RESEARCH ARTICLE
VENTILATORY FUNCTION RESPONSE TO TRAINING OF CERVICAL MUSCLES IN MECHANICAL
NECK PAIN: A RANDOMIZED CONTROLLED STUDY
1, *
Sumaya S. Mohamed,
2Aisha A. Hagag,
2Mohamed A. Shendy and
3Mohammed M. El-Batanony
1Department of Physical Therapy, of Outpatient Clinics, Cairo University Hospitals, Egypt
2Department of Physical Therapy for Cardiovascular/ Respiratory Disorders and Geriatrics,
Faculty of Physical Therapy, Cairo University, Egypt
3Department of Occupational Medicine, Faculty of Medicine, Cairo University, Egypt
ARTICLE INFO ABSTRACT
Background: Neck pain is a common musculoskeletal complaint with tremendous impact on
health and quality of life. Neck pain also leads to pulmonary function restrictive disorder. Aim:
This study aimed to investigate the effect of deep cervical muscle training using pressure biofeedback
device on ventilatory functions in patients with chronic mechanical neck pain. Subjects: Forty
subjects of both sexes with mean age 24.8± 1.87 years were participated in this study. They were divided into two groups equal in number; the study group (A) and the control group (B) who were
suffering from chronic mechanical neck pain. Methods: Group A received deep cervical flexor
strengthening exercises and traditional physical therapy modalities. Group B received only traditional physical therapy modalities. Both groups were assessed using the neck disability index questionnaire for functional disability, visual analogue scale for pain intensity, craniocervical flexion test for deep cervical flexor muscle strength and spirometric tests for ventilatory functions. Patients were assessed
before and after treatment. Results: The results of this study showed that there was significant
improvement in craniocervical flexion test, maximum voluntary ventilation and peak expiratory flow rate in the study group only (p = 0.0001). There was a statistically significant improvement in neck disability index (p = 0.0001), visual analogue scale (p= 0.0001), forced vital capacity (p = 0.002) and forced expiratory volume in 1 second (p= 0.01) in both groups, however, there
was no statistically significant difference between both groups. Conclusion: It is concluded that deep
cervical flexor strengthening exercise combined with traditional physical therapy modalities have better clinical effects on the mechanical neck pain and ventilatory functions than traditional physical therapy modalities alone in patients with chronic mechanical neck pain.
INTRODUCTION
Mechanical neck pain (MNP) is typically reported as diffuse, nonspecific pain, especially with neck movements (1). Activity related neck pain is a prominent symptom of most mechanical neck disorders (MND) which include whiplash assossciated disorders, torticollis and myofascial neck pain (2). Neck pain is a common disabling and costly musculoskeletal disorder with a mean overall prevalence in the general population of approximately 23% (3). It is more common during middle age, with females recording higher prevelance than males (4). MNP may include symptoms in the neck and upper extremity (5). It is characterized by insidious onset, which could originate from multiple factors such as depression, anxiety, poor posture and muscle strain arising from participation in sports and occupational antecedents (6). Its course is characterized by periods of remission and exacerbation, but the majority of patients do not completely recover from their symptoms (7). In addition to neck pain, patients with chronic MNP present with various motor dysfunctions, such as an inhibition of deep cervical flexor
*Corresponding author: Sumaya S. Mohamed,
Department of Physical Therapy, of Outpatient Clinics, Cairo University Hospitals, Egypt
(DCF) muscle activation accompanied by hyperactivity and increased fatigability of the superficial neck flexors, increased forward head posture (FHP), (8, 9), sensorimotor disturbances in the form of decreased proproception, neuromuscular disturbances and psychosocial dysfunction (8). Pulmonary function tests (PFT) represents an important part in respiratory medicine. Spirometry is a common test of pulmonary function that provides information regarding the presence of obstruction or possible restriction in people with suspected pulmonary dysfunction (10). Pulmonary restriction is a term used to describe a group of respiratory disorders related to an impaired filling of the lungs with air (11). This predisposes to reduction of lung volumes, respiratory flows and maximum voluntary ventilation (MVV), which are the characteristic and diagnostic signs of restrictive disorders. This is particularly apparent in cases of neuromuscular weakness (12). Neuromuscular weakness is also a physical sign in musculoskeletal pain conditions (11). It was hypothesised that the observed respiratory dysfunction in chronic neck pain patients are caused by: weakness of the deep neck flexor and extensor muscles, reduced stability of the cervical and thoracic spine and changes in rib cage mechanics (13). These mechanical changes leads to alterations in the force length curves of the sternocleidomastoid muscles due to muscle hyperactivity and restricted range of motion of the cervical spine (13). Muscular Article History:
Received 17th November, 2018
Received in revised form 29th December, 2018
Accepted 25th January, 2019
Published online 28th February, 2019
International Journal of Recent Advances in Multidisciplinary Research
Vol. 06, Issue 02, pp.4617-4622, February, 2019
Keywords:
performance of DCF can be increased with the use of pressure biofeedback unit (PBU) training (14). It is generally true that PBU training facilitates effective contraction of the DCF muscles (14, 15), by bending the head instead of the neck through a nodding action so that the DCF musles are activated as opposed to the activation of the superficial ones. Hence, normal neck postures and arrangement are recovered (15). This study was conducted to investigate the effect of DCF training on ventilator functions and deep cervical muscle strength and to find out the effect of this technique on pain and functional disability in patients with MNP.
PATIENTS AND METHODS
This study is a randomized controlled trial which was approved by the ethical committee of the Faculty of Physical Therapy, Cairo University. Approval from all patients was formally obtained by signing a consent form. This study was conducted in the out clinic of Faculty of Medicine, Cairo University. Forty patients ofboth genders (14 males and 26 females) with chronic MNP were enrolled in this study under the following inclusion criteria: age 20- 30 years old, neck pain duration from six to twelve months and pain complaints at least once per week, body mass index (BMI) < 30 kg/m2 and non smoker patients (current or past). Exclusion criteria were current or past smokers, BMI > 30 kg/m2, pain in any other non related body area, history of: neck pain of traumatic origin, clinical abnormalities or surgeries of the thoracic cage or vertebral column, occupational industrial exposures, serious comorbidities and malignancies.Patients were divided into two groups: Group (A): study group included 20 patients (8 males and 12 females) who received cervical muscle training plus the traditional physical therapy program and Group (B): control group included 20 patients (6 males and 14 females) who received traditional physical therapy program only. Subjects were classified as having MNP based on presence of FHP and protracted shoulders (16), tender trapezius, levator scapulae, rhomboids, supraspinatus, and infraspinatus muscles on palpation (17) and weakness of DCF muscles that stabilize the cervical spine measured by craniocervical flexion test (CCFT) (18). All subjects were familiarized with the objectives, equipment and procedures of the study and received sessions 3 times per week for a total period of 4 weeks.
Instrumentation
Instrumentation for cervical evaluation: 1- PBU
(Chattanooga group, Australia, no: 657277) was used to assess the endurance of the DCF by performing the (CCFT). 2- Neck pain intensity, pain induced disability and physical activity level were assessed by adminstration of visual analogue scale (VAS) and the neck disability index (NDI) questionnaire.
Instrumentation for pulmonary function evaluation:
Pulmonary function tests were assessed by using a spirometer (APS-PRO Jaeger, serial no. 201484-146402, Germany).
Instrumentation for treatment: Traditional physical therapy
modalities: utrasound (Phyaction CL- uniphy, serial no. 70408, Belgium) and thermal agent (infrared lamp) and the PBU to strength the DCF.
Outcome measures
Initially, demographic data and patient characteristics were collected, including age, weight (kg) (measured to the nearest
0.1 kg using a standard weight scale) and height (cm) (measured to the nearest 0.1 cm with subject standing erect against a vertical scale). Pain intensity was assessed using the VAS. It represents a horizontal line of 10 cm with word anchors at each end representing the extreme feelings. Patients indicated the point on the line that best corresponded to the pain (19, 20). The NDI questionnaire (score out of 50) was used to measure the patient’s perceived disability resulting from their neck pain. There are ten sections in this questionnaire and each section is scored 0-5 points. Its interpretation is 0-20% minimal disability, 21-40% moderate, 41-60% severe, 61-80% crippled and 81-100% bed bound (8). The DCF endurance was examined using the PBU to perform the CCFT (11). CCFT was performed with the subjects in crook lying position. With the PBU placed beneath the occiput and inflated to baseline of 20 mmHg, patients were instructed to perform head nodding. The test consists of 5 incremental stages (22, 24. 26,28 and 30 mm Hg). Three repetitions in each increment were required before progressing to the next one.The test was continued in the same fashion until successful completion (three ten-second holds at 30 mmHg) or substitution of activity of SCM or scaleni was observed or palpated, overshooting target pressure, neck retraction and dial needle flickering (21). Pulmonary function tests or spirometry was performed by using a spirometer (22). Forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), peak expiratory flow rate (PEF) and maximum voluntary ventilation (MVV) were measured by spirometer (23). All PFT were carried out at a fixed time of the day to minimize diurnal variation (8). A nose clip was used to avoid any potential air leakage and patients sealed their mouths around a disposable mouthpiece and were verbally encouraged to breathe in and out through it (11). The patients were asked to perform a rapid full inspiration, followed by a non hesitated maximum forced expiration, then ending by another rapid maximum inspiration (24).The test was repeated three times and the maximum of the 3 trials was obtained (8).
Treatment procedures
1. Traditional physical therapy program
a. Thermal agent (infrared lamp): Infrared irradiation
was applied for 20 min at a 40 cm distance from the neck region (25).
b. Therapeutic ultrasound: Ultrasound was applied on
myofascial trigger points to decrease the pain (26, 27). The continuous ultrasound was used with 1.5 W/cm2 intensity and at a frequency of 1 MHz over the neck area for 10 minutes (25).
2. DCF training: Pressure biofeedback unit training facilitates
effective contraction of the DCF muscles instead of superficial muscles (14, 15). DCF training started with the same preparatory steps of the CCFT. Patients were then instructed to perform head nodding and to hold it for 10 seconds starting with 22 mm Hg increment level and progressively targeting all the 5 increments till 30 mm Hg. Minimum requirement for satisfactory performance was 26 mmHg while 28 and 30 mmHg were targets for ideal performance (21). Training included 3 sets in a session, 10 repetitions per set with 2 minutes rest between sets (28).
Data collection: All the outcome measures were collected for
Statistical Analysis: All statistical analyses were performed using the statistical package for social studies (SPSS) version 19 for windows. Descriptive statistics and t- test was conducted for comparison of the mean age and BMI of both groups. Chi squared test was conducted for comparison of sex distribution between both groups. T-test was conducted for comparison of NDI, VAS, CCFT, FVC, FEV1, MVV and PEF between both groups. Paired t-test was conducted for comparison between pre and post treatment mean values of NDI, VAS, CCFT, FVC, FEV1, MVV and PEF in each group. The level of significance for all statistical tests was set at p≤ 0.05.
RESULTS
Comparing the demographic characteristics of the subjects of both groups revealed that there was no significant difference between both groups in the mean age and BMI (p > 0.05) and no significant difference between both groups in sex distribution (p = 0.5), as shown in Table 1.
NDI, VAS and CCFT in both groups: As shown in Table 2,
there was no significant difference between the study and control groups pre treatment regarding the NDI (p=0.44), VAS(p=0.38)andCCFT(p=0.12),whiletherewasasignificant decrease in the NDI in both the study group and control group as well as, a significant decrease in the VAS in both groupspost-treatmentcomparedwithpre-treatment(p= 0.0001).
The study group had a significant increase in the CCFT post treatment compared with pre treatment (p=0.0001), however, the changes were non significant in the control group (p = 0.11). T-test for comparison between post treatment mean values of CCFT of study and control groups showed a significant increase in CCFT of the study group compared with that of control group post treatment (p = 0.0001), however no significant difference was noted in NDI and VAS between both groups.
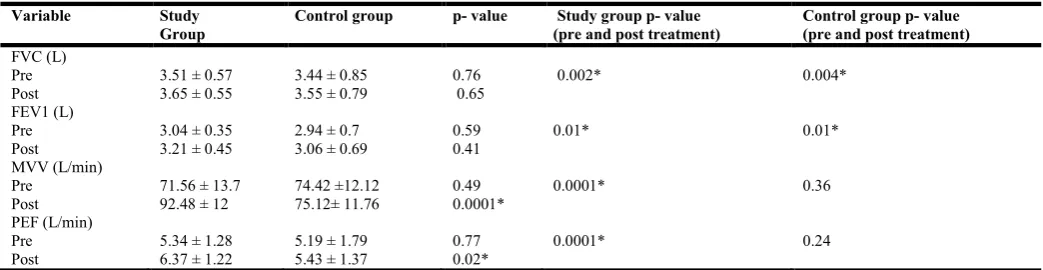
FVC, FEV1, MVV and PEF in both groups: Table 3 showed
that there was no significant difference in the FVC (p=0.76), FEV1 (p=0.59), MVV (p=0.49) and PEF (p=0.77) between the study and control groups pre treatment, while there was a significant increase in the FVC (p=0.002) and FEV1 (p=0.01) values in the study group post-treatment compared with pre-treatment. Almost similar changes were noted in FVC (p=0.004) and FEV1 in the control group (p=0.01). MVV and PEF increased significantly in the study group post- treatment compared to pre-treatment (p=0.0001), however the same variables showed no significant difference in the control group post- treatment. T-test for comparison between post treatment mean values of MVV and PEF between both groups post treatment showed a significant increase in study group compared to control group; (p=0.0001) for MVV and (p=0.02) for PEF. However, non significant difference was foundintheFVCandFEV1betweenstudyandcontrolgroups post treatment; (p= 0.65) for FVC and (p=0.41) for FEV1.
Table 1. Descriptive statistics for the mean age, sex and BMI of study and control groups
Variable Study group n=20 Control group n=20 p-value
Age (years) 24.65 ± 2.05 24.9 ± 1.68 0.67
Sex (male/ female) female: n=12 (60%) and
male: n=8 (40%)
female: n=14 (70%) and
male: n=6 (30%) 0.5
BMI( Kg/m2) 25.23 ± 2.08 24.34 ± 2.93 0.27
Significance set at p≤ 0.05; n: number .
Table 2. Means and p-values for NDI, VAS and CCFT pre and post treatment in both groups
Variable Study group Control group p- value Study group p-value (pre and post treatment)
Control group p-value (pre and post treatment)
NDI (%) Pre Post
26.85 ± 3.54 8.75 ± 2.09
25.7 ± 5.55 10.25 ± 3.66
0.44
0.12 0.0001* 0.0001*
VAS Pre Post
6 ± 1.45 1.9 ± 0.71
5.6 ± 1.42 2.2 ± 0.89
0.38
0.24 0.0001* 0.0001*
CCFT (mm Hg) Pre
Post
23.6 ± 1.39 29.3 ± 0.97
23 ± 1.02 23.55 ± 1.6
0.12
0.0001* 0.0001* 0.11
Data was expressed in means ± SD; NDI: neck disability index; VAS: visual analogue scale; CCFT: craniocervical flexion test; *: significant where p≤ 0.05.
Table 3. Mean and p-values for FVC, FEV1, MVV and PEF pre and post treatment in both groups
Variable Study
Group
Control group p- value Study group p- value (pre and post treatment)
Control group p- value (pre and post treatment)
FVC (L) Pre Post
3.51 ± 0.57 3.65 ± 0.55
3.44 ± 0.85 3.55 ± 0.79
0.76 0.65
0.002* 0.004*
FEV1 (L) Pre Post
3.04 ± 0.35 3.21 ± 0.45
2.94 ± 0.7 3.06 ± 0.69
0.59 0.41
0.01* 0.01*
MVV (L/min) Pre
Post
71.56 ± 13.7 92.48 ± 12
74.42 ±12.12 75.12± 11.76
0.49 0.0001*
0.0001* 0.36
PEF (L/min) Pre Post
5.34 ± 1.28 6.37 ± 1.22
5.19 ± 1.79 5.43 ± 1.37
0.77 0.02*
0.0001* 0.24
DISCUSSION
The present study investigated the ventilatory functions response to training of DCF muscles using PBU in patients with chronic MNP. The current results indicated that improvements in ventilatory functions were more marked in the study group compared to the control group. Our results regarding the significant improvements in NDI and VAS in both groups post-intervention as compared to pre-intervention, were similar to the results found by (Amr and Amira) in which they stated that there was a significant decrease in the VAS and a significant improvement of the NDI after one month of intervention in both groups, one group received ultrasound, thermotherapy and TENS and the other one received the same modalities in addition to DCF strength exercise (25). However, (Chan and colleagues) used only thermotherapy and TENS for his control group and proved non significant changes in both the NDI and VAS post-treatment compared to pre-post-treatment (29). (Jasper and colleagues, Graham and colleagues) also considered the ultrasound to be of no benefit in reduction of neck pain (30, 31). Contradictory results were found by (Sihawong and colleagues) regarding the DCF training, as they investigated the effects of an exercise program focusing on muscle stretching and endurance training on the 12-month incidence rate of neck pain in office workers. Using NDI and VAS in their assessment, they found that there was no significant difference in these variables between the intervention and control groups (32). The thermal and non-thermal effects of US would transiently increase the flexibility of tendons, ligaments, and joint capsules, which consequently decreases joint stiffness, pains, and accompanying muscle spasm and temporarily increases blood flow (33) ; (25). Thermotherapy is recommended by practitioners for chronic neck pain patients (34) ; (35) due to its physiological effects of increasing blood flow and metabolism, and increasing elasticity of connective tissue, thereby relieving pain (36) ; (37).
The FHP of subjects with chronic neck pain (26, 38), has been associated with compressive loading of the cervical tissues (25, 39). The improved cervical posture created through DCF exercise, may have an additional long-term benefit of reducing recurrent episodes of neck pain (25, 40). The results of the current study proved that DCF training exercises lead to a significant increase in the CCFT values, thereby reflecting improvements in strength and endurance of the DCF muscles of the study group compared to the control group. These results agreed with (Izquierdo and colleagues) as they proved significant improvements in the CCFT in the group receiving DCF training (41). However, these results disagree with (O'Leary and colleagues) as they found that the group receiving DCF exercise using the PBU, didn't have any significant increase in strength and endurance (42). DCF exercise, is an exercise/examination method that is characterized by low loading and induces proper postures and activation of deep, instead of superficial, muscles (15, 43). This method bends the head instead of the neck so that the DCF muscles are activated as opposed to activation of the SCM and AS. Hence, normal neck postures and arrangement are recovered (15, 44). The significant improvements in FVC and FEV1 of the control group in the current study, is suggested to be due to the physiological effects of heating therapy on muscles stated above. Therefore, relaxation of the shortened accessory respiratory muscles and increase of its
flexibility is thought to be a reason for improving respiratory function and increasing the FVC and FEV1 values. (Izquierdo and colleagues, Jull and colleagues) considered DCF training as a form of exercise that enhances the DCF activation, restores the coordination between the deep and superficial cervical flexors and enhances the neuromuscular control of the cervical flexor muscles (41, 45). MVV is suggested to be an indicator of neuromuscular control (13, 46) and is affected by loss of co-ordination of respiratory muscles (47). Therefore, this crucial role of DCF muscles in neuromuscular control and cervical stability is a good explanation for the significant increase of MVV in the study group only. However (Kennedy and colleagues) proved that DCF are capable of only small peak flexion torque or compression forces, therefore have a limited capacity to contribute to cervical stability (48). PEFR is the maximum rate of flow in forced expiration starting from full inspiration. PEFR not only reflects airway calibre but also muscle strength and voluntary effort (49).
Since DCF training improves the strength and endurance of the DCF and corrects the muscle imbalance between the superficial and deep flexors, thus this explains the statistically significant increase in the PEFR in the study group which is dependent on muscle strength and voluntary effort. A study by (Jintae a n d colleagues) proved that the FVC and FEV1 were statistically decreased in the FHP group as compared to the normal posture group. They stated that this was due to the weakness of cervical muscles secondary to the bad neck posture, which in turn decreased the FVC and FEV1 (50). Weaknesses of the neck muscles resulted in a FHP in addition to decline in thoracic mobility (9, 51), which means increased kyphosis in the upper thoracic region and a reduction in the volume of the thorasic cage. This creates a resistance to exhalation and therefore lowers the FVC and FEV1. DCF has a major postural function in supporting and straightening the cervical lordosis (52, 53). Therefore, retraining the DCF muscles improves the ability to maintain an upright posture of the cervical spine which decreases the FHP (53, 54). This proves our results, as the DCF training corrected the FHP which in turn lead to significant improvement in FVC and FEV1in the study group.
Conclusion
The results of this study supported the importance of management of neck pain using deep cervical flexor training program and its effect on improving the ventilatory functions.
REFERENCES
1. Daniels J. and Rebecca M. (2011): The cervical spine. Common Musculoskeletal Problems: A Handbook; chapter 2, 5-13: Springer, Newyork.
2. Ajediran Bello, Jacquelyn A. and Emmanuel Bonney (2015): Comparative effects of portable and stationary traction in the management of mechanical neck disorders. Rehabilitation Process and Outcome; 4: 1–6.
3. Hoy D., Protani M., De R. and Buchbinder R. (2010): The epidemiology of neck pain. Best Practices in Clin Rheumatol; 24(6):783-792.
pain: Rationale and design of a randomized controlled trial. BMC Musculoskeletal Disord J; 11(1): 11-14.
5. Manuel Saavedra-Hernadez, Adelaida M. Castro-Sanchzer, Manuel Arroyo-Morales and Joshua A. Cleland (2012): short term effects of kinesio taping versus cervical thrust manipulation in patients with mechanical neck pain :a randomized clinical trial. Journal of Orthopaedic and Sports Physical Therapy 42 (8): 724–730
6. Clair D., Edmondston S. and Allison G. (2006): Physical therapy treatment dose for non-traumatic neck pain: a comparison between two patient groups. Orthop Sports Phys Ther J; 36(11): 867–875.
7. Cote P., Cassidy J., Carroll L. and Kristman V. (2004): The annual incidence and course of neck pain in the general population: a population- based cohort study. Pain; 112(3): 267-273.
8. Kapreli E., Vourazanis E., Billis E., Oldham J. and Strimpakos N. (2009): Respiratory dysfunction in chronic neck pain patients: A pilot study. Cephalgia J; 29(7): 701-10.
9. Wirth B., Amstalden M., Perk M., Boutellier U. and Humphreys B. (2014): Respiratory dysfunction in patients with chronic neck pain- Influence of thoracic spine and chest mobility. Manual Therapy J; 19(5): 440–444.
10.Ruppel G. (2009): Manual of pulmonary function testing; 9th ed. El Sevier, Mosby (U.S.A.)
11.Zacharis Dimitriadis, Eleni Kapreli, Nikolaos Strimpakos and Jacqueline Oldham (2014): Pulmonary function of patients with chronic neck pain: A spirometry study. Respir Care; 59(4): 543-549.
12.Perrin C., Unterborn J., Ambrosio C. and Hill N. (2004): Pulmonary complications of chronic neuromuscular diseases and their management. Muscle Nerve; 29(1): 5-27. 13.Kapreli E., Vourazanis E. and Strimpakos N. (2008): Neck pain causes respiratory dysfunction. Medical Hypotheses; 70(5): 1009-1013.
14.Dong Yeon. (2015): Deep cervical flexor training with a pressure biofeedback unit is an effective method for maintaining neck mobility and muscular endurance in college students with forward head posture. Journal of Physical Therapy Science; 27(10): 3207-3210.
15.Jin Kim and Kwang Kwag. (2016): Clinical effects of deep cervical flexor muscle activation in patients with chronic neck pain. Journal of Physical Therapy Science; 28(1): 269-273.
16.Joshua A., John D., Julie M. Fritz and Julie M. Whitman. (2006): Interrater reliability of the history and physical examination in patients with mechanical neck pain. Archives of Physical Medicine and Rehabilitation; 87(10): 1388-1395.
17.Duyur B., Genc H., Altuntas V. and Erdem H. (2009): Disability and related factors in patients with chronic cervical myofascial pain. Clin Rheumatol; 28(6): 647–654 18.James G. and Doe T. (2010): The craniocervical flexion
test: intra- tester reliability in asymptomatic subjects. Physiother Res Int; 15(3): 144-149.
19.Klimek L., Bergmann K., Biedermann T., Bousquet J., Hellings P., Jung K., et al. (2017): Visual analogue scales (VAS): measuring instruments for the documentation of symptoms and therapy monitoring in cases of allergic rhinitis in everyday health care. Allergo J Int: 26(1):16–24. 20.Doulaptsi M., Prokopakis E., Seys S., Pugin B., Steelant B.
and Hellings P. (2018): Visual analogue scale for sino-nasal symptoms severity correlates with sino-sino-nasal outcome test 22: Paving the way for a simple outcome tool
of CRS burden. Clinical and Translational Allergy; 8(1): 1-6.
21.Nezamuddin M., Shahnawaz Anwer, Sohrab Khan and Ameed Equebal (2013): Efficacy of pressure-biofeedback guided deep cervical flexor training on neck pain and muscle performance in visual display terminal operators. Journal of Musculoskeletal Research; 16(3): 1-8.
22.Duu Wen Sewa and Thun How Ong. (2014): Pulmonary Function Test: Spirometry. Proceedings of Singapore Healthcare; 23(1): 57-64.
23.Booker R. (2009): Interretation and evaluation of pulmonary function tests. Nurs Stand J; 23(39): 46-56. 24.Jintae Han, Soojin Park, Youngju Kim, Yeonsung Choi and
Hyeonnam Lyu. (2016): Effects of forward head posture on forced vital capacity and respiratory muscles activity. Phys Ther Sci J; 28(1): 128–131.
25.Amr Almaz Abdel-aziem & Amira Draz. (2016): Efficacy of deep neck flexor exercise for neck pain: A randomized controlled study. Turk J Phys Med Rehab; 62(2): 107-115. 26.Peng Xia, Xiaoju Wang, Qiang Lin, Kai Cheng, and
Xueping Li. (2017): Effectiveness of ultrasound therapy for myofascial pain syndrome: a systematic review and meta-analysis. J Pain Res; 10: 545–555.
27.Almir Vieira, Alessandra Kelly, Carlos Eduardo, Fabiana Rodrigues and Rinaldo Roberto. (2017): Additional effect of static ultrasound and diadynamic currents on myofascial trigger points in a manual therapy program for patients with chronic neck pain: A randomized clinical trial. American Journal of Physical Medicine and Rehabilitation; 96(4): 243–252.
28.Zaheen Iqbal, Reena Rajan, Sohrab Khan and Ahmad Alghadir. (2013): Effect of deep cervical flexor muscles training using pressure biofeedback on pain and disability of school teachers with neck pain. Journal of Physical Therapy Science; 25(6): 657-661.
29.Chan Y., Wang T., Chang C., Chen L., Chu H., Lin S., et al. (2015): Short-term effects of self-massage combined with home exercise on pain, daily activity and autonomic function in patients with myofascial pain dysfunction syndrome. Journal of Physical Therapy Science; 27(1):217–221.
30.Jasper D., Wendy G., Scholten Peeters, Bart J., Jan Pool, Maurits W., et al. (2017): Clinical practice guideline for physical therapy assessment and treatment in patients with nonspecific neck pain. Physical Therapy; 98(3): 162–171. 31.Graham N., Gross A., Carlesso L., Santaguida P.,
Macdermid J., Walton D., et al. (2013): An icon overview on physical modalities for neck pain and associated disorders. Open Orthop J; 7(4): 440–460.
32.Sihawong R., Janwantanakul P. and Jiamjarasrangsi W. (2013): Effects of an exercise programme on preventing neck pain among office workers: a 12-month cluster-randomised controlled trial. Occupational and Environmental Medicine; 71(1): 63–70.
33.Unalan H., Majlesi J., Aydin F. and Palamar D.(2011): Comparison of high-power pain threshold ultrasound therapy with local injection in the treatment of active myofascial trigger points of the upper trapezius muscle. Arch Phys Med Rehabil; 92(4): 657–662.
34.Wolsko P., Eisenberg D., Davis R., Kessler R. and Phillips R. (2003): Patterns and perceptions of care for treatment of back and neck pain: results of a national survey. Spine; 28: 292–297.
Thermotherapy self-treatment for neck pain relief: A randomized controlled trial. European Journal of Integrative Medicine; 4(4): 371–378.
36.Nadler S., Weingand K. and Kruse R. (2004): The physiologic basis and clinical applications of cryotherapy and thermotherapy for the pain practitioner. Pain Physician; 7: 395–399.
37.Gerard A., Ning Yan and Jill Stark. (2015): Mechanisms and efficacy of heat and cold therapies for musculoskeletal injury. Postgraduate Medicine; 127(1): 57-65.
38.Szeto G., Straker L. and O'Sullivan P. (2005): Comparison of symptomatic and asymptomatic office workers performing monotonous keyboard work--2: Neck and shoulder kinematics. Man Ther; 10: 281-91.
39.Harms-Ringdahl K., Ekholm J., Schüldt K., Németh G. and Arborelius U. (1986): Load moments and myoelectric activity when the cervical spine is held in full flexion and extension. Ergonomics; 29: 1539-52.
40.Falla D., Jull G., Russell T., Vicenzino B. and Hodges P. (2007): Effect of neck exercise on sitting posture in patients with chronic neck pain. Phys Ther; 87: 408-417.
41.Izquierdo T., Pecos-Martin D., Girbaes E., Plaza-Manzano G., Caldentey R., Melus R., et al. (2016): Comparison of cranio-cervical flexion training versus cervical proprioception training in patients with chronic neck pain: A randomized controlled clinical trial. Journal of Rehabilitation Medicine; 48(1): 48–55.
42.O’Leary S., Jull G., Kim M., Uthaikhup S. and Vicenzino B. (2012): Training Mode–Dependent Changes in Motor Performance in Neck Pain. Archives of Physical Medicine and Rehabilitation; 93(7): 1225–1233.
43.Rubini E., Costa A. and Gomes P. (2007): The effects of stretching on strength performance. Sports Med; 37: 213– 224.
44.Jull G., Falla D. and Hodges P. (2005): Cervical flexor muscle retraining: physiological mechanisms of efficacy. Paper presented at: 2nd International Conference on Movement Dysfunction. Scotland.
45.Jull G., Falla D., Vicenzino B. and Hodges P. (2009): The effect of therapeutic exercise on activation of the deep cervical flexor muscles in people with chronic neck pain. Man Ther ; 14: 696–701.
46.Kahlaee A., Ghamkhar L. and Arab A. (2017): The association between neck pain and pulmonary function. American Journal of Physical Medicine and Rehabilitation; 96(3): 203–210.
47.Imtiaz Rasool, Shamim Jabeen and Abdul Munnan Durrani. (2001): Maximum voluntary ventilation values in young kashmiri adults through electronic spirometery. JK-Practitioner; 8(4): 235-236.
48.Kennedy E., Albert M., and Nicholson H. (2017): Do longus capitis and colli really stabilise the cervical spine: A study of their fascicular anatomy and peak force capabilities. Musculoskeletal Science and Practice; 32: 104–113.
49.Dobra R. and Equi A. (2017): How to use peak expiratory flow rate. Archives of Disease in Childhood - Education and Practice Edition; 103(3): 158–162.
50.Jintae Han, Minji Go and Yeong-Ju Kim. (2015): Comparison of forced vital capacity and maximal voluntary ventilation between normal and forward head posture. J Korean Soc Phys Med; 10(1): 83-89.
51.Han J., Park S., Kim Y., Choi Y. and Lyu H. (2016): Effects of forward head posture on forced vital capacity and respiratory muscles activity. Journal of Physical Therapy Science; 28(1), 128–131.
52.Dusunceli Y. (2009): Efficacy of neck stabilization exercises for neck pain: a randomized controlled study. J Rehabil Med; 41(8): 626-631.
53.Gupta B., Aggarwal S., Gupta B., Gupta M. and Gupta N. (2013): Effect of deep cervical flexor training vs. conventional isometric training on forward head posture, pain, neck disability index in dentists suffering from chronic neck pain. Journal of Clinical and Diagnostic Research; 7(10): 2261-2264.
54.Jull G., O’Leary S. and Falla D. (2008): Clinical assessment of the deep cervical flexor muscles: The craniocervical flexion test. Journal of Manipulative and Physiological Therapeutics; 31(7): 525–533.
.