Vol. 1, No. 2 (2013): 53-57 Research Article
Open Access
I
ISSSSNN::22332200--22224466
Thyroid peroxidase activity as toxicity target for
fluoride in patients with thyroid dysfunction
Swati Singla and Shashi A*
Department of Zoology, Punjabi University, Patiala- 147002, Punjab, India
* Corresponding author: Shashi Aggarwal, email: [email protected]
ABSTRACT
The present study aimed to assess the effects of drinking water fluoride (F) on the activity of thyroid peroxidase (TPO) enzyme involved in thyroid hormone synthesis. 840 fluorotic patients affected with thyroid hypo and hyper function and 140 euthyroid without fluorosis representing control were randomly selected from high endemic fluoride areas of Bathinda district, Punjab, India. The findings indicate significant (P<0.001) increase in the levels of serum F, urinary F and Urinary iodine (I) in fluorotic patients affected with thyroid disease. Significant (P<0.001) inhibition was recorded in activity of TPO in fluorotic patients with thyroid hypofunction and the activity was elevated in hyperthyroid fluorotic patients. Pearson’s bivariate correlation revealed strong positive correlation between water F and serum F (r= 0.98, P<0.01). Negative correlation existed between serum F vs TPO (r= -0.93, P<0.003), urinary I vs TPO (r = -0.95, P<0.002) and serum TSH vs TPO (r = -0.8876, P<0.001). The activity of TPO showed positive correlation with T3 (r = 0.963, P<0.01) as well as with T4 (r = 0.965, P<0.001). From the present study it may be concluded that the ingestion of drinking water with high concentration of fluoride leads to stress of the mechanism of biosynthesis of thyroid hormones, as evidenced by depletion in the activity of TPO, which may be produced by the attraction of fluoride with oxidized form of iodide and/or with the iodide site on the TPO molecule. This tends to decrease in concentration of T3, T4 and increase production of TSH in the serum.
Keywords:
Fluorosis, iodine, thyroid peroxidaseINTRODUCTION
Over the past decade there has been an increasing focus on the effects of hazardous chemicals on human endocrine systems. Exposure to specific environmental toxins has been shown to interfere with the production, transportation and metabolism of thyroid hormones (TH) by a variety of mechanisms or in modifying the metabolism of thyroid hormones. Environmental endocrine disruptors are exogenous substances that can interfere with TH synthesis, deiodinase function in peripheral tissues, proteins in the blood, and the agonistic or antagonistic actions of certain chemicals on target tissue receptors [1]. Fluorine containing compound have been listed among the most significant endotoxins that appear in natural environment as after effects of industrial activity of humans. The high cell membrane penetrating power, bioaccumulation, and biodegradable property of fluoride cause it to have a major impact on ecotoxicology [2].
The U.S National Research Council [3] states fluoride is an endocrine disruptor and has the potential to disrupt the function of many tissues that require iodine. Studies that have examined human populations with adequate intake of iodine have reported mixed results about fluoride’s ability to produce goiter [4]. The research has been more consistent, however, where the examined populations had either excessive iodine intakes [5], or deficient iodine intakes [6]. Thyroid disruptors can affect thyroid physiology in many phases of thyroid regulation. The complex system of iodine uptake, thyroid hormone production, interconversion of thyroid hormones and hormone degradation and elimination can be directly altered by thyroid disruptors [7].
The biosynthesis of thyroid hormone from thyroglobulin is catalyzed by thyroid peroxidase (TPO), an integral membrane protein. TPO is also a major
autoantigen in autoimmune thyroid diseases [8]. Alteration in the process of iodide organification has been detected in almost all thyroid diseases [9]. The qualitative abnormalities in the enzyme TPO system have been proved in patients with congenital thyroid diseases, and quantitative disturbances were observed in multinodular goiter, toxic adenoma, thyroiditis, and carcinoma [10].
In India, fluorosis from drinking water contamination due to fluoride is a major health problem. Fluoride is known to influence hormones at levels of action, including hormone secretion, activity and binding to target tissue [11,12]. Hence fluoride assay in biological fluid can be used as diagnostic and prognostic aid in patients with different hormonal disturbance living in fluoride endemic areas. It is important to determine whether long consumption of fluoride in drinking water can disrupt the activity of TPO. This study focused on TPO because it is an important factor in the TH axis and to correlate the interrelation of thyroid dysfunction and TPO activity during chronic fluoride toxicity.
MATERIALS AND METHODS
Subjects
860 fluorotic patients of both sexes in the age group 20-46 years (mean age 33.20-46 ± 10.42 years) were randomly selected from high fluoride endemic areas of Bathinda district, Punjab, India. Out of them 633 were suffering from hypothyroidism and 227 patients with hyperthyroidism 140 age and sex matched euthyroid control without fluorosis were included in the study. Institutional Human Ethical Committee approved this study.
Sample collection and preparation
Fasting venous blood samples were collected and centrifuged immediately at 3000 rpm for 10 minutes. Sera was separated and stored at -370C until analysis. First morning urine samples were collected for the analysis of urinary fluoride and iodine.
Estimation of fluoride and iodine
Fluoride content of drinking water, serum and urine samples was estimated with Orion ion selective electrode (EA940, Boston, MA, USA). The level of iodine in the urine was determined by the method of Dunn et
al. [13]. On the basis of water fluoride concentration five study groups were made viz; Control (0.76-1.00 mg/L), I (1.01-4.00 mg/L), II (4.01-8.00 mg/L), A-III (8.01-12.00 mg/L) and A-IV (12.01-16.00 mg/L).
Assay of thyroid peroxidase
Serum thyroid peroxidase activity was measured by Enzyme Linked Immunosorbent Assay (ELISA) using ABNOVA thyroid peroxidase (ELISA) kit (Biocheck, Inc. California).
Statistical analysis
The data were analyzed with Sigma Stat (SPSS, Inc., Chicago, IL, USA) using one-way ANOVA followed by post hoc Tukey’s Least Significant Difference (LSD) multiple comparison test. The fluorotic groups were compared individually with the control group. Association between variables was assessed by Pearson’s bivariate coefficient of correlation; p < 0.05 was considered significant.
RESULTS AND DISCUSSION
The concentration of urinary iodine (P<0.001) and fluoride was higher than that of euthyroid controls. The serum fluoride level was elevated significantly (P<0.01) in fluorotic patients. (Table 1).
One way ANOVA (F4,772 =79.795) followed by Post hoc Tukey’s LSD multiple comparison test revealed that the activity of TPO decreased significantly (q =0.16 to 0.26, 95% CI = -1.09 to 1.39, P<0.05 - 0.001, Fig. 1) in hypothyroid fluorotic patients among all study groups as well as when compared with control group. The maximum decline (44.8%) was observed in study group A-IV exposed to highest concentration of fluoride (12.01-16.00 mg/L).
The activity of TPO increased in fluorotic patients with thyroid hyperfunction. One way ANOVA (F4,366 = 11.374) with post hoc Tukey’s LSD multiple comparison test revealed that the activity of TPO elevated significantly (q = -0.14 to -0.02, 95% CI = -0.48 to 0.32, P<0.05 - 0.001, Fig. 2) in fluorotic patients compared with control group. The maximum elevation was noted in study group A-I exposed to 1.01-4.00 mg/L of fluoride. The activity of TPO declined among the fluorotic groups, as the fluoride content elevated.
Table 1. Concentration of fluoride (F) in drinking water and body fluids and urinary Iodine (I) in subjects of different study group
Study group
No. of patients
Water F Range (mg/L)
Mean water F (mg/L)
Serum F (mg/L)
Urinary F (mg/L)
Urinary I (µml/L)
Control 140 0.76 - 1.00 0.84 ± 0.19 0.02±0.004 0.89±0.23 2.58 ± 1.02
A-I 160 1.01 -4.00 3.02 ± 1.28 0.32±0.028a 3.68±0.53a 4.85 ± 1.24a
A-II 200 4.01 -8.00 6.95 ± 2.07 0.37±0.019ab 3.09±0.45a 5.49 ± 1.59 ab
A-III 240 8.01 – 12.00 10.18 ± 1.83 0.42±0.023abc 2.86±0.41ab 6.98 ± 2.03 ab
A-IV 260 12.01 – 16.00 13.67 ± 2.04 0.58±0.035abcd 2.23±0.32abc 8.56 ± 2.68 abcd
One way ANOVA with post hoc test (Tukey’s-LSD multiple comparison test ‘q’)
Figure 1. Mean serum activity of thyroid peroxidase (TPO) in control and fluorotic patients of thyroid hypofunction in different study groups
*Means designated with different letters abcd are significantly different, P < 0.05 – 0.001 among study groups
Correlation analysis
Pearson’s bivariate correlation showed significant positive correlation (r = 0.988, P<0.01) between water and serum fluoride. As the retention of fluoride in the body was increased, its excretion from the body through urine was declined and the elimination of iodine in the urine was increased. Urinary iodine and fluoride levels showed positive correlation (r = 0.43, P=0.08) which was statistically non-significant.
Figure 2. Mean serum activity of thyroid peroxidase (TPO) in control and fluorotic patients of thyroid hyperfunction in different study groups
*Means designated with different letters abcd are significantly different, P < 0.05 – 0.001 among study groups
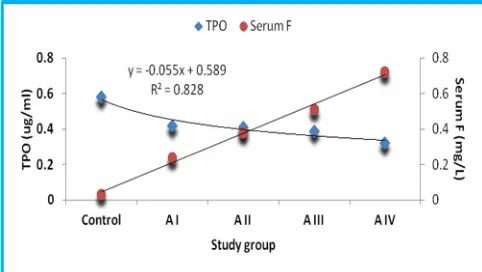
Figure 3. Correlation between Serum Fluoride and activity thyroid peroxidase (TPO) in different study groups
The activity of TPO exhibited an inverse relationship with serum F (r= -0.937, P<0.003, Fig. 3) in hypothyroid patients. However, in hyperthyroid patients, the activity of TPO exhibited positive statistically non significant correlation with serum F (r = 0.34, P= 0.86). There was negative correlation between urinary iodine and activity of TPO (r= -0.953, P<0.002, Fig 4) in different study groups. As the concentration of iodine in the urine was increased, the activity of TPO get depleted.
Serum levels of TSH and activity of TPO exhibited negative correlation (r= -0.876 P<0.001, Fig 5). The activity of TPO showed positive correlation with T3 (r = 963, P<0.01, Fig 6) as well as with T4 (r = 0.965, P<0.001, Fig 7). Regression analysis revealed that water fluoride being a strong predictor of alterations in serum F (y= 0.165x-0.119, R2= 0.991) and in activity of TPO (y= - 0.055x+ 0.589, R2= 0.828).
Figure 4. Correlation between Urinary Iodine (I) and activity thyroid peroxidase (TPO) in different study groups
Figure 5. Correlation between TSH and activity thyroid peroxidase (TPO) in different study groups
Figure 6. Correlation between T3 and activity thyroid peroxidase (TPO) in different study groups
Figure 7. Correlation between T4 and activity thyroid peroxidase (TPO) in different study groups
The activity of TPO in the hypothyroid patients was significantly (P<0.001) decline which could be due to destruction in thyroid tissue and replacement with fibroblast and lymphocyte. The clinicopathological findings in fluorotic patients affected with thyroid dysfunction showed various types of thyroid colloid adenoma and goiters [15]. The decrease of enzyme activity in the thyroid gland is somewhat intriguing considering the degree of tissue destruction which caused hypothyroidism [16].
Activity of TPO showed positive correlation with T3 and T4 levels in hypothyroid patients. As the activity of TPO was depleted, the level of thyroid hormones declined. But TPO activity has negative corelation with levels of TSH in fluorotic patients. Fluoride is a well-established TSH analogue, which explains the similarities in abnormal thyroid pathology with iodine deficiency. Not only may fluoride act like TSH in its absence, but it can also enhance TSH effects and alter the expression of G proteins [17] thereby influencing all aspects of iodine uptake, transport, and T4 to T3 conversion.
Defects of TPO are both quantitative and qualitative, the alterations include impaired binding to heme, thyroglobuline or iodine substrate, abnormal localization in the erythrocyte, and abnormal susceptibility to inhibition [18].
In the present study, the level of serum F and TSH was increased significantly (P<0.001). However, fluoride is known to inhibit the activity of Na+/K-ATPase and TPO in the thyroid gland [19]. The decreased activity of Na+/K-ATPase could adversely affect accumulation of iodide in the thyroid, which is opposite to stimulation of Na+/K-ATPase induced by hypothyroidism [20]. This effect might be due to accumulation of fluoride in the thyroid, directly inhibiting the Na+/K-ATPase [21] or the combined activity of fluoride and high TSH on activation of the protein kinase C, which decreases the activity of Na+/K-ATPase [22]. TPO is also an integral membrane protein that is present in the apical plasma membrane of thyroid epithelial cells, and is also under external TSH control through adenylate cyclase (AC)/cAMP activation [23]. Similar to TSH, fluoride at low levels stimulates AC and at higher doses inhibits AC [24].
Fluoride had significant effect on TPO activity, and decreases T3 and T4 levels and increases TSH. This disruption of TPO activity could be a sensitive TH end point for various concentrations of water fluoride. Several chlorinated POPs disrupt the TH axis, including polychlorinated biphenyls, polychlorinated dibenzo-p-dioxins, and dibenzofurans [25,26]. In animal studies, Boas et al. [27] reported that fluorinated compounds such as PFOS and PFOA also inhibited TPO activity in the rats, with reductions in T4 and T3.
The TPO activity in hyperthyroidism patients was significantly elevated in comparison with the control. One possible explanation for these findings could be that chronic TSH stimulation leads to increased iodide binding because of increased gland peroxidase content [28], increased iodide trapping, and presumably increased H2O2 generation [29] hence increase TPO activity [30].
CONCLUSION
From the present study it may be concluded that the ingestion of drinking water with high concentration of fluoride leads to stress of the mechanism of biosynthesis of thyroid hormones, as evidenced by depletion in the activity of TPO, which may be produced by the attraction of fluoride with oxidized form of iodide and/or with the iodide site on the TPO molecule. This tends to decrease in concentration of T3, T4 and increase production of TSH in the serum.
REFERENCES
1. Brar NK, Waggoner C, Reyes JA. et al. (2010). Evidence for thyroid endocrine disruption in wild fish in San Francisco Bay, California, USA. Relationships to contaminant exposures. Aqu Toxicol, 96 (3): 203–215. 2. Haque S, Pal S, Mukherjee AK. et al. (2012).
3. National Research Council. Fluoride in drinking water: a scientific review of EPA’s standards (2006). National Academies Press, Washington D.C
4. Burgi H, Siebenhüner L, Miloni E (1984). Fluorine and the Thyroid Gland: A Review of the Literature. Klin Wochenschr, 62 (12): 564-569.
5. Wang X (2001). Effects of high iodine and high fluorine on children’s intelligence and thyroid function. Chinese J Endemiol, 20 (4): 288-290.
6. Hong F, Cao, Y and Yang, D (2001). Research on the effects of fluoride on child intellectual development under different environmental conditions. Chinese Primary Health Care, 15: 56-7.
7. Miller MD, Crofton KM, Rice DC. et al. (2009). Thyroid-disrupting chemicals: interpreting upstream biomarkers of adverse outcomes. Environ Health Perspect; 117:1033-1041.
8. Dunn JT, Dunn AD (2001). Update on intrathyroidal iodine metabolism .Thyroid, 11 (5): 407-14.
9. Swain M, Swain T, Kumar MB (2005). Autoimmune thyroid disorders-an update. Indian J Clin Biochem, 20; 9-17.
10. Hasan HG, Mahmood TJ, Ismael PA (2011). Studies on the relationship between chromium(iii) ion and thyroid peroxidase activity in sera of patients with thyroid dysfunction. IBN AL- Haitham J Pure Appl Sci, 24 (2).
11. Susheela AK, Bhatnagar M, Vig K. et al. (2005). Excess fluoride ingestion and thyroid hormone derangements in children living in Delhi,India. Fluoride, 38: 98-108. 12. Shashi A, Singla S (2009). Thyroid function
derangements in patients of bathinda district suffering from fluorotoxicosis. Biosci Biotech Res Commun, 2(1): 65-70.
13. Dunn JT, Crutchfield HE, Gutekunst R. et al. (1993). Two simple methods for measuring iodine in urine. Thyroid, 3: 119–123.
14. Bachinskii PP, Gutsalenko OA, Naryzhniuk ND. et al. (1985). Action of the body fluorine of healthy persons and thyroidopathy patients on the function of hypophyseal-thyroid the system. Probl Endokrinol (Mosk), 31(6): 25-29.
15. Shashi A, Singla S, Sharma N (2009). Clinicopathological study of goiter in high fluoride areas of Bathinda district Punjab. Biosci Biotech Res Comm, 2(2): 155-161.
16. Masahiro S, Roy L, Harri L et al. (1984). Thyroid T4– deiodinase activity in normal and abnormal human thyroid gland. Metabol, 33 (4): 332-336.
17. Delemer B, Dib K, Saunier B. et al. (1991). Alteration of the functional activity of Gs protein in
thyrotropin-desensitized pig thyroid cells. Mol Cell Endocrinol, 75: 123-131.
18. Rapoport B, McLachlan SA (2001). Thyroid autoimmunity. J Clin Invest, 108:1253-1259.
19. Zhan X, Li AJ, Wang XM. et al. (2006). Effects of fluoride on growth and thyroid function in young pigs. Fluoride, 39: 95-100.
20. LeGrow AB, Fielding DC, Pressley TA (1999). Stimulation of Na/K-ATPase by hypothyroidism in the thyroid gland. J Endocrinol, 160: 453-60.
21. Murphy AJ, Hoover JC (1992). Inhibition of the Na/K-ATPase by fluoride. Parallels with its inhibition of the sarcoplasmic reticulum CaATPase. J Biol Chem, 267:16995-17000.
22. Bocanera LV, Krawiec L, Nocetti G. et al. (2001). The protein kinase C pathway inhibits iodide uptake by calf thyroid cells via sodium potassium-adenosine triphosphatase. Thyroid, 11(9): 813-817.
23. Gerard CM, Lefort A, Christophe D. et al. (1990). Distinct transcriptional effects of cAMP on 2 thyroid specific genes: thyroperoxidase and thyroglobulin. Horm Metab Res, 23:38–43.
24. Jenq SF, Jap TS, Hsieh MS. et al. (1993). The characterization of adenyl cyclase activity in FRTL-5 cell line. Chin Med J (Taipei), 51:159-65.
25. Boas M, Feldt RU, Skakkebaek NE. et al. (2006). Environmental chemicals and thyroid function.Eur J Endocrinol, 154: 599–11.
26. Song M, Kim YJ, Park YK. et al. (2012). Changes in thyroid peroxidase activity in response to various chemicals. J Environ Monit, 14: 2121-26.
27. Boas M, Feldt RU, Main KM (2012). Thyroid effects of endocrine disrupting chemicals. Mol Cell Endocrinol, 355: 240–48.
28. Nagataki S, Uchimura H, Matsuyama Y (1973). Thyrotropin and thyroidal peroxidase activity. Endocrinol, 92: 363-71.
29. Yamamoto K, DeGroot LJ (1974). Peroxidase and NADPHcytochrome c reductase activity during thyroid hyperplasia and involution. Endocrinol, 95:606-612. 30. Nataf BM, Fragu P, Othman SB (1978). Relationship
between peroxidase activity and serum TSH, T4 and T3, levels in rats in the course of iodine deficiency. Acta Endocrinol, 88:449-505.
*****
© 2013; AIZEON Publishers; All Rights Reserved