1
2015-2016 DATA COLLECTION INSTRUMENT
FOR PRELIMINARY ACCREDITATION2
STANDARD 6: COMPETENCIES, CURRICULAR OBJECTIVES, AND CURRICULAR DESIGN
The faculty of a medical school define the competencies to be achieved by its medical students through medical education program objectives and is responsible for the detailed design and implementation of the components of a medical curriculum that enable its medical students to achieve those competencies and objectives. Medical education program objectives are statements of the knowledge, skills, behaviors, and attitudes that medical students are expected to exhibit as evidence of their achievement by completion of the program.
3
OVERVIEW : SUPPORTING DOCUMENTATION FOR STANDARD 6
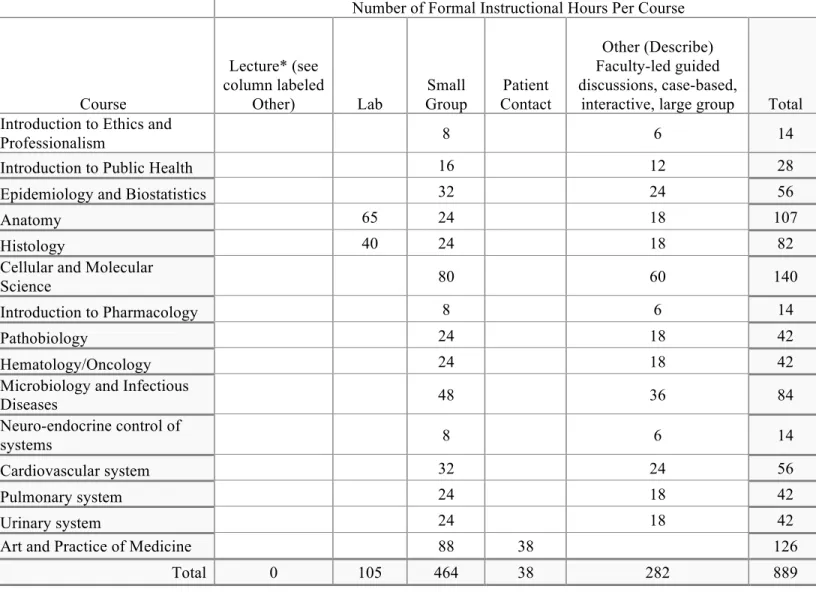
Table 6.0-1 | Planned Year/Phase 1 Instructional Formats Source: School-reported
Using the academic year when the charter class will be in the first year of the curriculum, list each first-year course and provide the total number of instructional hours for each listed instructional format. Note that “small group” includes case-based or problem-solving sessions. Provide the total number of hours per course and instructional format. Provide a definition of “other” if selected. Add rows as needed.
Number of Formal Instructional Hours Per Course
Course Lecture* (see column labeled Other) Lab Small Group Patient Contact Other (Describe) Faculty-led guided discussions, case-based,
interactive, large group Total
Introduction to Ethics and
Professionalism 8 6 14
Introduction to Public Health 16 12 28
Epidemiology and Biostatistics 32 24 56
Anatomy 65 24 18 107
Histology 40 24 18 82
Cellular and Molecular
Science 80 60 140
Introduction to Pharmacology 8 6 14
Pathobiology 24 18 42
Hematology/Oncology 24 18 42
Microbiology and Infectious
Diseases 48 36 84 Neuro-endocrine control of systems 8 6 14 Cardiovascular system 32 24 56 Pulmonary system 24 18 42 Urinary system 24 18 42
Art and Practice of Medicine 88 38 126
4
Table 6.0-2 | Planned Year/Phase 2 Instructional Formats Source: School-reported
Using the academic year when the charter class will be in the second year of the curriculum, list each second-year and provide the total number of instructional hours for each listed instructional format. Note that “small group” includes case-based or problem-solving sessions. Provide the total number of hours per course and instructional format. Provide a definition of “other” if selected. Add rows as needed.
Number of Formal Instructional Hours Per Course
Course Lecture* (see column labeled Other) Lab Small Group Patient Contact Other (Describe) Faculty-led guided discussions, case-based,
interactive, large group Total
Gastrointestinal system 24 18 42
Endocrine system and
metabolism 24 18 42 Nutrition 16 12 28 Reproductive system 24 18 42 Nervous system 32 24 56 Psych 24 18 42 Musculo-skeletal system 24 18 42
Clinical Immunology and
Rheumatology 24 18 42
Skin 16 12 28
Genetics 24 18 42
Art and Practice of Medicine 88 37 125
Total 0 0 320 37 174 531
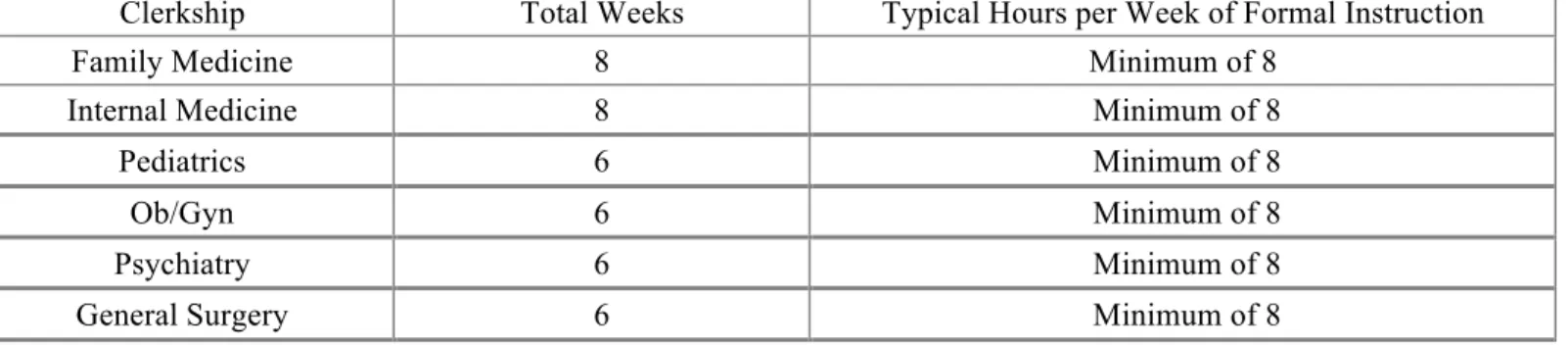
Table 6.0-3 | Planned Year/Phase 3-4 Weeks/Formal Instructional Hours per Clerkship Source: School-reported
Using the academic years when the charter class will be in years three and four of the curriculum, provide the total number of weeks and formal instructional hours (lectures, conferences, and teaching rounds) for each clerkship in years three-four of the curriculum. Provide a range of hours if there will be significant variation across sites. Note that hours devoted to patient care activities should NOT be included. Add rows as needed.
Clerkship Total Weeks Typical Hours per Week of Formal Instruction
Family Medicine 8 Minimum of 8
Internal Medicine 8 Minimum of 8
Pediatrics 6 Minimum of 8
Ob/Gyn 6 Minimum of 8
Psychiatry 6 Minimum of 8
5 STANDARD 6 NARRATIVE RESPONSE
a. If the school plans to offer a parallel curriculum (“track”) to a subset of students, include the
following information in each description, and highlight the difference(s) from the curriculum of the standard medical education program:
1. The location of the parallel curriculum (main campus or geographically distributed campus)
2. The year the parallel curriculum will be first offered
3. The focus of the parallel curriculum, including the additional objectives that students must
master
4. The general curriculum structure (including the sequence of courses/clerkships in each
curriculum year/phase)
5. The number of students who will participate in each year of the curriculum
6
6.1 FORMAT / DISSEMINATION OF MEDICAL EDUCATION PROGRAM OBJECTIVES AND LEARNING OBJECTIVES
The faculty of a medical school define its medical education program objectives in outcome-based terms that allow the assessment of medical students’ progress in developing the competencies that the
profession and the public expect of a physician. The medical school makes these medical education program objectives known to all medical students, faculty, residents, and others with responsibility for medical student education and assessment. In addition, the medical school ensures that the learning objectives for each required learning experience (e.g., course, clerkship) are made known to all medical students and those faculty, residents, and others with teaching and assessment responsibilities in those required experiences.
7 6.1 SUPPORTING DATA
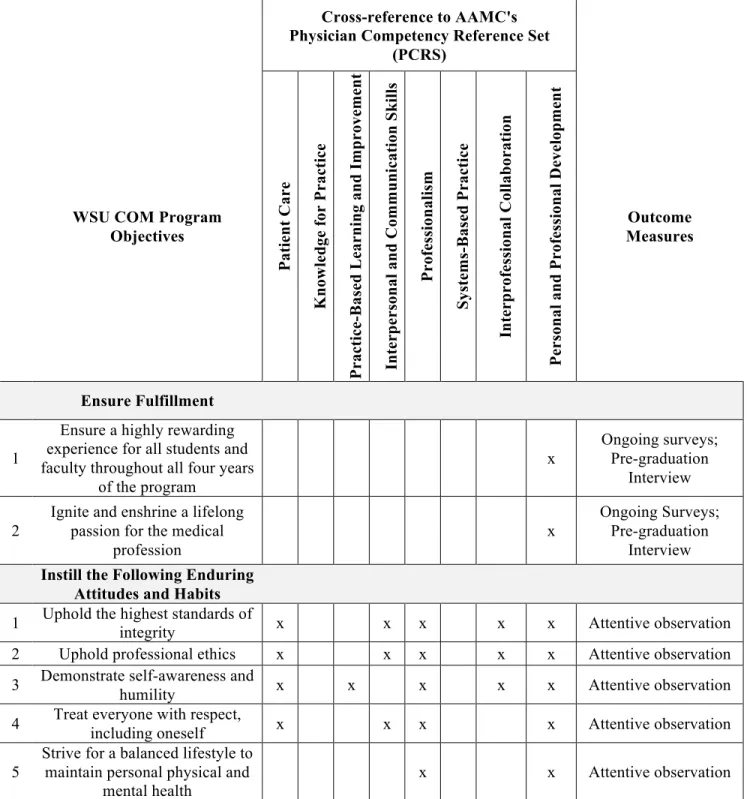
Table 6.1-1 | Competencies, Program Objectives, and Outcome Measures
Source: School-reported As available, for each general competency expected of graduates, provide the related medical education program objectives and the outcome measure(s) that specifically will be used to assess students’ attainment
of each related objective and competency. Add rows as needed.
Cross-reference to AAMC's Physician Competency Reference Set
(PCRS)
WSU COM Program Objectives Pa ti en t C ar e Kn ow le d ge f or P ra ct ic e Pr ac ti ce -Ba se d Le ar n in g an d I m p ro ve m en t In te rp er so n al a n d C om m u n ic at io n S k il ls Pr of es si on al is m Sy st em s-Ba se d P ra ct ic e In te rp ro fe ssi on al C ol la b or at io n Pe rs on al a n d Pr of es si on al D ev el op m en t Outcome Measures Ensure Fulfillment 1
Ensure a highly rewarding experience for all students and faculty throughout all four years
of the program x Ongoing surveys; Pre-graduation Interview 2
Ignite and enshrine a lifelong passion for the medical
profession
x
Ongoing Surveys; Pre-graduation
Interview
Instill the Following Enduring Attitudes and Habits
1 Uphold the highest standards of
integrity x x x x x Attentive observation
2 Uphold professional ethics x x x x x Attentive observation
3 Demonstrate self-awareness and
humility x x x x x Attentive observation
4 Treat everyone with respect, including oneself x x x x Attentive observation
5
Strive for a balanced lifestyle to maintain personal physical and
mental health
8
6 Demonstrate empathy x x x x Attentive observation
7 Demonstrate cultural sensitivity x x x x x Attentive observation
8 Promote healthcare equity x x x Attentive observation
9 Be dependable and diligent x x x x Attentive observation
10 Promote professional teamwork x x x x x x x Attentive observation
11 Demonstrate and expect
accountability x x x x x x x Attentive observation
12 Seek new knowledge and
understanding x x x x Attentive observation
13 Share knowledge and understanding x x x x x x x Attentive observation
14 Strive to identify, prioritize, and solve problems x x x x x Attentive observation
15 Tolerate uncertainty x x x x x Attentive observation
16 Improve quality x x x x x x Attentive observation
17 Increase effectiveness and cost-efficiency x x x x x x Attentive observation
18 Reduce risk x x x x x x x Attentive observation
Impart the Following Knowledge
1
Scientific knowledge: principles of human biology, physiology,
and psychology
x x x Written exams
2
Medical knowledge: etiology and presentation of common diseases; related diagnostics, treatments, and outcomes
x x x Written exams
3
Ethics knowledge: ethical foundations of healthcare
professions
x x x x x x x Written exams
4
Public health knowledge: population-level perspective on
health and disease
x x x x Written exams
5
Legal knowledge: legal foundations of healthcare
professions
x x x x x Written exams
6
Healthcare economics knowledge: healthcare policy,
financing, and business
x x x x x Written exams
7
Operational systems knowledge: how the whole healthcare ecosystem operates
x x x x x Written exams
8
Informational systems knowledge: how medical
information is managed, accessed, and used
x x x x Written exams
9 1
Emergency Response: recognize emergencies, take appropriate actions and seek appropriate help if needed
x x x x Performance on Simulations
2
Communication: communicate effectively with patients,
families, and healthcare professionals
x x x x Attentive observation; OSCE
3
Listening: listen intently to patients, families, and healthcare professionals
x x x x Attentive observation; OSCE
4
Interpretation: interpret communications accurately and
in context x x x x
Attentive observation; OSCE; Written exams 5
Information gathering: acquire pertinent information, from
history, physical exam, diagnostic tests, etc.
x
Attentive Observation;
OSCE
6 Analysis: critically appraise all
pertinent information x OSCE; Written exams
7 reasoning adapted to each case Reasoning: Practice clinical x Attentive observation; OSCE; Written exams
8 Diagnosis: formulate
well-reasoned differential diagnoses x
Attentive observation; OSCE; Written exams 9
Treatment: formulate and proficiently implement the most
effective treatment plan validated by evidence
x Attentive observation; OSCE; Written exams
10 Documentation: Maintain and safeguard meticulous records x x x x x Attentive observation
11 Teamwork: function effectively as interprofessional team member or team leader
x x x x x Attentive observation
12
Reflection: reflect on patient care, self-care and self-directed
learning
x x x x Written narrative
13 Learning: effectively practice
lifelong, self-directed learning x x x x x Written exams
14
Teaching: effectively teach patients, families, students, and
coworkers
10 6.1 NARRATIVE RESPONSE
a. Describe the status of development of the medical education program objectives and their linkage to
the relevant competencies.
The medical education program objectives and their linkages to competencies have been completed by the Curriculum Design Committee and have been reviewed and approved by the ad hoc Curriculum
Committee.
b. Describe how the medical school has identified outcome measures and linked them to the medical
education program objectives. How is the medical school ensuring that the outcome measures selected are sufficiently specific to allow a judgment that, in summary, each of the medical education program objectives have been met?
The objectives of the medical education program are statements of the items of knowledge, skills, behaviors, and attitudes that medical students are expected to exhibit as evidence of their achievement. The educational objectives, along with their associated outcome measures, reflect whether and how well graduates are developing these competencies as a basis for the next stage of their training.
There are several widely recognized definitions of the knowledge, skills, behaviors, and attitudinal attributes appropriate for a physician, including those described in the AAMC's Medical School
Objectives Project, the general competencies of physicians resulting from the collaborative efforts of the Accreditation Council for Graduate Medical Education (ACGME) and the American Board of Medical Specialties (ABMS), and the physician roles summarized in the CanMEDS 2005 report of the Royal College of Physicians and Surgeons of Canada.
To ensure that the outcome measures selected are sufficiently specific to allow a judgment that, in
summary, each of the medical education program objectives have been met, the WSU COM selected from a wide variety of available assessment methods to provide the most accurate evaluation of the
achievement of learners relative to each of the program, course, and session objectives, using the methods described in the MedBiquitous standards set forth by the AAMC. (MedBiquitous Curriculum Inventory
Working Group Standardized Vocabulary Subcommittee. (2012). Curriculum Inventory standardized
instructional and assessment methods and resource types (September 2012 version). Washington, DC: Association of American Medical Colleges.)
c. Describe how medical education program objectives will be disseminated to each of the following
groups:
1. Medical students in the charter class
2. Faculty with responsibility for teaching, supervising, and/or assessing medical students I the first
and second years of the curriculum
Education program objectives will be provided to the medical students in the charter class as part of the student handbook forwarded to them prior to the decision date confirming their intent to matriculate (under the AAMC Traffic Rules). They will also be available on the college website, and will be provided to the students annually at orientations. Program objectives are available in one45, and will be included in all course syllabi.
Faculty will be provided the medical education program objectives through faculty development workshops, in meetings with course/clerkship directors, by the chairs at departmental meetings, through
11
the website, and in email. Program objectives are available in one45, and will be included in all course syllabi.
d. Describe how learning objectives for each required first and second-year course will be disseminated
to each of the following groups:
1. Medical students
2. Faculty with responsibility for teaching, supervising, and/or assessing medical students in the
required course
3. Residents and other non-faculty teachers with responsibility for teaching, supervising, and/or
assessing medical students in the first or second year course
Learning objectives for medical students, faculty, and residents and other non-faculty teachers will be disseminated through the course syllabi, one45, and on the WSU COM web site. Faculty, residents and non-faculty teachers will be made aware of the course objectives through faculty development training, distribution of the syllabi in one45, and posting on the website.
12 6.2 REQUIRED CLINICAL EXPERIENCES
The faculty of a medical school define the types of patients and clinical conditions that medical students are required to encounter, the skills to be performed by medical students, the appropriate clinical settings for these experiences, and the expected levels of medical student responsibility.
6.2 SUPPORTING DATA
Table 6.2-1 | Required Clinical Experiences Source: School-reported
Provide the criteria established to date for the patient types or clinical conditions that medical students are expected to encounter, the required procedures/skills, and clinical settings, along with the corresponding level(s) of student responsibility for each.
Patient Type or
Clinical Condition Procedure/Skill Clinical Setting(s)
Level of Student Responsibility Please see Appendix 6-01 (total of 13 pages) for a full list of required clinical experiences organized by
clerkship. 6.2 NARRATIVE RESPONSE
a. Describe the status of planning, to date, for the list of required patient types/clinical encounters and
procedural skills for each required clinical clerkship or for the clerkship year as a whole.
As part of the curriculum design effort, faculty have identified required patient types/clinical encounters and procedural skills for each required clinical clerkship.
b. Describe how and by which individuals and groups the list of required clinical encounters and skills
was developed. Note if the Curriculum Committee or other central oversight body (e.g., a clerkship directors committee) played or will play a role in reviewing and approving the list of patient types/clinical conditions and skills across courses and clerkships.
The curriculum design working groups tasked with identifying the core clinical encounters and skills generated that detail from guidelines promulgated by national organizations of medical educators within the clerkship fields. The curriculum design working group has reviewed and approved the lists. In the future, clerkship directors will review and propose revisions through the Curriculum Committee governance structure.
c. Describe which individuals and/or groups is developing the list of alternative experiences designed to
remedy gaps when students are unable to access a required encounter or perform a required skill. The faculty working group tasked with identifying the required patient types/core clinical encounters and procedural skills were tasked with identifying alternative experiences to remedy gaps when students are unable to access a required encounter or perform a required skill. These were reviewed by the Curriculum Advisory Team and approved by the ad hoc Curriculum Committee. Future clerkship directors will participate on a subcommittee of the Curriculum Committee, and will be responsible for subsequent revisions; these will be submitted to the Curriculum Committee for approval.
13
d. Describe how medical students, faculty, and residents will be informed of the required clinical
encounters and skills and the corresponding levels of student responsibility.
For faculty, the required clinical encounters and skills and the corresponding levels of student
responsibility will be provided at dedicated workshops to orient the faculty to the curricular elements. For residents, they will be provided by the clerkship directors as part of the “residents as teachers” program, and then will be provided by the clerkship directors to the residents at the start of each rotation. All requirements will be contained in the curriculum mapping program and will be posted on the clerkship website.
For students, the required clinical encounters and skills, along with information on the levels of student responsibility, will be part of the orientation to the clerkships. Their progress in achieving the required encounters of completing the approved alternative will be reviewed regularly by their mentors. The clerkship directors will review student progress at the mid-point of each clerkship, and will be responsible for monitoring completion and/or arranging for an alternative experience. Students will be able to monitor their own progress using a passport system. Students will also have access to the website, as well as to the curriculum mapping software.
14
6.3 SELF-DIRECTED AND LIFE-LONG LEARNING
The faculty of a medical school ensure that the medical curriculum includes self-directed learning experiences and time for independent study to allow medical students to develop the skills of lifelong learning. Self-directed learning involves medical students’ self-assessment of learning needs; independent identification, analysis, and synthesis of relevant information; and appraisal of the credibility of
information sources.
6.3 NARRATIVE RESPONSE
a. Provide examples that illustrate the opportunities that will exist during the first two years (phases) of
the curriculum for students to engage in all of the following components of self-directed learning as a unified sequence (use the names of relevant courses and clerkships from the Overview tables when answering):
1. Identify, analyze, and synthesize information relevant to their learning needs
2. Assess the credibility of information sources
3. Share the information with their peers and supervisors
4. Receive feedback on their information-seeking skills
Example: Case-Based Sessions
All system-based courses in the first phase of the curriculum include case discussions in a small group format integrated into the curricular design. Students will be required to prepare in advance of these sessions. In advance of each system-based course class, students are required to identify, analyze, and synthesize information relevant to their learning needs. Individually and in small groups, students will assess the credibility of information sources. Faculty and librarians are required to formally prepare students in how to use credible information sources. In this example, students may compare the results of their data searches in medical journals and subscription services with open source information.
Through the case discussions in class, students will be expected to participate actively in each of the four elements, sharing the information with their peers and faculty. In illustration, as part of the Endocrinology sessions, students will be required to share information. Students will receive mid-course feedback from their course director and a written narrative evaluation at the end of each course which will address each of the elements.
The entire curriculum is based on active learning principles with students working alone or together in advance of class to master content elements
b. Referring to the sample weekly schedules requested below, describe the amount of unscheduled time
available for medical students to engage in self-directed learning and independent study in the first two years (phases) of the curriculum.
The Curriculum Committee has determined that on average, the medical students will not have more than 28 hours per week of scheduled class time. This will ensure that the students have unscheduled time available for self-directed learning and independent study. There will be optional sessions to help students with content and concepts, as needed and desired.
15
c. Note if medical students in the first two years/phases of the curriculum will have required activities
outside of regularly-scheduled class time, such as assigned reading or online modules that include information to prepare them for in-class activities. Describe how this “out-of-class” time will be accounted for in calculating student academic workload.
Faculty will prepare learning modules, delivered on-line, that will prepare students for case discussions and in-class activities. Individual course directors are expected to use the curriculum mapping software to understand the totality of assignments during any given week, and are expected to communicate regarding expectations. The modules consist of a combination of podcasts and guided readings, and may include problems and formative assessments. These leaning modules are mapped to the learning objectives of the courses and also to case-presentations. The number of modules required for each case will be carefully managed and will be the primary determinant of the time out of class required for each week. The Evaluation and Assessment Subcommittee of the Curriculum Committee will track the types and volume of the assignments expected during “out-of-class” time, and will compare this data to the comments provided by the students during the mandatory end of course evaluation. At set times during the year, the Subcommittee will present their findings and recommendations to the Curriculum Committee and the chief academic officer. Periodically, students and faculty will be surveyed regarding this component of the medical education program.
SUPPORTING DOCUMENTATION REQUIRED FOR ELEMENT 6.3
1. Sample weekly schedules that illustrate the amount of time in the first and second (phases) years of
the curriculum that medical students will spend in scheduled activities.
Art and Practice of Medicine Sample Weekly Schedule
Time Mon Tue Wed Thu Fri
8:00 AM
Active learning in class
Patient H&P Patient H&P Patient H&P
Systems course Quiz 9:00 AM Systems course Quiz Review 10:00 AM Active learning in class Active learning in class Active learning in class APM Quiz
11:00 AM APM Quiz Review
12:00 PM Lunch Lunch Lunch Lunch Lunch
1:00 PM
APM Sessions or Clinical Experience
2:00 PM APM Large Group
3:00 PM
APM Skills Lab
16
2. Formal policies or guidelines limiting the amount of scheduled time during a given week during the
pre-clerkship phase of the curriculum.
17
6.4 INPATIENT / OUTPATIENT EXPERIENCES
The faculty of a medical school ensure that the medical curriculum includes clinical experiences in both outpatient and inpatient settings.
6.4 SUPPORTING DATA
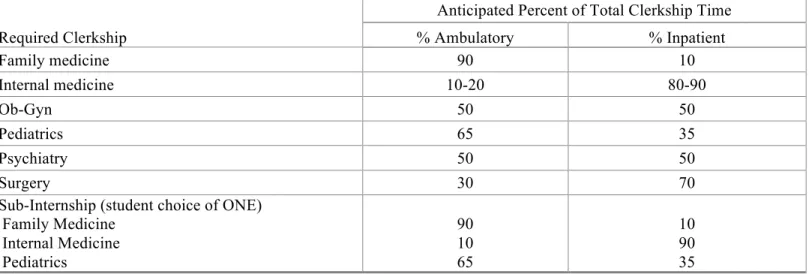
Table 6.4-1 | Percent Total Clerkship Time Source: School-reported
Provide the anticipated percent of time that medical students will spend in inpatient and ambulatory settings in each required clinical clerkship. If clerkship names differ from those in the table, substitute the name used by the medical school. If the amount of time spent in each setting varies across sites, provide a range.
Required Clerkship
Anticipated Percent of Total Clerkship Time
% Ambulatory % Inpatient Family medicine 90 10 Internal medicine 10-20 80-90 Ob-Gyn 50 50 Pediatrics 65 35 Psychiatry 50 50 Surgery 30 70
Sub-Internship (student choice of ONE) Family Medicine Internal Medicine Pediatrics 90 10 65 10 90 35 6.4 NARRATIVE RESPONSE
a. Describe planning to date to ensure that medical students will spend sufficient time in both
ambulatory and inpatient settings to meet the objectives for clinical education.
The Curriculum Design Committee is planning the initial elements of the required clerkships in order to ensure the clinical encounters and skills, as well as the setting (ambulatory and inpatient), are identified in the goals and objectives of the individual clerkship rotations. Central planning is a critical component in order to ensure comparability of experiences across the regional campuses. These experiences will be submitted to the ad hoc Curriculum Committee for formal approval. As the clerkship directors are identified for each of the required campuses, they will also participate as a Subcommittee of the permanent Curriculum Committee.
18 6.5 ELECTIVE OPPORTUNITIES
The faculty of a medical school ensure that the medical curriculum includes elective opportunities that supplement required learning experiences and that permit medical students to gain exposure to and deepen their understanding of medical specialties reflecting their career interests and to pursue their individual academic interests.
6.5 SUPPORTING DATA
Table 6.5-1 | Required Elective Weeks Source: School reported
Indicate the anticipated number of weeks of electives that will be required of all medical students in each year of the planned curriculum.
Year Total Required Elective Weeks
1 0
2 0
3 0
4 16
6.5 NARRATIVE RESPONSE
a. Describe the policies or practices that will require or encourage medical students to use electives to
pursue a broad range of interests in addition to their chosen specialty.
The Curriculum Committee is considering the development of a policy on the number of electives that may be taken in any one specialty. The career counseling program has included the discussion of electives throughout the four year medical education program, and will be particularly emphasized as a topic in the third year as student prepare to participate in the Visiting Students Application System (VSAS). A strong component of career counseling will include group and one-on-one discussions with the students on the importance of gaining exposure to a broad range of specialties. The associate dean for student affairs is responsible for ensuring this type of counseling is included from the first year of the program.
19 6.6 SERVICE-LEARNING
The faculty of a medical school ensure that the medical education program provides sufficient opportunities for, encourages, and supports medical student participation in service-learning and community service activities.
6.6 NARRATIVE RESPONSE
a. Will there be a school requirement that medical students participate in a service-learning experience,
either as part of a regular course or clerkship or as a selective? If so, describe the status of developing these experience(s), including their location in the curriculum.
The medical education program requires an interprofessional service learning experience during the second year of studies. The goals and objectives of the course were developed by the Interprofessional Education Planning Committee, which includes representation from interprofessional faculty from the Colleges of Medicine, Nursing, and Pharmacy.
b. Describe how medical students will be informed about opportunities to participate in voluntary
service-learning and community service activities. How will student participation be encouraged? The associate dean for student affairs provides regular communications with students, beginning at orientation sessions at the start of each academic year. At periodic intervals throughout the school year, the associate dean for student affairs will inform students of upcoming voluntary options at regular meetings with the students, through email, and by posting them on the college’s website. Additionally, WSU provides the whole student body with a list of opportunities in the community (Support
CougSync.pdf).
To date, voluntary service-learning and community service activities have been identified as:
• Charity clinics
• Health fairs (interprofessional)
• Refugee work
• Community organizing
• Presentations to students ranging from elementary school, high school and colleges
• Cougar Care Coach (a mobile interprofessional clinic)
As part of their professional development and their contribution back to the community, all students will be encouraged to participate in the volunteer activities.
c. Describe how the medical school will support service-learning activities through the provision of
funding or staff support.
The COM is committed to supporting service-learning activities through direct and indirect contributions to the program. Faculty will participate as advisors and mentors, while staff will support the program by handling administrative functions. General supplies for the projects will be supported from the operating and foundation dollars at the college level. Additionally, students may apply for funding from the Associated Students of Washington State University Spokane (ASWSUS) for service learning projects.
20 6.7 ACADEMIC ENVIRONMENTS
The faculty of a medical school ensure that medical students have opportunities to learn in academic environments that permit interaction with students enrolled in other health professions, graduate, and professional degree programs and in clinical environments that provide opportunities for interaction with physicians in graduate medical education programs and in continuing medical education programs. 6.7 SUPPORTING DATA
Table 6.7-1 | Master’s and Doctoral Degree Students Taught by Medical School Faculty Source: School-reported
List the number of students currently enrolled in Master’s and doctoral degree programs taught by medical school faculty. Include degree programs in the biomedical or biological sciences where students are taught by medical school faculty. Add rows as needed.
Department or Program No. of Master’s Students No. of Doctoral Students
Speech & Hearing Sciences 52 0
Biomedical Sciences 1 6
Clinical Sciences N/A N/A
Table 6.7-2 | Residents and Fellows Source: School-reported
Provide the total number of residents and clinical fellows on duty in ACGME-accredited programs at clinical sites that will be used for required clinical clerkships where: 1) the medical school is or intends to be the program sponsor and 2) the medical school does not intend to be the program sponsor. Also see the response to element 3.1.
1) No. of fellows/residents in sites where the medical school is or intends to be the program sponsor
2) No. of fellows/residents in sites where the medical school does not intend to be the program sponsor
Fellows: 0 TBD
Residents: 0 124
Table 6.7-3 | Continuing Medical Education Source: School-reported
If the medical school and/or its clinical affiliates are accredited by the ACCME to sponsor continuing medical education for physicians, use the table below, adding rows as needed, to indicate each sponsoring organization’s current accreditation status, the length of accreditation granted, and the year of the next accreditation review.
Program Sponsor Accreditation Status Length of Accreditation Term
Providence Health System Fully Accredited* 4 years
Rockwood Health System Provisionally Accredited* 2 years
* Accredited through Washington State Medical Association (WSMA); WSMA is recognized by the ACCME to sponsor continuing medical education.
21 6.7 NARRATIVE RESPONSE
a. Describe any plans to increase the number of or expand enrollment in graduate programs (Master’s or
Ph.D.) over the next several years. Note if any decreases in graduate programs are anticipated. The college is planning a PhD program in biomedical sciences, with goals to provide opportunities for clinical and translational medical research integrated with faculty at partner clinical sites. The WSU COM is also in the early planning stages to expand the enrollment in its masters’ level program in Speech and Hearing Sciences. No decreases in current graduate programs are planned.
b. Describe plans to expand or reduce graduate medical education programs in sites where medical
students will be completing required clinical clerkships.
WSU COM is working with its clinical affiliates in establishing or expanding GME programs at sites where the medical students will be completing required clinical clerkships. These activities are part of the strategic vision for WSU; increasing the number of residency positions throughout the state in the areas of most need is part of the approach to attracting and retaining physicians in those areas.
c. List the health professions/professional degree programs located at the same campus as the medical
school. WSU
Speech and Hearing Sciences
o BS
o MS
Nutrition and Exercise Physiology
o BS
o MS
Health Policy and Administration
o MHPA Nursing o BSN o RN o MN o DNP o Ph.D. Pharmacy o Pharm. D. Ph.D.
Eastern Washington University Dental Hygiene o BS o MS Occupational Therapy o BS o BA o MOT Physical Therapy o DPT Public Health o MPH University of Washington WWAMI: M.D. program MedEx: PA program RIDE: DDS program
22
d. Provide examples of opportunities that will be available for medical students to interact with students
in other health professions education programs during both required courses/clerkships and voluntary
(e.g., service-learning) activities. Also see the response to element 7.9 and to element 6.6.
During their second year, medical, nursing, and pharmacy students (in cohorts) will participate in a team-based community engagement project to include planning, implementing, and evaluating a collaborative health related community-based project. In addition to providing an opportunity to develop
interprofessional skills, this experience will also include a requirement for the medical students to develop a reflection paper based on their experiences. Faculty members will review the paper, and provide written feedback to the students.
Medical students will have the opportunity to voluntarily interact with all students on service-learning projects as they design their own experiences.
e. Describe how medical students will be exposed to continuing medical education activities for
physicians and note if student participation in any continuing medical education programs will be expected or required.
The clinical affiliates will notify medical students of continuing medical education (CME) events and will offer opportunities for the medical students to participate at each of the distributed campuses.
23 6.8 EDUCATION PROGRAM DURATION
A medical education program includes at least 130 weeks of instruction. 6.8 SUPPORTING DATA
Table 6.8-1 | Number of Scheduled Weeks per Year Source: School-reported
Use the table below to report the planned number of scheduled weeks of instruction in each academic year/phase of the medical curriculum (do not include vacation time). Refer to the overview section if the medical school offers one or more parallel curricula (tracks).
Curriculum Year/Phase Number of Scheduled Weeks
Year/Phase One 43
Year/Phase Two 40
Year/Phase Three 44
Year/Phase Four 43
Total Weeks of Scheduled