1
Osteopetrosis
Abstract
Osteopetrosis is a congenital bone disease caused by malfunctioning osteoclasts. It is extremely rare and difficult to diagnose because of this. However, increasing awareness is resulting in advances in cures and treatment options for osteopetrosis sufferers. The genetic type of osteopetrosis has a large degree of influence on the difficulty of treatment and prognosis. Malignant Infantile Osteopetrosis (MIOP) is the most devastating and depends strongly on early diagnose for an agreeable outcome. Normal bone anatomy and osteoclast function will be explained and case reports of both human and non-human occurrences of osteopetrosis will demonstrate the wide range of manifested symptoms and severity of this disease.
Introduction
Osteopetrosis is a congenital disease that is characterized by malfunctioning or missing osteoclasts.1 The first description of the disease was provided in 1904 by Albers Schonberg.1-4 There are three main types of osteopetrosis which include: 1) autosomal dominant osteopetrosis (ADO), 2) intermediate autosomal recessive, and 3) autosomal recessive.1 Autosomal dominant is the most frequent form occurring in approximately 5 in every 100 000 births. It is divided into two subtypes. The first subtype (ADO-I) is the least severe form and results in subtle bone thickening and is frequently asymptomatic. The second, and more severe, subtype (ADO-II) is asymptomatic in 10-20% of sufferers and when symptoms do arise they usually do not manifest until the early twenties.5 Autosomal recessive osteopetrosis or Malignant Infantile Osteopetrosis
2
(MIOP) is the least common and most severe form. It occurs in 1 in every 200-300 000 births,6 and is fatal within the first ten years of life without early treatment.5
Normal Bone Anatomy and Osteoclast Function
An average healthy adult with properly functioning bone physiology will have
approximately 80% cortical bone and 20% trabecular bone overall. They will also have about 21 000 000 cortical osteons and 14 000 000 trabecular osteons. In order to maintain a proper bone matrix bones are constantly undergoing remodeling to prevent the buildup of microdamage. Bones are vital because they provide us with protection and help with locomotion by serving as attachments for muscles and ligaments. A typical adult will have bone porosity that is less than 5%, but it is normal for that percentage to increase with age. Bone diameter also increases with age because formation is usually faster than resorption resulting in increased outer bone
thickness.7 However, disease processes such as osteopetrosis actually result in decreased porosity and increased bone thickness on the inside of bones making them unstable.8
This instability is caused by decreased or malfunctioning osteoclasts. In osteopetrosis osteoclasts are either absent or fail to function normally. This prevents healthy bone remodeling and creates an elaborate but unstable bone matrix.8 Normal bone remodeling has four main steps. The first is activation of osteoclast precursors, second is the resorption process which takes between 2 and 4 weeks to complete. During resorption osteoclasts secrete enzymes that break down the old or damaged bone matrix. The third step is reversal where the transition between resorption of old bone and formation of new bone takes place. The fourth and final step is bone formation when osteoblasts create new healthy bone. This step can take between 4 and 6 months
3
to complete.7 Despite the fact that normal bones only have a turnover rate of 2-3% it is enough to maintain a strong healthy matrix with the proper proportions of trabecular and cortical bone.7
Symptoms
Osteopetrosis results from decreased numbers or functionality of osteoclasts in the bones. Because of the malfunctioning osteoclasts old bone is not properly resorbed and new bone begins to fill the medullary cavity. This causes the bone to be brittle and break easily and will eventually smother the marrow.1 The destruction of the marrow results in a lowered immune response and in many cases causes misdiagnoses as leukemia.6 In MIOP the results of this osteoclast
destruction are more severe. The symptoms begin within the first months of life and include but are not limited to:
Hypercalcemia.
Hepatosplenomegaly.
Leukoerythroblastosis.
Respiratory distress or speedy respiration.
Blindness or deafness due to nerve compression.
Bronchopneumonia.
Osteomyelitis.
Anemia and general failure to thrive in infants.1,4-6
Patients with ADO-I do not experience most of the above symptoms. However, they can have bone thickening in the cranial vault which can cause nerve compression resulting in blindness or deafness, but they do not usually have brittle or weak bones.9 Whereas ADO-II victims do often
4
experience brittle bones due to decreased resorption, but this does not become a problem until later in life and neither dominate form is associated with a decreased lifespan.1
Diagnoses
Diagnosis of osteopetrosis is difficult because its symptoms can mirror those of other diseases, such as leukemia.1 The simplest way to diagnose osteopetrosis in severe cases of ADO or MIOP is radiographically. A regular radiograph of MIOP will show increased bone density and a “bone in bone appearance”6(p. 91)
(see Figure 1 and 2). In severe cases of ADO the bones will appear thick and no medullary canal will be visible (see Figure 3).1 There are also several biochemical markers that can indicate osteopetrosis, but they are not necessarily definitive, and unless osteopetrosis is already suspected they are not likely to be checked. Several of these markers are mSx2 and RANKL. MSx2 is present in cells for the purpose of regulating bone formation and its absence can be indicative of osteopetrosis. RANKL is a main osteoclast differentiating factor and decreased amounts have been linked to osteopetrosis.10 Another reliable way to diagnose osteopetrosis is bone marrow and trephine biopsy. If the patient
biopsied is positive for osteopetrosis a trephine biopsy will show thickening in the trabeculae and larger amounts of woven bone. Decreased bone marrow spaces will also be apparent.3
Nuclear Medicine
Studies have indicated that Nuclear Medicine can also be an asset in the diagnoses of osteopetrosis. A whole-body bone scan performed on an osteopetrosis patient will usually show extreme radioactive uptake at the epiphysis and metaphysis of the humeri, tibias and fibulas, spine and distal femur (see Figure 4).11 The diagnoses can then be confirmed by regular x-ray or
5
bone biopsy. However, nuclear medicine continues to have practical applications after the initial diagnoses of the disease. Bone scintigraphy can be used as a method for tracking the progression of the disease and detecting fractures and bone lesions that may not appear on regular x-ray. It also has the added benefit of imaging the entire skeleton while minimizing the dose to
approximately 6.3 mSv. This is especially relevant because of the diseases propensity for effecting children.12 This low radiation dose also makes nuclear medicine a good option for patients who are asymptomatic or only display minor symptoms.12
Magnetic Resonance Imaging and Computed Tomography
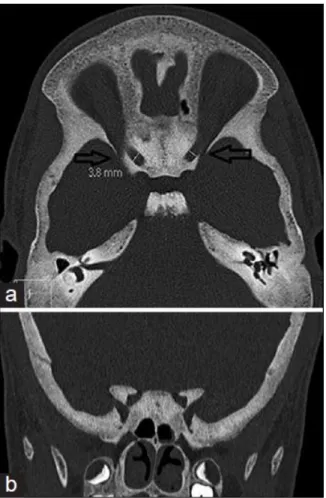
Magnetic Resonance Imaging (MRI) and Computed Tomography (CT) can also be useful when partnered with x-ray in both confirming diagnoses and identifying rare complications of the disease. MRI can potentially identify hydrocephalus, narrowed nerve channels, and cerebral or nerve atrophy.12 One rare complication associated with osteopetrosis is temporary or
permanent blindness caused by optic nerve compression. This results from thickening of the skull which narrows the optic channel. If this is allowed to continue or goes undiscovered it can result in nerve atrophy and permanent blindness. CT is useful in displaying the bones that are compressing the nerve while MRI shows the resulting compression of the soft tissue (see Figures 5 and 6).13
Treatment
Bone marrow transplant (BMT) is currently the only method of treatment that has the potential to be curative for MIOP, but in order for it to be successful it has to be administered very early in life. BMT can cure MIOP because if done before too much damage has occurred it
6
can provide normally functioning osteoclasts that can prevent further buildup of unstable bone.8 Recent studies have also shown some success when cord blood is transplanted into the
intramedullary cavity.14
Recently a promising experiment was performed on osteopetrotic mice that were lacking mSx2 and had below average amounts of RANKL. The mice showed skeletal abnormalities and tooth defects. The mice were bred with mice that overexpressed RANKL and the resulting offspring showed diminished skeletal abnormalities. This showed that compensation for RANKL deficiency could be a potential treatment for osteopetrosis in the future.10
Since there are very few curative treatments for osteopetrosis many methods just focus on dealing with symptoms. For MIOP sufferers antibiotics are frequently used to deal with
infections arising from the decreased marrow activity,6 and experimental methods for dealing with fractures in ADO patients have recently been developing as well. Healing of fractures in ADO patients is difficult due to the malformed bone and immunodeficiency, but recent fixation methods designed to minimize infection have been successful. A patient with osteomyelitis due to the white blood cell impairment common in osteopetrosis had a femoral head and greater trochanter resection performed. Arthroplasty was made difficult by the malformed bone, but an experimental cementless implant was attempted with a spacer that was loaded with antibiotics. Several infections arose along the way but a successful hip transplant was eventually performed. This showed potential for future treatment of osteopetrotic patients suffering from osteomyelitis.1
Complications of Treatment
There are many complications associated with BMT and cord blood transplantation primarily caused by the need for a compatible donor, but another rare complication of BMT in
7
osteopetrosis patients in hypercalcemia. This is a fairly rare complication but if the patient being treated is over the age of two the chances of hypercalcemia rise dramatically.8 The most
concerning difficulty that arises from cord blood transplantation is the possibility of delayed engraftment or rejection.14
Human Case Study
A 2 month old female presented with bronchopneumonia, elevated respiration, and anemia. An abdominal examination revealed that she also had an enlarged liver and spleen. Tests showed elevated leukocytes and a reduced number of platelets, and x-rays showed increased density throughout all of her bones and decreased medullary spaces. Her ribs also had a spatula appearance with thickened ends (see Figure 1). She was diagnosed with MIOP and treated with antibiotics, blood transfusions, calcium, and vitamin D. However, survival with MIOP is largely dependent upon bone marrow transplants, and how quickly certain symptoms begin to manifest themselves. For example, hematological symptoms usually appear within the first year, but since they were already apparent at 2 months her likelihood of survival was reduced. Other likely issues associated with MIOP include low calcium levels and hearing and vision impairment. This patient did not have any vision defects or a calcium deficiency, but there is approximately a 75% chance that vision problems will develop.6
Non-Human Case Study
A recent study done on osteopetrotic poultry suggests a viral component that is believed to be caused by the herpes virus. In poultry osteopetrosis is more commonly referred to as “thick
8
leg disease.”9(p.188) Despite the cause of osteopetrosis in poultry being different than the cause in humans the symptoms are the same. Bone resorption in the diaphysis of long bones is inhibited and as a result bones become brittle and thickened. However, this malformation is usually isolated to the long bones of the legs. The performers of the study attempted to vaccinate against osteopetrosis but were unsuccessful. They studied 64 birds with confirmed osteopetrosis and found that 30% did not move around, 50% were lame, and 20% exhibited signs of anxiety and depression. As a result of the lack of mobility many of the birds were emaciated because they did not get up to feed. The researchers also found that the poultry that developed osteopetrosis had less light per day than those who did not develop the disease, and they were also overcrowded resulting in increased CO2 levels which caused respiratory problems in many of the birds. This suggested a possible environmental cause of the disease in poultry.15
Conclusion
MIOP may be a rare disease but early detection is critical so awareness of its clinical signs and symptoms is essential. Despite the limited curative treatments for osteopetrosis many experimental treatment options are developing as awareness about the disease grows. Research conducted to better understand the disease such as the mice lacking mSx2 shows potential for future treatment on humans. ADO may not be as severe a form but early detection can still result in improved quality of life, and with the reduced healing abilities of these patients advances in surgical procedures that allow for proper healing can have dramatic benefits.
9
References
1. Manzi G, Romanò D, Moneghini L, Romanò CL. Successful staged hip replacement in septic hip osteoarthritis in osteopetrosis: a case report. BMC Musculoskel Dis. 2012;13(1):50-55. doi: 10.1186/1471-2474-13-50.
2. Çiftçi B, Çetin N. Osteopetrosis. Turk J Rheumatol. 2013;28(3):216-217. doi: 10.5606/tjr.2013.2824.
3. Walia H, Jain R, Nirwan R, Bansal R, Gupta G. Osteopetrosis: trephine biopsy an essential tool. Int J Stud Res. 2013;3(2):45-47. doi: 10.4103/2230-7095.136496.
4. Stroescu R, Bizerea T, Pop E, Mărginean O, Micle I, Dobre M. A rare case of failure to thrive in infants: malignant infantile osteopetrosis. J Pediatr. 2013;16(63):49-53.
5. Peer M, O'Donoghue K. Osteopetrosis in pregnancy: a rare case report. Obstet Med (1753-495X). 2012;5(1):27-29. doi: 10.1258/om.2011.110039.
6. Kumar KJ, Bandaru K, Prashanth SN, Mamatha S. Malignant infantile osteopetrosis. Indian J Hum Genet. 2013;19(1):90-92. doi: 10.4103/0971-6866.112911.
7. Clarke B. Normal bone anatomy and physiology. J Am Soc Nephrol. 2008; 3(3):5131-5139. doi: 10.2215/CJN.04151206.
8. Kulpiya A, Mahachoklertwattana P, Pakakasama S, Hongeng S, Poomthavorn P.
Hypercalcemia and altered biochemical bone markers in post-bone marrow transplantation osteopetrosis: a case report and literature review. Pediatr Transplant. 2012;16(5):E140-E145. doi: 10.1111/j.1399-3046.2011.01475.x.
9. Mitri Z, Tangpricha V. Osteopetrosis, hypophosphatemia, and phosphaturia in a young man: a case presentation and differential diagnosis. Case Reports in Endocrinology. 2012;:1-5. doi: 10.1155/2012/238364.
10. Castaneda B, Simon Y, Lézot F, et al. Role of RANKL (TNFSF11)-dependent osteopetrosis in the dental phenotype of Msx2 null mutant mice. PLoS One. 2013;8(11):1-9. doi:
10.1371/journal.pone.0080054.
11. Xue YL, Shen CT, Qin ZL, Luo QY. A rare patient with osteopetrosis presenting in whole-body bone super scan. J Radiol Diagn Imag. 2013; 1(2):37-39. doi:
10.14205/2309-4427.2013.01.02.1.
12. Barral CM, Andrade GS, Ferreira MJM, et al. The role of whole-body bone scintigraphy in a case of osteopetrosis. Egypt J Radiol Nucl Med. 2014; 45(4):1249-1253. doi:
10.1016/j.ejrnm.2014.06.008.
13. Kumar N, Singh A, Saxena R, Menon V, Sharma S. An unusual cause of optic atrophy in a child. Indian J Opthalmol. 2014; 62(4):494-495. doi: 10.4103/0301-4738.132111.
10
14. Buchbinder D, Steward C, Soni A, et al. Successful cord blood transplantation in a patient with malignant infantile osteopetrosis and hemophilia. Pediatr Transplant. 2013;17(1):E20-E24. doi: 10.1111/j.1399-3046.2012.01758.x.
15. Uzunova K, Stamatova-Yovcheva K, Dimova V, Yovchev D, Halil M. Anatomical and ethological changes in poultry affected by osteopetrosis. Scientific Papers: Anim Sci Biotechnol. 2014;47(1):188-191.
11
Figure 1. A radiograph showing increased bone density. Image courtesy of: Kumar KJ, Bandaru K, Prashanth SN, Mamatha S. Malignant infantile osteopetrosis. Indian J Hum Genet. 2013;19(1):90-92. doi: 10.4103/0971-6866.112911.
12
Figure 2. Radiographs demonstrating spatula shaped ribs (a) and bone in bone appearance (b). Image courtesy of: Walia H, Jain R, Nirwan R, Bansal R, Gupta G. Osteopetrosis: trephine biopsy an essential tool. Int J Stud Res. 2013;3(2):45-47. doi: 10.4103/2230-7095.136496.
13
Figure 3. AP and Lateral hip projections pre-operative after failed fixation with a non-union of the femoral neck. Image courtesy of: Manzi G, Romanò D, Moneghini L, Romanò CL.
Successful staged hip replacement in septic hip osteoarthritis in osteopetrosis: a case report. BMC Musculoskel Dis. 2012;13(1):50-55. doi: 10.1186/1471-2474-13-50.
14
Figure 4. Nuclear Medicine bone scan showing abnormal radioactive uptake in epiphysis and metaphysis of long bones. Image courtesy of: Barral CM, Andrade GS, Ferreira MJM, et al. The role of whole-body bone scintigraphy in a case of osteopetrosis. Egypt J Radiol Nucl Med. 2014; 45(4):1249-1253. doi: 10.1016/j.ejrnm.2014.06.008
15
Figure 5. MRI showing compressed optic nerve sheath. Image courtesy of: Kumar N, Singh A, Saxena R, Menon V, Sharma S. An unusual cause of optic atrophy in a child. Indian J
Opthalmol. 2014; 62(4):494-495. doi: 10.4103/0301-4738.132111
Figure 6. CT showing increased bone density and narrowed optic canals. Image courtesy of: Kumar N, Singh A, Saxena R, Menon V, Sharma S. An unusual cause of optic atrophy in a child. Indian J Opthalmol. 2014; 62(4):494-495. doi: 10.4103/0301-4738.132111