientswith non-infectious
neurological
disorders, including cerebrovascular disease,hydrocephalus,
encephalomyelitis
andepilepsy.
CSF specimens,
upon
collection, wereplaced
ina
refrigerated
centrifuge
(4C)
andspun
at3000
rpm
for 10min. Cell supernatantswere storedat
-80C
until use.Assay
for
TNF:TNF
concentrations inCSFweremeasured
by
a quantitative immunoenzymaticsandwich assay
(Quantikine,
R&DSystems,
Min-neapolis, MN,
USA).
Samples
and standards wereC. M. Mastroiannietal.
incubated in anti-TNF monoclonal
antibody-coated
polystyrene
microtiter wells.A
horseradishperoxidase-conjugated
anti-TNF0polyclonal
anti-body
wasthenadded and allowedtobindtheTNF
captured by
the firstantibody, completing
the sandwich. Afterwashing,
substrate solution was added to the wells. The reaction wasstopped
by
addition of 2N
HiSO
4 and optical density(OD)
at 492nmwasmeasured usinganELISA
microreader.To
estimate the amount ofTNFz
in the CSFsamples
we constructed a standard curveby
usingconcentrations of
TNF
ranging from 0 to1000pg/ml.
Unknown values ofTNF
in thesamples
were determinedby referring
to thestandard curve and
expressed
aspg/ml.
The detection limit ofthe assay was 4.8pg/ml.
Assay
for fie-M: /2-M
concentrations were assessedby
theIMx
system(Abbott
Laboratories, NorthChicago,
IL, USA),
according
tothe manufacturer’sinstructions. The
IMx
system is based on arapid
microparticle enzyme immunoassay
(MEIA),
in which submicronparticles are coated witha mousemonoclonal antibody specific
for/2-M.
Theuse ofmicroparticles increases the assay kinetics and
decreases the assay incubation. The sensitivity of
the IMx
/2-M
was calculated to be better than5
tg/1.
Normal/2-M
values were consideredequal
or less than 3
mg/1.
ADA activity measurement:
ADA
activity wasmea-sured in fresh CSF
samples
aftercentrifugation
at300g for 10min.
ADA
assay wasperformed
at37C by
using the colorimetric method ofGiusti,vbased onthe determination of the amount of
NH3
released in the reaction mixture. The enzymatic activity was calculatedby referring
to a standardcurve of ammonium
sulphate
in buffer and wasexpressed
asIU/37C/1.
NormalADA
values were consideredequal
or less than 4IU/1.
Statistical analysis: The Mann-Whitney
U-test
was used for statistical analysis.Results
CSF levels of
TNF,
/2-M
andADA
weremeasured in ten patients with
TBM
and in 15 controlsubjects
withnon-infectiousCNS
disorders.Data
are shown in Figure 1 and areexpressed
asmean
+
SEM.TNF
concentrations inTBM
patients
(155_21.62pg/ml)
were significantlyhigher
than those found in controls(5.69-+-0.77
pg/ml)
(p
< 0.0001).
Similarly,TBM
patients had elevatedCSFvaluesof/32-M
(8.69
___
1.07mg/1)
andADA (10.83
_+
1.61IU/37C/1)in
comparisonwith those observed in thenon-TBM
cases(1.34
-t- 0.12mg/1
and 1.02 0.16IU/37C/1,
respectively) (p
<
0.0001 forboth).
The kinetics ofTNF0 and both
j2-M
andADA
values
during
the course ofTBM
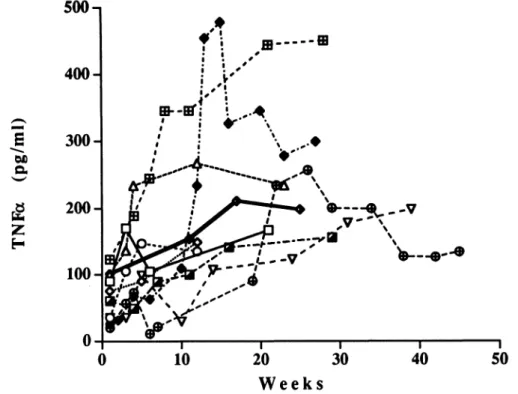
were illustratedrespectively in Figures 2 and 3.
In all patients
CSF
levels ofTNF
were low on admission, then progressively increased andre-mained detectable for a
long period
of time.Antibiotictreatmentdidnot
appear
toinfluencetheTNF
levels.Similarly,
there was no correlationbetweenthecytokineconcentrationsandthe clinical course of the disease.
Onthe
contrary,/2-M
andADA
values resultedto be elevated on admission.
Later,
a progressivedecline was observed.
Only
two patients withculture-proven TBM
showed a further increase inCSF/2-M
andADA
values,despite
theadministra-tionof antituberculoustreatment. The
peak
of these12-/
I0-
8-
6-
4-
2-
0-150
O-FIG. 1. Levelsof/t2-M, ADAandTNF intheCSFsamples (n 66) fromTBM patients comparedwiththose (n 15) obtained in controlswith non-infectiousneurologicaldiseases.Dataare expressed as themean
___
SEM.Comparisonsbetweengroupsaremade by non-parametrictest(Mann-WhitneyU-test)and differencesinCSFlevelsof/Y2-M, ADAandTNFwere statistically significant(p <0.0001 forall).300
200
100
0
0
10
20
30
40
50
Weeks
FIG.2.Timecourse ofTNFlevelsinsequentialCSFsamples from thetenTBMpatients.
10
20 40
Weeks
.0
0 10 20 30 40
Weeks
FIG.3.Time course ofJ2-MandADAlevelsinsequentialCSFsamples
fromthe tenTBMpatients.
immuneactivation markerswas associated with the
development
of complications(hydrocephalus,
hemiplegia)
and an unfavourable clinical course ofmeningitis.
Discussion
Cetl-mediated immunity
plays
an important role in the control of infectionsby M.
tuberculosis. Itiswidely
assumed thatT-lymphocytes,
through
lymphokine-mediated macrophage
activation, are the major immune cells involved both in thepathogenesis and protective mechanisms in human tuberculosis.1
5’0
In the case ofTBM,
it is conceivable that theinvolvement of cellular immune system mainly
occursin thecentralnervoussystem
(CNS).
In
this respect, thedosage
in theCSF
of two markers ofimmune activation, such as
fl2-M
andADA,
representsauseful tool toinvestigatethe
degree
towhich cell-mediatedimmunity is stimulated in the
CNS.
/2-M
is a portion of the majorhistocompat-ibility
complex
class I antigen(MHC-1)
and isexpressed
on the surface oflymphocytes
andmacrophages.
Withregard
to the adenosinedeaminase, the activity of this
enzyme
is increased inlymphoid
cells,especially during
T-cellprolifera-tionand differentiation.
Previous investigations have
already
demon-$0 strated a close correlation between elevated CSF
ADA
values andTBM,
1’12 whileanincreaseintheCSFconcentrations
of/2-M
has beenreported
only
C. M. Mastroianniet al.
study,
both/2-M
andADA
levels were found tobe elevated in the CSF ofall
TBM
patients, thusindicating
a marked stimulation ofimmune systemwithin the CNS. The increased CSFlevels
of/2-M
were
possibly
a consequence of cell-mediatedcytotoxicity directed against
macrophages
infectedby M.
tuberculosis.14 The elevation of CSFADA
values was most likely related to the local immune
response
as the result ofproliferating lymphocytes
in
response
to mycobacterial antigen.Intrathecalimmune activation
appears
to be also associatedwithincreasedcytokine expressionintheCNS.
Indeed,ourresults showed thatTBM
patientshad significantly higher CSF
TNFo
concentrationsthan those found in control
subjects
withnon-infectious
neurological
diseases. The localproduction
ofTNF
is low in the initialphase
ofTBM,
whilethepeak
in theCSF concentrationwasobtained later.
Moreover,
the CSF levels of thiscytokine didnot decrease
during
the course of thedisease, but
they
were elevated for along
time in all patients, irrespective of the antibiotictherapy
and the clinicalcourseof
TBM.
Thispatternisquitedifferentfrom thatobservedinthecase
of/2-M
andADA,
whose levels declinedrapidly during
thecourse of the disease.
Only
two patients whodeveloped
neurological complications showed afurtherincrease inthe
CSF/2-M
andADA
values. Takentogether,
ourfindings
suggest thata greatstimulation ofimmune T-cells primarily occurs in
the acute
phase
ofTBM
and may account for theearly
increase in the CSF/2-M
andADA
values.On the contrary, the enhancement of cytokine
expression related to
TNF production
is a later but moreprolonged phenomenon.
It is likely thatbrain
macrophages
activatedby
T-cell-mediatedpathway
are the source ofTNFo
inTBM
patients.This hypothesis is also
supported by
previous investigations that have demonstrated thatM.
tuberculosis cell wall components can trigger the
release of
TNFo
from human and murinemacrophages,
as well as frompleural
fluidmononuclear cells of patients with
pulmonary
tuberculosis.5,15,16
In conclusion, our data
provide
direct evidence thatTNFo
isproduced
and selectively concentratedfora
long period
oftime in the CSF from patientswith
TBM.
Thechronicrelease ofTNFo
at the siteof the infection suggests that this cytokine maybe
involved in the
complex
immunoregulatorymech-anism that contributes to
mycobacterial
contain-ment and elimination.
References
1. Rosenblum MG, Donato NJ. Tumor necrosis factor : multifaceted peptidehormone.CritRevImmunol1989;9: 21-44.
2. HavellEA. Evidencethattumornecrosisfactor has importantrolein antibacterialresistance.JImmunol 1989; 143: 2894-2899.
3. BermuduzLEM,YoungLS.Tumornecrosisfactor, alone in combination withIL-2,butnotIFN-gamma,isassociated withmacrophage killing of Mycobacteriumaviumcomplex.JImmunol1988; 140: 3006.
4. BarnesPF,FongS-E, Brennan Pj,Twoney PE,MazumderA,ModlinRL. LocalproductionoftumornecrosisfactorandIFN-yintuberculouspleuritis.
JImmuno11990; 145: 149-154.
5. TakashimaT,UetaC, Tsuyuguchi I, Kishimoto S. Production oftumor
necrosisfactoralpha bymonocytes frompatientswithtuberculouspleuritis.
InfectImmun1990; 58: 3286-3292.
6. GlimakerM,KragsbjergP,Forsgren M,Olc&nP.Tumornecrosis
factor-(TNF00 incerebrospinal fluid from patients with meningitisat different etiologies: highlevelsofTNFindicate bacterialmeningitis.JInfectDis 1993;167: 882-889.
7. GiustiG.Adenosine deaminase.In:Bergmeyer HU,ed. MethodsinEnwmatic
Analysis.Wienhen:VerlagChemie, 1974; 1092-1099.
8. Leveton C, BarnassB,ChampionB,etal. T-cell mediatedprotectionin mice againstvirulentMycobacteriumtuberculosis.InfectImmun1989; 57: 390-395. 9. Ellner J,WallisRS.Immunologicaspects ofmycobacterialinfections. Rev
InfectDis1989; 2(Suppl2):S455-S459.
10. OrmeIM,MillerES,RobertAD,etal.T-lymphocytes mediating protection ofmice against cytolysis during the course of Mycobacterium tuberculosis infection.Evidencefor differentkineticsandrecognitionof widespectrum ofprotein antigens.JImmuno11992;148: 189-196.
11. MalanC,DonaldPR,GoldenM,Taljaard jjF.Adenosine deaminase levels incerebrospinalfluidinthediagnosisof tuberculousmeningitis.JTropMed
Hyg1984;87: 33-40.
12. RiberaE, Martinez-VazquezJM,OcanaI,Segura R,Pascual C.Activityof adenosine deaminaseincerebrospinalfluidfor thediagnosisandfollow-up of tuberculousmeningitisinadults.JInfectDis1987; 155: 603-607. 13. AdachiN. Beta-2-microglobulinlevelsinthecerebrospinalfluid:theirvalue
disease marker.EurNeurol1991;31: 181-185.
14. WallisRS, Vjecha M,Amir-TahmassebM,etal. Influence oftuberculosis humanimmunodeficiencyvirus(HIV-1):enhancedcytokine expression and elevatedfle-microglobulininHIV-1 associated tuberculosis.JInfectDis 1993; 167: 43-48.
15. Moreno C, Taverne J, Mehlert A, et al. Lipoarabinomannan from Mycobacteriumtuberculosis induces theproductionoftumournecrosisfactor from humanandmurinemacrophages.ClinExpImmuno11989; 76: 240-245. 16. Barnes PF, ChatterjeeD,AbramsJS,etal.Cytokine productioninducedby
Mycobacterium tuberculosis lipoarabinomannan. Relationship to chemical
structure.JImmuno11992;149: 541-547.
ACKNOWLEDGEMENTS.This work supportedinpartby grant from M.U.R.S.T.(40% 1991), Rome,Italy. WethankDrPietroGallo(ISS COA, Rome)forhelpin statisticalanalysis.
Received 5 November 1993"
accepted in revised form 7 December 1993
Submit your manuscripts at
http://www.hindawi.com
Stem Cells International Hindawi Publishing Corporation
http://www.hindawi.com Volume 2014
Hindawi Publishing Corporation
http://www.hindawi.com Volume 2014
INFLAMMATIONof
Behavioural
Neurology
Endocrinology
International Journal ofHindawi Publishing Corporation
http://www.hindawi.com Volume 2014
Hindawi Publishing Corporation
http://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporation
http://www.hindawi.com Volume 2014
BioMed
Research International
Oncology
Journal ofHindawi Publishing Corporation
http://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity Hindawi Publishing Corporation
http://www.hindawi.com Volume 2014
PPAR Research
The Scientific World Journal Hindawi Publishing Corporation
http://www.hindawi.com Volume 2014
Immunology Research
Hindawi Publishing Corporation
http://www.hindawi.com Volume 2014
Journal of
Obesity
Journal ofHindawi Publishing Corporation
http://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
Ophthalmology
Journal ofHindawi Publishing Corporation
http://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporation
http://www.hindawi.com Volume 2014
Research and Treatment
AIDS
Hindawi Publishing Corporation
http://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Parkinson’s
Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014 Hindawi Publishing Corporation