A
GNIESZKAC
ISOWSKA1, D
OROTAT
ICHACZEK−G
OSKA1, A
NNAS
ZOZDA2, E
WAL
EWCZYK2,
M
ARLENAK
ŁAK1The Bactericidal Activity of Complement
in Sera of Children with Infectious Hyperbilirubinemia
Bakteriobójcza aktywność dopełniacza surowicy u dzieci
chorych na żółtaczkę zakaźną
1Department of Biology and Medical Parasitology, Silesian Piasts University of Medicine in Wrocław, Poland 2J. Korczak Lower Silesian Pediatrics Center in Wrocław, Poland
Adv Clin Exp Med 2007, 16, 5, 629–634 ISSN 1230−025X
ORIGINAL PAPERS
© Copyright by Silesian Piasts University of Medicine in Wrocław
Abstract
Background. Jaundice is a frequently encountered problem during the neonatal period. Some reports have suggest− ed that unexplained hyperbilirubinemia may be associated with bacterial infections in infants. It has been suggested that the bactericidal action of sera of neonates with hyperbilirubinemia is lower than that of healthy children. The mechanism by which bilirubin interferes with serum is still not entirely understood and requires continual study.
Objectives.The aim of this study was to establish if hyperbilirubinemia in neonates with various infections is asso− ciated with decreased bactericidal activity of their sera and complement level.
Material and Methods. Normal human serum (NHS) samples obtained from 58 children with hyperbilirubinemia were used. Each infant suffered from a non−viral infection and developed jaundice. Normal cord serum (NCS) sam− ples obtained from 35 healthy newborns were used as controls. The susceptibility of the E. coli529 K1 strain to the bactericidal action of NHS and NCS as well as total hemolytic complement activity were determined and compared.
Results.The E. coli529 K1 strain showed variable sensitivity to the bactericidal action of NHS and NCS.
Conclusions. The percentages of surviving E. coli529 K1 in NHS and NCS were similar. There was no correla− tion between complement and bilirubin levels in NHS. The complement and bilirubin levels did not show a direct influence on the bactericidal activity of the sera (Adv Clin Exp Med 2007, 16, 5, 629–624).
Key words: bactericidal activity of serum, complement, hyperbilirubinemia, jaundice, E. coli.
Streszczenie
Wprowadzenie.Żółtaczki są dużym problemem wieku noworodkowego. Wykazano, że hiperbilirubinemia o nie− wyjaśnionej przyczynie może być związana z zakażeniami bakteryjnymi. Sugeruje się, że surowica noworodków, u których obserwuje się hiperbilirubinemię wykazuje zmniejszoną aktywność bakteriobójczą wobec bakterii Gram−ujemnych w porównaniu z aktywnością surowicy dzieci zdrowych. Mechanizm oddziaływania bilirubiny z surowicą nie został jednak dotychczas w pełni poznany i wymaga dalszych badań.
Cel pracy.Ustalenie, czy żółtaczki zakaźne noworodków są związane ze zmniejszoną bakteriobójczą aktywnością surowicy oraz zmniejszeniem hemolitycznej aktywności dopełniacza.
Materiał i metody. W badaniach wykorzystano surowicę od 58 dzieci z hiperbilirubinemią. Wszystkie dzieci cier− piały z powodu niewirusowych zakażeń, w przebiegu których rozwinęła się żółtaczka. Jako materiału kontrolnego użyto surowicy pępowinowej pochodzącej od 35 zdrowych noworodków. Określono i porównano stężenie dopeł− niacza oraz bakteriobójczą aktywność surowicy w obu badanych grupach.
Wyniki.Szczep E. coli529 K1 wykazał zróżnicowaną podatność wobec surowicy dzieci z hiperbilirubinemią i su− rowicy pępowinowej.
Wnioski. Przeżywalność szczepu E. coli529 K1 w surowicy dzieci z hiperbilirubinemią i surowicy pępowinowej była podobna. Nie zaobserwowano korelacji między dużym stężeniem bilirubiny a zmniejszeniem hemolitycznej aktywności dopełniacza w surowicy dzieci chorych. Nie wykazano również bezpośredniego wpływu dopełniacza i bilirubiny na bakteriobójczość tych surowic (Adv Clin Exp Med 2007, 16, 5, 629–624).
Jaundice is a frequently encountered problem during the neonatal period. Although up to 60% of term newborns have clinical jaundice in the first week of life, few have a significant underlying dis− ease [1]. Jaundice can be associated with severe illnesses such as hemolytic disease, metabolic and endocrine disorders, enzymatic deficiencies of the liver, and infections. Some reports have suggested that unexplained hyperbilirubinemia may be asso− ciated with bacterial infections in newborn and infants [2, 3]. Bacteremia and sepsis have been well documented as a cause of neonatal jaundice in seriously ill newborns in whom jaundice was the primary presenting sign [4]. Authors have con− cluded that bacterial infections should be consid− ered a possible cause of neonatal unconjugated hyperbilirubinemia during the first week of life, regardless of the physical condition of the infant. Urinary tract infections (UTI) are considered a cause of prolonged jaundice [1]. It is well known that the clinical manifestations of UTI can cover a wide spectrum, ranging from severe illness to unspecific signs and symptoms such as growth problems, diarrhea, fever, vomiting, abnormal uri− nation, and jaundice [5].
It has been suggested that the bactericidal action of the serum of neonates with hyperbilirubinemia is lower than that of healthy newborns and infants [6]. This could presumably be a result of the toxic effects of bilirubin on cells responsible for the synthesis of complement proteins or its direct reaction with the proteins of the serum’s bactericidal system. The aim of this study was to establish if hyperbilirubinemia in neonates who suffered from various infections is associated with decreased bactericidal activity of their serum and complement level.
Material and Methods
Sera
Normal human serum (NHS) samples ob− tained from the remains of blood used in routine diagnostics from 58 children with hyperbilirubine− mia of both sexes who had not been treated with any antimicrobial drugs were used. The children were hospitalized in the J. Korczak Lower Silesian Pediatrics Center in Wrocław in 2005–2006. Each infant suffered from an infection and developed jaundice, most probably in the course of or conse− quent to that infection. No cases were encountered in which jaundice could be attributed to a viral infection. The infants were assessed hematologi− cally by routine techniques. Normal cord serum (NCS) samples obtained from 35 healthy new− borns whose mothers were not previously treated
with antibiotics were used as controls. The NHS and NCS samples were collected and kept frozen in 0.5 ml portions at –70°C. A suitable volume of the serum was thawed immediately before experi-ments and used only once.
Total hemolytic complement activity of NHS and NCS was measured by the method described by Wedgwood and Janeway [7]. The titer of com− plement activity was expressed as the reciprocal of the dilution which lysed 50% of a standardized suspension of sheep red blood cells previously sensitized by rabbit antibodies (CH50 units).
Bacterial Strain
The Escherichia coli 529 K1 strain from the collection of the Department of Biology and Medical Parasitology of Silesian Piasts University of Medicine was used. The strain was isolated from the urine of a child with a UTI and identified by the API 20 E test.
Bactericidal Activity of Serum
The bactericidal activity of NHS and NCS was determined as described previously [8]. Briefly, the strain was grown overnight and then bacterial cells of the early exponential growth phase were transferred to fresh nutrient broth and incubated at 37°C for 0.5 h. After incubation, the bacterial cells were centrifuged (4 000 rpm for 20 min). The bac-teria were then added to 7.5% NHS or NCS (the sera were diluted with 0.1 M NaCl). Bacteria with sera were incubated in a water bath at 37°C. After 0, 60, and 180 min the samples were collected, diluted, and cultured on nutrient agar plates for 18 h at 37°C. The number of colony-forming units (c.f.u.) at time 0 was taken as 100%. If the survival ratio of the E. coli529 K1 strain after 180 min of incubation in the serum was less than 90%, 90–110%, and higher than 110%, the serum had bactericidal, bacteriostatic, and non-bactericidal activities, respectively.
Results
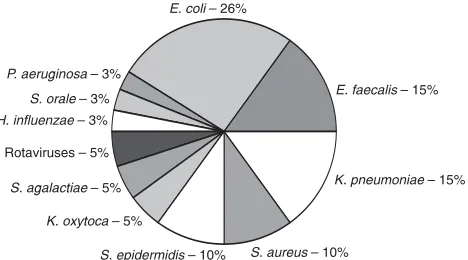
pharyngitis (29), UTI (14), and umbilicus inflam− mation (8) were common. Gastroenteritis, pneu− monia, bacteremia, and conjunctivitis were rare. Some infants had more than one infection. Frequently, otitis media with rhinitis and pharyn− gitis occurred together with UTI (8 cases) or with umbilicus inflammation (4). Pathogenic organisms (39 strains) were isolated from samples of urine, stool, blood, and pharyngeal, nasal, conjunctival, and umbilical swabs. E. coli, Enterococcus fae− calis, andKlebsiella pneumoniaewere the organ− isms most commonly isolated (Fig. 1).
The white blood counts ranged from 7,640 to 23,710 per cubic millimeter with a mean of 12,830. The C−reactive protein (CRP) level did not diverge from the norm in most patients. Only in three cases was the CRP level higher: 61.0 mg/l and 11.3 mg/l (intrauterine infections), and 55.0 mg/l (pneumonia).
The susceptibility of E. coli529 K1 to the bac− tericidal action of the NHS obtained from the chil− dren with infectious hyperbilirubinemia and the NCS from the healthy newborns was determined. The strain showed variable sensitivity to the bac− tericidal action of NHS and NCS. Non−bacterici− dal activity in 12 (20.7%), bacteriostatic activity in 1 (1.7%), and bactericidal activity in 45 (77.6%) were detected among the 58 samples of NHS. In the healthy control group, bactericidal activity in 26 (74.3%) and non−bactericidal activity in 9 (25.7%) of the 35 NCS samples were observed.
Total hemolytic complement activity (expressed as CH50 units) in the NHS which demonstrated
bactericidal activity against E. coli 529 K1 strain was never lower than 20.0 U/ml and oscillated between 20.0 U/ml and 85.7 U/ml. In addition, the complement level in 26.7% of the samples was
≥50.0 U/ml. The bilirubin level in this group of serum samples varied from 4.0 mg/dl to 16.5 mg/dl. Bilirubin levels higher than 12.5 mg/dl were observed in only 31.1% of these samples. In the case of NHS with non−bactericidal activity, 66.7% had complement levels lower than 20.0 U/ml. Furthermore, it was found that the complement level among the rest of these serum samples oscil−
lated between 20.0 U/ml and 47.6 U/ml. In as many as 58.3% of the samples the bilirubin level was higher than 12.5 mg/dl. The serum samples with bacteriostatic activity had a rather low lev− els of complement and bilirubin (20.0 U/ml and 5.66 mg/dl, respectively).
Total hemolytic complement activity in the NCS which showed bactericidal activity against
E. coli529 K1 was also never lower than 20.0 U/ml, and 34.6% of the samples had ≥50.0 U/ml. In the group of NCS with non−bactericidal activity, 77.8% had complement levels lower than 50.0 U/ml.
These experiments showed that the percent− ages of surviving E. coli529 K1 in NHS and NCS were similar. Moreover, the complement and bilirubin levels did not reveal any direct influence on the bactericidal activity of these serum samples (Fig. 2–3). However, in the control group only 3 and among the NHS samples as many as 12 had com− plement levels ≥20.0 U/ml. In addition, there was no correlation between the complement and biliru− bin levels in the NHS samples obtained from the children with infectious hyperbilirubinemia (Fig. 4).
Discussion
Bacterial infection is a recognized cause of hyperbilirubinemia in newborns, and some reports suggest that unexplained indirect hyperbilirubine− mia may be the only manifestation of bacteremia or incipient sepsis in otherwise healthy newborns [4, 9]. In contrast to these data, Maisels and Kring stated that if indirect hyperbilirubinemia is ever the only sign of bacteremia and incipient sepsis, it must be a rare event indeed [10]. Attention has also been directed to the relationship between UTI and the development of jaundice in young infants [5]. Authors observed that the incidence of UTI in asymptomatic, afebrile jaundiced infants is similar to the incidence of UTI in febrile infants. Jaundice may thus be the first sign of UTI in asymptomatic patients before other signs and symptoms become evident. Therefore it has been suggested that testing for UTI should be part of the
S. epidermidis– 10%
K. oxytoca– 5%
S. agalactiae– 5% Rotaviruses – 5%
H. influenzae– 3%
S. orale– 3%
P. aeruginosa– 3%
E. coli– 26%
E. faecalis– 15%
K. pneumoniae– 15%
S. aureus– 10%
Fig. 1. Pathogenic organisms isolated from children with hyperbilirubinemia
diagnostic evaluation of asymptomatic jaundiced infants. According to the results of the present study and other authors’ data [11], infectious hyperbilirubinemia is often related to UTI.
Because the immunity of human neonates to Gram−negative bacteria, including E. coli K1, is decreased, which results in a higher incidence of infections such as septicemia, meningitis, and
−4.00 −3.00 −2.00 −1.00 0.00 1.00 2.00 3.00 4.00 5.00
0 10 20 30 40 50 60 70 80 90 100 110
complement level [CH stężenie dopełniacza [CH
H ] H ]
50 50
% of survival [log] % przeżywalności [log]
Fig. 2.The relationship between the survival of E. coli529 K1 and complement levels in: a) NHS from children with hyperbilirubinemia, b) NCS from healthy newborns
Ryc. 2. Zależność między przeżywalnością szczepu E. coli529 K1 a poziomem dopełniacza: a) w surowicy dzieci z hiperbilirubinemią, b) w surowicy pępowinowej
−4.00 −3.00 −2.00 −1.00 0.00 1.00 2.00 3.00 4.00 5.00
0 10 20 30 40 50 60 70 80 90 100 110
complement level [CHH ] stężenie dopełniacza [CHH ]
50 50
% of survival [log] % przeżywalności [log]
a)
−4.00 −3.00 −2.00 −1.00 0.00 1.00 2.00 3.00 4.00 5.00
0 5 10 15 20 25
% of survival [log] % przeżywalności [log]
bilirubin level stężenie bilirubiny
(mg/dl)
Fig. 3. The relationship between E. coli529 K1 survival and bilirubin levels in NHS from children with hyperbiliru− binemia
Ryc. 3. Zależność między przeżywalnością szczepu E. coli529 K1 a stężeniem bilirubiny w surowicy dzieci z hiper− bilirubinemią
0 10 20 30 40 50 60 70 80 90
0 5 10 15 20 25
bilirubin level stężenie bilirubiny complement level [CH ]
poziom dopełniacza [C
50
H ]50
(mg/dl)
Fig. 4. The relationship between complement and bilirubin levels in NHS from children with hyperbilirubinemia
References
[1] Bilgen H, Özek E, Ünver T, Biyikli N, Alpay H, Cebeci D: Urinary tract infection and hyperbilirubinemia. Turk J Pediatr 2006, 48, 51–55.
[2] Escobedo MB, Barton LL, Marshall RE, Zarkowsky H:The frequency of jaundice in neonatal bacterial infec− tions. Clin Pediatr 1974, 13, 656–657.
[3] Ng SH, Rawstrong JR:Urinary tract infections presenting with jaundice. Arch Dis Child 1971, 46, 173–176.
[4] Linder N, Yatsiv I, Tsur M, Matoth I, Mandelberg A, Hoffman B, Yevin R, Tamir I: Unexplained neonatal jaundice as an early diagnostic sign of septicemia in the newborn. J Perinatol 1988, 8, 325–327.
[5] Garcia FJ, Nager AL:Jaundice as an early diagnostic sign of urinary tract infection in infancy. Pediatrics 2002, 109, 846–851.
[6] Miler I, Vondráček J, Hromádková L:The bactericidal activity of sera of healthy neonates and of newborns with hyperbilirubinemia to Escherichia coli. Folia Microbiol 1979, 24, 143–152.
[7] Wedgwood RJP, Janeway CA:Serum complement in children with “collagen diseases”. Pediatrics 1953, 11, 569–581.
[8] Cisowska A, Bugla−Płoskońska G, Tichaczek−Goska D, Doroszkiewicz W, Jankowski S:The susceptibility of
Escherichia colistrains with sialic acid−containing lipopolysaccharides or capsules to the bactericidal action of normal human serum. VII Konferencja „Biologia molekularna w diagnostyce chorób zakaźnych i biotechnologii”. Warszawa, 4 grudnia 2004. Materiały naukowe; SGGW Warszawa, 2004, 41–47.
[9] Rooney JC, Hill DJ, Danks DM: Jaundice associated with bacterial infection in the newborn. Am J Dis Child 1971, 122, 39–41.
[10] Maisels MJ, Kring E: Risk of sepsis in newborns with severe hyperbilirubinemia. Pediatrics 1992, 90, 741–743.
[11] Dudek R: Hiperbilirubinemia noworodków w materiale własnym Kliniki Patologii Noworodka. Nowa Pediatria 1999, 5, 22–24.
[12] Feigin RD, McCracken GH, Klein JO:Diagnosis and management of meningitis. Pediatr Infect Dis J 1992, 11, 785–814.
[13] Johnson JR:Virulence factors in Escherichia coliurinary tract infection. Clin Microbiol Rev 1991, 4, 80–128.
[14] Basiewicz−Worsztynowicz B, Nienartowicz B, Saraczyńska E, Rybska K, Jankowski A, Jankowska A:
Spontaniczna bakteriobójcza aktywność surowicy u dzieci z przewlekłym zapaleniem wątroby. Adv Clin Exp Med 2001, 10, 25–30.
[15] Ferrante A, Thong YH: Inhibition of serum bactericidal activity by bilirubin. Immunol Lett 1982, 4, 103–105.
Address for correspondence:
Agnieszka Cisowska
Department of Biology and Medical Parasitology Silesian Piasts University of Medicine
Mikulicza−Radeckiego 9 50−367 Wrocław Poland
Tel.: +48 071 784 15 20
E−mail: [email protected]
pyelonephritis at this age [12, 13], the present study investigated the bactericidal activity of NHS of infants with infectious hyperbilirubinemia on the E. coli K1 strain. It has been established that the spontaneous bactericidal activity of the sera of children with chronic hepatitis B is significantly diminished compared with that of healthy controls [14]. A statistically significant decline in hemolyt− ic complement activity in the sera of HBV−infect− ed children was also observed. In addition, Miler et al. [6] found decreased bactericidal activity in the sera of jaundiced infants in contrast to healthy newborns and hence it was postulated that jaun− diced newborns may be more susceptible to vari− ous infections than normal neonates. The authors suggested that the diminished bactericidal action of the serum might be attributed to a functional defect in the complement system. They assumed that the low bactericidal activity of sera of children
with hyperbilirubinemia can be possibly explained either by an increased in vivo consumption of complement due to intravascular hemolysis or by a toxic effect of bilirubin on cells synthesizing complement proteins. In the present experiments, a decreased bactericidal activity of sera of jaun− diced infants compared with healthy newborns was not observed. Additionally, the presented data demonstrated that a high bilirubin level did not correlate with decreased complement level and, consequently, diminished bactericidal action of serum. The experimental data presented by Ferrante and Thong [15] showed that the addition of various amounts of bilirubin alters the bacteri− cidal activity of human serum. This was probably due to the direct effect of bilirubin on complement activation. The mechanism by which bilirubin interferes with serum is still not fully understood and requires further study.
Conflict of interest: None declared