2 INTORDUCTION
Nanoparticle drug formulations have many unique properties that differentiate them from small molecule drugs. The pharmacokinetics of nanoparticle agents often vary substantially from their small molecule counterparts. This change in pharmacokinetics occurs because small molecule drugs that are encapsulated into nanoparticles follow the pharmacokinetic behavior of the carrier.1 Nanoparticle agents, such as liposomes and especially PEGylated liposomes, typically have the benefit of prolonged duration of drug exposure as well as increased delivery of the drug to the site of action.2 The clearance mechanisms affecting liposomes are theorized to differ from those of small molecule drugs, which partly explains the prolonged duration of exposure noted with liposomal agents. Conventional liposomes are thought to be cleared mainly by uptake into cells of the mononuclear phagocyte system (MPS). As a result, liposomal agents accumulate in MPS-associated tissues such as the spleen and liver.2 This differs from the typical renal elimination or hepatic metabolism clearance pathways followed by small molecule drugs. The addition of polyethylene glycol (PEG) onto the surface of the liposome to create a PEGylated formulation helps further stabilize the liposome and reduce the rate of clearance by cells of the MPS.1
Liposomal formulations have also been noted to have smaller volumes of distribution than the small molecule drugs they contain. A reduced volume of distribution helps prevent accumulation of the drug into off-target tissues.1 This is especially important with anticancer agents, where off-target distribution of drugs can have cytotoxic effects on healthy tissues. One class of drug that has been used clinically in multiple nanoparticle formulations is anthracyclines, a type of anticancer antibiotic.
Anthracyclines, such as doxorubicin and daunorubicin, exert their anticancer activity through intercalation of DNA base-pairs and subsequent inhibition of DNA topoisomerase II.3 Anthracyclines have been an area of interest for nanoparticle development partly because of serious adverse effects, namely cardiotoxicity, associated with non-specific tissue distribution. Cardiotoxicity can manifest as either acute cardiovascular complications, which tend to resolve with removal of the drug, or chronic cardiotoxicity. Chronic myocardial damage as a result of anthracycline use is typically irreversible and can eventually lead to heart failure and death. Liposomal formulations of doxorubicin have been shown to drastically reduce the incidence of anthracycline-induced cardiotoxicity. This occurs because
liposomal formulations distribute preferentially into tumors as a result of leaky tumor microvasculature, leaving normal heart tissue with intact vasculature relatively safe from accumulating high
concentrations of the drug.3
3
essential feature of the drug development process is selecting an appropriate starting dose for phase 1 clinical trials. Starting doses are derived from the results of pharmacokinetic and toxicological studies in preclinical animal models, such as mice, rats, and dogs.4 One commonly used method for predicting pharmacokinetic behavior in humans is allometric scaling. Allometric scaling, which has historically been used as a way to predict physiological characteristics based on total body weight, can also be used to predict pharmacokinetic parameters based on other physiological variables. One application of
allometric scaling in pharmacokinetics has been to predict drug clearance based on blood flow or weight of the eliminating organ, such as the kidneys or liver. By assessing the relationship between clearance and these physiological variables in multiple different mammalian species, a prediction of human clearance can be made using interspecies scaling.4
As mentioned above, nanoparticle formulations of drugs take on the pharmacokinetic profile of their carriers and thus have different clearance mechanisms than are typical of small molecule drugs.1 The purpose of this study was to evaluate if traditional interspecies allometric scaling can be applied to different types of nanoparticle formulations of small molecule drugs. More specifically, the study aimed to identify which physiological variables, if any, most accurately predict the clearance of these agents in humans. Based on the proposed involvement of the MPS in clearance of nanoparticles, MPS-related physiological variables were assessed in addition to more typical physiological variables, such as body weight and liver blood flow. Anthracyclines were selected as the agents of interest because of the availability of four different formulations: non-liposomal (NL) doxorubicin (NL-doxorubicin;
Adriamycin®), PEGylated liposomal doxorubicin (PLD; Doxil®), non-PEGylated liposomal daunorubicin (DaunoXome®), and polymeric micellar doxorubicin (SP1049C). Based on our prior allometric studies of PEG-liposomal agents alone, it was hypothesized that interspecies scaling using MPS-associated parameters would better predict clearance for all types of nanoparticle formulations while liver-associated factors would produce the most accurate predictions for small molecule doxorubicin.5
MATERIALS AND METHODS
Pharmacokinetic Studies of NL-Doxorubicin
4
tumor-bearing Fischer rats with doxorubicin at 6 mg/kg as a single IV bolus. Blood samples were collected at 4, 24, 48, 72, 96, and 120 hours after administration (n=4 at each time point). Plasma concentrations of doxorubicin were determined using a spectrofluorometer.7 For beagle dogs,
doxorubicin was injected at 0.5 mg/kg as a single IV bolus to the superficial limb vein. Serial blood draws were obtained at 0.083, 0.17, 0.25, 0.5, 0.75, 1, 2, 4, 6, 8, 10, 12, 24, 48, and 72 hours after drug
administration (n=3). Plasma concentrations of doxorubicin were quantified using HPLC.8 Concentration versus time data for patients were extrapolated from a study that administered Adriamycin® to twelve female patients with breast cancer at a dose of 50 mg/m2 as a single IV bolus over 3 minutes. Serial blood draws were taken at 0.17, 0.33, 0.67, 1, 2, 4, 6 or 8, 12 or 16, and 24 hours post-dose. Doxorubicin concentrations in plasma were determined using HPLC.9
Pharmacokinetic Studies of Doxil®
Mice received Doxil® at 6 mg/kg as a single IV bolus via the tail vein, with plasma samples being obtained 0.083, 2, 4, 8, 24, 48, 72, and 96 hours after drug administrations (n=3 at each time point).5 Concentration versus time data for rats were extrapolated from a study that administered Doxil® to rats as a 1 mg/kg IV bolus with blood draws taken at 0.5, 2, 4, 8, 24, 48, and 72 hours after administration (n=6). The same study also administered Doxil® to dogs at 1.5 mg/kg as a 30 minute IV infusion with serial blood sampling occurring at 0.05, 0.5, 1, 2, 4, 8, 12, 24, 36, 48, 72, and 96 hours after the infusion (n=6).5,8,10 Concentration versus time data for patients with various solid tumors came from an open-label phase I study where Doxil® was administered over a dose range of 30 – 60 mg/m2 as a 1 hour IV infusion. Serial blood draws were obtained at 0.33, 1, 3, 5, 7, 28, 48, 72, 96, 336, 505, and 670 hours after the infusion (n=15).5,11 Sum total doxorubicin concentrations were determined using HPLC.5 Pharmacokinetic Studies of DaunoXome®
5
infusion (n=3). Sum total daunorubicin concentrations in plasma were determined using HPLC.
Concentration versus time data in patients with Kaposi’s sarcoma were extrapolated from a study that administered DaunoXome® at a dose of 40 mg/m2 as an IV infusion over 30 – 60 minutes. Serial blood draws were collected at 0.5, 1, 4, 8, 12, 16, 20, 24, and 48 hours after the end of the infusion. Plasma concentrations of daunorubicin were determined using a thin-film fluorescence scanning technique.12 Pharmacokinetic Studies of SP1049C
Pharmacokinetic studies of SP1049C in mice, rats, and dogs were performed in order to
determine sum total concentration of doxorubicin in plasma. All animal studies followed their respective Institutional Animal Care and Use Committee (IACUC) protocols. SP1049C is a polymeric micellar
formulation of doxorubicin; polymeric components were provided by Alexander Kabanov and NL-doxorubicin was from Fresenius Kabi USA, Lake Zurich, IL. Female SCID mice received SP1049C at 5 mg/kg as a single IV bolus via the tail vein. Plasma samples were obtained at 0.083, 1, 6, and 24 hours after injection (n=3 at each time point). SP1049C was administered to female Sprague-Dawley rats at 5 mg/kg infused over 5 minutes, with serial blood draws being taken at 0.083, 0.25, 0.5, 1, 2, 4, 8, 24, and 48 hours after the start of the infusion (n=3). Female beagle dogs received SP1049C at 1 mg/kg as an IV infusion over 10 minutes. Serial blood draws were obtained at 0.17, 0.25, 0.5, 1, 2, 4, 8, 24, and 48 hours after the start of the infusion (n=3). Sum total drug (encapsulated plus released) concentrations in plasma were determined using a previously validated HPLC assay.13 Patients with refractory cancers were administered SP1049C over a dose range of 5 – 90 mg/m2 as an IV infusion at a rate of 2 mL/min. Venous blood draws were taken at 0.083, 0.17, 0.33, 0.67, 1, 2, 4, 8, 24, 48, 72, and 96 hours after the end of infusion. Pharmacokinetic parameters for the 70 mg/m2 dosing group were used to extrapolate concentration versus time data for allometric scaling in this study (n=7). Sum total doxorubicin
concentrations were quantified using reverse-phase HPLC.14 Allometric Scaling
The standard allometric equation historically used body weight to predict physiological variables, such as heart rate, in various different mammals.15 In this study, the standard allometric equation was used to predict clearance based on a number of physiological variables as described below in mice, rats, dogs, and humans. The standard allometric equation is a power function, as shown below, where Y is the pharmacokinetic parameter of interest, a is the allometric coefficient, W is the
physiological variable of interest, and b is the allometric exponent:16
6
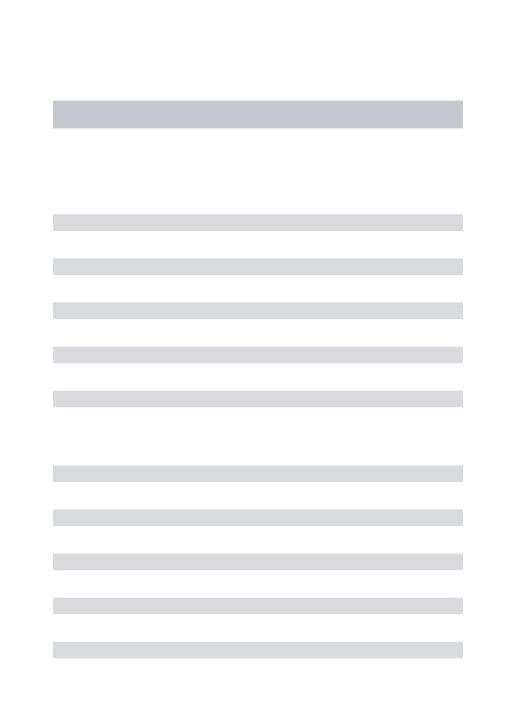
To obtain the values for the allometric coefficient (a) and allometric exponent (b), a log-log plot is generated of the physiological variable of interest on the x-axis and the pharmacokinetic parameter, clearance, on the y-axis. Values for drug clearance in mice, rats, dogs and humans were plotted on log-log coordinates against values for several physiolog-logical variables in these species. Table 1, which was adapted from Caron et al. (2011), contains values for the physiological variables used in this study. Coefficient of determination (R2) values were obtained based on the relationship between clearance and each physiological variable in mice, rats, dogs, and humans. The R2 values were then used to determine which physiological variables would potentially have utility in predicting clearance in humans. Human data were removed from the plots to obtain the allometric equations used in generating “predicted” human clearance values.
Table 1: Values used for physiological variables in mice, rats, dogs, and human5
Physiological Variable Mice Rats Dogs Humans
Body weight (kg) 0.02 0.24 11.6 69.9
Liver weight (kg) 0.00175 0.00549 0.2632 1.6705
Spleen weight (kg) 0.0001 0.0003 0.0216 0.169
Kidney weight (kg) 0.00032 0.001095 0.044 0.286
Liver blood flow (mL/min) 1.8 8.28 247.2 1,346.4
Spleen blood flow (mL/min) 0.09 0.378 20 71.5
Total monocyte count 11,232 191,100 474,000,000 1,200,000,000
MPS function in blood (MFI)17 40 100 340 530
Pharmacokinetic Analysis
Clearance values were calculated through importing mean concentration versus time data into Phoenix® WinNonlin® 6.3 (Certara USA, Princeton, NJ). A non-compartmental analysis was used to calculate clearance for NL-doxorubicin, Doxil®, and DaunoXome in mice, rats, dogs, and humans. Clearance values for SP1049C in mice, rats, and dogs were also obtained through non-compartmental analysis of concentration versus time data. Due to the lack of availability of published concentration versus time data for SP1049C in humans, concentration versus time profiles were simulated using published pharmacokinetic parameters using a three-compartment model in Phoenix® WinNonlin® 6.3. Regression analyses of clearance on physiological variables were performed to obtain R2 values.
RESULTS
7
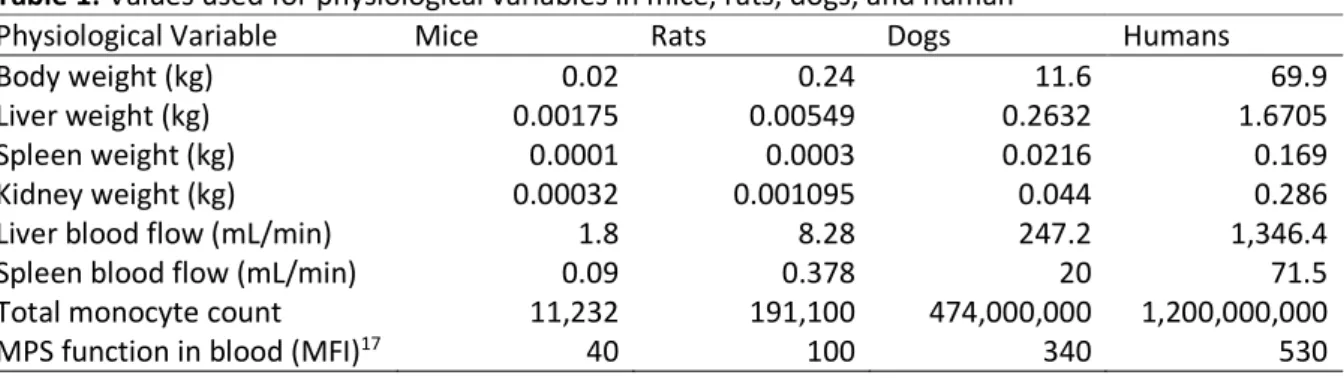
The estimated clearances for each drug in mice, rats, dogs, and humans are summarized in Table 2. Dose-normalized mean concentration versus time data were plotted for NL-doxorubicin, Doxil®,
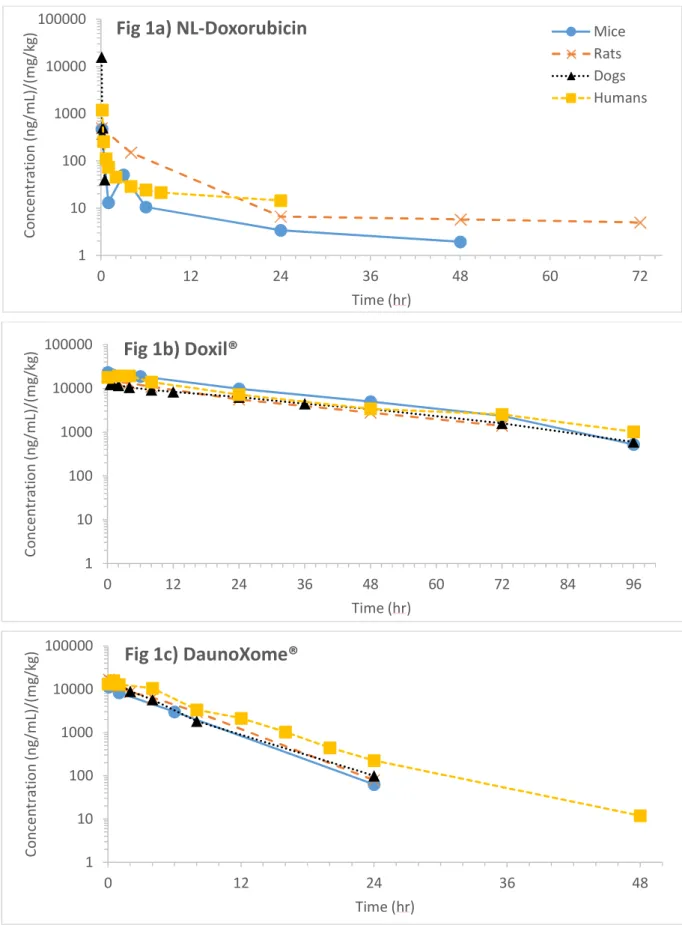
DaunoXome®, and SP1049C in each of the four species studied (Figures 1a – 1d). The two liposomal anthracycline formulations, Doxil® and DaunoXome®, had the lowest clearances across all species. Standard allometric scaling of clearance with each of the physiological variables listed in Table 1 was then performed. A number of physiological parameters traditionally correlated with clearance of small molecule drugs were used to scale clearance, including body weight, liver blood flow, liver weight, and kidney blood flow. Figure 2a illustrates that body weight scaled well with clearance of all four drugs, producing higher R2 values for the liposomal agents, Doxil®(R2=0.997) and DaunoXome®(R2=0.998), than micellar SP1049C (R2=0.923) or NL-doxorubicin (R2=0.874). To assess the hypothesis that MPS-associated variables would be better predictors of nanoparticle clearance than the aforementioned traditional physiological variables, clearance was also scaled with multiple MPS-associated variables, including spleen weight (Figure 2b), spleen blood flow (Figure 2c), total monocyte count (Figure 2d), and MPS function in blood (Figure 2e).
The R2 values from scaling clearance with each of the physiological variables are summarized in Table 3. Overall, scaling clearance of NL-doxorubicin with physiological variables produced the lowest R2 values, in the range of 0.80 to 0.92. The two physiological variables most closely correlated with NL-doxorubicin clearance were spleen weight (R2=0.924) and kidney weight (R2=0.922). Clearance of SP1049C was most closely correlated with spleen blood flow (R2=0.968) and total monocyte count (R2=0.967). Clearances of liposomal agents were more highly correlated with the MPS-associated physiological variables than were clearances of SP1049C or NL-doxorubicin. Doxil® and DaunoXome® were similar with regards to which physiological variables were most closely correlated with clearance. The association between clearance of Doxil® and DaunoXome® with baseline MPS function in blood, liver blood flow, spleen blood flow, and body weight all resulted in R2 values > 0.98.
Table 2: Clearance (mL/hr) of NL-doxorubicin, Doxil®, DaunoXome®, and SP1049C in mice, rats, dogs, and humans
Clearance (mL/hr)
Drug Mice Rats Dogs Humans
NL-doxorubicin 37.649 74.645 869.7 40,720
Doxil® 0.030 0.560 27.37 121.6
DaunoXome® 0.405 3.455 187.6 716.3
8 1 10 100 1000 10000 100000
0 12 24 36 48 60 72
C o n ce n tr a ti o n ( n g /m L) /( m g /k g ) Time (hr)
Fig 1a) NL-Doxorubicin
MiceRats Dogs Humans 1 10 100 1000 10000 100000
0 12 24 36 48 60 72 84 96
C o n ce n tr a ti o n ( n g /m L) /( m g /k g ) Time (hr)
Fig 1b) Doxil®
1 10 100 1000 10000 100000
0 12 24 36 48
C o n ce n tr a ti o n ( n g /m L) /( m g /k g ) Time (hr)
9
Figure 1: Dose-normalized mean plasma concentration versus time profiles for NL-doxorubicin (a),
Doxil® (b), DaunoXome® (c), and SP1049C (d) in mice, rats, dogs, and humans 1 10 100 1000 10000 100000
0 12 24 36 48 60 72 84 96 108
C o n ce n tr a ti o n ( n g /m L) /( m g /k g ) Time (hr)
Fig 1d) SP1049C
0.01 0.1 1 10 100 1000 10000 100000
0.01 0.1 1 10 100
C le a ra n ce ( m L/ h r)
Body Weight (kg)
Fig 2a) Body Weight
10 0.01 0.1 1 10 100 1000 10000 100000
0.0001 0.001 0.01 0.1 1
C le a ra n ce ( m L/ h r)
Spleen Weight (kg)
Fig 2b) Spleen Weight
0.01 0.1 1 10 100 1000 10000 100000
0.01 0.1 1 10 100
C le a ra n ce ( m L/ h r)
Spleen Blood Flow (mL/min)
Fig 2c) Spleen Blood Flow
0.01 0.1 1 10 100 1000 10000 100000
1.00E+04 1.00E+05 1.00E+06 1.00E+07 1.00E+08 1.00E+09 1.00E+10
C le a ra n ce ( m L/ h r)
Total Monocyte Count
11
Figure 2: Standard allometric plots of the relationship between drug plasma clearance and body weight
(a), spleen weight (b), spleen blood flow (c), total monocyte count (d), and baseline MPS function in blood (e) for NL-doxorubicin, Doxil®, DaunoXome®, and SP1049C in (from left to right) mice, rats, dogs, and humans.
Table 3: R2 values obtained by scaling clearance of NL-doxorubicin, Doxil®, DaunoXome®, and SP1049C with physiological variables in mice, rats, dogs, and humans
NL-doxorubicin Doxil® DaunoXome® SP1049C
Body weight (kg) 0.874 0.997 0.998 0.923
Liver weight (kg) 0.920 0.965 0.983 0.964
Spleen weight (kg) 0.924 0.958 0.978 0.966
Kidney weight (kg) 0.922 0.968 0.984 0.958
Liver blood flow (mL/min) 0.908 0.983 0.993 0.947
Spleen blood flow (mL/min) 0.873 0.981 0.995 0.968
Total monocyte count 0.800 0.976 0.989 0.967
MPS function in blood (MFI) 0.832 1.000 0.995 0.907
Prediction of Human Clearance
To generate the allometric equations used for predicting clearance in humans, human data were removed from the allometric plots. The equations of the regression lines obtained from interspecies scaling of clearance in mice, rats, and dogs were then used to predict clearance in patients. These
0.01 0.1 1 10 100 1000 10000 100000
10 100 1000
C
le
a
ra
n
ce
(
m
L/
h
r)
Baseline MPS Function in Blood (MFI)
12
predicted clearances were compared to the observed clearances for each drug in humans obtained from previously published pharmacokinetic studies.9,11,12,14 Table 4 summarizes the coefficients and
exponents of the standard allometric equations obtained by scaling clearance of NL-doxorubicin, Doxil®, DaunoXome®, and SP1049C with each physiological variable in mice, rats, and dogs. Table 5 describes the percent difference between predicted and observed human clearance values for each drug and physiological variable.
Predicting NL-doxorubicin clearance in humans using standard allometric equations was ineffective for all physiological variables tested, including body weight and liver blood flow. The
nanoparticle agents performed similarly with respect to which physiological variables provided the best predictions of clearance in humans. With the exception of spleen weight, the MPS-associated variables generally provided more accurate predictions of clearance in humans than non-MPS-associated
variables. The standard allometric equations incorporating MPS function in blood produced the smallest percent differences from observed values with -22.34%, -16.60%, and -14.05% for Doxil®, DaunoXome®, and SP1049C, respectively. Scaling with spleen blood flow also produced fairly accurate estimates of clearance for the liposomal formulations Doxil® and DaunoXome®.
Table 4: Allometric coefficients (a) and exponents (b) for standard allometric equations scaling clearance with physiological variables in mice, rats, and dogs
NL Doxorubicin Doxil® DaunoXome® SP1049C
a b a b a b a b
Body weight (kg) 219.2 0.5057 2.154 1.0649 16.30 0.9703 1641 0.9386 Liver weight (kg) 2004 0.6284 180.0 1.269 998.7 1.175 118100 1.206 Spleen weight (kg) 8126 0.5813 2899 1.167 13340 1.084 2.0E+6 1.121 Kidney weight (kg) 6402 0.6440 1962 1.308 8984 1.209 1.0E+6 1.231 Liver blood flow
(mL/min)
22.61 0.6521 0.0195 1.344 0.2179 1.235 22.86 1.231 Spleen blood flow
(mL/min)
145.3 0.5891 0.9013 1.201 7.384 1.108 767.7 1.122 Total monocyte
count
2.163 0.2989 0.0002 0.6095 0.0027 0.5624 0.2539 0.5694 MPS function in
blood (MFI)
13
Table 5: Percent difference between predicted and observed clearances of NL-doxorubicin, Doxil®,
DaunoXome®, and SP1049C in humans
NL Doxorubicin Doxil® DaunoXome® SP1049C
Body weight (kg) -95.39% 63.12% 40.21% 49.21%
Liver weight (kg) -93.21% 183.9% 154.8% 270.2%
Spleen weight (kg) -92.90% 199.4% 171.1% 360.2%
Kidney weight (kg) -92.98% 213.8% 176.1% 261.6%
Liver blood flow (mL/min) -93.90% 157.5% 122.7% 174.5%
Spleen blood flow (mL/min) -95.59% 25.01% 16.89% 56.02%
Total monocyte count -97.25% -43.78% -51.87% -36.64%
MPS function in blood (MFI) -96.55% -22.34% -16.60% -14.05%
DISCUSSION
Interspecies allometric scaling has commonly been used to predict clearance in humans and first in-human doses based on preclinical pharmacokinetic studies.4 The use of standard allometric scaling for predicting clearance has been tested extensively in a wide variety of small molecule drugs and, despite some limitations, has been shown to produce fairly accurate results for many drugs.18 However, very few studies have focused on allometric scaling for clearance of nanoparticle agents.5 Nanoparticle formulations of drugs exhibit different pharmacokinetic behavior than their small molecule counterparts. Once encapsulated into a nanoparticle, the small molecule drug adopts the
pharmacokinetic characteristics of the carrier agent.2 With the advent and growth of nanotechnology for drug delivery in cancer and other diseases, it has become increasingly important to assess if traditional methods of allometric scaling can be successfully applied to nanoparticle formulations. We performed a prior allometric study of only PEG-liposomal formulations, including PEG-liposomal doxorubicin (Doxil®), CKD602 (S-CKD602), and cisplatin (SPI-077). Findings from this study suggested that MPS-associated physiological variables may be more closely correlated with clearance of these PEG-liposomal agents than traditional scaling variables.5 The results of this current study show that allometric scaling can be used to successfully predict human clearance of different types of nanoparticle agents, especially when using MPS-associated variables.
14
the rate of clearance.2 DaunoXome®, a liposomal formulation that lacks the incorporation of PEG-lipids, had a slightly more rapid clearance than that of Doxil® in mice, rats, dogs, and humans. SP1049C and NL-doxorubicin had the most rapid clearances across all species. SP1049C is a micellar formulation of doxorubicin currently being investigated for its ability to disrupt Pgp transport and maintain activity in doxorubicin-resistant tumors.19 However, even though SP1049C is a nanoparticle agent its rate of clearance more closely resembled that of NL-doxorubicin than either of the two liposomal formulations.
The R2 values obtained from scaling clearance of each anticancer agent with the physiological variables of interest were used as an initial assessment of which physiological variables were most closely associated with clearance. It was hypothesized that higher R2 values would indicate a closer association, therefore resulting in more accurate predictions of human clearance. General trends could be noted between R2 values and the accuracy of clearance predictions; for example, R2 values were generally lower for NL-doxorubicin than any of the nanoparticle agents. NL-doxorubicin also had the most consistently inaccurate predictions of human clearance, with predicted clearances being
approximately 95% less than the observed clearance in humans. Although it was expected that very high R2 values would be associated with more accurate predictions of human clearance, this did not appear to be the case. For example, the standard allometric plot scaling DaunoXome® clearance with liver blood flow had a high R2 value of 0.993, yet the prediction of human clearance based on liver blood flow for DaunoXome® was inaccurate (122.7% higher than measured clearance). Furthermore, two allometric plots with nearly identical R2 values could generate predictions of clearance in humans with vastly different levels of accuracy. For example, scaling of SP1049C clearance with spleen weight and total monocyte count had R2 values of 0.966 and 0.967, respectively. However, the accuracy of SP1049C clearance predictions was 360.2% high for spleen weight and only 36.64% low for total monocyte count.
One reason for the inconsistency between R2 values and accuracy of clearance predictions could be that the R2 values were generated by incorporating human data into the model, as the goal was to assess the extent to which each physiological variable was associated with clearance across all four species. However, in the allometric equations used for predicting human clearance, the R2 values changed. These data also suggests that the pharmacokinetic disposition and allometric factors associated with clearance across species may not be the same. In future studies, R2 values with and without human data should be compiled, since the values without human data may act as better indicators for how well the allometric equation will predict clearance in humans. There is also evidence suggesting that R2 values may be of limited usefulness in evaluating the accuracy of clearance
15
of all of the physiological variables included, the R2 values produced are fairly high regardless of how well that physiological variable predicts clearance. One study demonstrated that clearance values randomly generated within a wide but plausible range for mice, rats, and dogs produced R2 values > 0.75 in all cases, with the median being R2 = 0.95. These findings led the authors to conclude that, while R2 values may still be useful to report, they should not be used as a statistical measure of the accuracy of allometric predictions.20
Considering the debatable utility of R2 values as an indicator for the strength of allometric relationships, clearance for NL-doxorubicin, Doxil®, DaunoXome®, and SP1049C in humans was predicted based on allometric equations for each physiological variable. It was hypothesized that NL-doxorubicin would be better predicted by traditional clearance variables of other small molecule drugs, such as liver weight and liver blood flow, since these drugs are predominately cleared through
enzymatic reduction in the liver and subsequent biliary excretion.21 However, the results of this study suggest that both traditional and MPS-associated physiological variables consistently underestimate the rate of doxorubicin clearance in humans. One possible reason for the poor prediction of
NL-doxorubicin clearance using standard allometric scaling is that the equation did not include a term to account for protein binding. NL-doxorubicin has fairly high plasma protein binding, with a fraction bound of approximately 0.75.21 Plasma protein binding of drugs has been shown to differ greatly between smaller animals, such as rats, and humans.22 This difference in binding introduces additional variability into the model and could account for the poor accuracy of clearance predictions. An alternative allometric model, which incorporates the ratio of the fraction unbound between rats and humans, has been found to produce more accurate estimates of clearance for a number of highly protein bound small molecule drugs and may be more useful than the standard equation for predicting clearance of NL-doxorubicin.22
16
unable to produce accurate predictions of SP1049C clearance in humans. These findings suggest that the MPS in blood may play a potential role in the clearance of this non-liposomal nanoparticle.
DaunoXome® and Doxil®, both of which are liposomal formulations, had similar results for the use of interspecies allometric scaling to predict clearance in humans. The allometric equation generated from scaling clearance with MPS function in blood produced the smallest percent differences between predicted and observed human clearances at -16.60% and -22.34% for DaunoXome® and Doxil®, respectively. Scaling with spleen blood flow produced human clearance estimates similar in accuracy to those generated from scaling with MPS function in blood. Using total monocyte count as a predictor of clearance did not perform as well, resulting in a percentage difference of 51.87% for DaunoXome® and -43.78% for Doxil®. For these agents, it was hypothesized that scaling with MPS-associated variables would generate the most accurate estimates of clearance in humans, as compared to more traditional variables such as body weight and liver weight. Of the four MPS-associated variables investigated for predicting Doxil® and DaunoXome® clearance, only spleen blood flow and MPS function in blood outperformed more traditional scaling variables such as body weight. These results are consistent with our prior allometric studies of PEGylated liposomal agents.5
It was expected that Doxil® and DaunoXome® clearances would not scale well with total monocyte count, even though the clearance of liposomal agents is thought to occur through uptake into
macrophages and monocytes.2 Consistent with our prior studies reporting no relationship between monocyte number and the pharmacokinetics of nanoparticle agents, these results suggest that perhaps the functionality of the MPS is more predictive of liposomal clearance than the absolute number of cells.17,23 The physiological variable of MPS function in blood, which measures the extent of
phagocytosis, produced the most accurate predictions of human clearance for these two drugs. Total monocyte count, on the other hand, only accounts for the absolute number of cells present and not their level of activity. Thus, physiological variables that measure the intrinsic activity of MPS cells may be more useful for scaling clearance of liposomal agents.
17 CONCLUSION
This study illustrates that interspecies allometric scaling of drug clearance can successfully be applied to nanoparticle formulations of small molecule drugs. Clearances of both PEGylated and non-PEGylated liposomal formulations of anthracyclines were most accurately predicted through scaling with the MPS-associated variables of spleen blood flow and MPS function in blood. Clearance of the non-liposomal nanoparticle used in this study, SP1049C, was also better predicted using MPS-associated variables, namely MPS function in blood and total monocyte count. These findings suggest that the physiological variables selected for standard allometric scaling of clearance should be tailored to the proposed clearance pathways of each drug. For nanoparticles undergoing clearance by the MPS, scaling with MPS-associated variables may produce more accurate results than traditional scaling variables.
18 References
1. Drummond DC, Meyer O, Hong K, Kirpotin DB, Papahadjopoulos D. Optimizing liposomes for delivery of chemotherapeutic agents to solid tumors. Pharmacol Rev. 1999;51(4):691-743.
2. Zamboni WC. Liposomal, nanoparticle, and conjugated formulations of anticancer agents. Clin Cancer Res. 2005;11(23):8230-4.
3. Tahover E, Patil YP, Gabizon AA. Emerging delivery systems to reduce doxorubicin cardiotoxicity and improve therapeutic index: focus on liposomes. Anticancer Drugs. 2015;26(3):241-58.
4. Kang HE, Lee MG. Approaches for predicting human pharmacokinetics using interspecies pharmacokinetic scaling. Arch Pharm Res. 2011;34(11):1779-88.
5. Caron WP, Clewell H, Dedrick R, Ramanathan RK, Davis WL, Yu N, et al. Allometric scaling of pegylated liposomal anticancer drugs. J Pharmacokinet Pharmacodyn. 2011;38(5):653-69.
6. Madden A, Zamboni WC. (2014). [Doxorubicin Plasma Pharmacokinetic Studies]. Unpublished raw data.
7. Siegal T, Horowitz A, Gabizon A. Doxorubicin encapsulated in sterically stabilized liposomes for the treatment of a brain tumor model: biodistribution and therapeutic efficacy. J Neurosurg.
1995;83(6):1029-37.
8. Gabizon AA, Barenholz Y, Bialer M. Prolongation of the circulation time of doxorubicin encapsulated in liposomes containing a polyethylene glycol-derivatized phospholipid: pharmacokinetic studies in rodents and dogs. Pharm Res. 1993 May;10(5):703-8.
9. Robert J, Illiadis A, Hoerni B, Cano JP, Durand M, Lagarde C. Pharmacokinetics of adriamycin in patients with breast cancer: correlation between pharmacokinetic parameters and clinical short-term response. Eur J Cancer Clin Oncol. 1982;18(8):739-45.
10. Working PK, Dayan AD. Pharmacological-toxicological expert report. CAELYX. (Stealth liposomal doxorubicin HCl). Hum Exp Toxicol. 1996;15(9):751-85.
11. Gabizon A, Isacson R, Rosengarten O, Tzemach D, Shmeeda H, Sapir R. An open-label study to evaluate dose and cycle dependence of the pharmacokinetics of pegylated liposomal doxorubicin. Cancer Chemother Pharmacol. 2008;61(4):695-702.
12. Gill PS, Espina BM, Muggia F, Cabriales S, Tulpule A, Esplin JA, et al. Phase I/II clinical and pharmacokinetic evaluation of liposomal daunorubicin. J Clin Oncol. 1995;13(4):996-1003. 13. Zamboni W, Edwards R, Mountz J, Eiseman J, Basse P, Zamboni B, et al. The development of
19
14. Danson S, Ferry D, Alakhov V, Margison J, Kerr D, Jowle D, et al. Phase I dose escalation and pharmacokinetic study of pluronic polymer-bound doxorubicin (SP1049C) in patients with advanced cancer. Br J Cancer. 2004;90(11):2085-91.
15. Boxenbaum H. Interspecies scaling, allometry, physiological time, and the ground plan of pharmacokinetics. J Pharmacokinet Biopharm. 1982;10(2):201-27.
16. Mahmood I, Balian JD. The pharmacokinetic principles behind scaling from preclinical results to phase I protocols. Clin Pharmacokinet. 1999 Jan;36(1):1-11.
17. Caron WP, Lay JC, Fong AM, La-Beck NM, Kumar P, Newman SE, et al. Translational studies of phenotypic probes for the mononuclear phagocyte system and liposomal pharmacology. J Pharmacol Exp Ther. 2013 Dec;347(3):599-606.
18. Mahmood I, Balian JD. Interspecies scaling: predicting clearance of drugs in humans. Three different approaches. Xenobiotica. 1996;26(9):887-95.
19. Valle JW, Armstrong A, Newman C, Alakhov V, Pietrzynski G, Brewer J, et al. A phase 2 study of SP1049C, doxorubicin in P-glycoprotein-targeting pluronics, in patients with advanced adenocarcinoma of the esophagus and gastroesophageal junction. Invest New Drugs. 2011;29(5):1029-37.
20. Tang H, Mayersohn M. Utility of the coefficient of determination (r2) in assessing the accuracy of interspecies allometric predictions: illumination or illusion? Drug Metab Dispos. 2007;35(12):2139-42. 21. Doxorubicin Hydrochloride Injection [package insert]. Bedford, OH: Bedford Laboratories; 2014. 22. Tang H, Mayersohn M. A novel model for prediction of human drug clearance by allometric scaling. Drug Metab Dispos. 2005;33(9):1297-303.
23. Zamboni WC, Maruca LJ, Strychor S, Zamboni BA, Ramalingam S, Edwards RP, et al. Bidirectional pharmacodynamic interaction between pegylated liposomal CKD-602 (S-CKD602) and monocytes in patients with refractory solid tumors. J Liposome Res. 2011;21(2):158-65.
24. Song G, Tarrant TK, White TF, Barrow DA, Santos CM, Timoshchenko, RG, et al. Roles of chemokines CCL2 and CCL5 in the pharmacokinetics of PEGylated liposomal doxorubicin in vivo and in patients with recurrent epithelial ovarian cancer. Nanomedicine. 2015;11(7):1797-807.