R
ENATAJ
ABŁOŃSKA1, R
OBERTŚ
LUSARZ1, J
OANNAR
OSIŃCZUK−T
ONDERYS2,
W
OJCIECHB
EUTH3, W
ALDEMARC
IEMNOCZOŁOWSKI4Functional Assessment of Patients
with Lumbar Discopathy
Czynnościowa ocena pacjentów z chorobą dyskową kręgosłupa
1Department of Neurological and Neurosurgical Nursing, Collegium Medicum in Bydgoszcz,
Toruń in the GCM, Poland
2Department of Diseases of Nervous System, Wrocław Medical Univeristy, Poland
3Department and Clinic of Neurosurgery and Neurotraumatology, Collegium Medicum GCM in Bydgoszcz,
Toruń, Poland
4Department of Methodology Scientific Methodology Labor, Medical College in Bydgoszcz, NCU, Toruń,
Poland
Adv Clin Exp Med 2009, 18, 4, 389–399 ISSN 1230−025X
ORIGINAL PAPERS
© Copyright by Wroclaw Medical University
Abstract
Background.Disc disease is a complex of changes in the structures that make up the intervertebral disc and spinal
canal. Functional assessment is evaluation of the ability to cope with the activities of everyday life.
Objectives.The aim was to functionally assess patients treated surgically for lumbar discopathy before and after
the intervention.
Material and Methods.The study was conducted in a group of 46 patients qualified for surgery for lumbar dis−
copathy. The Repty Functional Index (RFI, Polish: WFR) was used to gather data.
Results.The respondents showed complete operational autonomy both before and after treatment. Scores ranged
from 85–105 points. RFI increased for sphincter control both in urinating (mean increase from 6.96 to 7.0 points) and defecating (6.91 to 7.0 points). The index also rose in the category of locomotion (going on foot from 6.61 to 6.74 points). Decreases were noted in personal care and mobility.
Conclusions.Patients with discopathy of the spine show complete independence in carrying out the activities of
everyday life. The functional assessment was somewhat worse at the time of release from the neurosurgical ward
(Adv Clin Exp Med 2009, 18, 4, 389–399).
Key words:discopathy, spine, evaluation, functioning.
Streszczenie
Wprowadzenie.Choroba dyskowa jest zespołem zmian strukturalnych tworzących krążek międzykręgowy i ka−
nał kręgowy. Ocena czynnościowa to umiejętność radzenia sobie z czynnościami dnia codziennego.
Cel pracy. Ocena czynnościowa chorych leczonych operacyjnie z powodu dyskopatii lędźwiowej kręgosłupa
przed i po zabiegu.
Materiał i metody.Badaniami objęto grupę 46 chorych przyjętych na oddział z powodu dyskopatii lędźwiowej,
którzy zostali zakwalifikowani do leczenia operacyjnego. Do zbierania danych wykorzystano Wskaźnik Funkcjo− nalny „Repty” (WFR).
Wyniki.Respondenci, zarówno przed, jak i po leczeniu operacyjnym wykazują pełną samodzielność; uzyskana
punktacja mieściła się w przedziale 85–105 pkt. WFR zwiększył się w kategorii kontrola zwieraczy, zarówno w od− dawaniu moczu (średnio z 6,96 pkt. do 7,0 pkt.), jak i w oddawaniu stolca (średnio z 6,91 pkt. do 7,0 pkt.). Wska− źnik wzrósł również w kategorii lokomocja – w chodzeniu pieszo: z 6,61 pkt. do 6,74 pkt. Spadek średniej punk− towej odnotowano w samoobsłudze i mobilności.
Wnioski.Pacjenci z chorobą dyskową kręgosłupa wykazują pełną samodzielność w wykonywaniu czynności dnia
codziennego. Ocena czynnościowa badanych jest nieco gorsza po zastosowanym leczeniu operacyjnym, w dniu wypisu z oddziału (Adv Clin Exp Med 2009, 18, 4, 389–399).
Disc disease, also called discopathy or damage to the disc, is a group of structural changes as an aftereffect of disorders of mutually arranged ele− ments creating the intervertebral disc and spinal canal [1–3]. Discopathy is a degenerative disease of the organ of movement and consists of three pathogenic factors which can be analyzed in terms of biomechanics (overload), pathobiology (inflam− mation), and neurophysiology (nociception) [2]. Everyday mechanical wear and the aging process continuously influence the destruction of interver− tebral discs. The process lies in the biomechanical and tissue decomposition of a disc caused by the burden of the spine, inborn defects, as well as spinal damage caused by past disease and injury [4, 5]. Thus the height of the intervertebral disc drops, which destabilizes the whole motive seg− ment and leads to damage of the remaining ele− ments. Its functional abilities worsen in visibly significant ways, i.e. elasticity, carrying capacity, and ability to regenerate [4, 6, 7]. Stimuli that damage tissues in turn cause inflammation, which is a complex defensive reactive of the organism. The hernial process of discopathy causes vertebral canal invasion and reduces its lumen to various degrees, particularly on the lateral sides in which nerve roots run. Roots damaged in this way generate neuropathic pain, as opposed to receptor pain [8].
Although most people complaining of spinal pain are successfully cured by conservative meth− ods, some require surgery; however there is no consensus regarding treatment [7, 9, 10]. The assessment of neurological status is fundamental in deciding the choice of treatment and also the main criterion defining its effectiveness. Despite many clinical observations, great advances in medicine, and experience, spinal pain is common, persistent, and chronic and tends to recur without any perceptible cause. It results in a total inability of the afflicted to perform at work and is also often the cause of total loss of working ability [11]. According to statistics, 90% of the population of the USA experience discopathy sometime during their life. One can assume that the data in other developed countries are similar [10].
Functional assessment is an evaluation of the ability to perform the activities of everyday life. These include the ability to be independent of other persons in satisfying basic life necessities, such as moving, nourishing, controlling physio− logical functions of the organism, and carrying our hygienic activities [12]. Although they are physi− cal processes, they also have a psychological dimension because a deficit of physical efficiency has an unfavorable impact on mood and quality of life. Efficient and independent functioning has sig−
nificant practical and emotional meaning for the patient and is conducive to a feeling of indepen− dence [11].
The aim of this study was to conduct function− al assessments of patients treated surgically for lumbar discopathy before and after the interven− tion, i.e. on the day of leaving the hospital ward.
Material and Methods
The examinations were conducted at the Department of Neurosurgery and Neurotraumato− logy in the Efficient Therapy Division of J. Biziel Regional Hospital in Bydgoszcz, Poland. The examinations were conducted on 46 patients qual− ified for surgery for lumbar discopathy. Approval of the Bioethics Committee of the Collegium Medicum in Bydgoszcz to conduct this study was obtained.
The subjects were characterized regarding age, sex, place of residence, education, profession− al status, and the kind of job they were currently doing. Table 1 presents these data. In the examina− tions, the Repty Functional Index (RFI, in Polish: WFR) was used. The RFI/WFR was introduced by J. Opara et al. [13] at the Repty Silesian Rehabilitation Center in the Tarnowskie Mountains in 1998. It was created as a modifica− tion of American FIM (Functional Independence Measure) scale. The RFI, in contrast to the FIM, does not cover items connected with “social awareness” (interpersonal contacts, problem solv− ing, memory) because they do not subject to point opinion and belong more to the sphere of special psychological and sociological tests [12].
The RFI is a universal tool which can be suc− cessfully applied in assessing independence in var− ious neurological diseases as well as illnesses of the organ of movement, especially after cerebral injury or damage to the peripheral nervous system, diseases of the extrapyramidal system, muscle dis− eases, spinal pain, arthrosis, and after limb ampu− tation [13–15]. The examinations were carried out on the same patient twice: on the day before their operation as well as on leaving the ward, usually on the seventh day after surgery.
Results
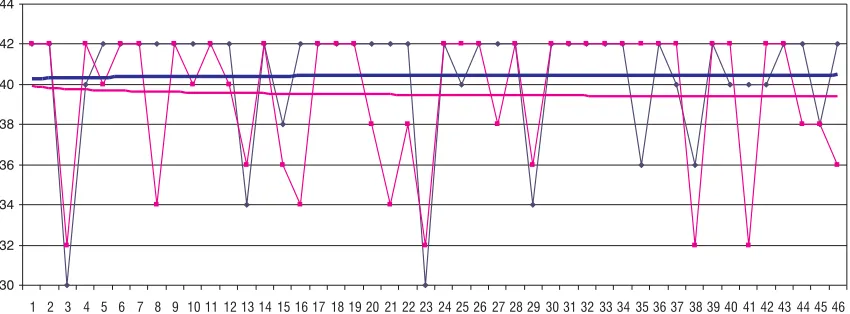
The examinations showed that the respondents were able to perform independently both before and after surgery. Their RFI scores ranged from
85–105 points (Table 2, Fig. 1). The mean ± SD
score before intervention was 101.3 ± 4.713 and after intervention 100.43 ± 5.868, which means that the functional assessment after the operation was a little worse, by 0.9 points (Table 3).
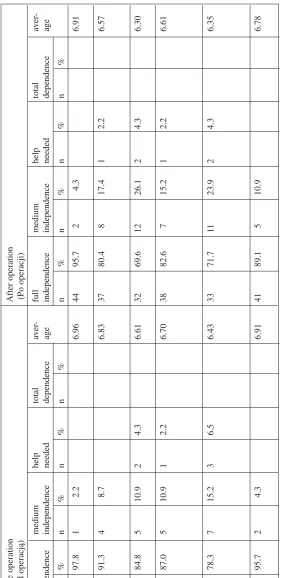
The different categories of the RFI scale were then subjected to analysis. For personal care, the first group of functional assessment, the values decreased from 40.43 to 39.52 points (Table 4, Fig. 2). This drop was visible in every determinant of the criterion, although it was most visible for care of appearance and personal hygiene (from 6.83 points before the operation to 6.57 points after). Consuming meals caused the least problem (drop of 0.05 points).
Examined feature Number of people examined %
(Badana cecha) (Liczba zbadanych pacjentów)
Age – years ≤40 18 39.1
(Wiek – lata) 41–50 16 34.8
> 50 12 26.1
total 46 100.00
Sex women 18 39.1
(Płeć) men 28 60.9
total 46 100.0
Education basic 0 0.0
(Wykształcenie) vocational 23 50.0
average 16 34.8
high 7 15.2
total 46 100.0
Place of residence – no. inhabitants village 14 30.4
(Miejsce zamieszkania – liczba town: ≤25,000 6 13.0
mieszkańców) town: 26,000–100,000 10 21.7
city: > 100,000 16 34.8
total 46 100.0
Job status student 0 0.0
(Status zawodowy) active professionally 32 69.6
pension/annuity 7 15.2
pension/annuity + active 2 4.3
unemployed 5 10.9
total 46 100.0
Kind of work physical labor 26 73.9
(Rodzaj pracy) mental labor 12 26.1
total 46 100.0
Table 1.Characteristics of the examined population
Tabela 1.Charakterystyka badanej populacji
RFI/WFR Score Before operation After operation (Ocena RFI/WFR) (Przed operacją) (Po operacji)
n % n %
85 0 0 2 4.3
87 1 2.2 0 0
89 2 4.3 1 2.2
91 0 0 2 4.3
93 1 2.2 3 6.5
95 2 4.3 4 8.7
97 3 6.5 0 0.0
99 3 6.5 4 8.7
101 7 15.2 4 8.7
103 9 19.6 5 10.9
105 18 39.1 21 45.7
Total 46 100.0 46 100.0
(Razem)
Table 2.Assessment of functional capacity according to the RFI scale
Tabela 2.Ocena wydolności funkcjonalnej badanych wg skali WFR
N Mean SD Min Max
(Średnia) (Min.) (Maks.) Before operation 46 101.30 4.713 87 105 (Przed operacją)
After operation 46 100.43 5.868 85 105 (Po operacji)
Table 3.Average total scores according to the RFI scale
RFI/WFR Before operation After operation (Przed operacją) (Po operacji) full medium help total aver − full medium help total aver − independence independence needed dependence age independence independence needed dependence age n% n % n % n % n % n % n % n % Having meals 45 97.8 1 2.2 6.96 44 95.7 2 4.3 6.91
(Przyrządzanie posiłków) Care of one’s appearance
42 91.3 4 8.7 6.83 37 80.4 8 17.4 1 2.2 6.57
and hygiene (Dbałość o wygląd i higienę) Bath
39 84.8 5 10.9 2 4.3 6.61 32 69.6 12 26.1 2 4.3 6.30
(Kąpiel) Getting dressed
40 87.0 5 10.9 1 2.2 6.70 38 82.6 7 15.2 1 2.2 6.61
– upper parts of the body (Ubieranie – górne części ciała) Getting dressed
36 78.3 7 15.2 3 6.5 6.43 33 71.7 1 1 23.9 2 4.3 6.35
– lower parts of the body (Ubieranie – dolne części ciała) Hygiene
44 95.7 2 4.3 6.91 41 89.1 5 10.9 6.78 (T oaleta) T able 4.
Assessment of functional capacity according to the RFI scale: personal care
T
a
bela 4.
Sphincter control is another category of func− tional assessment. In this criterion, urinating and defecating are taken into account. There was some improvement in both: urinating increased from 6.96 to 7.0 points and defecating from 6.91 to 7.0 points (Table 5, Fig. 3).
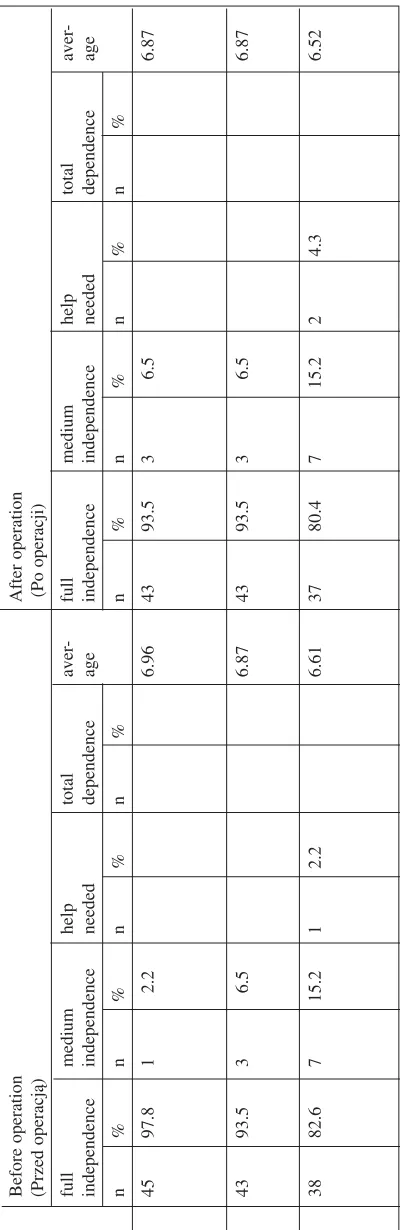
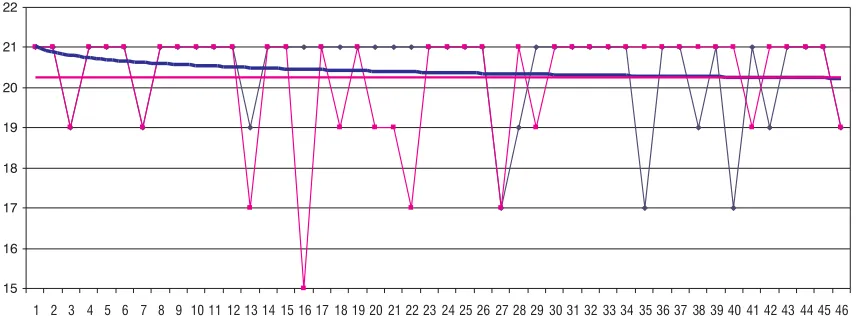
The third category of functional assessment was mobility. Here one can observe a general decrease from 20.43 points to 20.26 (Table 6, Fig. 4). The most frequent problem patients had in this regard was going under a shower or into a bathtub; one respondent (2.2%) required help in this action before intervention and two respondents (4.3%) after intervention.
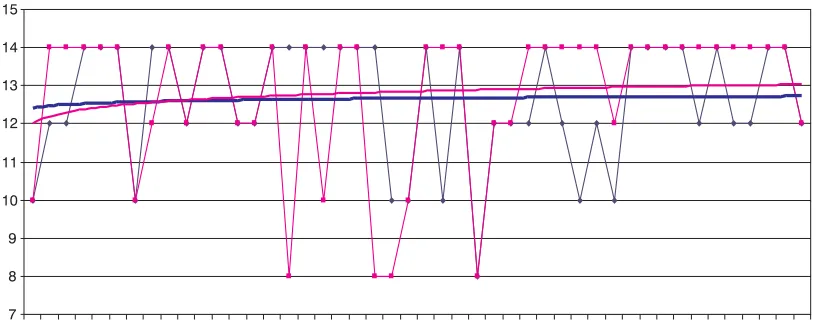
The results concerning locomotion show that the mean value for this category rose slightly after surgery, from 12.65 to 12.78 points (Table 7, Fig. 5). This category consists of two determinants: walk−
ing and using stairs. The first remained at an approximately steady level (6.61 points before surgery and 6.74 after) and the second stayed at the same level of 6.04 points. In fact, the number of people with full independence in walking stairs increased (from 26 to 30) and the number of peo− ple with moderate independence dropped (from 18 to 11), while two needed help before the operation and four afterwards. One person was classified as entirely dependent in this regard after the opera− tion.
Communication was the last analyzed catego− ry of functional assessment. The results show small differences: 97.8% of the respondents showed independent verbal speech as well as aural and visual understanding (Table 8, Fig. 6).
The statistical analysis demonstrated that the functional assessments before and after the applied
Fig. 1.General level of functional capacity according to the RFI scale
Ryc. 1.Poziom ogólny wydolności funkcjonalnej badanych wg skali WFR
30 32 34 36 38 40 42 44
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46
before treatment after treatment log (before treatment) log (after treatment)
Fig. 2.Level of functional capacity according to the RFI scale: personal care
Ryc. 2.Poziom wydolności funkcjonalnej badanych wg skali WFR – samoobsługa
30 32 34 36 38 40 42 44
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46
before treatment after treatment
RFI/WFR Before operation After operation (Przed operacją) (Po operacji) full medium help total aver − full medium help total aver − independence independence needed dependence age independence independence needed dependence age n% n % n % n % n % n % n % n % Urinating 4 5 97.8 1 2.2 6.96 46 100.0 7.00
(Oddawanie moczu) Defecating
44 95.7 2 4.3 6.91 46 100.0 7.00 (Oddawanie stolca) T able 5.
Assessment of functional capacity according to the RFI scale: sphincter control
T
a
bela 5.
Ocena wydolności funkcjonalnej badanych wg skali WFR – kontrola zwieraczy
RFI/WFR Before operation After operation (Przed operacją) (Po operacji) full medium help total aver − full medium help total aver − independence independence needed dependence age independence independence needed dependence age n% n % n % n % n % n % n % n %
Getting up from bed onto
45 97.8 1 2.2 6.96 43 93.5 3 6.5 6.87
a wheelchair (Wstawanie z łóżka na wózek) Sitting on a toilet bowl
43 93.5 3 6.5 6.87 43 93.5 3 6.5 6.87
(Siadanie na muszli klozetowej) Going under the shower
38 82.6 7 15.2 1 2.2 6.61 37 80.4 7 15.2 2 4.3 6.52
or into a bathtub (W
ejście pod prysznic
albo do wanny)
T
able 6.
Assessment of functional capacity according to scale the RFI: mobility
T
a
bela 6.
RFI/WFR Before operation After operation (Przed operacją) (Po operacji) full medium help total aver − full medium help total aver − independence independence needed dependence age independence independence needed dependence age n% n % n % n % n % n % n % n % W alking 37 80.4 9 19.6 6.61 40 87.0 6 13.0 6.74 (Chodzenie) Stairs 26 56.5 18 39.1 2 4.3 6.04 30 65.2 1 1 23.9 4 8.7 1 2.2 6.04
(Chodzenie po schodach)
T
able 7.
Assessment of functional capacity according to the RFI scale: locomotion
T
a
bela 7.
Ocena wydolności funkcjonalnej badanych wg skali WFR – lokomocja
RFI/WFR Before operation After operation (Przed operacją) (Po operacji) full medium help total aver − full medium help total aver − independence independence needed dependence age independence independence needed dependence age n% n % n % n % n % n % n % n %
Listening or V
isual 45 97.8 1 2.2 6.96 45 97.8 1 2.2 6.96
comprehensive (Rozumienie ze słuchu) Verbal speech
45 97.8 1 2.2 6.96 45 97.8 1 2.2 6.91 (Mowa) T able 8.
Assessment of functional capacity according to the RFI scale: communication
T
a
bela 8.
treatment were on the same level. This difference was not statistically significant (p > 0.05). This was related to the fact that some of the mean val− ues of the individual categories of the RFI increased while others decreased. However, the average assessments of the whole group before and after treatment were quite similar.
Discussion
Of the great number of spine ailments, the broadest and most known group constitutes disco− genic pain caused by pathology in the area of an intervertebral disc [16]. The pain, together with neurological disorders and loss of dexterity, is only a consequence. Spinal pain caused by a degenera− tive disease of an intervertebral disc is often found
in young and middle−aged people, who are the most agile and professionally active. It is a cause of decreased work efficiency, absence due to sick leave, and resignation from jobs which require physical involvement or extensive physical effort. It is also the reason for early retirement in many cases or for applying for a disability pension. It might result in discouragement, apathy, depres− sion, and even a nervous breakdown [9, 17, 18].
Surgery provides the possibility of treating spinal pain caused by degenerative disc disease: it interrupts the cascade of degenerative changes in the spine, reproduces the correct anatomical rela− tionships, and retains ability of movement [19, 20]. Current reports indicate significant improvement in health status after such intervention in 75–96% of cases, depending on the author [1, 9, 21, 22]. An essential problem is the quality of functioning with
Fig. 3.Level of functional capacity according to the RFI scale: sphincter control
Ryc. 3.Poziom wydolności funkcjonalnej badanych wg skali WFR – kontrola zwieraczy
10 10,5 11 11,5 12 12,5 13 13,5 14 14,5 15
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46
before treatment after treatment
log (before treatment) log (after treatment)
Fig. 4.Level of functional capacity according to the RFI scale: mobility
Ryc. 4.Poziom wydolności funkcjonalnej badanych wg skali WFR – mobilność
15 16 17 18 19 20 21 22
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46
before treatment after treatment
disc disease, as the restrictions imposed by the dis− ease relate to professional, social, cultural, as well as family life [3].
It seems that only surgery is an essential cor− relate of better functioning in those who under− went this sort of treatment. The complex and changeable clinical picture of those suffering from discopathy makes it difficult to form an objective and unambiguous opinion of the results of treat− ment. Patients referred for surgery show more pathological neurological symptoms than those who continue conservative treatment. The indica− tors of improvement directly after surgery are greater than in a corresponding period of conserv− ative treatment. Total retreat of neurological deficits more often involves patients who have been operated [9, 23]. Of the factors which influ−
ence the functional assessment of patients with discopathy, one should mention at least three main components of the disease: the pain, the degree of disability, and the deficiency symptoms.
The above examinations showed that the patients generally demonstrated full independence both before and after intervention, but that after the neurosurgical operation this independence was slightly less. After intervention, improvement in efficiency was observed in sphincter control and walking ability. However, there were decreases in the indicators of personal care activities and mobility, although these differences were not sta− tistically significant. On the other hand, according to Frost [24], the index of functional efficiency after surgery, i.e. on leaving the hospital, obtained using the same examination tool, improved from
Fig. 5.Level of functional capacity according to the RFI scale: locomotion
Ryc. 5.Poziom wydolności funkcjonalnej badanych wg skali WFR – lokomocja
7 8 9 10 11 12 13 14 15
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46
before treatment after treatment log (before treatment) log(after treatment)
Fig. 6.Level of functional capacity according to the RFI scale: communication
Ryc. 6.Poziom wydolności funkcjonalnej badanych wg skali WFR – komunikacja
8 9 10 11 12 13 14 15
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46
80.9 points (partial dependence before surgery) to 95.2 points (independence after surgery). Different authors’ case studies [25, 26] also show that patients who underwent a neurosurgical operation revealed improvement in functional efficiency on leaving the hospital ward. A review of the litera− ture also permits the conclusion that most patients present a very high degree of functional inefficien− cy before surgery [26, 27].
The assessment of patients’ functional effi− ciency with disc disease is one of the criteria applied in evaluating treatment results. It is essen−
tial mainly because it adequately predicts the chances of returning to work; a limitation of one’s own activity is a factor in one’s inability to work [11]. Last but not least, it seems one is able to conduct the assessment after treatment.
The authors concluded that patients with lum− bar discopathy show full independence in terms of executing the activities of everyday day. The func− tional assessment of those who were examined was a little worse after surgery, i.e. on leaving the hospital ward.
References
[1] Milecki M, Łukowski S, Rąpała K, Białecki J:Wyniki leczenia choroby dyskowej usztywnieniem międzytrzo−
nowym z dostępu tylnego za pomocą koszyków metalowych. Ortop Traumatol Rehabil 2004, 6, 3, 277–281.
[2] Bazan M:Bólowe zespoły kręgosłupowo−korzeniowe dolnego odcinka kręgosłupa. Skalpel 2006, 3, 24–26.
[3] Lisiński P, Jachowska A, Samborski W:Metody fizjoterapeutyczne w leczeniu wysunięć krążka międzykrę−
gowego w odcinku lędźwiowym kręgosłupa. Fizot Pol 2006, 3, 4, 6, 222–227.
[4] Luoma K, Riihimaki H, Luukkonen R, Raininko R, Vlikari−Juntura E, Lamminen A:Low back pain in rela−
tion to lumbar disc degeneration. Spine 2000, 25, 4, 487–492.
[5] Brzezicki G, Gaca M, Jankowski R:Obraz dyskopatii lędźwiowo−krzyżowej w badaniu rezonansu magnety−
cznego u chorych leczonych operacyjnie. Neuroskop 2003, 1, 5, 51–54.
[6] Dziak A:Bóle i dysfunkcje kręgosłupa. Med Sport, Kraków 2007, ed 1, 655–988.
[7] Księżopolska−Orłowska K:Przydatność krioterapii w kompleksowym postępowaniu usprawniającym chorych
na dyskopatię lędźwiową. Rozprawa habilitacyjna. Studio AWP, Warszawa 2004, 1 ed, 12–28.
[8] Wordliczek J, Dobrogowski J: Medycyna bólu. Prz Piśmien Chir 2006, 13, 8–14.
[9] Radziszewski RK:Analiza porównawcza stanu neurologicznego chorych na dyskopatię kręgosłupa lędźwiowego
leczonych zachowawczo lub operacyjnie. Pol Merk Lek 2007, 22, 129, 186–191.
[10] Bełdziński P, Dzierżanowski J, Słoniewski P:Minimalne inwazyjne techniki chirurgicznego leczenia choroby
dyskowej kręgosłupa lędźwiowego. Ortop Traumatol Rehabil 2004, 6, 3, 308–313.
[11] Rycerski W, Opara J, Berezowski K: Przydatność oceny czynności życia codziennego do przewidywania
powrotów do pracy osób poddanych rehabilitacji z powodu dyskopatii lędźwiowej. Ortop Traumatol Rehabil 2002, 4, 1, 69–74.
[12] Karabanowicz A, Panas A, Ślusarz R, Beuth R, Grzelak L, Szrajda J: Ocena sprawności funkcjonalnej
w chorobach układu nerwowego. Ann UMSC 2005 Sect D 2005, 60, supl 16, 190, 352–353.
[13] Opara J, Szeliga−Cetnarska M, Chromy M, Dmytyk J, Ickowicz T: Skale Udarów „Repty”. Wskaźnik
funkcjonalny „Repty” dla oceny czynności życia codziennego u chorych z niedowładem połowiczym po udarze mózgowym. Część II. Neurol Neurochir Pol 1998, 4, 803–812.
[14] Opara J:Analiza przydatności wybranych skal udarów do oceny wyników rehabilitacji chorych z niedowładem
połowiczym. Rozprawa habilitacyjna. ŚAM w Katowicach, Katowice 1996, ed 1, 18–22.
[15] Niedziałek D:Zespoły bólowe kręgosłupa. Essent Med 2005, 3, 66.
[16] Nowakowski A, Cabaj M, Kubaszewski Ł:Endoprotezoplastyka krążka międzykręgowego w części lędźwiowej
kręgosłupa – doświadczenia wstępne. Neuroskop 2003, 1, 5, 58–61.
[17] Zarzycki D, Kaliciński M, Bakalarek B, Winiarski A, Radło P, Rymarczyk A, Sebastianowicz: Zabiegi
endoskopowe w chirurgii kręgosłupa. Ortop Traumatol Rehabil 2005, 7, 3, 295–301.
[18] Saran T:Przyczyny zespołów bólowych odcinka lędźwiowo−krzyżowego kręgosłupa i współczesne metody ich
leczenia. Med Ogólna 2005, 11, 40, 3, 178–185.
[19] Milecki M, Łukowski S, Rąpała K, Białecki J:Wyniki leczenia choroby dyskowej usztywnieniem międzytrzo−
nowym z dostępu tylnego za pomocą koszyków metalowych. Ortop Traumatol Rehabil 2004, 6, 3, 277–281.
[20] Kamieniak P, Janusz W, Trojanowski T:Dolegliwości bólowe po usunięciu dysku lędźwiowego. An UMCS
Sect D 2005, 60, supl 16, 7, 75–78.
[21] Radek A, Zapałowicz K:Choroba krążków międzykręgowych lędźwiowego odcinka kręgosłupa. Valetudinaria
– Post Med Klin Wojsk 2001, 6, 1–2, 40–44.
[22] Glinkowski W, Ciszek B:Wybrane zagadnienia morfologii i właściwości krążków międzykręgowych (część I).
Ortop Traumatol Rehabil 2004, 6, 2, 141–148.
[23] Żelazny S:Zespoły bólowe neurologiczne kręgosłupa i rdzenia jako problem społeczny. Med Rodz 2001, 4, 1,
10–11.
[24] Frost K: Ocena funkcjonalna chorych ze schorzeniami kręgosłupa. Praca magisterska. Collegium Medicum
w Bydgoszczy, UMK w Toruniu, Toruń 2006, 63–86.
[25] Czapiga B, Horanin M, Jarmundowicz W, Mierzwa J, Rosińczuk−Tonderys J, Weiner A:Subiektywna ocena
[26] Ostrowska M:Wybrane aspekty jakości życia pacjentów z dyskopatią. [W:] Krajewska−Kułak E, Szczepański M, Łukaszuk C, Lewko J (red.): Problemy terapeutyczno−pielęgnacyjne: od poczęcia do starości, Białystok 2007, wyd. 1, tom II, 95–101.
[27] Sierpowska A, Cywińska−Wasilewska G, Warzecha D: Ocena sprawności funkcjonalnej chorych z krę−
gozmykiem. Postępy Rehabil 2006, 2, 11–15.
Address for correspondence:
Renata JabłońskaDepartment of Neurological and Neurosurgical Nursing Techników 3
85−801 Bydgoszcz Poland
Tel.: +48 52 585 21 93 E−mail: [email protected]
Conflict of interest: None declared