R E S E A R C H A R T I C L E
Open Access
Autism spectrum disorders and fetal hypoxia in a
population-based cohort: Accounting for missing
exposures via Estimation-Maximization algorithm
Igor Burstyn
1,2*, Xiaoming Wang
3,4, Yutaka Yasui
3, Fortune Sithole
1, Lonnie Zwaigenbaum
5Abstract
Background:Autism spectrum disorders (ASD) are associated with complications of pregnancy that implicate fetal hypoxia (FH); the excess of ASD in male gender is poorly understood. We tested the hypothesis that risk of ASD is related to fetal hypoxia and investigated whether this effect is greater among males.
Methods:Provincial delivery records (PDR) identified the cohort of all 218,890 singleton live births in the province of Alberta, Canada, between 01-01-98 and 12-31-04. These were followed-up for ASD via ICD-9 diagnostic codes assigned by physician billing until 03-31-08. Maternal and obstetric risk factors, including FH determined from blood tests of acidity (pH), were extracted from PDR. The binary FH status was missing in approximately half of subjects. Assuming that characteristics of mothers and pregnancies would be correlated with FH, we used an Estimation-Maximization algorithm to estimate HF-ASD association, allowing for both missing-at-random (MAR) and specific not-missing-at-random (NMAR) mechanisms.
Results:Data indicated that there was excess risk of ASD among males who were hypoxic at birth, not materially affected by adjustment for potential confounding due to birth year and socio-economic status: OR 1.13, 95%CI: 0.96, 1.33 (MAR assumption). Limiting analysis to full-term males, the adjusted OR under specific NMAR
assumptions spanned 95%CI of 1.0 to 1.6.
Conclusion:Our results are consistent with a weak effect of fetal hypoxia on risk of ASD among males. E-M algorithm is an efficient and flexible tool for modeling missing data in the studied setting.
Background
The autism spectrum disorders (ASD) comprise a group of neurodevelopmental conditions that are associated with impaired verbal and non-verbal communication and social interaction, and restricted and repetitive pat-terns of behavior, which typically manifest before age of 3 years [1]. Although relatively rare[2-7], ASD can have a devastating effect on the quality of life of entire families and is associated with considerable societal eco-nomic burden[8]. There is some evidence that ASD pre-valence is on the increase[9], although it remains unclear as to whether this increase can be completely accounted for by changes in case definition and improved ascertainment. While some genetic risk factors
for ASD are known [10], the potential contribution of environmental factors has not been excluded and media-tions involving gene-environment interacmedia-tions would contribute to the observed genetic complexity in ASD. A recent review suggests that advanced parental age and fetal growth restriction place children at an elevated risk of developing ASD[11]. However, a recent meta-analysis concluded it is premature to implicate specific preg-nancy complications in etiology of ASD[12]. Nonethe-less, Kolevzon et al.[11], on the basis of epidemiological evidence, advanced a hypothesis that neonatal or fetal hypoxia are implicated in ASD, even though hypoxia was not measured in any of the reviewed studies. Chronically high maternal levels of dopamine have also been suggested by Previc[13] as the underlying cause of ASD, which would be expected to correlate with occur-rence of fetal hypoxia. More recently Mueller and Bale [14] argued, based on studies of stress sensitivity in * Correspondence: [email protected]
1
Department of Medicine, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Alberta, Canada
Full list of author information is available at the end of the article
juvenile mice following prenatal hypoxic insults, that males are more susceptible to development of maladap-tive stress responses associated with many neurodeve-lopmental disorders such as ASD. They suggested that this vulnerability is determined by sex-specific differ-ences in placental physiology[14]. Excess of ASD among males is well-documented[15]. If fetal hypoxia were equally likely among boys and girls, but boys were more susceptible to its effect on ASD risk, this would contri-bute to explaining male predominance among ASD patients.
Parallel line of research suggests that neonatal ence-phalopathy caused by perinatal asphyxia/hypoxia in infants born at term is associated with neurological impairment later in life[16]. Therefore, it may well be that foetal hypoxia is simply an upstream cause of neo-natal encephalopathy that then relates to risk of ASD. Indeed, the most recent review of the contribution of neonatal encephalopathy to infant neurological develop-ment concluded that even moderate post-asphyxia neo-natal encephalopathy appears to contribute to cognitive and sensory-motor impairments, although heterogeneity in published results was noted[17].
In fact, one study of 239 children who survived neona-tal encephalopathy reported that 4.2% were diagnosed with an ASD. This represents, after adjustment for con-founders, about a 6-fold increase in ASD risk compared to ASD rates among 563 children who did not have neonatal encephalopathy (0.9%)[18]. The small sample size here led to render results of this report vulnerable to observing“significant”findings purely due to chance and the 95% confidence intervals of the relative risk esti-mate (2 to 17)[18] is extremely wide, casting doubts about the reproducibility of the finding[19].
None of the epidemiological studies conducted to date studied direct effects of hypoxia at birth on ASD. There-fore, we tested, in a population-based birth cohort, the hypothesis that risk of ASD is related to fetal hypoxia and investigated whether this effect is greater among males.
Methods
Record linkage
This cohort and analysis of association of perinatal risk factors with risk of ASD are described elsewhere, with-out consideration of fetal hypoxia[20], defined as fetal scalp pH < 7.25, or umbilical artery pH < 7.20, or venous pH < 7.28. Delivery records held by the Alberta Perinatal Health Program (APHP) identified the cohort of singleton live births in the province of Alberta, Canada, between January 1, 1998 and December 31, 2004. The APHP provided information regarding rele-vant ante- and peri-natal risk factors. Information on the risk factors was collected on admission to hospital
for delivery, as part of routine clinical care. They are con-sidered to be accurate and any internal inconsistency in the records is scrutinized by APHP; if apparent error in the delivery records cannot be resolved, APHP records a missing value for a given variable. The unique Personal Health Number (PHN) of mother and child along with child’s gender and date of birth in APHP file were used to follow-up the cohort through records held by the Alberta Health and Wellness (AHW). In the universal healthcare insurance system of Alberta, all residents are served by physicians who bill the government for their services, linked to specific diagnostic codes, International Classification of Diseases 9thedition (ICD-9). Children matched in APHP file to AHW records were followed-up by the investigators until March 31, 2008 for (a) ICD-9 codes indicating ASD (299.0 or 299.8) listed with the physician billing record, (b) child’s residency and mortal-ity (in a given fiscal year ending on March 31) and (c)
mothers’socioeconomic status. Outcome was defined
using most liberal definition from our previous work: at least one ASD claim by any physician because such case definition showed good sensitivity and specificity and did not affect associations between studied risk factors and ASD[20]. Such case definition for ASD is analogous to the one used in another, very similar Canadian study, where it was shown to have acceptable sensitivity and specificity relative to gold standard diagnostic assessment in a specialty clinic[21]. Study protocol was approved by the University of Alberta Health Ethics Research Board and the custodians of the data.
Statistics
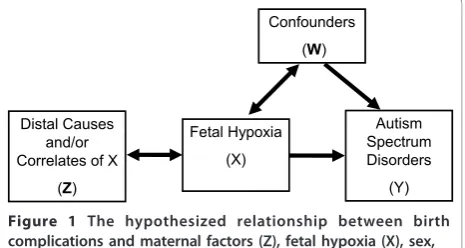
Causal model considered in this paper is shown in Figure 1. Our hypothesis is that ASD (Y) is caused by fetal hypoxia (X). Birth year and socio-economic status (W) are treated as confounders (as is fetal gender unless the effect modification by gender is tested), because there is little reason to suspect that such broad proxies for trends in health (social-economic status) and chance
Fetal Hypoxia (X)
Autism Spectrum Disorders
(Y) Confounders
(W)
Distal Causes and/or Correlates of X
(Z)
of being diagnosed (birth year) would only act as antece-dents of fetal hypoxia without also being associated with risk of ASD. We make a very strong assumption that all other covariates (Z) are assumed to be correlated with ASD through fetal hypoxia, but relax it when we test the notion that prematurity can also have a direct effect on the risk of ASD. Our justification for this approach is that we focus on testing a specific well-justified hypothesis. In most of the analyses, unless otherwise indicated, covariates Z include maternal age (≤25, 25-≤ 30, 30- ≤35, >35 years), maternal weight (>91 kg or < 45 kg), maternal height < 152 cm, pre-pregnancy dia-betes, gestational diadia-betes, bleeding (< 20 and/or > 20 weeks), cigarette smoking (any), poor weight gain (26-36 weeks < 0.5 kg/week), parity (0, 1, 2, 3,≥4), pre-eclamp-sia, presentation (cephalic or breech/shoulder), type of labor (spontaneous, induced, no labor/C-section), gesta-tional age (< 37,≥37 weeks), birth weight (< 2.5, 2.5-4.5, > 4.5 kg), Apgar at 1 and 5 min (< 7). A logistic regression model was fitted to data relating odds of ASD to fetal hypoxia, to estimate odds ratios (ORs) and associated 95% confidence intervals (CIs).
Fetal hypoxia status, the binary exposure variable of interest (X), was missing in approximately one half of our study subjects. Based on the notion that some vari-ables (Zs) including characteristics of mothers and preg-nancies would be correlated with the exposure X, we used an EM algorithm[22] to tackle the estimation pro-blem of the association between fetal hypoxia (X) and ASD (Y), in the presence of missing values in X. The basic idea of the EM algorithm is to use subjects’ char-acteristics Zs and the outcome Y to model X using the subjects with observed values of X. With the model for X with Zs and Y, we can weigh the two possibilities of the missing value of X, X = 1 and X = 0, in the likeli-hood function for maximum-likelilikeli-hood statistical infer-ence on parameters. Since the model for X with Zs and Y contains the parameters of interest, the weighted like-lihood function can be iteratively maximized: estimating the weights using the current parameter estimates; and constructing the weighted likelihood function, which can then be maximized to update the parameter esti-mates. We initially make an assumption that, given Z and Y, missingness of X occurs at random: the missing-at-random (MAR) assumption, which assumes random missing conditioned on Z and Y. Under the MAR con-ditioned on Z and Y, using those who have X for mod-eling X with Z and Y is valid. It is reasonable to doubt the validity of MAR assumption in this situation, if we consider the possibility that the likelihood of X = 1 is systematically higher for a given Z among those that were tested for fetal hypoxia. For example, clinicians can consider factors other than those measured as Zs in ordering test for fetal hypoxia, such that their suspicion
of a positive result, over and beyond what Zs suggest, is elevated before the test is performed. If this were the case, then missingness in X is not at random (not-missing-at-random, NMAR). To consider the NMAR case, we introduce (0 ≤ r ≤ 1), the ratio of expected probabilities of having hypoxia in X missing group and non-missing group for a given set of Zs. Given informa-tion from Zs, setting = 1 means we assume MAR. Any case with < 1 amounts to postulating a special case of
NMAR. There is no data on how much smaller than 1r
should be in our particular setting. Such values can arise from separate experiments (not possible in our situa-tion), or sensible guesses of values ofr can be made for the purposes of sensitivity analysis (route we followed); yet another approach is to follow fully Bayesian paradigm and place a prior on r. It is not possible to
optimizer from our data using EM algorithm. We
con-sidered in sensitivity analyses a range of r spanning values consistent with excellent (r = 0.1) to moderate (r= 0.7) additional clinical judgment indicating the like-lihood of positive test, over and beyond Zs. Note that
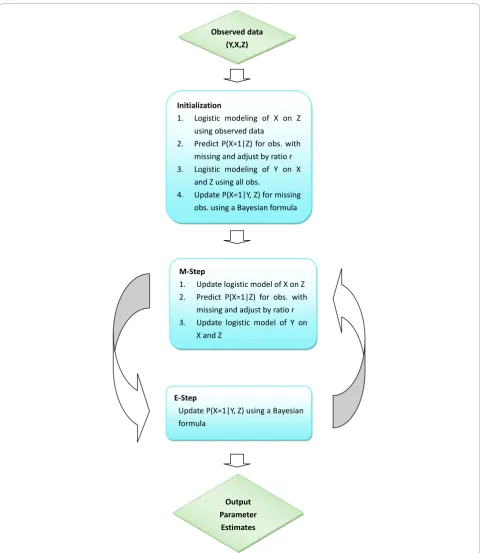
r = 0.5 suggests that those not tested are only at 50% risk of hypoxia (given Zs) compared to those who were tested: this is consistent with the notion of predictive ability of the clinical judgment, beyond Zs, that the hypoxia test is positive. As we shall see below (Table 1), intensive testing for hypoxia is associated with a factor of 2-5 increase in detecting hypoxia, which gives strong evidence that testing is ordered only on strong suspicion of hypoxia and thatr is in the range of 0.5 or smaller. All EM algorithms used in this paper converged within 250 iterations. Mathematical details are given in the Additional File 1 and sketch of SAS (SAS Institute, Cary, NC) code required to implement the method is given in Additional File 2. Schematic presentation of EM algorithm we implemented is given in Figure 2.
Results
As expected, there was some disagreement among tests on the same neonate. However, overall prevalence of fetal hypoxia among those tested appeared to be similar whether all tests were required to be congruent (10%) or only one had to be positive (14%). Measurement of fetal scalp pH, although relatively infrequent, appears to be associated with elevated likelihood of the overall positive test result, perhaps because not of the inherent superior sensitivity of the test, but because it is adminis-tered only when there is considerable suspicion that the fetus may be hypoxic. There were 200,557 full-terms births in the cohort and gestational age at birth was missing for 444 neonates. 1,011 of full-terms neonates were diagnosed with ASD during the follow-up.
Table 2 summarizes data on ASD and measures of fetal hypoxia as observed for births of all gestational ages. Among the subgroup of 17,083 infants classified as hypoxic, 113 were diagnosed with ASD during the fol-low-up (0.66%). The observed rate of ASD was slightly lower among 88,553 infants who tested negative for fetal hypoxia (530 ASD cases, 0.60%) and much lower among subjects 113,254 whose fetal hypoxia status was unknown, that is mostly not tested (495 ASD cases, 0.44%). The observed rate of ASD was the highest among males who were hypoxic at birth (100 ASD cases, 1.10%). Males who were tested and did not appear to be hypoxic at birth had a slightly lower observed rate of ASD (452 ASD cases, 0.99%), but males who were not tested for hypoxia certainly had a reduced observed rate of ASD compared to those males who were tested (400 ASD cases, 0.70%). The observed rates of ASD among female children did not vary with measures of fetal hypoxia (0.16% among hypoxic vs. 0.18% among non-hypoxic) and was much lower than among males (1.10% among hypoxic vs. 0.99% among non-hypoxic).
Among full-term births the pattern of observed rates is similar to that seem among all births in Table 2. The
observed ASD rate among full-terms births was higher among those who tested positive for hypoxia (0.62%, 96/ 15,557) compared to those who tested negative for hypoxia (0.58%, 557/95,352). The test for hypoxia was not performed among 105,205 members of this sub-cohort who had an even lower observed rate of ASD (454, 0.43% affected). 480 of 49,165 full-term male births with data on hypoxia were diagnosed with ASD during the follow-up (observed rate 0.98%). Among 8,286 males hypoxic at birth, the observed rate of ASD was 1.03% (85 cases), but among males not hypoxic at birth the observed rate of ASD was slightly lower: 0.97% (395 cases). In this male sub-cohort, when information on hypoxia was missing, the observed rate of ASD was even lower 0.69% (364 cases). 77 of 46,187 full-term female births with data on hypoxia were diagnosed with ASD during the follow-up (observed rate 0.17%). Among 7,271 females hypoxic at birth, the observed rate of ASD was 0.15% (11 cases), but among females not hypoxic at birth the observed rate of ASD was higher: 0.17% (66 cases). In this female sub-cohort, when information on hypoxia was missing, the observed rate of ASD was the same as among girls who tested as not hypoxic at birth: 0.17% (90 cases).
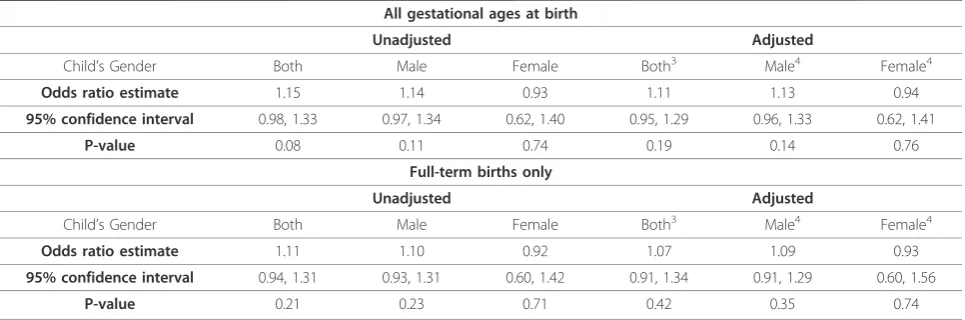
We will next examine ASD rate modeled using E-M algorithm among births of all gestational ages. Table 3 (top) presents results from E-M algorithm that modeled the presence of fetal hypoxia for 113,254 out of 218,890 subjects and then estimated odds ratios for the associa-tion of ASD with fetal hypoxia with and without adjust-ment for suspected confounders (Ws) and with and without stratification on child’s gender. In stratified ana-lyses, strata-specific modeling of missing exposures was performed using values of Zs specific to each gender. There is a clear suggestion of a small excess risk of ASD only among males who were hypoxic at birth: unad-justed OR 1.14, 95%CI: 0.97, 1.34. This result is not Table 1 Ascertainment of Fetal Hypoxia1Among Neonates
Test(s) Subjects tested All tests positive At least one test positive
Number of subjects % Number of subjects %
All three tests 26 1 4 12 46
Two tests
Fetal scalp and umbilical arterial blood pH 178 27 15 77 43
Umbilical arterial and venous pH 41,245 3,583 9 8,866 21
Fetal scalp and umbilical venous blood pH 4 0 0 0 0
One test
Fetal scalp pH 47 16 34 16 34
Umbilical arterial blood pH 75,775 7,727 10 7,727 10
Venous umbilical blood pH 3,561 385 11 385 11
Any of the three tests 120,836 11,739 10 17,083 14
materially affected by adjustment for potential con-founding due to birth year and socio-economic status: adjusted OR 1.13, 95%CI: 0.96, 1.33. As expected from descriptive analyses (Table 2), there is no indication that ASD risk among females is associated with positive test
for fetal hypoxia. The formal test of the (multiplicative) interaction of male gender and hypoxia on the risk of ASD did not indicate that males had a higher degree of association between hypoxia and ASD than females:P= 0.68 for interaction OR of 0.91 (details of the model not Observeddata
(Y,X,Z)
Initialization
1. LogisticmodelingofXonZ
usingobserveddata
2. PredictP(X=1|Z)forobs.with
missingandadjustbyratior
3. LogisticmodelingofYonX
andZusingallobs.
4. UpdateP(X=1|Y,Z)formissing
obs.usingaBayesianformula
MͲStep
1. UpdatelogisticmodelofXonZ
2. PredictP(X=1|Z)forobs.with
missingandadjustbyratior
3. UpdatelogisticmodelofYon XandZ
EͲStep
UpdateP(X=1|Y,Z)usingaBayesian
formula
Output
Parameter
Estimates
shown). Given uncertain role that prematurity plays in ASD etiology[23], we could not justify treating it a sole antecedent of hypoxia and not a risk factor on its own. To control for possible confounding effect of prematur-ity we repeated the analysis on full-term births only (Table 3, bottom). The results are largely consistent with those obtained on full cohort, but suffer from loss of precision. The observation provides some further jus-tification in not treating Z as confounders in the bulk of our analyses.
Lastly, we investigated the impact of specific NMAR assumption on our results in a sub-set of full-term male infants where the conservative analyses under the MAR assumption indicated a possible positive associa-tion (Table 4). There was also evidence that missing-ness of data on hypoxia was associated with risk of ASD in males, but not in females. Under the realistic NMAR assumption (r from 0.1 to 0.5), it appears that point estimate of the effect (OR) of hypoxia on risk of ASD among males who were born at full-term Table 2 Summary of Data on Reported Fetal Hypoxia and Diagnosis of Autism Spectrum Disorders in the Same Child (All Gestational Ages at Birth)1
Child’s Gender Autism Spectrum Disorders Fetal Hypoxia Total
Present2 Absent4 Unknown
Both Present N 113 530 495 1,138
%3 0.66 0.60 0.44 0.52
(0.06) (0.03) (0.02) (0.02)
TotalN 17,083 88,553 113,254 218,890
Male Present N 100 452 400 952
%3 1.10 0.99 0.70 0.85
(0.11) (0.05) (0.03) (0.03)
TotalN 9,109 45,594 57,257 111,960
Female Present N 13 78 95 186
%3 0.16 0.18 0.17 0.17
(0.04) (0.02) (0.02) (0.01)
TotalN 7,974 42,959 55,997 106,930
1: singletons born in Alberta 1998-2004 and followed up till March 31, 2008.
2: at least one of the three tests for fetal hypoxia is positive, i.e. fetal scalp pH < 7.25, or umbilical artery pH < 7.20, or venous pH < 7.28. 3: percentage of exposed to different states of fetal hypoxia (with standard errors).
4: excludes subjects with base pH, i.e. this reference category has pH in normal physiological range.
Table 3 Association of Fetal Hypoxia at Birth1and Diagnosis of Autism Spectrum Disorders2: Results of Logistic Regression Fitted with EM Algorithm for Handling Unknown Exposures That are Modeled From Maternal and Birth Characteristics Under MAR Assumption (r = 1) Stratified on Child’s Gender
All gestational ages at birth
Unadjusted Adjusted
Child’s Gender Both Male Female Both3 Male4 Female4
Odds ratio estimate 1.15 1.14 0.93 1.11 1.13 0.94
95% confidence interval 0.98, 1.33 0.97, 1.34 0.62, 1.40 0.95, 1.29 0.96, 1.33 0.62, 1.41
P-value 0.08 0.11 0.74 0.19 0.14 0.76
Full-term births only
Unadjusted Adjusted
Child’s Gender Both Male Female Both3 Male4 Female4
Odds ratio estimate 1.11 1.10 0.92 1.07 1.09 0.93
95% confidence interval 0.94, 1.31 0.93, 1.31 0.60, 1.42 0.91, 1.34 0.91, 1.29 0.60, 1.56
P-value 0.21 0.23 0.71 0.42 0.35 0.74
1: at least one of the three tests for fetal hypoxia is positive, i.e. fetal scalp pH < 7.25, or umbilical artery pH < 7.20, or venous pH < 7.28. 2: singletons born in Alberta 1998-2004 and followed up till March 31, 2008.
increases to 1.2-1.3 with 95%CIs that lie approximately between 1.0 and 1.6. Even if deviation from the MAR assumption was weak (r = 0.7), the resulting change in inference is dramatic: 95%CIs widen somewhat and shift from 0.91-1.29 (Table 3) to 0.99-1.46 (Table 4), while the point estimate increases from 1.09 (Table 3) to 1.20 (Table 4).
Discussion
There are many difficulties with these data beyond miss-ing-ness: both exposures and outcomes are suspected of being misclassified, which would bias apparent OR esti-mates, most likely towards the null if both misclassifica-tion mechanisms are non-differential. Covariates from perinatal database are known to be recorded accurately [Ms N. Bott of APHP, personal communications] because they use data essential to medical care, not just billing, even though some information (such as maternal smoking[24] used to model risk of fetal hypoxia) is known to be collected with error. Of course error in variables can bias our results, but we lack information on the extent and direction of such bias. Our analysis is also limited by small number of girls, so that our failure to detect an association among them may simply be due to low power. Short follow-up for some members of the cohort born in 2004 may have introduced error due to incomplete ASD ascertainment, since they were be only 4 at the end of follow-up, but our previous results sug-gest that in this population peak age of diagnosis was between ages of 3 and 4 [20], therefore our data cannot address this potential limitation. Nonetheless, our data are valuable because they enable the first test of associa-tion of fetal hypoxia with risk of ASD in a populaassocia-tion- population-based birth cohort. Innovative statistical methodology that we used to meet challenged posed by the data should prove to be helpful to researchers facing similar complications.
We observed that males who were tested for foetal hypoxia were more likely to develop ASD. This supports the generally establish contention that ASD patients tend to have complicated pregnancies[11], which often involve, upon suspicion, testing for foetal hypoxia. Pre-sence of hypoxia itself, under the causal models that we considered, appears to only affect males. This finding is consistent with oura priori specified hypothesis about greater sensitivity of males to hypoxia-induced insults during gestation.
We conducted most of our analyses under a strong assumption that the majority of observed pregnancy and birth characteristics only affected risk of ASD through fetal hypoxia. In doing so, we reflected on discussion by Newschaffer and Cole[25] of testing alternative causal models in studies of perinatal risk factors in ASD. Since our entire analysis is predicated on apparent association of hypoxia with pregnancy and birth characteristics (Z), we can reject the“etiologic heterogeneity” model[25]: if hypoxic status was independent of Z we would not have been able to implement analysis that relies on EM-algo-rithm. We tested a priorjustified effect modification by gender and report non-multiplicative interaction on the basis of stratified analysis. Then we have to consider “epiphenomena” models [25].“Epiphenomena model 2” is in fact represented by Figure 1 and was estimated here directly. With respect to“epiphenomena model 1”, it is currently unreasonable to suspect that ASD causes fetal hypoxia, since that would postulate a fetus that is both destined to have ASD and able to affects its own supply of oxygen. This leaves the possibility that“shared risk factor” model[25] applies and there may be con-founding by direct effect of elements of Z on risk of ASD if model in Figure 1 is fitted to the data. We con-sidered confounding by prematurity: in a stratum of full-term infants for who we had sufficient sample size to obtain meaningful estimates (92% of all subjects) we found little evidence that prematurity induced associa-tion between hypoxia and ASD. None of the other ele-ments of Z appeared to be likely candidates for examining the direct effect on risk of ASD. Of course given how little we know about causes of ASD, it is pos-sible that we failed to postulate and test true causal model. If that is the case, then our estimates may in fact be biased by latent confounding or effect modification, which is of course true of most observational research into subject matters, such as ASD, where uncertainty abounds about what the actual causes may be.
Missing values are common in public health research. Understanding the missing mechanism is the key for a proper missing data analysis. Relaxing unrealistic MAR assumptions changed the point estimate of the disease-exposure odds ratio and sifted confidence intervals (P-values) towards the region conventionally thought of Table 4 Association of Fetal Hypoxia at Birth1 and
Diagnosis of Autism Spectrum Disorders2: Results of Logistic Regression Fitted with EM Algorithm for Handling Unknown Exposures That are Modeled From Maternal and Birth Characteristics Under Specific NMAR Assumption Among Full-Term Male Births
Deviation from MAR3 Strong Strong Moderate Weak
r 0.1 0.2 0.5 0.7
Odds ratio estimate 1.28 1.28 1.24 1.20
95% confidence interval 1.03, 1.60 1.03, 1.58 1.01, 1.52 0.99, 1.46
P-value 0.03 0.03 0.04 0.06
1: at least one of the three tests for fetal hypoxia is positive, i.e. fetal scalp pH < 7.25, or umbilical artery pH < 7.20, or venous pH < 7.28.
2: singletons born in Alberta 1998-2004 and followed up till March 31, 2008, effects adjusted for birth year and socio-economic status.
as “significant”. Thus, the use of EM-algorithm for dealing with the special missing value problem in this project in conjunction with sensitivity analysis using the specified NMAR assumption altered statistical inference and was therefore useful.
Conclusions
Our results are consistent with a weak effect of fetal hypoxia on risk of ASD that is confined to males. It may well be that some latent indication or an unknown correlated of testing for hypoxia at birth are responsible for the increased risk of ASD among males and there-fore investigation of role of hypoxia at birth in ASD remains a fruitful area for research.
Additional material
Additional file 1: EM Algorithm with either MAR or NMAR assumptions. Mathematical details of EM algorithm implemented in this article.
Additional file 2: Implementation of EM Algorithm for missing values in SAS software. SAS code that was used to implement EM algorithm presented in this article with annotation that allow adapting it to similar applications.
Acknowledgements
Igor Burstyn and Lonnie Zwaigenbaum were supported, respectively, by the Population Health Investigator and Health Scholar salary awards from the Alberta Heritage Foundation for Medical Research. This study is based on data supplied by Alberta Health and Wellness (AHW) and the Alberta Perinatal health Program (APHP). The interpretation and conclusions contained herein are those of the researchers and do not necessarily represent the views of the Government of Alberta or APHP. Neither the Government, nor AHW, nor the APHP expresses any opinion in relation to this study. We are grateful to AHW and APHP for supplying and linking the data; special thanks go to Alex Marinov, Wendy Mitchell, Nancy Piche, Nancy Bott and Sharon Zhang. Craig Newschaffer provided invaluable comments on the final draft of the manuscript.
Author details 1
Department of Medicine, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Alberta, Canada.2Department of Environmental and Occupational Health, School of Public Health, Drexel University, Philadelphia, Pennsylvania, USA.3Department of Public Health Sciences, School of Public Health, University of Alberta, Edmonton, Alberta, Canada.4School of Statistics and Management, Shanghai University of Finance and Economics, Shanghai, China.5Department of Pediatrics, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Alberta, Canada.
Authors’contributions
All authors credited with this work made substantial intellectual contribution to the submitted manuscript. IB led overall project; the current analysis address the hypothesis he developed and attempted to test. IB, SF and LZ designed the study, oversaw data acquisition, contributed to analysis and interpretation of the data and co-wrote the manuscript. XW and YY devised and implemented data analysis via E-M algorithm, they led the preparation of technical appendices and made substantial contribution to writing the main body of the manuscript. All authors reviewed and approved the submitted version of the manuscript.
Competing interests
The authors declare that they have no competing interests.
Received: 19 July 2010 Accepted: 5 January 2011 Published: 5 January 2011
References
1. Bailey A, Phillips W, Rutter M:Autism: towards an integration of clinical, genetic, neuropsychological, and neurobiological perspectives.J Child Psychol Psychiatry1996,37:89-126.
2. Bertrand J, Mars A, Boyle C, Bove F, Yeargin-Allsopp M, Decoufle P: Prevalence of autism in a United States population: the Brick Township, New Jersey, investigation.Pediatrics2001,108:1155-1161.
3. Yeargin-Allsopp M, Rice C, Karapurkar T, Doernberg N, Boyle C, Murphy C: Prevalence of autism in a US metropolitan area.JAMA2003,289:49-55. 4. Williams E, Thomas K, Sidebotham H, Emond A:Prevalence and
characteristics of autistic spectrum disorders in the ALSPAC cohort.Dev Med Child Neurol2008,50:672-677.
5. Fombonne E:Epidemiological surveys of autism and other pervasive developmental disorders: an update.J Autism Dev Disord2003, 33:365-382.
6. Ouellette-Kuntz H, Coo H, Yu CT, Chudley AE, Noonan A, Breitenbach M,
et al:Prevalence of pervasive developmental disorders in two Canadian provinces.Journal of Policy and Practice in Intellectual Disabilities2006, 3(3):167-172.
7. Ouellette-Kuntz H, Coo H, Lloyd JE, Kasmara L, Holden JJ, Lewis ME:Trends in special education code assignment for autism: implications for prevalence estimates.J Autism Dev Disord2007,37:1941-1948. 8. Ganz ML:The lifetime distribution of the incremental societal costs of
autism.Arch Pediatr Adolesc Med2007,161:343-349.
9. Centers for Disease Control and Prevention (Eds):Prevalence of Autism Spectrum Disorders–Autism and Developmental Disabilities Monitoring Network.Morbidity and Mortality Weekly Report2007,56.
10. Szatmari P, Paterson AD, Zwaigenbaum L, Roberts W, Brian J, Liu XQ,et al: Mapping autism risk loci using genetic linkage and chromosomal rearrangements.Nat Genet2007,39:319-328.
11. Kolevzon A, Gross R, Reichenberg A:Prenatal and perinatal risk factors for autism: a review and integration of findings.Arch Pediatr Adolesc Med
2007,161:326-333.
12. Gardener H, Spiegelman D, Buka SL:Prenatal risk factors for autism: comprehensive meta-analysis.Br J Psychiatry2009,195:7-14.
13. Previc FH:Prenatal influences on brain dopamine and their relevance to the rising incidence of autism.Med Hypotheses2007,68:46-60. 14. Mueller BR, Bale TL:Sex-specific programming of offspring emotionality
after stress early in pregnancy.J Neurosci2008,28:9055-9065.
15. Newschaffer CJ, Croen LA, Daniels J, Giarelli E, Grether JK, Levy SE,et al:The epidemiology of autism spectrum disorders.Annu Rev Public Health2007, 28:235-258.
16. van Handel M, Swaab H, de Vries LS, Jongmans MJ:Long-term cognitive and behavioral consequences of neonatal encephalopathy following perinatal asphyxia: a review.Eur J Pediatr2007,166:645-654. 17. Pin TW, Eldridge B, Galea MP:A review of developmental outcomes of
term infants with post-asphyxia neonatal encephalopathy.Eur J Paediatr Neurol2009,13:224-234.
18. Badawi N, Dixon G, Felix JF, Keogh JM, Petterson B, Stanley FJ,et al:Autism following a history of newborn encephalopathy: more than a
coincidence?Dev Med Child Neurol2006,48:85-89.
19. Poole C:Low P-values or narrow confidence intervals: which are more durable?Epidemiology2001,12:291-294.
20. Burstyn I, Sithole F, Zwaigenbaum L:Autism spectrum disorders, maternal characteristics and obstetric complications among singletons born in Alberta, Canada.Chronic Diseases in Canada2010,30(4).
21. Dodds L, Spence A, Shea S, Fell DB, Armson BA, Allen AC,et al:Validity of autism diagnoses using administrative health data.Chronic Diseases in Canada2009,29(3):102-107.
22. McLachlan GJ, Krishnan T:The EM Algorithm and Extensions.JOHN WILEY & SON, INC; 1997.
23. Buchmayer S, Johansson S, Johansson A, Hultman CM, Sparen P, Cnattingius S:Can association between preterm birth and autism be explained by maternal or neonatal morbidity?Pediatrics2009,124: e817-e825.
level in an active smoker is uncertain.Nicotine and Tobacco Research
2009,11(6):670-678.
25. Newschaffer CJ, Cole SR:Invited Commentary: Risk Factors for Autism– Perinatal Factors, Parental Psychiatric History, and Socioeconomic Status. Am J Epidemiol2005,161:926-928.
Pre-publication history
The pre-publication history for this paper can be accessed here: http://www.biomedcentral.com/1471-2288/11/2/prepub
doi:10.1186/1471-2288-11-2
Cite this article as:Burstynet al.:Autism spectrum disorders and fetal hypoxia in a population-based cohort: Accounting for missing exposures via Estimation-Maximization algorithm.BMC Medical Research Methodology201111:2.
Submit your next manuscript to BioMed Central and take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution