*Corresponding author: Morchad Bouabid
Department of Fixed Prosthodontics. Faculty of Dentistry
Current Multidisciplinary Studies
Available Online atVol.
WHEN TO REMOVE TRADITIONAL FIXED PROSTHESES?
Department of Fixed Prosthodontics.
A R T I C L E I N F O
Received 10th May, 2019 Received in revised form 2nd June, 2019
Accepted 26th July, 2019
Published online 28th August, 2019
Keywords:
Fixed prosthesis– traditional -remove- causes.
INTRODUCTION
According to WHLIE BENBERG, removal is a "challenge that allows to judge the intelligence, ingenuity and capacity of the practitioner, a challenge made even more difficult by the improvement of cast techniques"[1].
There is no certainty regarding the longevity of fixed prosthetic treatments, but the clinical studies (SCURR IA
subject reasonably agree on an average lifespan of about 10 to 15 years. Indications of re-operation are unfortunately too numerous. They are often the cause of a loss of confidence of the patient vis-à-vis his practitioner, a significant sour stress for the latter and represent a significant financial cost for both. The practitioner must always explain to his patient, that fixed prosthesis does not mean definitive prosthesis (fig. 1,2).
Fig 1 Panoramic X-ray: important bone resorption with mediocre prosthetic
design.
Copyright © 2019 Morchad Bouabid., This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted
use, distribution, and reproduction in any medium, prov
Morchad Bouabid
Department of Fixed Prosthodontics. Faculty of Dentistry Rabat, Morocco
International Journal of
Current Multidisciplinary Studies
Available Online at http://www.journalijcms.comVol. 5, Issue,08(A), pp.1050-1055,August,2019
RESEARCH ARTICLE
WHEN TO REMOVE TRADITIONAL FIXED PROSTHESES?
Morchad Bouabid
Department of Fixed Prosthodontics. Faculty of Dentistry Rabat, Morocco
A B S T R A C T
The evolution of fixed prosthesis production techniques makes it possible today to obtain prostheses that are too often considered as "definitive" because of a great deal of aesthetic and functional precision .However, despite the respect of the various stages
no practitioner can claim to be safe from prosthetic failure. This is valid regardless of his experience, his rigor or his skill.
These risks can be prosthetic origin periodontal, endodontic, aesthetic or functional.
According to WHLIE BENBERG, removal is a "challenge that the intelligence, ingenuity and capacity of the practitioner, a challenge made even more difficult by the
There is no certainty regarding the longevity of fixed prosthetic treatments, but the clinical studies (SCURR IA [2]) on the subject reasonably agree on an average lifespan of about 10 to operation are unfortunately too numerous. They are often the cause of a loss of confidence of vis his practitioner, a significant source of stress for the latter and represent a significant financial cost for both. The practitioner must always explain to his patient, that fixed prosthesis does not mean definitive prosthesis (fig. 1,2).
n with mediocre prosthetic
Fig 2 Removal of the mandibular bridge with extraction of the abutment teeth
without effort.
In this article we will review the causes of the following nature:
General;
Periodontal and prosthetic;
Endodontic and Dental;
Esthetics.
General etiology[3,4]
Some patients require, for medical reasons, exploratory examinations such as magnetic resonance imaging (MRI) or a computed tomography (CT).
The presence of alloy used in the composition of certain prosthetic elements generates artefacts and justifies the need to remove them. Also, the use of certain metals (nickel, chromium)
This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
WHEN TO REMOVE TRADITIONAL FIXED PROSTHESES?
Faculty of Dentistry Rabat, Morocco
evolution of fixed prosthesis production techniques makes it possible today to obtain prostheses that are too often considered as "definitive" because of a great deal of aesthetic and functional precision .However, despite the respect of the various stages of development, no practitioner can claim to be safe from prosthetic failure. This is valid regardless of his
These risks can be prosthetic origin periodontal, endodontic, aesthetic or functional.
Removal of the mandibular bridge with extraction of the abutment teeth without effort.
In this article we will review the causes of the following nature:
Periodontal and prosthetic; Dental;
Some patients require, for medical reasons, exploratory examinations such as magnetic resonance imaging (MRI) or a
The presence of alloy used in the composition of certain prosthetic elements generates artefacts and justifies the need to remove them. Also, the use of certain metals (nickel, chromium)
IJCMS
in sensitive subjects, causes the emergence of allergic reactions which force the disassembly of the elements involved (fig.3).
Fig 3 Allergic reaction due to metal diffusion in periodontal tissues.
In addition, the presence of several metals, of different nature and with a large potential difference, creates ionic fluxes that cause galvanic micro-currents at the origin of metalloses or intolerances.
And finally, the aging of the population, the awareness of the importance of dental care and the evolution of techniques make the recurrence of doing a fixed prothesis of a dent not uncommon during one’s lifespan.
Periodontal and prosthetic Etiology
A perfect knowledge of the clinical aspect of a pathological periodontium (color, mobility, gingival recessions, periodontal pockets ...) completed by a radiological examination (bone resorption, biological space ...) allows to unseal a possible disease and therefore to consider the removal [5].
Failures related to a diagnostic error
Most of the prosthetic failures considered from the periodontal angle are due to misdiagnosis. They are generally related (fig.4,5):
Fig 4 Restoration of the incisial-canine block by ceramic-ceramic crowns...
Fig 5 : ... Result 2 years later; it is a misdiagnosis (bad oral hygiene).
Either to a bad analysis of the motivation of the patient;
Or a poor periodontal evaluation (pathology of periodontal support tissues) and / or occlusal (traumatic occlusion) pre-prosthetic;
Or in connection with a misinterpretation of the radiological image;
Or in connection with a wrong prosthetic realization.
Failures related to an error during prosthetic treatment may be related to
The dental preparation
The periodontal integration of the prosthetic elements depends on the presence of a biological space and the quality of the mucogingival tissues [6].
Its aggression leads to a chronic attack, with apical migration of the marginal gingiva and serious aesthetic consequences (fig.6).
Fig 6 Root denudation due to overcontouring and excessive brushing.
Morchad Bouabid IJCMS, 2019; Vol. 5(8): 1050-1055.
Clinical trials: (fig.7,8)
Fig 7 Multiple dental preparations for receiving metal-ceramic restorations.
Fig 8 When trying the restoration; the gingiva should not appear whitish.
During fitting, the gingiva must retain its color, if it whitens then too much support has taken place in the cervical region. Respect of the papillae is allowed by open embrasures, allowing good access to hygiene by the patient.
Overly closed embrasures cause compression of the papillae, with inflammation that will become chronic, jeopardizing periodontal health [10].
The occlusal function
Occlusal trauma has been the subject of numerous studies in the development of periodontal problems, all of which conclude that it is responsible either for a healthy periodontal period or with a particular pathology, hence the importance of occlusion adjustment (fig.9) [11,12]
The quality of the occlusal integration of a prosthetic element is essential for its durability (fig.10,11).
Failure to respect the occlusal morphology (over-occlusion, sub-occlusion, erroneous triturating anatomy, etc.) causes a shift in the intermaxillary ratios with a repercussion on the articular and muscular structures.
Prematurities and interferences cannot be eliminated by simple coronoplasty, they will be corrected by realizing new prostheses.
Fig 9 Ceramic's fracture due to an occlusal disorder.
Fig 10 Bridge's fracture at the connection ...
Fig 11 Due to reduced usable occlusal height, note the reddish appearance next
to the pontic.
Endodontic and dental etiologies [9,13]: Endodontic pathologies
The preservation of pulp vitality should always be preferred, for reasons of strength and as a warning signal.
This, the realization of crowns on living teeth is an act requiring a great thoroughness in its elaboration.
Failure to comply with certain principles (new dental drills, under irrigation, intermittence) leads to a "dentin wound" that can go as far as necrosis (fig.12,13).
Fig.13 The radio examination shows an insufficient canal treatment on the 16
which must be resumed.
It is then necessary to either remove the crown or cut an access cavity through the occlusal surface of the crown to perform the endodontic treatment (fig.14).
Fig.14 But the presence of the inlay-core prevents the resumption of
endodontic treatment through the crown and leads to the removal with section of the restoration.
The carious recovery
A poor hermeticity of the dento-prosthetic joint is always possible and very often facilitates the accumulation of the dental plaque at the origin of the carious recurrence.
The bacterial infiltration then causes a weakening of the dental stump, as well as the decohesion of the dental cement. It is therefore necessary to remove the crown to perform the care, remake a crown and thus succeed in keeping the tooth as long as possible (fig.15,16).
The preservation of pulp vitality should always be preferred, for reasons of strength and as a warning signal.
This, the realization of crowns on living teeth is an act thoroughness in its elaboration.
Failure to comply with certain principles (new dental drills, under irrigation, intermittence) leads to a "dentin wound" that
canal treatment on the 16
It is then necessary to either remove the crown or cut an access cavity through the occlusal surface of the crown to perform the
core prevents the resumption of endodontic treatment through the crown and leads to the removal with section
prosthetic joint is always often facilitates the accumulation of the dental plaque at the origin of the carious recurrence.
The bacterial infiltration then causes a weakening of the dental stump, as well as the decohesion of the dental cement. It is e crown to perform the care, remake a crown and thus succeed in keeping the tooth as long
Fig.15 Recurrence of caries under prosthetic ...
Fig.16 Requires removal and completion of a new restoration.
The fracture of teeth
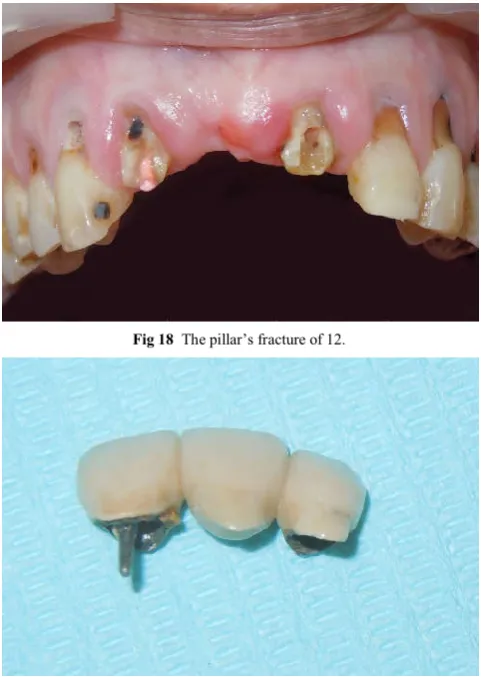
This is one of the main reasons for removal in fixed prosthesis. These fractures and cracks can be consecutive to a traumatism of the teeth, caused by a shock, a repeated mechanical stress (as in the patient bruxomane) or sometimes in the normal conditions of mastication following the rupture of roots too weakened by the previous treatments, and this is unrelated to the seniority of the prosthesis (fig.17,18,19).
Fig 17 Metal-ceramic bridge replacing the 11.
Dental fractures are related to the types of crown and root reconstructions used (metallic or resin)
[14], have shown that dental fractures are more numerous with
Recurrence of caries under prosthetic ...
Requires removal and completion of a new restoration.
This is one of the main reasons for removal in fixed prosthesis. These fractures and cracks can be consecutive to a traumatism of the teeth, caused by a shock, a repeated mechanical stress (as in the patient bruxomane) or sometimes in the normal conditions of mastication following the rupture of roots too weakened by the previous treatments, and this is unrelated to the seniority of the prosthesis (fig.17,18,19).
ceramic bridge replacing the 11.
Morchad Bouabid IJCMS, 2019; Vol. 5(8): 1050-1055.
crown and root(metallic)reconstructions than with carbon fiber posts associated with a composite.
Fig 18 The pillar’s fracture of 12.
Fig 19 Realization of an inlay-core in direct technique at the level of the 12, it
allows to put back the same bridge.
If this fracture is located at the junction between the post and the pillar, removal of the anchor is possible depending on its situation through different techniques: Masserman kit, Gonon extractor.
On the other hand, if one has a root fracture, this leads almost systematically to the extraction of the tooth. But before we get there it is necessary to determine whether the tooth cannot undergo a hemisection or a root amputation especially when it is a strategic tooth.
Aesthetic Etiologies [15,16,17,18,7]
Aesthetics has a part of subjectivity specific to each, but there are still a number of objective criteria that must be respected to promote successful integration of the prosthesis into the oral cavity (fig.20).
Failures related to a periodontal problem (fig.21,22)
The aesthetic integration of a fixed prosthesis is not conceivable out of the periodontal context. The position of the free edge of the marginal gingiva, its volume and color have an aesthetic impact all the more marked as they appear upon smiling.
Fig 20 Periodontal inflammation with absence of embrasures.
Fig 21 Panoramic X-ray: 2 ceramic-metallic bridges replacing 11, 21 and 31,41
without root canal treatment, noted the root resorptions.
Fig 22 The clinical examination of the 2 bridges shows an unsightly appearance
that requires removal.
Gingival recessions and gingival hyperplasia are important unsightly factors in the removal of an overactive prosthesis, particularly in the presence of a gummy smile.
The aesthetic failures strictly speaking
Disharmony of form and arrangement;
Disharmony of the gingival line;
Asymmetry in relation to the median line;
Failure of the color.
Many other reasons to remove restorations that have become inadequate:
Replace crowns with matt resin vestibular encrustation with more aesthetic ceramics (fig.23);
Also consider the change of a metal-ceramic crown by an all-ceramic crown.
Fig.23 Restoration with in resin vestibular encrustation. Note material’s
degradation and metal’s visibility.
CONCLUSION
In fixed prosthese, the failures are particularly heavy consequences and can intervene at all levels involved for these restorations. They can occur immediately after prosthesis placement or appear again later. These failures can be of types: periodontal, endodontic, esthetic, prosthetic or functional. Any failure requires reintervention; the latter still does not want to say the removal of the prosthetic element but it may be a repair of the prosthesis in the mouth.
For this reason the therapeutic decision will be made after a careful and precise clinical and radiological examination while trying to answer the wishes of the patient.
Références
1. LIEBENBERG W.H. Dépose des prothèses fixées sans les endommager.Clinic (Paris), 1995, l6, 6, 421- 429. 68 2. SCURRIA M., et al. Meta-analysis of fixed partial
denture survival: Prostheses and abutments.
J.Prosthet.Dent. 1994, 79, 459-464. 94
3. DERRIEN G., JARDEL V. Le démontage des prothèses fixées (Odontologie). Encycl. Med. Chir. (Elsevier, Paris), 23-305-B-10 (1999). 38
4. 4. DOT O., BRUNET A. Réintervention en prothèse fixée. Réalités Cliniques, 2000, 11, 3,315-324. 42 5. Estrabaud Y, Arduin J-L, Daniel A, Delaunay B.
L’examen parodontal préprothétique : réflexions cliniques. Journal de parodontologie 1990 ; 9 (3) : 237-244. 5X
6. BALDENSPERGER R., et al. Le descellement. Actual. Odonto-Stomatol, 1977, 119, 561 -578. 9
7. Laborde G, Borghetti A. Préparations intra-creviculaires et parodonte marginal. Réalités cliniques 1992 ; 3(2) : 203-214. 8
8. Laborde G, Margossiam P, Maille G, Botti S, Dinardo Y, Miramont E, Couderc G, Koubi S. Esthétique et approche clinique des limites de préparations en prothèse fixée. Rev. Odont. Stomat. 2010 ; 39 ; 35-44. 11
9. TREVELO A. Démontage des couronnes prothétiques à recouvrement périphérique. Réalités Cliniques, 1996,1, 3, 28 1-290. 97
10. NEVINS M., et al. L'embrasure en prothèse parodontale. Cah. Prothèse, 1979, 28, 151-161. 82
11. Laborde G, Borghetti A, Gilardenghi M, Heraud J. Réalisation et accès aux limites intrasulculaires : vers la stabilité du parodonte marginal. Cah. Prothèse 1988 ; 62 : 7-17. 9
12. Laborde G, Lacroix P, Margossian P, Laurent M. Les systèmes céramo-céramiques. Réalités cliniques 2004 ; 15(1) : 89-104. 10
13. Sakout M., Chraibi B. Reprise du traitement canalaire: quand et dans quel pronostic. Web journal du dentiste, février 2005, volume I, n° 1. 15
14. MARTINEZ-IN SUA A, et al. Comparison of the fracture resistances of pulps teeth restored with a cast post and core or carbon-fiber post with a composite core.
J .Prosthet. Dent. , 1998,80, 527-532. 73
15. EXBRAYAT J., et al. Manuel de prothèse fixée unitaire. Paris: Masson, 1993, 221p. 46
16. SHILLINGBURG H.T. et al. Bases fondamentales en prothèse fixée (3èmc édition). Paris: éditions Cdp, 1998, 572p. 95
17. Estrabaud Y, Arduin J-L, Daniel A, Delaunay B. L’examen parodontal préprothétique : réflexions cliniques. Journal de parodontologie 1990 ; 9(3) : 237-244. 3
18. Gontier S, Cheylan J-M, Degrange M. Scellement et collage des reconstitutions corono-radiculaires. Cah. Prothèse 2001 ; 113 : 35-49. 5