A B S T R A C T
Introduction
Although simplistic and one-sided explana-tions have been legion over the years, most theorists tend today to see addiction as a multi-factorial (bio-psycho-social) phenom-enon. Moreover, although few endorse the type of “vulgar constructionism” criticized e.g. by Best (1995), many agree that addiction is to some extent and in some sense a socially constructed problem. Thus West (2007), for example, contends that addiction is a social construct with fuzzy borders, yet a condi-tion in which many underlying pathologies and abnormalities become manifest. Put in a different way, even if addiction is not “just” an invention by powerful claims makers, the ways in which a “deviant” substance use or behaviour is defined, how such deviances are reacted to by society, and – thereby – the consequences to the individual of her/his deviance, as well as the long-term trajectory of her/his condition, are strongly influenced by norms and traditions that vary with time and place (Blomqvist 1998a). This means that addiction can be seen as an example of what Hacking (1999) has named “interactive kinds”,
J. Blomqvist: What is the worst thing you could get hooked on? Popular images of addiction problems in contemporary Sweden
AImS
To investigate potentially crucial aspects of Swedes’ perceptions of nine different addictions.
DATA AND mETHODS
Population survey, sent out to 2,000 adult Swedes (18–74 years), focusing on the perceived severity of, responsibility for, options to recover from, and character of addiction to cigarettes, snuff, alcohol, cannabis, amphetamine, cocaine, heroin, medical drugs, and gambling. RESULTS
There are large differences in the ways in which various addiction problems are perceived. Whereas tobacco use, and to some extent gambling, are seen as relatively harmless “habits”, not particularly easy to get hooked on but easy to quit, the use of drugs such as heroin, amphetamine, and cocaine is seen as a major societal problem, and users are seen both as “sinners” who need to mend their ways and as powerless “victims”. In between comes the use and misuse of alcohol, cannabis and medical drugs, about which perceptions are more divided. CONCLUSIONS
Respondents tend to downplay the risks and dangers with addictive habits that are common and familiar in mainstream culture, and to dramatise the risks and dangers with such habits that are
What is the worst
thing you could get
hooked on?
Popular images of
addiction problems in
contemporary Sweden
i.e. phenomena, the official and/or predominant definitions of which influence the self-definition and behaviour of those defined, thereby in turn at least partly confirming the official or institutionalised views.
Occasionally, the significance of others’ attributions and labelling for the origin and developmental course of various addictions, as well as for the options of finding a path out has attracted the attention of researchers, not seldom from a social historical perspective (e.g. Roman & Trice 1977; Gus-field 1981; Room 1985; Goldberg 2000). Others have found that dominating views that stigmatise the addict may pre-vent him/her from seeking help or lead to discrimination of ex-problem users in work life (Kilty & Meenaghan 1977; Dean & Rud 1984; Blomqvist 2002). There is also reason to contend that the long-term outcome of treatment is to a large part dependent on what happens outside the clinic door (e.g. Moos 1994; Blomqvist & Cameron 2002).
In Sweden, the clearly varying official discourses and policies on alcohol and narcotics are well known and well documented (e.g. Christie & Bruun 1985; Hübner 2001), and there are also indications that the Swedish “doxa”1 on
nar-cotic drugs, picturing these as almost inevitably dependence generating (Bergmark & Oscarsson 1988) may decrease other people’s inclination to offer help and support (Blomqvist 2004). People who recover from a heroin addiction seem also to be met with greater distrust than people who recover from an addiction to alcohol (Klingemann 1992; Blomqvist 2002). Moreover, the historical dominance, not least in the USA, of the “popular disease theory”, describing alcoholism as an inexorably progressive deteriorating process (cf. Pattison 1976), has been criticised by some as being directly counter-productive to the options of resolving an alcohol problem (e.g. Peele 1989). Finally, increasing research has shown in recent decades that “self-change” is by far the most common path to recovery from most addictions (e.g. Blomqvist 1996; Cunningham 2000; Klingemann & Sobell 2007; Blomqvist et al. 2007). Research on the processes and influences behind such solutions has clearly demonstrated the important role of other peoples’ support, demands, and general attitudes in motivating attempts to overcome an addiction, as well as in maintaining the resolution (e.g. Blomqvist 1999; 2002; Gran-field & Cloud 1999; Bischof et al. 2004).
uncommon or “strange”. This may have unfortunate consequences for addicts’ options to find a path out of their predicaments. KEy WORDS Addiction, images, consequences, population data, Sweden
Although there are thus clear indications that the “governing images” (Room 1978) or dominant “social representations” (Moscovici 1981; 1989) of, various addic-tions may play a not insignificant role to the prevalence and long-term course of these problems, as well as to the options of finding working strategies to counteract them, there is no conclusive and empiri-cally founded knowledge of how these at-titudes and images differ between e.g., various addictions, various cultures, vari-ous demographic subgroups, and varivari-ous professions. Rather, the current focus on the perceived need to develop “evidence based practices” tends to distract attention from what might be called “the social con-text of recovery”. Even if there is certainly good reason to improve the effectiveness and responsiveness of prevailing treat-ment systems (e.g., Humphreys & Tucker 2002; Blomqvist et al. 2007), this is un-fortunate, given that only a small propor-tion of all people with addicpropor-tion problems ever come into contact with these systems (ibid.). The study reported in this paper has been part of an effort to improve our knowledge about the “images of addic-tion” underlying how people with such problems are met by their environment, including professionals in the addiction treatment field, and so to lay a foundation for the development of more realistic strat-egies to counteract such problems.
“The social context of
recovery” – aims and research
questions
The research project “The social context of recovery
– views of addiction and
re-covery in the population and in various professional groups” has been financed bya grant from the Swedish Research Coun-cil (VR 2004–1831). The main objective of this project has been to get a better under-standing of the beliefs and assumptions underlying how people who are trying to overcome their addiction problems are met by treatment professionals and significant others. More concretely, the study endeav-oured to ascertain what people believe about nine different addictions or misuse problems occurring in Sweden (addictions to alcohol, cannabis, heroin, ampheta-mine, cocaine, medical drugs, cigarettes, snuff, and gambling). The main part of the project has been a fairly extensive survey, mailed out to a representative population sample. In a complementary part, three smaller surveys have been directed at three samples of about 200 professionals each, mainly working with addiction problems in each of the social services, health care, and criminal justice systems (cf. Samuels-son et al. 2009; Christophs 2009).
The study has partly built on the in-ternational so-called SINR study (Klin-gemann 2003)2, and the Swiss study on
popular attitudes toward “natural recov-ery” and about the key elements of a “self-change friendly society” that has been reported by Klingemann (2005; Klinge-mann & KlingeKlinge-mann 2007). Although the present study has broadened the scope of these studies, the latter study in particular provides valuable options for comparison regrading perceptions of self-change. Later studies conducted in Finland (e.g. Koski-Jännes et al. 2009), Canada (Cunningham 2009) and Russia, using basically the same questionnaire as the Swedish study pro-vide further possibilities for comparisons. Another source of inspiration has been a Nordic study on substance use and control
policies carried out in 1995 and reported e.g. by Hübner (2001), a study that also provides some data for comparison.
This article presents the results from the Swedish population survey, focusing on differences between the nine different ad-dictions with regard to how serious they are judged to be as societal problems, their perceived “addictiveness“, how easy they are believed to be to recover from (with and without professional or formally or-ganised help), to what extent moral re-sponsibility for developing and solving the undesired condition is attributed to the afflicted individual, and the perceived basic character of the problem in question.
Q Method
the survey
“Addiction”, “dependence”, and “misuse” are examples of the kind of “fat words”, the use of which Christie & Bruun (1969) lamented already four decades ago. It is obvious that much of the conceptual con-fusion from those days persists today, and that there are a number of dimensions and aspects that could be relevant when it comes to the exploration of prevailing images of various addictions. The delib-erations that underlie the choice of study variables for this investigation, has built on a number of previous efforts to improve our understanding of these issues. One ex-ample is Mäkelä’s (1980) remark that so-ciety’s response to any type of deviance will be affected by the extent to which the deviant individual is seen as doing harm to her/himself and/or to her/his environ-ment, and by whether effective means to alter the deviance are believed to be avail-able. Another has been Gusfield’s (1981) distinction between the moral connotation
of social problems, and their cognitive sig-nificance, and still another Brickman and colleagues’ (1982) assertion that the issue of moral responsibility for human prob-lems actually involves two questions: the question of blame (or responsibility for causing a problem), and the question of control (or capability and responsibility for solving a problem). Based on these and other considerations, the survey has tried to capture some dimensions and aspects of prevailing “images of addiction” that can be assumed to be crucial to how people with various addiction problems are met and treated by others in practice.
Data collection
The survey was mailed out by Statistics Sweden in 2005 to a representative popu-lation sample of 2,000 adult Swedes (18– 74 years) drawn from the official Swedish population data base (RTB). More con-cretely the questionnaire contained, be-sides questions about demographic and socio-economic circumstances, questions asking respondents to rank the “serious-ness” of various addictions compared to other social problems, questions about the perceived risk of developing an addiction to or dependence on the substances or activities chosen for the study, about the perceived responsibility for developing and resolving an addiction to these sub-stances or activities, and questions about the perceived chances of recovery – with and without treatment or other formal help – from the same addictions. In addition, information was gathered on respondents’ own experiences – by themselves or some-one close – of the use of or addiction to the substances/activities in question, of treat-ment and/or “self-change”, and of having
tried to help others with addiction prob-lems. Finally, a number of questions were included aimed at capturing respondents’ political
– ideological orientation, trust
in various authorities, “social distance” to people with addiction and other social problems, personal “locus of control”, and perceptions of major obstacles to recovery from and desirable societal strategies to counteract various addictions.Response rate and potential attrition bias Valid responses were provided by 1,098 respondents, giving a response rate of 54.6%. Although this is a low figure, it is not uncommon for surveys like the present one covering issues such as problem con-sumption of alcohol and use of illegal drugs (cf. Hague & Irgens-Jensen 1987; Kühlhorn et al. 2000; Hübner 2001). Attri-tion was somewhat lower among women than men, in the oldest age group (60–74) than among younger respondents, among respondents who were married or cohabi-tating than among singles, in the high-est income groups than in lower groups, among native-born Swedes than among people born in other countries, and among respondents with university education than among respondents with lower edu-cation. In an effort to account for sampling and attrition bias, data were weighted, using the mentioned variables and place of residence (rural, urban, or metropoli-tan) as calibration variables. All reported analyses except sample sizes are based on weighted data, although a number of test analyses showed few and insignifi-cant differences between results based on weighted and unweighted data. In spite of the weighting process, it must be born in mind that the validity of the results may
to a certain extent have been jeopardized by the low response rate. This means that caution is needed in generalizing results to the population level. Since problem drinkers and users of illegal drugs can be expected to be overrepresented among non-respondents, and socially “undesir-able” behaviour can generally be expected to be underreported (e.g. Kühlhorn et al. 2000), this caveat will be particularly rel-evant with regard to future analyses of the connections between respondents’ images of various addictions and their own expe-riences with potentially dependence gen-erating substances or activities. However, as concerns the differences between their images of various addictions, which is the focus of the present paper, the results are likely to be more reliable.
the respondent group
Table 1 describes the respondent group in terms of some basic demographic charac-teristics, showing e.g., an even distribution of women and men, that just under one third were university educated whereas a quarter had only completed elementary school, that one third lived in the metro-politan area and one tenth in rural areas, and that the great majority of the respond-ents were native-born Swedes.
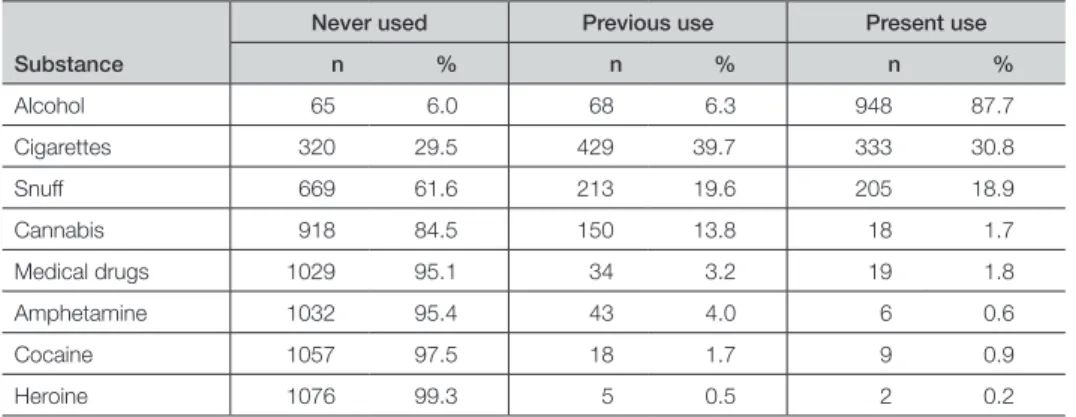
Table 2 describes respondents’ lifetime experiences with potentially addictive substances, which by and large seem to mirror the Swedish “addiction scene”3
fairly well, the most common experiences being, in order of magnitude, with drink-ing, smokdrink-ing, snuff use, and – although to a much lesser degree – cannabis use, and where experiences with amphetamine, co-caine, (illegal use of) medical drugs, and, in particular, heroin, are very limited. The
most obvious difference between respond-ents’ reports and what is known about the overall prevalence of the habits in ques-tion in Sweden, is that the proporques-tion of present smokers and snuff users seems to have been higher in the respondent group than what was the case in the population at the time when the survey was conduct-ed, although this difference may partly be due to differing definitions.
Table 3, finally, shows respondents’ re-ported experiences with addiction prob-lems, their own or those of somebody close (family or close friend). As can be seen, with the exception of dependence on tobacco, few admit to having
experi-enced such problems personally. For ex-ample, although more than nine out of ten are previous or present drinkers, only about six per cent, the same proportion as those who never drank, report having been addicted to or dependent on alcohol. The fact that more than four out of ten admit to being or having been dependent on to-bacco suggests that this is seen much less stigmatising than other addictions. At the same time, almost two thirds of all re-spondents report being aware of a present or former dependence or misuse problem in someone close. However, less than half of these respondents report that they per-sonally tried to help some of these people.
Table 1. Respondent characteristics
Women (N = 545) Men (N = 553) All (N = 1.098)
Characteristics n % n % n %
age 44.2 (s =15.5) 44.1 (s=14.8) 44.2 (s=15.7)
married /cohabiting 243 44 7 237 42.9 481 43.8
University education 175 32.2 147 26.5 322 29.3
only elementary education 126 23.2 148 26.7 274 25.0
living in a metropolitan area 197 36.2 163 29.5 360 32.8
living in a rural area 52 9.6 60 10.8 112 10.2
Born in sweden 467 85.7 466 84.3 933 85.0
Table 2. Personal substance use experiences (N = 1.098)a
Never used Previous use Present use
Substance n % n % n % alcohol 65 6.0 68 6.3 948 87.7 Cigarettes 320 29.5 429 39.7 333 30.8 snuff 669 61.6 213 19.6 205 18.9 Cannabis 918 84.5 150 13.8 18 1.7 medical drugs 1029 95.1 34 3.2 19 1.8 amphetamine 1032 95.4 43 4.0 6 0.6 Cocaine 1057 97.5 18 1.7 9 0.9 Heroine 1076 99.3 5 0.5 2 0.2
Finally, it should be mentioned that less than five per cent of all respondents reported personal experiences of addic-tion treatment, whereas one quarter was aware of a treatment episode experienced by someone close. About four out of ten judged these treatment experiences to have been helpful. At the same time, further analyses revealed that about one fifth of the respondents claimed to have quit what they saw as an addictive habit, predominantly smoking or using snuff, without treatment, and just over one third reported similar experiences in someone close. Data on respondents’ political-ide-ological orientation, “social distance” to people with addiction problems, personal “locus of control”, trust in various authori-ties etc. will be the object of future analy-ses, and are not presented here.
Q Some theoretical caveats
Besides the uncertainties caused by the low response rate, a few words are war-ranted about what can and what cannot be captured by asking respondents to re-port their attitudes to, and perceptions
of, rather complex matters by answering survey questions with pre-coded response alternatives. Thus, as pointed out by Hüb-ner (2001), the basic idea that there exists a “public opinion” that can be measured by traditional polls to representative samples is certainly open to debate (cf. Bourdieu 1972; Österman 1998). For example, there is no reason to believe that all respond-ents have the same competence in, or the same knowledge of, the issues covered by the survey (ibid., Hübner 2001). Further, it is important to consider that opinions in real life are created in interactions be-tween individuals and groups, and are formed in situations where taking a posi-tion means choosing between real groups that are in conflict (ibid.). This means that an opinion poll carried out at one certain point in time can only “scan the surface”, but not give an in-depth understanding of how opinions are mobilised, and what a certain standpoint means to various re-spondents (Österman 1998). In addition, the problem posed by a poll will always correspond to specific interests that gov-ern the meaning of the responses (ibid.). Respondent her/himself Somebody close Tried to help
somebody a Dependence to n % n % % alcohol 72 6.8 519 48.6 49.4 tobacco 448 42.3 575 55.1 42.7 Cannabis 23 2.1 149 14.2 56.7 Gambling 27 2.6 128 12.3 59.2 medical drugs 31 2,9 122 11.2 57.2 narcotic drugsb 12 1.2 135 13.0 59.9 any addiction 471 42.9 723 65.9 42.2
a) Percentage of all respondents who were aware of a problem by somebody close; b) Except cannabis
Table 3. Experiences of dependence/misuse problems in oneself and/or somebody close (N = 1.098)
These interests are not likely to be shared by all respondents, which means that it is not unproblematic to assign the same value and the same “meaning” to the same response by various respondents. Finally, attitudes and perceptions are not individ-ual characteristics but processes, governed by changing circumstances, actual events and various kind of information, which in turn means that connections captured by opinion polls may be rather casual (Öster-man 1998; Hübner 2001). Another general caveat is that the wording of questions and response alternatives may influence sur-vey results in a significant way, especially when the issues concerned are emotion-ally or ideologicemotion-ally “loaded”, something that can be said to be true at least about the drug issue in Sweden (Hübner 2001). Of special interest here may be that there is no obvious equivalent to the concept “ad-diction” in modern Swedish, and that the survey therefore consistently asked about “misuse of or dependence on” various sub-stances and behaviours. At the same time, “addiction”, “misuse”, and “dependence” are all “fat words” (cf. above), and in Swe-den the two latter could be expected to be used more or less interchangeably, by lay people and various “experts” alike, to sig-nify the same broad class of phenomena as the English term “addiction”. All in all this means that the results presented in this paper need to be interpreted and dis-cussed with regard to the currents of the “addiction scene” (see Note 3), and the dif-fering “instutionalised responses” to and media representations of matters like alco-hol, narcotic drugs, tobacco and gambling in Sweden (Hübner 2001)4. It also means
that the survey results should only be seen as an “aerial photo” of prevailing images
of or attitudes towards various addictions in contemporary Sweden. A fuller under-standing of the meaning of this “aerial photo”, warrants further analyses, explor-ing the connections between respondents’ images of various addictions, and e.g., their living situation, their own experi-ences in the field, their appreciation of the stigma attached to various addictions, and their political-ideological orientation. In addition, further inquiry will be needed into the processes by which respondents’ images of various addictions are formed.
Results
Based on the considerations discussed in the Methods section, the present analysis focuses on three basic dimensions of pre-vailing “images of addiction”: (a) the per-ceived severity of various addictions, (b) the attribution of moral responsibility for various addictions, and (c) the perceived “character” of various addictions. These three basic dimensions have, as will be seen, in turn be operationalised into more specific aspects. Even if the choice of as-pects has by necessity been somewhat ar-bitrary, the ambition has been to focus on what might be crucial to how people with various addiction problems are met and treated by others in practice.
Q Which is the “worst” addiction?
There are many ways in which the sever-ity of an addiction problem could be de-fined. On a societal level, severity could refer e.g. to the prevalence of the problem, the aggregate costs for the harm caused by addicts, or society’s efforts to prevent the problem and/or treat addicts. On an indi-vidual level, severity could refer e.g. to the stigma surrounding various addictions,
the “addictiveness” of (or the risk of get-ting “hooked” on) a certain substance or a certain habit, to what extent and how an addictive habit impairs the user’s mental and physical health and/or causes harm to the environment, as well as to how easy the addiction is to “cure”, and what it takes to do so. The survey has tried to capture at least some of these aspects, and in the analysis the relations between dif-ferent aspects have been explored in an effort to further clarify the significance of respondent’s judgements.
How dangerous are different addictions to society?
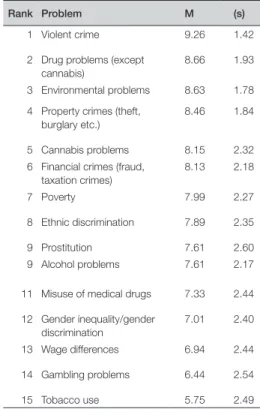
As mentioned in the discussion on opin-ion polls in the introductopin-ion, the fact that there may be wide differences in the ex-tent to which an issue concerns various re-spondents is crucial to the interpretation of their images of various drugs or activities. To gain some estimation of this, respond-ents were asked to rank fifteen such issues on a ten-point scale with the anchor-points “not severe at all” and “very severe”. The general outline of this question was bor-rowed from the Nordic survey reported by Hübner (2001), although some issues were added, and the wordings of some is-sues were changed. The exact wording of the question was (in translation): “How serious do you think that the following societal problems are on a scale from 1 to 10?” Table 4 shows respondents’ average ratings of the fifteen issues mentioned in the question.5
As can be seen, violent crimes end up in a class of their own as the most severe societal problem, followed by “hard” drugs6 and environmental problems, and,
in a separate class, crimes against
prop-Rank Problem M (s)
1 violent crime 9.26 1.42 2 Drug problems (except
cannabis)
8.66 1.93
3 Environmental problems 8.63 1.78 4 Property crimes (theft,
burglary etc.)
8.46 1.84
5 Cannabis problems 8.15 2.32 6 Financial crimes (fraud,
taxation crimes) 8.13 2.18 7 Poverty 7.99 2.27 8 Ethnic discrimination 7.89 2.35 9 Prostitution 7.61 2.60 9 alcohol problems 7.61 2.17
11 misuse of medical drugs 7.33 2.44 12 Gender inequality/gender discrimination 7.01 2.40 13 Wage differences 6.94 2.44 14 Gambling problems 6.44 2.54 15 tobacco use 5.75 2.49
note: Differences between groups of items are statisti-cally significant (paired samples t-tests of all subse-quent pairs of items; p < .05)
Table 4. Rated severity of various societal problems (scale 1 – 10; N = 1.098)
erty. Cannabis is ranked clearly below other narcotic dugs, together with finan-cial crimes and poverty, whereas all other addiction problems appear at the lower end of the ranking list. Alcohol problems, together with prostitution, are ranked be-low ethnic discrimination, but above the misuse of medical drugs, and gambling problems and tobacco use are ranked as the two least severe concerns among the available options, below gender discrimi-nation and wage differences. As indicated by the standard deviations, it also fol-lows from the fact that “hard” drugs are ranked close to the upper end of the scale, that there is fairly widespread consensus
among respondents about the severity of these drugs, whereas the opinions on the severity of, e.g. tobacco and gambling as societal problems are more divided. It is possible that the “high profile” of narcotic drugs as a societal problem should partly be seen as an effect of the fact that the sur-vey was mainly about addiction problems. However, this interpretation is contradict-ed by the fact that alcohol problems, the misuse medical drugs, gambling problems and tobacco all turn up at the end of the list. As claimed above, another dimension that may be important for the interpreta-tion of respondents’ images of different addictions is their personal acquaintance with various substances and activities. Albeit these relations will be the object of future, separate analyses, this suggests that the low ranking of tobacco use as a so-cietal problem should be seen in the light of the fact that tobacco dependence seems to be surrounded by less stigma than other addictions (cf. above). In addition, since respondents were explicitly asked to rank the severity of the fifteen issues as societal
problems, it is also important to consider the way in which such problems are of-ficially defined and handled, which may influence people’s attitudes towards espe-cially such issues with which they have little personal experience. Thus, respond-ents’ ratings of the severity of narcotic drugs should most likely to a large extent be seen as reflections of the strong official stance in Sweden against any use of these drugs, and the fact that objections to this policy have been more or less banned in the media (cf. Note 1).
Although the two studies are not totally comparable, it is also fairly obvious that opinions have not changed much since
1995, when the study reported by Hübner (2001) was carried out. Thus, drug prob-lems ranked next to violent crimes in the previous study, too7, whereas both alcohol
problems and smoking ranked relatively low8. The most obvious difference seems
to be that prostitution, which ranked low-est among men and third lowlow-est among women in 1995, has “moved up the scale”, which may be due to the relatively large media attention during the past decade to the issue of “trafficking” and to the change in the legislation in this area in 1998, that made buying sex a crime. In addition, cannnabis, which was not distinguished from other narcotic drugs in the previous survey, may in reality have moved down-ward on the severity scale. One might per-haps also have expected that the changes in alcohol policy that followed Sweden’s accession to the EU in 1995, and the sub-sequent, rapid and large increase in con-sumption (e.g. Leifman 2004; Boman et al. 2007) should have reflected in alcohol problems moving “up the scale”. That this is not the case may partly be explained by most respondents making a clear distinc-tion between “normal drinking” and “al-cohol problems”, partly by the fact that the recent increase in drinking seems, un-like the simultaneous increase in Finland, so far to have had fewer negative conse-quences than might have been expected (e.g. Norström & Ramstedt 2006).
Perceived severity of various addictions at the individual level
Another crucial aspect of the “dangerous-ness” of various substances or activities concerns the risk for individual users of “getting hooked”. To get a grasp of this aspect respondents were asked, using a
four-point scale9 to rate the perceived risk
of developing a dependence or misuse if experimenting with each of the nine sub-stances or activities included in the study. As touched upon in the introduction, one of the reasons for setting the study up was the experience that people’s success in try-ing to recover from various addictions is influenced not least by whether they are met with trust and support or with dis-trust and repudiation by others – family and friends as well as professionals. Thus, respondents’ “change optimism” in this sense can be claimed to constitute another crucial aspect of the perceived severity at the individual level of a certain addiction. To asses this, respondents were asked to rate the perceived probability for recovery from various addictions – with and with-out the help of professional or formally or-ganised treatment – including mutual help groups such as AA, NA etc. These prob-abilities were rated on a five-point scale,
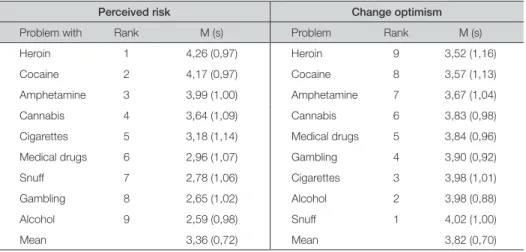
ranging from “no or very little probability” to “very high probability”. Table 5 shows the ranks and mean ratings for the risk of getting hooked on, and the overall options of recovery from, the nine addictions in questions. For all addictions, except snuff, the overall options of recovery meant the rated probability of finding a path out with
treatment (see further below).
As can be seen, there is, by and large, an inverse relation between respondents’ views on which addictions it is easiest to “get into” and “get out of”. Thus, the “hard” drugs (heroin, amphetamine, and cocaine) are not only seen as a large so-cietal problem, but also as highly addic-tive and very difficult to quit. At the other end of the scale, drinking, gambling, and snuff are seen as much less dependence generating, and as relatively easy to quit, should an addiction develop. Cannabis and medical drugs are allotted middle ranks in all these respects, whereas
ciga-Table 5. Overall perceived risk of becoming addicted and overall “change optimism” (scales 1–5; N = 1.098)
Perceived risk Change optimism
Problem with Rank m (s) Problem Rank m (s)
Heroin 1 4,26 (0,97) Heroin 9 3,52 (1,16)
Cocaine 2 4,17 (0,97) Cocaine 8 3,57 (1,13)
amphetamine 3 3,99 (1,00) amphetamine 7 3,67 (1,04)
Cannabis 4 3,64 (1,09) Cannabis 6 3,83 (0,98)
Cigarettes 5 3,18 (1,14) medical drugs 5 3,84 (0,96)
medical drugs 6 2,96 (1,07) Gambling 4 3,90 (0,92)
snuff 7 2,78 (1,06) Cigarettes 3 3,98 (1,01)
Gambling 8 2,65 (1,02) alcohol 2 3,98 (0,88)
alcohol 9 2,59 (0,98) snuff 1 4,02 (1,00)
mean 3,36 (0,72) mean 3,82 (0,70)
note: Regarding responsibility for causing the problem, differences between subsequent pairs of problems are significant except for cigarettes – gambling, cannabis – amphetamine, and cocaine – heroin – alcohol (paired samples t-tests, p < .05); regarding responsibility for solving the problem, all differences between all subsequent pairs of problems are significant.
rettes are rated as moderately addictive, although smoking is judged as fairly easy to quit. The small standard deviations also indicate that there is relatively good agree-ment between respondents both concern-ing the high risk of gettconcern-ing “hooked” on the “hard” drugs and the fairly low risk of getting “hooked” on alcohol and gam-bling. Concerning rated options on finding a path out of the addiction, standard devi-ations indicate fairly good agreement that it is relatively easy to successfully treat drinking and to some extent gambling problems, whereas opinions seem to be more divided regarding the same options when it comes to “hard” narcotic drugs.
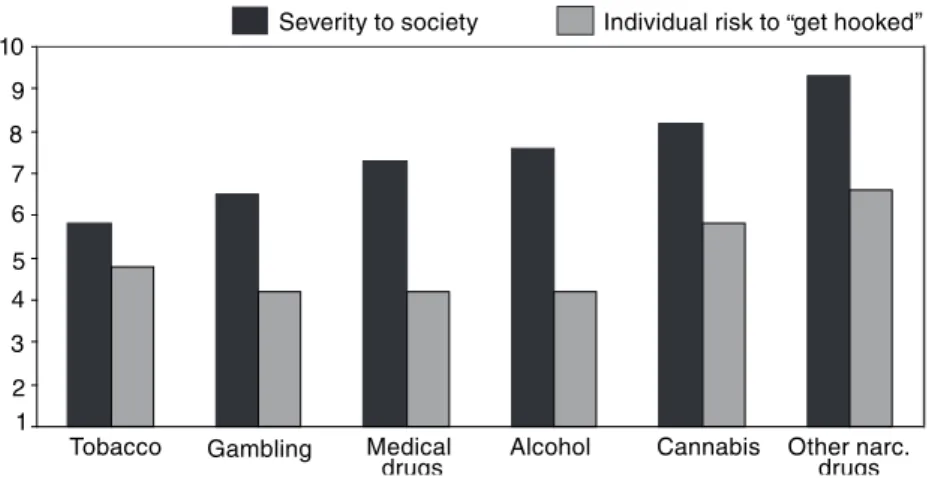
Harm to whom? Perceived severity at the societal and individual levels compared. How is the perceived dependence-gener-ating capacity of various substances/be-haviours related to how serious they are judged to be as societal problems? To shed light on this relation, the two ratings10 have
been brought together in Figure 1.
As shown in the figure, the perceived “dangerousness” at the societal and indi-vidual levels seem to converge regarding “hard” narcotic drugs and to some ex-tent cannabis, in the sense that these ad-dictions are judged to be the most severe ones on both levels. However, gambling, and the misuse of medical drugs and al-cohol are all seen as more severe societal problems than tobacco use, although the latter is judged to be stronger dependence generating. Whereas respondents’ ratings of the “addictive potential” of various sub-stances and activities seems to fit fairly well with what at least some researchers have claimed (cf. West 2007), the ratings of their severity to society fit rather poorly with what is known about e.g. the preva-lence and aggregate costs to society of vari-ous such problems in Sweden (cf. Note 3). This strengthens the assumption that these ratings to a large part represent the official stance on and the prevailing media image of these problems, and that there is a strong relation between the perceived
1 2 3 4 5 6 7 8 9 10
Tobacco Gambling Medical
drugs Alcohol Cannabis
Individual risk to get hooked„ Severity to society
Other narc. drugs „
“strangeness” of various problems and the extent to which they are seen as dangers to society (cf. above; Christie & Bruun 1985).
Change optimism and confidence in treatment
As already noted, respondents were asked to rate the probability for recovery from the nine addictions both without professional or formally organised help (“self-change”) and with such help. Based on these rankings, Figure 2 shows the perceived probability for “self-change”, and what treatment is as-sumed to be able to add in finding a solution.
As can be seen, the perceived options to quit without professional or formally organised help are high concerning tobac-co use and to some extent gambling, and lowest concerning “hard” narcotic drugs of which few Swedes have personal expe-rience (cf. Note 3 and Table 3). A closer analysis reveals that only eleven percent of the respondents believe that a heroin addict has any chance at all of finding a resolution on her/his own, whereas the same proportion for snuff use is close to seventy-five per cent. With the exception
of tobacco use, the figure also indicates that Sweden is rather far from being the type of “self-change friendly society” that for example Klingemann (2005; Klinge-mann & KlingeKlinge-mann 2007) has argued for. Rather, respondents’ views of the options for self-change seem far more pessimistic than topical research about the prevalence for such solutions can be claimed to give grounds for (Klingemann & Sobell 2007; Blomqvist et al. 2007). In fact, if the scale used in the figure should be transformed to a percentage scale, it would mean that, besides tobacco dependence, the rated probability for self-change would vary be-tween about twenty (heroin addiction) and slightly below fifty per cent (gambling). This should be put in the perspective of topical research, indicating that the large majority of recoveries from dependence not only on alcohol, but also on most nar-cotic drugs, take place outside the treat-ment system (e.g. Blomqvist 2009).
On the other hand, the figure also indi-cates that this pessimism is to a large ex-tent compensated for by a strong general confidence in the effectiveness of
addic-Snuff Cigarettes Gambling Alcohol Cannabis Cocaine Heroin 1 2 3 4 5 With treatment Self-change Amphe-tamine Medical drugs
tion treatment, where type of addiction does not seem to matter much. Thus, whereas the probability for a successful outcome of treatment of alcohol prob-lems, using the transformed scale, would be set at about seventy-five per cent, the corresponding probability for treatment for amphetamine misuse would be set at almost seventy per cent. The figure also shows that the relative importance of ex-pert help, i.e. the difference between the rated probabilities for recovery with and without treatment, is consequently judged to be larger for the “hard” drugs (heroin, amphetamine, and cocaine) than for e.g., addiction to alcohol and cannabis11, and to
be more ore less non-existent for depend-ence on tobacco (and even negative for snuff). By and large, this may be said to reflect the current situation in the addic-tion field in Sweden, where more energy and, in relative terms, more resources are spent on treating a rather limited number of drug addicts, than on treating a much larger number of problem drinkers and al-cohol misusers (cf. Blomqvist 2002; Mel-berg 2006), and where treatment of smok-ers and snuff ussmok-ers is rare12.
It is not self-evident how to interpret re-spondents’ high confidence in addiction treatment. Potentially, it could be seen as an indication of a generalised strong trust in (or at least nostalgia concerning) the benevolent welfare state (cf. Rothstein 1994) and/or as mirroring the promises of increasingly “effective cures” (mainly of a medical kind) that are recurrently report-ed by the mreport-edia (cf. Note 4). Whereas no final conclusions can be drawn from the fact that studies in Finland (Koski-Jännes et al. 2009) and Canada (Cunningham 2009) show a similar strong trust in
addic-tion treatment, further comparisons with studies in countries with less developed welfare ambitions may resolve this issue with time. The fact that both Canadian and Swiss respondents (Cunningham 2009; Klingemann & Klingemann 2007) are clearly more optimistic about the options for self-change from problematic cannabis use than Finns (Koski-Jännes et al. 2009) and Swedes, and the fact that Finns rate alcohol as a much larger societal problem than Swedes13, certainly shows that views
and attitudes differ between countries and contexts. In sum, however, respondents’ ratings on the severity, “addictiveness”, and options to “get out of” various addic-tions, rather clearly suggest that the less common and familiar – to the common citizen or in mainstream culture – a habit or a substance is, the “worse” – in most aspects – it is judged to be.
Q Who is responsible? The moral aspect
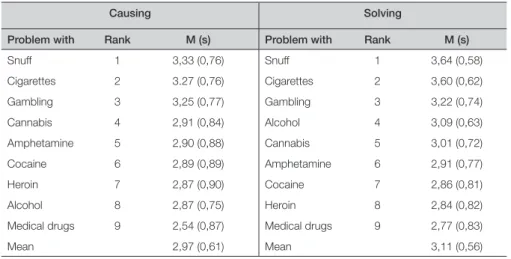
As mentioned, drawing on the work of Brickman et al. (1982) respondents were also asked to what extent they ascribed the responsibility for causing, as well as for solving the nine addiction problems to the single individual. The answers to these two questions are displayed in Table 6.
As shown by the high means in the first column of the table, addiction problems seem largely to be seen as the individual’s own fault. At the same time, there is a tendency that the more severe an issue is rated to be as a societal problem (cf. Ta-ble 4), the less likely the individual suf-ferer is to be blamed for having caused the problem. However, there seems to be two exceptions to this. Thus, the group of ad-dicts who are to the greatest extent seen as “victims” are those addicted to medical
drugs. In addition, problem drinkers are on the average blamed less for their condi-tion than are users of at least cannabis and amphetamine. A possible explanation is, in the first case, that the misuse of medi-cal drugs is seen to have been “created” by doctors or by the health care system who should therefore also take responsibility, whereas in the other case the results might be a reflection of repeated claims – from different parties with differing agendas14 –
that alcoholism is a “disease”.
As regards the responsibility for solving an addiction problem, respondents seem to put even greater pressure on the single individual, a fact that could at the same time and in some sense be said to refute the assumption of a widespread disease notion of addiction. Since this question asked whether the responsibility for solv-ing a problem should rest primarily with the individual or society, it should be pointed out that the high means do not
necessarily imply that the majority view is that society is not obliged to offer help, but rather that the main responsibility for solv-ing the problem lies with the individual client or patient, whether she or he is in treatment or not. Thus the majority stance should probably be interpreted according to the common view that you cannot help someone to quit an addiction, unless she or he really wants to do so. The rankings of various addictions are again, with the partial exception of the misuse of medical drugs, clearly related to their perceived “dangerousness” as social problems, mak-ing the individual the more responsible for the solution the less severe and/or the less risky a certain substance use or activ-ity is considered to be. However, the main impression from the data shown in Table 6 is that the blame for developing an addic-tion, as well as the responsibility for find-ing a path out is to a large extent attributed to the single individual.
Table 6. Degree to which the individual is deemed responsible for causing and solving the problem (scale 1– 4; N = 1.098)
Causing Solving
Problem with Rank M (s) Problem with Rank M (s)
snuff 1 3,33 (0,76) snuff 1 3,64 (0,58) Cigarettes 2 3.27 (0,76) Cigarettes 2 3,60 (0,62) Gambling 3 3,25 (0,77) Gambling 3 3,22 (0,74) Cannabis 4 2,91 (0,84) alcohol 4 3,09 (0,63) amphetamine 5 2,90 (0,88) Cannabis 5 3,01 (0,72) Cocaine 6 2,89 (0,89) amphetamine 6 2,91 (0,77) Heroin 7 2,87 (0,90) Cocaine 7 2,86 (0,81) alcohol 8 2,87 (0,75) Heroin 8 2,84 (0,82)
medical drugs 9 2,54 (0,87) medical drugs 9 2,77 (0,83)
mean 2,97 (0,61) mean 3,11 (0,56)
note: Regarding responsibility for causing the problem, differences between subsequent pairs of problems are significant except for cigarettes – gambling, cannabis – amphetamine, and cocaine – heroin – alcohol (paired samples t-tests, p < .05); regarding responsibility for solving the problem, all differences between all subsequent pairs of problems are significant.
Q What kind of problems?
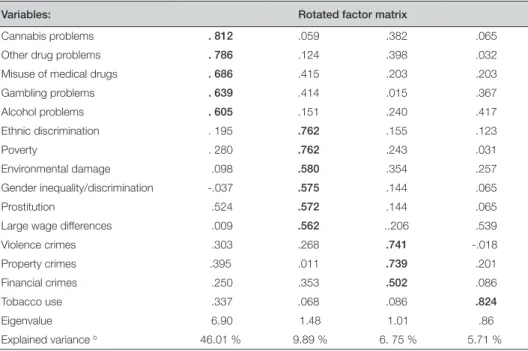
Although the choice of dimensions and aspects in trying to capture the prevail-ing popular images of various addictions, has – as already mentioned – by neces-sity been somewhat arbitrary, the analyses presented so far could be claimed to have given a reasonably coherent and meaning-ful result. There are, however, still some aspects that might be added to provide a more comprehensive understanding of the ways in which the percieved characters of various addictions diverge. One means for such an understanding would be to ex-plore how respondents’ perceptions of the severity of various addictions are connect-ed to each other, and to their perceptions of the severity of other social problems (cf. Hübner 2001). To this end, a factor analy-sis was conducted, using the data shown
in Table 4. As can be seen in Table 7, a four-factor solution in this analysis result-ed in a set of quite distinctive dimensions, explaining a fairly large proportion of the total variance.
The first factor can clearly be interpret-ed to represent an addiction or misuse problems factor with high loadings for the “traditional” addictions, as well as for gambling and to some extent prostitution. The second factor can be interpreted as a “social/political” factor, with high load-ings for issues that concern social and eco-nomic justice, gender and ethnic discrimi-nation, and environmental protection. The third factor stands out as a relatively distinctive “crime factor” with high load-ings for all of the, rather different types of, crimes that were included in the question. Finally, the analysis discerns “tobacco
Variables: Rotated factor matrix
Cannabis problems . 812 .059 .382 .065
other drug problems . 786 .124 .398 .032
misuse of medical drugs . 686 .415 .203 .203
Gambling problems . 639 .414 .015 .367 alcohol problems . 605 .151 .240 .417 Ethnic discrimination . 195 .762 .155 .123 Poverty . 280 .762 .243 .031 Environmental damage .098 .580 .354 .257 Gender inequality/discrimination -.037 .575 .144 .065 Prostitution .524 .572 .144 .065
large wage differences .009 .562 ..206 .539
violence crimes .303 .268 .741 -.018 Property crimes .395 .011 .739 .201 Financial crimes .250 .353 .502 .086 tobacco use .337 .068 .086 .824 Eigenvalue 6.90 1.48 1.01 .86 Explained variance b 46.01 % 9.89 % 6. 75 % 5.71 %
a) varimax rotation; b) total explained variance: 68. 4 %
use”, as an own – but as also indicated in Table 4, not particularly important – di-mension in Swedes’ apprehension of so-cial problems.
It can be noted that a similar analy-sis conducted on data from the above-mentioned Nordic survey (Hübner 2001), yielded three dimensions, represent-ing a “moral”, a “social/political”, and a “crime” factor, where smoking problems were grouped together with alcoholism, drug abuse, and prostitution in the first factor. The main difference is thus that to-bacco use here appears as a separate fac-tor, something that may to some extent be due to the fact that the two studies used partly different items and different word-ings (cf. above)15. In sum, this analysis can
be claimed to suggest that the public dis-course on addiction problems in Sweden is largely separated from the political dis-course, and that a distinction is also made, even if the border is somewhat blurred, between “addictions proper” (most clearly represented by heroin and other “hard” drugs) and “bad habits” (most clearly rep-resented by snuff use and smoking).
Another way of trying to summarise the perceived “character” of various addic-tions would be to apply to them the four “models of helping and coping”, deline-ated by Brickman’s and colleagues (1982). As already mentioned, these authors claim that the attribution of moral responsibility for human and/or social problems involves not one but two basic dimensions, namely the question of blame (“who caused he problem”) and control (“who is capable of and responsible for solving the problem”). By combining these two dimensions, they arrive at what they refer to as four “mod-els” of how a certain problem could and
should be handled. According to the “moral model” people are held responsi-ble for creating a proresponsi-blem as well as capa-ble of and responsicapa-ble for solving it, which means that help essentially takes the form of punishments and rewards. According to the “treatment model” (or perhaps rather the “expert model”) on the other hand, problems are seen as caused by forces beyond the subject’s own control, and as curable only by professional experts. By and large these two models correspond to the “badness-illness” dichotomy that has often been used to illustrate different ways of looking at addiction problems (cf. Mäkelä 1980). To this common figure of thought, the authors add the “enlighten-ment model”, according to which people are blamed for having caused their prob-lems, but are at the same time seen as inca-pable of solving them. As a consequence, the subject’s best hope for a solution lies in submitting to a higher moral authority that can help her or him to overcome their destructive impulses. Since this author-ity could obviously be both of a spiritual and a profane character, “fostering” might in fact be a better name for this model (cf. Blomqvist 1998b16). Finally, in the
“com-pensatory model”, people are seen as subjected to certain handicaps or obsta-cles imposed on them by the situation or by nature but as basically capable of and responsible for managing their own lives. Accordingly, they may be entitled to cer-tain help, given on their own terms, and aimed at empowering them to solve their own problems and manage their own lives on the same terms as other citizens.
Previous research suggests that the dis-tinctions suggested by Brickman et al. (1982) may be more fruitful when applied
in e.g., overarching socio-historical analy-ses (cf. Blomqvist 1998b), than in clinical contexts (e.g. West & Power 1995), and it is not self-evident how the four models could and should be operationalised, using the survey questions. One option would be to dichotomize the two questions on respon-sibility for causing and solving various problems, the answers to which are shown in Table 3. However, as indicated by the same table, that would obviously mean that a large majority of the respondents would be claimed to apply the “moral” model to all addictions, a result that does neither stand out as particularly meaning-ful nor as particularly informative in the present context. Further, as already indi-cated, the wording of the question on re-sponsibility for solving various problems was not ideal, asking respondents to rate to what extent this responsibility should be put on the individual or on society. Fi-nally, the “control” dimension in the work of Brickman et al. (1982) seems on closer scrutiny to be at least as much about the capacity to solve a problem as about the
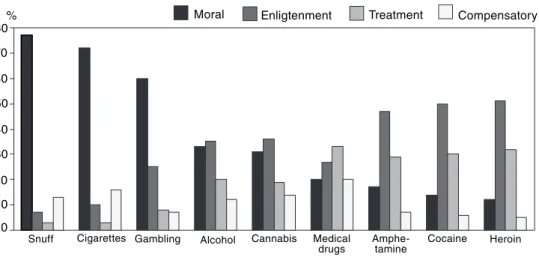
responsibility for doing so. Therefore, the rated responsibility for developing various addictions has here been combined with the rated options for “self-change” from the same problems17. The resulting
distri-bution of preferred “models for helping and coping” over the nine addictions is shown in Figure 3.
When interpreting this figure, it should first be noted that with the operationali-sation used, it follows from respondents’ ratings of the individual as largely respon-sible for acquiring an addiction (Table 6), that the “moral” and “enlightenment/ fostering” models are overall more com-monly endorsed than the “compensatory” and “treatment/expert” models. This said, it should be noted that respondents seem to apply different models for different ad-dictive substances or activities. At one end of the scale, tobacco use (snuff and ciga-rettes), and to some extent gambling, are predominantly seen as “moral concerns” or “bad habits”, in the sense that both starting and terminating these activities is predominantly seen as the individual’s
0 10 20 30 40 50 60 70 80% Moral Enligtenment
Snuff Cigarettes Gambling Alcohol Cannabis Amphe- Cocaine Heroin
tamine Medical
drugs
Treatment Compensatory
own business. At the other end of the scale is the use of “hard” drugs (heroin, cocaine, and amphetamine), where opinions are more divided, but where the “enlighten-ment” and “treat“enlighten-ment” models, both im-plying that the individual needs external help to overcome her/his predicament, and that the addict should be seen either as a “sinner” or a “crook” who needs help to mend his/her ways, or a powerless “vic-tim” who needs expert treatment, clearly predominate. In a “middle group” are ad-dictions to alcohol, cannabis and medi-cal drugs, where opinions are even more spread, but where the “compensatory” model gets more “votes” than it gets with regard to the “hard” narcotic drugs.
The fact that tobacco dependence stands out from the other addictions as being al-most exclusively seen through the eyes of the “moral model”, is in line both with the fact that this seems to be a fairly common and mundane experience (Table 3), as well as with the fact that tobacco use is ranked low as a societal problem (Table 4), and is singled out as an “own” dimension in the factor analysis (Table 7). In addition, it suggests that respondents’ assessments of the severity and character of tobacco use pay little attention to matters such as mortality, morbidity, and harm to others. Together, these data rather suggest that smoking and snuff use, in spite of recur-rent campaigns pointing to tobacco as a large public health problem, are predomi-nantly seen as “private” as opposed to either moral or political concerns in con-temporary Sweden.
The figure also indicates that legal sub-stances or activities are to a greater extent seen as moral matters than are illegal sub-stances – cannabis being a partial
excep-tion here. The fact that the enlightenment or “fostering” model is the one most en-dorsed by respondents concerning both al-cohol and narcotic drugs may partly have to do with the growing popularity of, and media attention to, AA, NA and other mu-tual help groups (cf. Note 4), partly with the fact that coercion has always been – and is probably been seen by most – as an integral part of society’s efforts to counter addiction problems. The relative unpopu-larity of the “treatment (or expert) model”, in spite of respondents’ strong confidence in the treatment system (see Figure 2), can perhaps be seen in the same light.
In sum, the results presented above may be claimed to hint that respondents down-play the severity of and risks with hab-its and conditions with which they have some – direct or indirect – personal experi-ence and/or which are seen as part of main-stream culture, whereas problems that are more uncommon or “alien” are perceived as more severe or dangerous. In addition, the former problems seem to be regarded as more “private” and to a larger extent as the individual’s own business, whereas users of “hard” drugs in particular are seen as be-ing both a threat to society and as victims of powers stronger than themselves.
Discussion
This article presented analyses of data from a survey aimed at capturing prevail-ing popular images of nine different ad-dictions in contemporary Sweden. The results show that these images vary greatly between different addictions, and in a fair-ly consistent way. These differences seem to have little to do with known facts about either the prevalence of different addic-tion problems, their harmful and
hazard-ous effects on user’s health and wellbeing, or their “costs” to society in the form of premature deaths, health care expendi-ture, lost years in work life, or potential harm to others. Rather, the popular images of various addictions seem to a large extent to reflect beliefs of a rather “ingrown” and stereotypical character. This is true above all as concerns respondents’ images of the “hard” narcotic drugs (amphetamine, cocaine, and heroin), which are clearly in line with the basic conceptions which have been used to justify Sweden’s tradi-tionally very restrictive drug policy, de-picting narcotic drugs as extremely dan-gerous and poisonous, with the capacity to quickly enslave every user, and almost impossible to quit (cf. Bergmark & Oscars-son 1988), a picture that has also recur-rently been reproduced by the media (cf. Hübner 2001). At the other end of the con-tinuum are the images of some relatively mundane and familiar “habits” – smoking, using snuff, and to some extent gambling – the dangers and addictive character of which seem rather to be played down by the respondents. In between come addic-tions to alcohol, cannabis, and medical drugs, about the severity and character of which there seems to be less consensus in popular thinking, perhaps due to the fact that rather divergent views on these issues have come to light repeatedly over the years, also in the media (cf. Hübner 2001; Blomqvist 2004).
The fact that respondents largely at-tribute the responsibility for the devel-opment of addictive problems, as well as the responsibility for solving them to the individual, may seem surprising, not least considering the fact that survey answers reflect a generally strong confidence in
the addiction treatment system and its po-tential benefits. One possible explanation may be that “treatment” of these problems is not mainly thought about in terms of, “expert” or “professional”, specific inter-ventions, but as much – in line with what the media tend to pay attention to in this area – in terms of AA, NA or other mutual help groups, backing up people who have made a decision to quit, and/or in terms of coercive care, exerting external control to make them do so.
Since “self-change” is today known to be the most common path out of many ad-dictions (e.g., Klingemann & Sobell 2007), and since supportive and encouraging, al-though not undemanding, social networks have been found to be crucial in such proc-esses (e.g., Blomqvist 1999; 2002), it can be deemed unfortunate that so few of the respondents endorse what Brickman et al. (1982) term the “compensatory model”, which guarantees the individual the nec-essary support, but without putting blame on her/him for their distressing condition, and without expressing scepticism or dis-trust. This is the more regrettable given that only a minority of the respondents who had reportedly experienced an addic-tion problem in someone close, actually had offered any personal help.
It is also tempting to dwell on the fact that dependence on smoking and snuff in particular are more often seen as “bad hab-its” than as “real addictions” or “diseas-es”, and to relate this to the fact that smok-ing has decreased substantially in Swe-den during the past two decades, largely due to “rational” reactions to measures such as information on health risks, price policy and, in particular, rendering smok-ing more difficult and more expensive.
Since earlier studies have shown that the adoption of a “disease notion” of alcohol problems may in certain respects function as a self-fulfilling prophecy, one might wonder whether a de-stigmatisation and wider acceptance of a view of substance use problems as a “central activity” in the subject’s way of life (Fingarette 1988) or as “lifestyles leading to predicaments” (Drew 1989), might not increase addicts’ options of cutting loose from their addiction (cf. Blomqvist 1998a; Blomqvist & Cameron 2002). This may also have a bearing on the present new wave of “bio-medicalisation” of addiction problems, proclaiming these problems to be “diseases of the brain” (see, e.g. www.hjarnfonden.se), a tendency that may thus in a longer run not necessarily prove to be particularly productive to ad-dicts’ options for finding a path out.
However, it needs to be pointed out that there are a number of study limitations that imply that these conclusions should be regarded as tentative. First, the relative-ly low response rate means that generalisa-tions need to be made with caution, even if attrition bias does not seem to be a major problem. Secondly, as has already been pointed out, a survey of this kind can only “scan the surface” when it comes to peo-ples’ conceptions and beliefs about vari-ous addictions. For example, the way in which this study was been conducted has not left room for more nuanced statements from the respondents, e.g. to the effect that the perceived risk of becoming addicted or options for self-change may vary not only
with type of addiction, but also with vari-ables such as age, gender, socio-economic status, and social context.
To overcome these limitations, more research will be needed. Further analysis of the data from the study presented here will focus on how respondents’ percep-tions of various addicpercep-tions relate to their personal addiction experiences, to socio-demographic factors such as age, gender, ethnic background, educational level, and family situation, and to wider political-ideological inclinations and attitudes, as well as to the stigma surrounding various addictions. In addition, the issues under study in the present survey will be ex-plored in further investigations, using qualitative methods, in an attempt to cap-ture more subtle aspects of prevailing ceptions of addiction and how these con-ceptions have been formed. To get a better grasp of how the “images of addiction” are influenced by various kinds of per-sonal addiction experiences, such studies should include not only lay people and professionals, but also persons with past and present addiction problems (cf. Koski-Jännes et al. 2009). Finally, and consider-ing that similar research is ongoconsider-ing in sev-eral countries, cross-cultural comparisons in this area offer, as already disussed, an interesting option.
Jan Blomqvist, Professor
Centre for social Research on alcohol and Drugs, soRaD
stockholm University
sE-106 91 stockholm, sweden E-mail: [email protected]
NOTES
1) Bergmark & Oscarsson (1988) use this term to refer to a set of undisputed, and alleged-ly undisputable, themes that they claim to provide the unreflected basis for any debate on and public action targeting the drug problem in Sweden. According to Hübner (2001) this “doxa” has, by and large, also been adopted by the media, thereby leaving little room in the public debate for oppo-nents to the official Swedish drug policy, based on zero tolerance.
2) Societal Images of Natural Recovery. This study explored the confidence in “self-change” from different addictions, based on 30 “key informants” (representing addiction professionals as well as “lay therapists” and “common people”) in nine large cities in seven different countries. The Swedish part of this study, reported by Andersson et al. (2004), was led by the present author. The results pointed to considerable differences between various addictions, but also between settings, and between professionals and lay people. 3) Regarding alcohol, less than 5 per cent of
the adult Swedish population are today lifetime abstainers (Blomqvist et al. 2007), whereas slightly more than 10 per cent could at the time of the survey be charac-terised as “frequent binge drinkers” (Selin 2004). With regard to tobacco use, the proportion of daily smokers in Sweden decreased from 36 per cent of the men and 29 per cent of the women in 1980, to 14 per cent of the men and 19 per cent of the women in 2004, and has decreased further since (Lundquist 2007). At the same time snuff use has increased, partly as a substitute for smoking, and 23 per cent of the men and 4 per cent of the women were daily users during 2004 (ibid.). As concerns narcotic drugs, Sweden’s extremely restric-tive policy in this area, making any use of narcotics classified substances a punishable crime, has been fairly successful in keeping youthful, recreational use on a low scale (Olsson 2009). For example, lifetime use of any narcotic substance among nine-graders has during the past decades fluctuated
bet-ween six and ten per cent (Leifman 2008). However, seen in a European perspective, Swedish drug policy seems to have been less successful in keeping down “heavy” drug abuse and drug-related mortality in particular (ibid.). Still, the use and misuse of narcotic drugs is uncommon in Sweden, as shown by the fact that, since the turn of the millennium, past year prevalence of cannabis use has been estimated to less than 2.5 per cent, and the use of other narcotic drugs to less than 1.5 per cent (ibid.) As for the misuse of medical drugs, there are no reliable reports on illegal use of drugs sold on prescription (which is probably not very common), albeit that the Swedish National Association for Helping Misusers of Pharmaceutics (RFHL), claim that a quarter of a million Swedes are dependent on (illegal or legally prescribed) such drugs. Finally, Jonsson et al. (2000) found that one and a half per cent of the population over 15 years were present problem gamblers, and that as many were former problem gamblers. The highest prevalence was found among the youngest men (ibid.).
4) By and large, Sweden has long spent more per-capita resources in care and treatment of alcohol and drug problems than most comparable countries. The main responsi-bility for this care lies with the municipal Social Services, and has to a large extent been focussed on social and psychosocial rehabilitation, although treatment for alco-hol problems has largely been more “thera-peutic” in character, and treatment for drug problems more aimed at re-socialisation (Blomqvist 2004). However, in recent years, the quest for “evidence-based practice” that has accompanied various attempts to make the public sector more rational and more cost-effective, has also given way for an increasing “bio-medicalisation” (cf. Blomqvist et al. 2009). This has become evident not least in the official rhetoric and in the media, where more attention seems at present to be paid to “promising” phar-macological treatments and to “disease-based” mutual help groups such as AA and
NA, than to traditional psychosocial care. In recent decades, with increased interna-tionalisation and increased Internet access, new forms of gambling have appeared and have become an integral part of the entertainment industry, including TV. At the same time, gambling problems have re-ceived increasing attention, and a number of separate treatment facilities for such pro-blems have been established. There are also a few specialised facilities for persons who misuse medical drugs, although those enga-ged in these matters often claim this to be a “hidden” problem, more or less neglected by both the prescribing doctors and the media. Finally, smoking has been officially discussed largely as a health issue, and as an economic burden to society, but seldom in terms of an individual “disease”. Ac-cordingly, the official strategy in this area – which has been fairly successful (see Note 3) – has largely consisted in a combination of health information (pamphlets, warning labels etc.), and campaigns and measures aimed at rendering smoking more difficult. Regarding snuff use, there has been some debate concerning potential health risks, but by and large, snuff has not been a big issue neither to the authorities nor in the media.
5) Although not necessarily statistically cor-rect in all aspects, paired t-test was consis-tently applied to all ratings to test whether the mean rating of a certain problem was statistically different from its next lower or higher counterpart.
6) It should be noted thought that the official drug discourse in Sweden does not make this distinction between e.g. cannabis and “harder” drugs
7) In this study, “crimes against the person” (murder, rape a.s.o.) ranked highest before “family violence” and “drug abuse”. 8) In places seven and nine out of ten
respec-tively.
9) Transformed in the analysis, for the sake of comparability, to a five-pont scale. 10) It should be observed that severity on
the societal level was, except for alcohol, gambling, medical drugs, and cannabis, only rated for “tobacco” and “other
narco-tic drugs” (than cannabis). Therefore, the individual risk to develop tobacco depen-dence has been calculated as the mean risk for cigarettes and snuff, and the risk to get “hooked” on other narcotic drugs (“hard drugs”) as the mean risk for amphetamine, cocaine, and heroin.
11) Although paired t-tests showed these dif-ferences to be statistically significant for all these addcitions (p < .05).
12) Except for the use of substitutes such as nicotine pills, chewing gums or plasters (or, for that part, substituting cigarettes for snuff ). It should also be noted there is an increasing commercial launching of such means.
13) This may at least partly be explained by the Finnish “experiment” with lower taxes on liquor to counter increased private im-port, that lead to a rapid increase in alcohol mortality and alcohol related harm during the years before the Finnish survey was conducted in 2007.
14) Whether the assumptions about metabolic or other physiological aetiological factors of the popular disease model of the 1940s (cf. Pattison 1976), AA: s concept of “spiritual disease”, or topical claims of all kinds of addictions as “brain diseases”.
15) In addition it can be noted that in a three-factor solution using the present data, “hard” drugs and cannabis got grouped together with all types of crime in a “moral-legal” factor, the “social/political” factor looked much the same as in the four-factor solution, and tobacco got grouped together with alcohol and gambling in what could be seen as a “bad habits” factor.
16) In this article, ”guilty” vs. “victim”, and “capable” vs. “incapable” are distinguis-hed as the two basic dimensions of the Brickman et al. model, and “discipline” or “fosterage” and “conversion” are discus-sed as the implications in practice of the “enlightenment” model.
17) Responsibility entirely or mostly on the individual vs. entirely or mostly on circumstances; and no or relatively low vs. moderate to very high probability for “self-change”.