Utility of Rapid B-Type Natriuretic Peptide Assay for Diagnosis of
Symptomatic Patent Ductus Arteriosus in Preterm Infants
Byung Min Choi, MD; Kee Hyoung Lee, MD; Baik Lin Eun, MD; Kee Hwan Yoo, MD; Young Sook Hong, MD; Chang Sung Son, MD; and Joo Won Lee, MD
ABSTRACT. Objective. In preterm infants, the rapid and accurate determination of the presence of a hemody-namically significant patent ductus arteriosus (PDA) is extremely important, but this is often difficult. Plasma B-type natriuretic peptide (BNP) measurement has been reported to be a helpful aid in the diagnosis of hemody-namically significant PDA in preterm infants. The aim of our study was to investigate the usefulness of a rapid BNP assay as a diagnostic marker of symptomatic PDA (sPDA) in preterm infants.
Methods. Sixty-six preterm infants, ranging from 25 to 34 gestational weeks of age, underwent clinical and echocardiographic examinations for PDA every other day from the third day of life until the disappearance of ductal flow. Blood samples were collected and plasma BNP concentrations were measured simultaneously us-ing a commercial kit, (Triage BNP test kit; Biosite Diag-nositics, San Diego, CA). When>2 clinically significant
features of PDA were noted, and a large ductal flow was confirmed by color Doppler echocardiography, sPDA was diagnosed and treated with indomethacin.
Results. On the third day after birth, the mean BNP concentration in the sPDA group (nⴝ 23) was signifi-cantly higher than in the control group (nⴝ43) (2896ⴞ 1627 vs 208ⴞ313 pg/mL). Seventeen infants (74%) in the sPDA group became asymptomatic after an initial course of indomethacin and their BNP levels concomitantly de-creased. Moreover, BNP concentrations were signifi-cantly correlated with the magnitudes of the ductal shunt, such as the ratio of left atrial to aortic root diam-eter and the diastolic flow velocity of the left pulmonary artery (rⴝ0.726 and 0.877). The area under the receiver operator characteristic curve for the detection of sPDA was high: 0.997 (95% confidence interval: 0.991-1.004). The best cutoff of BNP concentration for the diagnosis of sPDA was determined to be 1110 pg/mL (sensitivity: 100%; specificity: 95.3%).
Conclusion. In preterm infants, the circulating BNP levels correlated well with the clinical and echocardio-graphic assessments of PDA. Although not a stand-alone test, the rapid BNP assay provides valuable information for the detection of infants with sPDA that require treat-ment. Moreover, serial BNP measurements may be of value in determining the clinical course of PDA in pre-term infants. Pediatrics 2005;115:e255–e261. URL: www.
pediatrics.org/cgi/doi/10.1542/peds.2004-1837;patent duc-tus arteriosus, B-type natriuretic peptide, preterm infants, symptomatic PDA.
ABBREVIATIONS. PDA, patent ductus arteriosus; hsPDA; hemo-dynamically significant patent ductus arteriosus; BNP, B-type na-triuretic peptide; sPDA, symptomatic patent ductus arteriosus; LA/AO, a ratio of left atrium to the aortic root diameter; DFLPA, diastolic flow velocity of the left pulmonary artery; ROC, receiver operator characteristic; asPDA, asymptomatic patent ductus arteriosus.
R
apidly and accurately determining the indica-tions of therapeutic closure of a hemodynam-ically significant patent ductus arteriosus (hsPDA) in preterm infants is extremely impor-tant.1–3The currently used tools, such as the clinical findings, which include heart failure and the typical echocardiographic features of hsPDA, have unsatis-factory sensitivities and/or specificities.4–8A simple blood test that could easily, rapidly, and accurately help in diagnosing hsPDA would be of great use, especially in low birth weight infants. However, cur-rently no accepted blood test is available to aid in the diagnosis and management of preterm infants with PDA.Plasma B-type natriuretic peptide (BNP) measure-ment has been proposed as an aid in the diagnosis of hsPDA in preterm infants.9,10Preliminary evidences have demonstrated the potential usefulness of se-quential plasma BNP measurements in monitoring these infants with a rapidly changing hemodynamic status due to PDA.11,12 These 2 previous studies demonstrated the potential usefulness of sequential plasma BNP measurements in monitoring preterm infants with PDA. However, several confounders that may affect circulating BNP levels in preterm infants have not been evaluated and discussed.
However, the techniques for determining hormone levels are problematic, as are the time and amount of sample blood required for hormone analysis. The recently Food and Drug Administration–approved point-of-care, rapid whole-blood assay for BNP gives the clinician an opportunity to explore its potential usefulness. Moreover, after addition of 250 L of whole blood to the sample port of the disposable device, the assay is completed in 10 minutes.
In our previous studies13 using this commercially available bedside test, we observed the interrelation-ships between hemodynamic changes of ductal shunts and BNP concentrations in healthy preterm
From the Department of Pediatrics, College of Medicine, Korea University, Seoul, Korea.
Accepted for publication Nov 8, 2004. doi:10.1542/peds.2004-1837 No conflict of interest declared.
Reprint requests to (C.S.S.) Department of Pediatrics, Anam Hospital, Korea University Medical Center, #126-1, 5-Ga, Anam-Dong, Seongbuk-Gu, Seoul, 136-705, Korea. E-mail: pedson@ns.kumc.or.kr
infants without evidence of respiratory distress. We found that BNP concentrations are related to the magnitude of the ductal shunt and that they serve as an indicator of spontaneous closure of ductus arteri-osus in preterm infants. Therefore, it was expected that BNP measurements might be useful when de-ciding on the necessity and the appropriate time for the medical and surgical management of preterm infants with hsPDA.
In the present study, to investigate whether plasma BNP in premature infants can identify hsPDA requiring treatment, plasma BNP concentra-tions were measured prospectively in premature in-fants with and without symptomatic PDA (sPDA) and compared with other echocardiographic criteria of hemodynamic significance. Moreover, we exam-ined whether repeated plasma BNP measurements might be of value in determining the clinical course of PDA during the first 7 days of life. Finally, to investigate the diagnostic utility of a rapid BNP as-say for the differentiation of sPDA, the best cutoff value of BNP was determined.
METHODS Study Population
For Korean infants who had been admitted into the neonatal intensive care unit of Ansan Hospital, Korea University Medical Center, the entry criteria for this study were: (1) born at a gesta-tional age of 25 to 34 weeks, estimated from the last menstrual period; (2) admitted within 24 hours after birth; (3) no major congenital malformation, including cardiac abnormalities except for patent foramen ovale; and (4) an echocardiographic study for PDA started within 72 hours after birth. The study protocol was approved by the local research ethics committee of Ansan Hospi-tal, and written parental informed consent was obtained in all cases.
Eighty-five infants were initially enrolled during a 16-month period (from August 2002 to November 2003). Parental consent was refused for 5 infants, and 11 eligible infants were not studied, because the investigator (B.M.C.) was unavailable. Of 39 infants receiving surfactant, 3 infants with complications (pneumothorax,
n⫽2; pulmonary hemorrhage,n⫽1) were excluded.
After these exclusions, 66 infants remained in the study and were eligible for evaluation. Their mean gestational age was 29.9 weeks (range: 25–34 weeks) and the mean birth weight was 1356 g (range: 625–2180 g). Thirty-one (47.0%) infants were male, 49 (74.2%) had received some antenatal steroids, and 63 (95.5%) were born at our hospital (the others were transferred after delivery).
The information collected included demographic details and the use of antenatal steroids and exogenous surfactant. Oxygen requirements, ventilatory settings, and intraarterial blood pres-sures were recorded at the time of each echocardiographic scan.
We prospectively evaluated infants for PDA within the first 3 days of life using a variety of diagnostic methods and adminis-tered indomethacin if PDA became clinically apparent (but before it became symptomatic).
Echocardiographic Studies
An Acuson Cypress ultrasound machine (Acuson Corporation, Mountain Drive, CA) with a 7-MHz transducer incorporating color-flow, pulsed-wave, and continuous-wave Doppler was used. Echocardiography was performed every other day from the third day (48 –72 hours) of life on preterm infants who fulfilled the entry criteria. The structural normality of the heart was estab-lished during the course of the scanning.
Initially, ductal shunt flow was visualized in a high left parasternal view using color-flow Doppler echocardiography. Shunting was graded by assessing color Doppler flow in the main pulmonary artery: (1) “mild,” if a narrow jet was detected at the pulmonary end of the ductus by color Doppler echocardiography without disturbed flow at the level of the pulmonary valves; (2)
“moderate,” if a jet was wider and passed well into the pulmonary artery but not quite into the pulmonary valve; and (3) “large,” if a jet was very wide, reached the pulmonary valve, and swirled down into the pulmonary artery.
To estimate the magnitude of left-to-right shunting across PDA, 2 representative echocardiographic markers were evaluated. The ratio of the left atrial to aortic root diameter (LA/AO) was deter-mined in the parasternal long-axis view at the level of the aortic valve using a standard method.14Three measurements were taken
and averaged.
To obtain the diastolic flow velocity of the left pulmonary artery (DFLPA), a pulsed Doppler sample volume was placed on the left pulmonary artery, just after the bifurcation of the main pulmonary artery. The pulsed Doppler flow pattern of the left pulmonary artery was then recorded and the DFLPA was mea-sured from the screen. The DFLPA was estimated from the max-imum velocity during the diastolic period.15
When ductal flow was confirmed to have disappeared by color Doppler echocardiography, no subsequent echocardiographic ex-amination was performed. Throughout the study, echocardiogra-phy was performed by 1 investigator only (B.M.C.) to avoid any interobserver variability. Results were recorded on videotape for subsequent analysis. Hemodynamic variables were analyzed in terms of their possible correlation with BNP levels.
Diagnosis and Management of PDA
Clinical diagnoses of sPDA were made by individual attending pediatricians based on: (1) the presence of a systolic or continuous murmur; (2) a bounding pulse or a hyperactive precordial pulsa-tion; (3) a difficulty in maintaining blood pressure; (4) a worsening ventilatory status; and (5) chest radiographic evidence, ie, pulmo-nary congestion or cardiomegaly (a cardiothoracic ratio⬎60%) with increased pulmonary flow. We defined sPDA as the presence of 2 of these 5 signs with a confirmation of a large left-to-right ductal flow by color-flow Doppler echocardiography.
After confirming the diagnosis of sPDA, indomethacin was administered intravenously if not contraindicated. The initial dose was 0.2 mg/kg followed by 2 additional doses of 0.2 mg/kg at intervals of 12 hours. A subsequent clinical and echocardiographic assessment of sPDA was performed 48 hours after the initial course of indomethacin. If the diagnostic criteria for sPDA were no longer fulfilled, no additional indomethacin was administered and the infant was observed closely. When the criteria for sPDA were fulfilled again, an additional second course of indomethacin was administered.
In our unit, total fluid intakes of preterm infants were increased in a stepwise manner: 60 mL/kg per day on day 1, 80 mL/kg per day on day 3, and 100 mL/kg per day on day 7. However, after diagnosis of sPDA had been confirmed, fluid intakes were re-stricted to low maintenance to prevent congestive heart failure and worsening pulmonary edema.
Measurement of Plasma BNP
At the time of performing the Doppler echocardiographic mea-surements, blood samples for the measurement of BNP were collected by radial artery or umbilical artery catheter aspiration. BNP concentrations were detected using a commercial kit, (Triage BNP test; Biosite Diagnositics, San Diego, CA), by fluorescence immunoassay. The measurable range of BNP concentrations by the Triage assay was 5 to 1300 pg/mL (from August 2002 to December 2002) or 5 to 5000 pg/mL (from January 2003 to No-vember 2003).
Statistical Analyses
Categorical data are presented as numbers (%), and continuous data as mean ⫾ SD. We used the 2or Fisher’s exact test to
compare categorical variables and the Student’sttest, the pairedt
for Windows (SPSS Inc, Chicago, IL). A P value of ⬍.05 was considered significant.
RESULTS Characteristics of Preterm Infants
Of the 66 enrolled infants, 43 infants did not de-velop sPDA and the ductus closed spontaneously within 5 days of life (control group, mean gestational age: 30.3 weeks; mean birth weight: 1396 g). The remaining 23 infants developed sPDA, which re-quired treatment with indomethacin within 3 days of life (sPDA group, mean gestational age: 29.1 weeks; mean birth weight: 1283 g). The characteristics of these 2 groups are summarized in Table 1. No sig-nificant differences were observed in terms of gesta-tional age, birth weight, gender, delivery type, or the use of antenatal steroid. However, Apgar scores at 1 and 5 minutes, the use of surfactant, and the use of dopamine were statistically different in these 2 groups. In the control group, echocardiographic evaluations and blood samples for BNP were taken at 56.7 ⫾ 11.8 hours of life, compared with 52.4 ⫾ 14.4 hours in the sPDA group. Age at the first
eval-uation of the control group was similar to that of the sPDA group.
At the first echocardiographic evaluation (3 days after birth), only 14 infants in the control group had a left-to-right ductal shunt. By the color-flow Dopp-ler method, infants with a large ductal shunt were more frequent in the sPDA group (23 of 23) than in the control group (7 of 43 [16.3%]).
BNP Levels in the Control Group
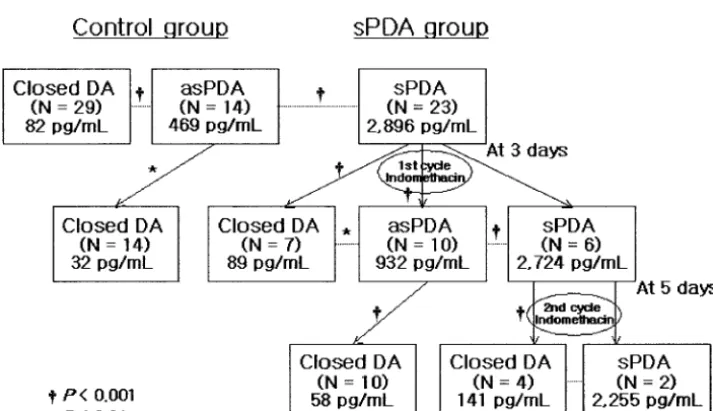
On the third day after birth, only 14 infants (32.5%) in the control group had a left-to-right ductal shunt but did not develop sPDA (asymptomatic PDA [as-PDA] group) (Fig 1). The mean BNP concentration of asPDA infants was significantly higher than that of closed ductus arteriosus infants (469 ⫾ 443 vs 82⫾ 73 pg/mL, respectively; P ⬍ .001), and BNP fell to the adult levels after spontaneous ductal closure 5 days after birth (32⫾ 24 pg/mL;P ⫽.003).
BNP Levels in the sPDA Group
On the third day after birth, the mean BNP con-centration for those who developed clinically
signif-Fig 1. Patencies of ductus arteriosus and changes of plasma BNP levels in the control group and sPDA groups according to the time during the first 7 days of life.
TABLE 1. Characteristic of Infants in the Control and sPDA Groups Control
(n⫽43)
sPDA (n⫽23)
PValue
Gestational age, wk 30.3⫾2.4 29.1⫾2.75 NS Birth weight, g 1396⫾418 1283⫾359 NS
Male/female 20/23 11/12 NS
Use of antenatal steroid 34 (79.1%) 15 (65.2%) NS Caesarean section 32 (74.4%) 16 (69.6%) NS Apgar score
1 min 4.2⫾1.8 2.7⫾2.0 .003
5 min 6.4⫾1.8 4.6⫾1.9 ⬍.001
RDS with surfactant therapy 17 (39.5%) 19 (73.9%) .008
Dopamine 19 (44.2%) 20 (87.0%) ⬍.001
Age at first evaluation, h 56.7⫾11.8 52.4⫾14.4 NS Large ductal shunt* 7 (16.3%) 23 (100%) ⬍.001 Values are expressed as numbers (%) of infants or means⫾SD. NS indicates not significant; RDS, respiratory distress syndrome.
icant PDA (sPDA group; Fig 1) was significantly higher than that of the control group (2896⫾1627 vs 208⫾ 313 pg/mL;P ⬍.001). On the fifth day after birth, 17 infants in the sPDA group became asymp-tomatic after the administration of 3 doses of indo-methacin. The ductus of 7 of these infants was par-ticularly closed by echocardiographic examination. There was a statistical difference in BNP concentra-tions before and after indomethacin administration in these 17 infants (2807⫾1524 vs 585⫾714 pg/mL, respectively; P⬍ .001). In the other 10 infants with asPDA, who had a reduced ductal shunt at posttreat-ment measureposttreat-ment, ductal closure was confirmed 2 days later.
On the other hand, in the remaining 6 infants in the sPDA group, PDA symptoms continued and no statistical difference was observed in BNP concentra-tions before and after indomethacin administration (3150 ⫾ 2027 vs 2747 ⫾ 1814 pg/mL, respectively). These 6 infants were treated with a secondary course of indomethacin treatment. Two days later, 4 of these infants became asymptomatic, and their mean BNP concentration was reduced significantly to 141⫾58 pg/mL (P ⫽ .004). The ductus of 2 infants did not close after the second indomethacin administration,
and no significant difference was found in their mean BNP concentration.
Correlation Between BNP Level and the Magnitudes of Ductal Shunt by Echocardiography
At the first echocardiographic evaluation, a signif-icant correlation was found between BNP concentra-tions and the LA/AO ratio (r⫽0.726;P⬍.001; Fig 2). In addition, BNP concentration and DFLPA, as determined using the pulsed-wave Doppler method, were found to be correlated (r⫽0.877;P⬍.001; Fig 3).
Association Between BNP Levels and a Diagnosis of sPDA
The area under the ROC curve for the detection of sPDA was high: 0.997 (95% confidence interval: 0.991–1.004; P ⬍ .001; Fig 4). The best cutoff BNP concentration for the diagnosis of sPDA was found to be 1110 pg/mL. At this cutoff level the sensitivity was 100% (23 of 23), the specificity was 95.3% (41 of 43), and positive predictive value was 92.0% (23 of 25).
DISCUSSION
BNP is one of a family of structurally similar pep-tide hormones that also includes atrial natriuretic peptide and C-type natriuretic peptide.16,17 BNP, which is produced by the cleavage of a precursor protein into BNP and the biologically inactive pep-tide N-terminal precursor protein, causes natriuresis, diuresis, vasodilatation, and smooth muscle relax-ation.18,19Unlike the atrial natriuretic peptide, which is stored in the cardiac atria and ventricles, the car-diac ventricles are the major source of plasma BNP, suggesting that BNP may be a more sensitive and a more specific indicator of ventricular disorders than other natriuretic peptides. Moreover, BNP release Fig 2. The LA/AO ratio compared with BNP. BNP was correlated
positively with the LA/AO ratio (r⫽0.726;P⬍.001).
Fig 3. The DFLPA versus BNP level. BNP was correlated posi-tively with DFLPA (r⫽0.877;P⬍.001).
seems to be in direct proportion to ventricular vol-ume expansion and pressure overload.20,21
Plasma concentrations of BNP increase in various pathologic states, particularly those involved in in-creased cardiac chamber wall stretch and expanded fluid volume (eg, in cases of heart failure, renal fail-ure, or primary hyperaldosteronism), or reduced peptide clearance (eg, in case of renal failure). BNP seems to have clinical utility in terms of excluding the diagnosis of heart failure in patients with symp-toms of breathlessness or fluid retention and may provide prognostic information about those with heart failure or other cardiac diseases.22–27 Also, there is some evidence that it may be useful for monitoring heart failure therapies.28,29
Yet, little data are available to suggest that BNP may be useful in a pediatric clinical setting. In pedi-atric clinical practice, BNP measurement has been suggested to be a means of determining the severity of congenital heart disease. Ootaki et al30 reported that BNP levels in plasma correlate well with biven-tricular volume, particularly with left venbiven-tricular volume in various congenital heart disease such as ventricular septal defect, atrial septal defect, and te-tralogy of Fallot and several cyanotic heart diseases. Suda et al31reported that plasma BNP reflects pres-sure and volume loading of the pulmonary artery and the right ventricle and suggested that BNP de-terminations may help to identify children with ven-tricular septal defect complicated by pulmonary hy-pertension, which demands early intervention. These results suggest that the measurement of plasma BNP may add clinically useful information relevant to the management of children with congenital heart dis-ease.
In healthy newborn infants, plasma BNP concen-trations are relatively high and vary greatly over the first few days. However, they reduce rapidly during the first week of life, suggesting that BNP has a physiologic regulatory role in the cardiovascular he-modynamic changes that occur during the postnatal period.32,33 Moreover, perinatal circulatory changes lead to an increase in ventricular volume and pres-sure load, which may stimulate BNP synthesis and secretion in the ventricle and increase circulatory BNP concentrations shortly after birth. Such in-creased levels of plasma BNP may act to alleviate the increased ventricular load after birth and may also support the heart function with a decreased preload in the first days of life. This may be because a raised circulatory BNP increases sodium and water excre-tion by the kidneys, suppresses renin and aldoste-rone secretion, and leads to venous and arterial di-latation.
Plasma BNP concentrations in preterm infants are higher than in healthy term infants for the first few days after birth.11,12 In particular, when PDA is present in preterm infants, the BNP concentration is abnormally high and reflects the magnitude of shunting through the PDA. Holmstrom et al11 sug-gested that the magnitude of shunting through the PDA is a major determinant of plasma BNP in pre-mature infants, based on clinical and echocardio-graphic assessments of shunt severity. In our
previ-ous studies,13plasma BNP levels in healthy preterm infants with a ductal shunt were higher than in pre-term infants without ductal shunt 24 hours after birth and then significantly decreased within 72 hours after birth according to the reduction in ducal flow.
The present study also demonstrates that plasma BNP levels in premature infants are strongly related to the hemodynamic influence of the PDA. On the third day after birth, the mean BNP concentration of the sPDA group, members of which developed clin-ically significant PDA, was significantly higher than that of the control group. These findings are consis-tent with a previous report12and suggest that BNP is a useful diagnostic marker of sPDA requiring treat-ment.
With the increasing use of the recently approved rapid BNP assay, it is important to determine diag-nostic cutoff values. We found that a BNP value ⬎ 1110 pg/mL on the third day after birth strongly predicted sPDA and thus indicates the need for in-tervention. Because circulating BNP is influenced considerably by several factors such as demographic factors, clinical situations, medical managements, and hemodynamic effects, large-scale randomized, clinical trials are necessary if we are to definitively determine the cutoff value in sPDA that best indi-cates the need for treatment in preterm infants.
In addition, the present study indicates that serial BNP measurements may add clinically useful infor-mation to the management of preterm infants with hsPDA. Plasma BNP levels in the sPDA group were found to be significantly lower after pharmacologic PDA closure, which concurs with the finding of a study by Holmstrom et al,11who demonstrated com-parable BNP changes after pharmacologic and sur-gical closure. Our results show a distinct fall of BNP, indicating hemodynamic improvement in hsPDA. Repeated BNP measurement may offer a simple and objective tool for following these preterm infants.
In the clinical management of preterm infants with hsPDA, it is important to quantify the shunt size and identify patients needing intervention. However, there is no generally accepted technique based on objective numerical values for the determination of ductal flow. The present study indicates that plasma BNP can reflect left-to-right ductal flow volume and may be helpful in identifying preterm infants with hsPDA that require early intervention. In fact, BNP was found to be significantly and positively corlated with the LA/AO ratio and DFLPA, which re-flects the magnitude of ductal shunt.
cutoff, the sensitivity was 95.2% (20 of 21) and the specificity was 93.3% (42 of 45).
In the branch pulmonary arteries there is an ab-normally high antegrade diastolic flow as the contin-uous stream of blood from the aorta pours into them via the ductus. In particular, DFLPA is considered to reflect the left-to-right ductal flow volume more di-rectly than other echocardiographic methods. Suzu-mura et al15 reported that a DFLPA of ⬎30 cm/ second, exceeding the mean control value by⫹2 SD on the third day after birth, suggests a large shunt. According to this result, the best cutoff of BNP con-centration for the detection of hsPDA is 1110 pg/mL; using this cutoff, the sensitivity was 88.0% (22 of 25) and the specificity was 97.6% (40 of 41).
Echocardiography is the main method used to de-tect PDA in newborns, and several markers of hsPDA have been identified using this method, in-cluding the LA/AO ratio, DFLPA, ductal size, left ventricular output and stroke volume, and reversed diastolic flow of the descending aorta. Echocardiog-raphy is required to confidently diagnose PDA, but the hemodynamic effects of PDA may be difficult to determine even with these typical echocardiographic features; also, the course of PDA cannot be reliably anticipated.7,8 Based on the results of the present study, it is believed that BNP measurement can be used as an adjunct to echocardiography in PDA. Although it is not a stand-alone test, the BNP assay provides valuable information quickly, concerning the detection of an infant requiring intervention for PDA, and for determining the clinical course of PDA in a preterm infant.
Overall, in this study, circulating BNP levels were found to correlate well with the clinical and echocar-diographic assessments of PDA in preterm infants, and changes in BNP levels were considered to indi-rectly represent ductal shunt changes. Particularly, a cutoff BNP level of 1110 pg/mL differentiated well between preterm infants with and without sPDA. Therefore, it is expected that the plasma BNP level is a useful diagnostic marker of sPDA in premature infants that may require treatment. Moreover, serial plasma BNP measurements may be of value in de-termining the clinical course of PDA in preterm in-fants.
CONCLUSIONS
The rapid assay for BNP measurement in blood seems to be a sensitive and specific test for differen-tiating preterm infants with and without sPDA in the neonatal intensive care setting. If additional studies validate these exploratory findings, it is possible that BNP will prove to be an additional cost-effective diagnostic armamentarium of attending pediatri-cians in neonatal intensive care units.
ACKNOWLEDGMENT
We thank the doctors and nurses at the neonatal intensive care unit, Department of Pediatrics, Ansan Hospital, Korea University Medical Center, for their enthusiastic support and cooperation.
REFERENCES
1. Cotton RB, Stahlman MT, Kovar I, Catterton WZ. Medical management of small preterm infants with symptomatic patent ductus arteriosus.
J Pediatr.1978;92:467– 473
2. Stefano JL, Abbasi S, Pearlman SA, Spear ML, Esterly KL, Bhutani VK. Closure of the ductus arteriosus with indomethacin in ventilated neo-nates with respiratory distress syndrome. Effects of pulmonary compli-ance and ventilation.Am Rev Respir Dis.1991;143:236 –239
3. Fowlie PW, Davis PG. Prophylactic indomethacin for preterm infants: a systematic review and meta-analysis.Arch Dis Child Fetal Neonatal Ed.
2003;88:F464 –F466
4. Davis P, Turner-Gomes S, Cunningham K, Way C, Roberts R, Schmidt B. Precision and accuracy of clinical and radiological signs in premature infants at risk of patent ductus arteriosus.Arch Pediatr Adolesc Med.
1995;149:1136 –1141
5. Skelton R, Evans N, Smythe J. A blinded comparison of clinical and echocardiographic evaluation of the preterm infant for patent ductus arteriosus.J Paediatr Child Health.1994;30:406 – 411
6. Urquhart DS, Nicholl RM. How good is clinical examination at detect-ing a significant patent ductus arteriosus in the preterm neonate?Arch Dis Child.2003;88:85– 86
7. Skinner J. Diagnosis of patent ductus arteriosus.Semin Neonatol.2001; 6:49 – 61
8. Evans N. Current controversies in the diagnosis and treatment of patent ductus arteriosus in preterm infants.Adv Neonatal Care.2003;3:168 –177 9. Pesonen E. Role of natriuretic hormones in the diagnosis of patent
ductus arteriosus in newborn infants.Acta Paediatr.2001;90:363–365 10. Holmstrom H, Omland T. Natriuretic peptides as markers of patent
ductus arteriosus in preterm infants.Clin Sci (Lond).2002;103:79 – 80 11. Holmstrom H, Hall C, Thaulow E. Plasma levels of natriuretic peptides
and hemodynamic assessment of patent ductus arteriosus in preterm infants.Acta Paediatr.2001;90:184 –191
12. Puddy VF, Amirmansour C, Williams AF, Singer DR. Plasma brain natriuretic peptide as a predictor of haemodynamically significant patent ductus arteriosus in preterm infants.Clin Sci (Lond).2002;103: 75–77
13. Lee JY, Seo WH, Choi BM, et al. Changes of plasma brain natriuretic peptide according to the changes of ductal shunt in healthy preterm infants.J Korean Pediatr Cardiol.2003;7:128 –137
14. Sahn DJ, DeMaria A, Kisslo J, Weyman A. Recommendations regarding quantitation in M-mode echocardiography: results of a survey of echo-cardiographic measurements.Circulation.1978;58:1072–1083
15. Suzumura H, Nitta A, Tanaka G, Arisaka O. Diastolic flow velocity of the left pulmonary artery of patent ductus arteriosus in preterm infants.
Pediatr Int.2001;43:146 –151
16. Nakao K, Mukoyama M, Hosoda K, et al. Biosynthesis, secretion, and receptor selectivity of human brain natriuretic peptide.Can J Physiol Pharmacol.1991;69:1500 –1506
17. Yasue H, Yoshimura M, Sumida H, et al. Localization and mechanism of secretion of B-type natriuretic peptide in comparison with those of A-type natriuretic peptide in normal subjects and patients with heart failure.Circulation.1994;90:195–203
18. Holmes SJ, Espiner EA, Richards AM, Yandle TG, Frampton C. Renal, endocrine, and hemodynamic effects of human brain natriuretic peptide in normal man.J Clin Endocrinol Metab.1993;76:91–96
19. Levin ER, Gardner DG, Samson WK. Natriuretic peptides.N Engl J Med.
1998;339:321–328
20. Nakagawa O, Ogawa Y, Itoh H, et al. Rapid transcriptional activation and early mRNA turnover of brain natriuretic peptide in cardiocyte hypertrophy. Evidence for brain natriuretic peptide as an “emergency” cardiac hormone against ventricular overload.J Clin Invest. 1995;96: 1280 –1287
21. Maeda K, Tsutamoto T, Wada A, Hisanaga T, Kinoshita M. Plasma brain natriuretic peptide as a biochemical marker of high left ventricular end-diastolic pressure in patients with symptomatic left ventricular dysfunction.Am Heart J.1998;135:825– 832
22. Tsutamoto T, Wada A, Maeda K, et al. Attenuation of compensation of endogenous cardiac natriuretic peptide system in chronic heart failure: prognostic role of plasma brain natriuretic peptide concentration in patients with chronic symptomatic left ventricular dysfunction. Circu-lation.1997;96:509 –516
23. Mair J, Friedl W, Thomas S, Puschendorf B. Natriuretic peptides in assessment of left-ventricular dysfunction.Scand J Clin Lab Invest Suppl.
1999;230:132–142
25. Nagaya N, Nishikimi T, Uematsu M, et al. Plasma brain natriuretic peptide as a prognostic indicator in patients with primary pulmonary hypertension.Circulation.2000;102:865– 870
26. Koglin J, Pehlivanli S, Schwaiblmair M, Vogeser M, Cremer P, vonSc-heidt W. Role of brain natriuretic peptide in risk stratification of patients with congestive heart failure.J Am Coll Cardiol.2001;38:1934 –1941 27. Cheng V, Kazanagra R, Garcia A, et al. Rapid bedside test for B-type
peptide predicts treatment outcomes in patients admitted for decom-pensated heart failure: a pilot study.J Am Coll Cardiol.2001;37:386 –391 28. Maisel AS. Use of BNP levels in monitoring hospitalized heart failure
patients with heart failure.Heart Fail Rev.2003;8:339 –344
29. Troughton RW, Frampton CM, Yandle TG, Espiner EA, Nicholls MG, Richards AM. Treatment of heart failure guided by plasma aminoter-minal brain natriuretic peptide (N-BNP) concentrations.Lancet.2000; 355:1126 –1130
30. Ootaki Y, Yamaguchi M, Yoshimura N, Oka S, Yoshida M, Hasegawa T. Secretion of A-type and B-type natriuretic peptides into the blood-stream and pericardial space in children with congenital heart disease.
J Thorac Cardiovasc Surg.2003;126:1411–1416
31. Suda K, Matsumura M, Matsumoto M. Clinical implication of plasma natriuretic peptides in children with ventricular septal defect.Pediatr Int.2003;45:249 –254
32. Yoshibayashi M, Kamiya T, Saito Y, et al. Plasma brain natriuretic peptide concentrations in healthy children from birth to adolescence: marked and rapid increase after birth.Eur J Endocrinol.1995;133:207–209 33. Koch A, Singer H. Normal values of B type natriuretic peptide in
infants, children, and adolescents.Heart.2003;89:875– 878
34. Silverman NH, Lewis AB, Heymann MA, Rudolph AM. Echocardio-graphic assessment of ductus arteriosus shunt in premature infants.
DOI: 10.1542/peds.2004-1837 originally published online February 1, 2005;
2005;115;e255
Pediatrics
Hong, Chang Sung Son and Joo Won Lee
Byung Min Choi, Kee Hyoung Lee, Baik Lin Eun, Kee Hwan Yoo, Young Sook
Patent Ductus Arteriosus in Preterm Infants
Utility of Rapid B-Type Natriuretic Peptide Assay for Diagnosis of Symptomatic
Services
Updated Information &
http://pediatrics.aappublications.org/content/115/3/e255
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/115/3/e255#BIBL
This article cites 33 articles, 10 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/cardiology_sub Cardiology
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_ Fetus/Newborn Infant
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2004-1837 originally published online February 1, 2005;
2005;115;e255
Pediatrics
Hong, Chang Sung Son and Joo Won Lee
Byung Min Choi, Kee Hyoung Lee, Baik Lin Eun, Kee Hwan Yoo, Young Sook
Patent Ductus Arteriosus in Preterm Infants
Utility of Rapid B-Type Natriuretic Peptide Assay for Diagnosis of Symptomatic
http://pediatrics.aappublications.org/content/115/3/e255
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.