Insulin Glargine versus Neutral Protamine
Hagedorn Insulin for Treatment of Diabetes
in Pregnancy
Jennifer G. Smith, M.D., Ph.D.,
1Tracy A. Manuck, M.D.,
1Jenifer White, RD, CDE,
2and David C. Merrill, M.D., Ph.D.
1ABSTRACT
We compared maternal and neonatal outcomes in diabetic pregnancies treated with either insulin glargine or neutral protamine Hagedorn (NPH) insulin. We performed a retrospective chart review of diabetic pregnant patients using the Diabetes Care Center of Wake Forest University during the years 2000 to 2005. Outcomes of interest included maternal hemoglobin A1C, average fasting and 2-hour postprandial blood sugars, mode of delivery, birth weight, 5-minute Apgar score<7, umbilical artery pH<7.20, incidence of neonatal hypoglycemia, and pregnancy complications. A total of 52 diabetic pregnant patients were included in this study. Twenty-seven women used insulin glargine. A total of 13 women used insulin glargine during the first trimester. Glycemic control was similar in women who used NPH insulin and insulin glargine, as determined by hemoglobin A1C levels and mean blood sugar values. There were no differences in mode of delivery, average birth weight, or neonatal outcomes. Maternal and fetal/neonatal outcomes appear similar in pregnant diabetic women who use either NPH insulin or insulin glargine in combination with a short-acting insulin analogue to achieve adequate glycemic control during preg-nancy. Insulin glargine appears to be an effective insulin analogue for use in women whose pregnancies are complicated by diabetes.
KEYWORDS:Insulin glargine, NPH, pregnancy
T
he incidence of diabetes in the United States has steadily risen over the past several decades. As a result, diabetes is one of the most commonly encoun-tered medical complications of pregnancy. It is well known that uncontrolled diabetes in pregnancy can lead to serious fetal, neonatal, and maternal sequelae. Fetal complications can include congenital malforma-tions, intrauterine growth restriction, macrosomia, and intrauterine death. Neonatal complications includehypoglycemia, hyperbilirubinemia, and respiratory dis-tress syndrome. Diabetes during pregnancy has also been shown to increase the risk of development of obesity, diabetes, and metabolic syndrome in offspring.1,2 Maternal complications associated with diabetes in preg-nancy include pregpreg-nancy-induced hypertension, pre-eclampsia, and worsening of chronic complications of diabetes including nephropathy and retinopathy. Therefore, stringent glycemic control during pregnancy
1Department of Obstetrics and Gynecology, Section on Maternal Fetal
Medicine;2Diabetes Care Center of Wake Forest University Medical Center Boulevard, Wake Forest University School of Medicine, Winston Salem, North Carolina.
Address for correspondence and reprint requests: Jennifer G. Smith, M.D., Ph.D., Department of Obstetrics and Gynecology, Section on Maternal Fetal Medicine, Wake Forest University School
of Medicine (e-mail: [email protected]).
Am J Perinatol 2009;26:57–62. Copyright# 2009 by Medical
Publishers, Inc., 333 Seventh Avenue, New York, NY 10001, USA. Tel: +1(212) 584-4662.
Accepted: July 4, 2008. Published online: October 31, 2008. DOI 10.1055/s-0028-1095181. ISSN 0735-1631.
is imperative to ensure a good maternal and fetal out-come.
Recommendations for glycemic control during pregnancy are much stricter than in nonpregnant dia-betic patients: goals are less than 90 to 105 mg/dL fasting and less than 120 mg/dL 2 hours postprandial. A goal of less than 140 mg/dL should be used if assessing blood glucose levels 1 hour postprandial. Various insulin regimens and formulations have been used in an attempt to achieve tight glycemic control during pregnancy, none of which has been shown to be superior.
Insulin glargine is an insulin analogue approved for clinical use in the United States in the year 2000. Due to its chemical structure, insulin glargine is very slowly absorbed, exhibiting a peakless activity profile over a 24-hour time period. Among its attributes, insulin glargine has been shown to reduce the risk of nocturnal hypoglycemia in nonpregnant type I and type II diabetic patients.3–5 Given the strict glycemic control that is recommended during pregnancy, nighttime hypoglyce-mia can be a difficult problem to address in pregnant patients, making insulin glargine an attractive choice for glycemic management in pregnancy.
Reports of insulin glargine use in pregnancy are limited.6–14No adverse effects in human pregnancy have been reported and animal studies have demonstrated the safety of insulin glargine during embryogenesis in animal models.15 This retrospective study provides additional information regarding maternal and fetal/neonatal out-comes in pregnancies in which mothers used either insulin glargine or neutral protamine Hagedorn (NPH) insulin in combination with other short-acting insulin analogues for blood glucose management during their pregnancies.
MATERIALS AND METHODS
After obtaining Institutional Review Board approval, we conducted a retrospective chart review of pregnant women and their infants who were treated at the Diabetes Care Center of Wake Forest University Baptist Medical Center and delivered at Forsyth Memorial Hospital. Women treated with either insulin glargine
or NPH insulin during the years 2000 to 2005 were included. There were no exclusion criteria.
Maternal outcome variables included average blood glucose values, hemoglobin A1C, and mode of delivery. Fetal and neonatal outcomes included birth weight, Apgar score at 5 minutes, umbilical artery blood gas at delivery, blood glucose at delivery, nadir blood glucose level, and need for neonatal intensive care unit (NICU) observation for greater than 4 hours due to hypoglycemia.
Data were analyzed usingttest, one-way analysis of variance, and x2 analysis. p<0.05 was considered significant.
RESULTS
Maternal Outcomes
A total of eight type 1, 26 type II, and eighteen gesta-tional diabetic patients were included in this study. The demographic data and insulin regimens used by these women are presented in Table 1. Type I diabetic patients were significantly younger and had a significantly longer duration of disease than either type II or gestational diabetic women.
Of the women using insulin glargine, two women were using prior to conception and continued its use throughout their entire pregnancy. Eleven women ini-tiated use of insulin glargine during the first trimester, and seven women began using insulin glargine during the second trimester. The average doses of insulin glargine at delivery were 5913.7 IU/d in type I diabetic women, 658.2 IU/d in type II diabetic women, and 39.77.7 IU/d in gestational diabetic women.
Although hemoglobin A1C data was limited (first trimester n¼17; second trimester n¼10; third trimestern¼10), glycemic control was similar between the NPH and insulin glargine–treated women (Fig. 1). There were no significant differences in hemoglobin A1C levels between treatment groups in any trimester (first trimester p¼0.88, second trimester p¼0.38, third trimester p¼0.12). Additionally, there was no
Table 1 Maternal Demographics
Insulin Glargine NPH
Type I
(n¼7)
Type II
(n¼13)
Gestational
(n¼7)
Type I
(n¼1)
Type II
(n¼13)
Gestational
(n¼11)
Age (ySEM) 24.41.5 311.3 35.01.3 22 33.31.1 331.8 Years diabetic (meanSEM) 12.91.9 4.51.4 N/A 11 5.11.1 N/A Nulliparous (%) 57 38 14 100 43 27 Gestational age of initiation of
intermediate or long-acting insulin (wkSEM)
11.63.2 12.31.2 29.91.4 1.0 7.02.0 30.01.1
significant difference between hemoglobin A1C levels within treatment groups over the course of gestation (insulin glarginep¼0.31, NPH insulinp¼0.20).
Adequate blood sugar data were available for analysis for 21 patients who used insulin glargine and 17 patients who used NPH insulin. Fasting blood glucose levels were significantly lower than postprandial blood glucose levels in both treatment groups. There was no significant difference between fasting or postprandial blood glucose levels in women who used either insulin glargine or NPH insulin (Fig. 2).
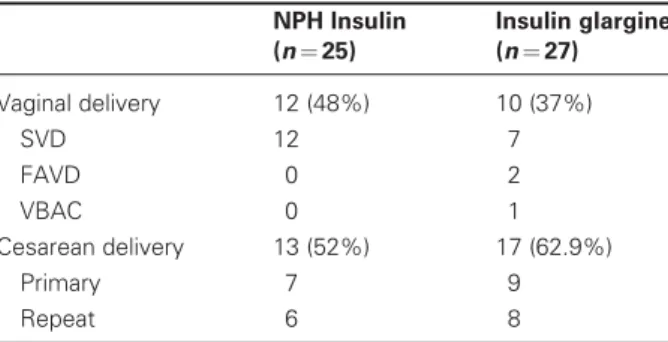
The average gestational age at delivery was 37.00.7 weeks gestation in women treated with NPH insulin and 36.30.96 weeks gestation in women treated with insulin glargine (p¼0.56). Of women using insulin glargine, 37% delivered vaginally compared with 48% using NPH insulin (Table 2). Nine women (33.3%) using insulin glargine and seven women (28%) using NPH insulin were delivered by primary cesarean section. Indications for primary cesarean section included macro-somia (n¼1), failure to progress (n¼6), non-reassuring fetal heart tones (n¼3), failed induction (n¼1), failed forceps (n¼1), and breech presentation (n¼3). There
was no significant difference regarding mode of delivery between the women who used NPH insulin versus insulin glargine (p¼0.6).
Pregnancy complications in the women using insulin glargine included preeclampsia (n¼2), preterm premature rupture of membranes (PPROM;n¼1), and intrauterine fetal demise (n¼1). The intrauterine fetal demise occurred at 204/7 weeks gestation in a patient
with a history of venous sinus thrombosis who was being treated with heparin and baby aspirin. Pregnancy com-plications in the women using NPH insulin were similar and included preeclampsia (n¼5) and PPROM (n¼2).
Neonatal Outcomes
Average birth weights were not significantly different between patients treated with insulin glargine and those treated with NPH insulin (3294189 g and 3274 137 g, respectively;p¼0.93). Additionally, there were no significant differences in the distribution of birth weights between the NPH insulin and insulin glargine groups (Table 3). There was only one 5-minute Apgar score<7. Although data were limited (insulin glargine n¼10, Figure 1 Hemoglobin A1C values by trimester in women who used insulin glargine and neutral protamine Hagedorn (NPH)
insulin. Data are expressed as meanstandard error of the mean.
Figure 2 Fasting and postprandial blood glucose values in women who used insulin glargine and neutral protamine Hagedorn
(NPH) insulin. Data are expressed as meanstandard error of the mean. *p<0.05 compared with postprandial blood glucose
NPH insulinn¼2), there was no significant difference between umbilical artery cord gas values (p¼0.55).
Neonatal blood sugars on admission to the NICU were 66.33.2 mg/dL in infants of women treated with NPH insulin (n¼20) and 58.93.8 mg/dL in infants of women treated with insulin glargine (n¼23;p¼0.16). Nadir neonatal blood sugars were not significantly differ-ent between groups (50.32.8 mg/dL insulin glargine versus 51.42.9 mg/dL NPH insulin, p¼0.79; see Table 3). Thirteen neonates were observed in the NICU for more than 4 hours after delivery, six from the NPH-treated group and seven from the glargine-treated group. Of these infants, three were observed for only 5 hours. None of the remaining infants were observed for blood glucose management alone.
Maternal and neonatal outcomes were also deter-mined for the subgroup of patients for whom adequate blood sugar data were available, and there were no significant differences from the data presented above.
DISCUSSION
A pregnancy category class C drug, insulin glargine is an insulin analogue that was approved for clinical use in 2000. Compared with NPH insulin, insulin glargine use in nonpregnant diabetic patients is associated with lower fasting plasma glucose levels, lower hemoglobin A1C
levels, and greater patient satisfaction.5,16 Although insulin glargine appears superior to NPH insulin in nonpregnant patients, use of this insulin analogue during pregnancy has been limited.6–14 These reports have suggested that insulin glargine use during pregnancy is effective in achieving adequate glycemic control. Although randomized, controlled trials have not been completed, there have been no adverse pregnancy out-comes reported to suggest than insulin glargine use during pregnancy is not safe.
This retrospective review comparing maternal and neonatal outcomes in pregnant women who used either insulin glargine or NPH insulin as the long-acting insulin analogue in their insulin regimen adds additional information to the growing literature regarding insulin glargine use in pregnancy. Although limited in numbers, prior animal and human studies have failed to demon-strate any adverse effects of insulin glargine use during the first trimester of pregnancy.6,8–10,15 In this retro-spective review, we report maternal and neonatal out-comes of an additional 13 women who were exposed to insulin glargine during the first trimester of pregnancy. Our study lacks sufficient power to definitively report that insulin glargine does notcauseany adverse outcomes when used during pregnancy. However, we did not demonstrate any significant differences in either mater-nal or fetal/neonatal outcomes between women who were exposed to either insulin glargine or NPH insulin during their pregnancy. There were no congenital anomalies observed in the women who were exposed to insulin glargine during the first trimester.
Interestingly, almost half of the gestational dia-betics described in this study were able to use a single daily injection of insulin glargine alone to control their diabetes. Therefore, a once-daily dosing regimen using insulin glargine may be appropriate for a large percent-age of patients with gestational diabetes. This simplified insulin administration regimen may improve patient compliance and therefore decrease the incidence of complications associated with uncontrolled or poorly
Table 3 Neonatal Outcomes
NPH (n¼25) Insulin glargine (n¼27)
Gestational age at delivery (wkSEM) 37.00.7 36.31.0 Birth weight (g)
<2500 4 2
2500–4000 18 16
4000–4500 3 5
>4500 0 1
5-min Apgar score<7 0 1 Uterine artery pH<7.20 3 (n¼10) 0 (n¼3) Infants staying in NICU for>4 h (n) 6 7 Neonatal blood sugar on admission (mg/dL) 66.33.2 58.93.8 Nadir neonatal blood sugar (mg/dL) 51.42.9 50.32.8
NPH, neutral protamine Hagedorn; SEM, standard error of the mean; NICU, neonatal intensive care unit. Table 2 Mode of Delivery
NPH Insulin
(n¼25)
Insulin glargine
(n¼27)
Vaginal delivery 12 (48%) 10 (37%) SVD 12 7 FAVD 0 2 VBAC 0 1 Cesarean delivery 13 (52%) 17 (62.9%)
Primary 7 9 Repeat 6 8
controlled gestational diabetes during the third trimester of pregnancy.
Based on existing literature, two major concerns exist regarding insulin glargine use during pregnancy. The first is the concern that insulin glargine may exhibit mitogenic properties. This concern is based on in vitro receptor binding studies that demonstrated that insulin glargine exhibited an increased binding affinity for the insulin-like growth factor (IGF)-1 receptor compared with human insulin.17 In addition, initial in vitro studies also demonstrated that insulin glargine exhibited an eightfold increased potency for stimulating DNA synthesis in human osteosarcoma cells.17Further studies in human diabetic muscle and several cell lines overexpressing the IGF-1 receptor have failed to demonstrate an increase in the mitogenicity of insulin glargine.18–20 In addition, in vivo studies in rats and mice receiving between 2 and 12.5 IU/kg of insulin glargine failed to show an increase in tumor formation after prolonged exposure.21 Perhaps most importantly, despite widespread use in the adult diabetic population, there have been no reports of adverse effects in non-pregnant humans.
Given the increased affinity for the IGF-1 recep-tor, another concern regarding insulin glargine use during pregnancy is the reported association between elevated serum IGF-1 levels and progression of diabetic retinopathy in pregnant patients.22 However, a recent study by Loukovaara et al23 failed to confirm these findings. In fact, they reported that there was no corre-lation between progression of diabetic retinopathy and systemic levels of IGF-1 and IGF binding proteins. Similar concerns regarding progression of retinopathy were raised after the introduction of insulin lispro use during pregnancy.24 Although an adequately powered prospective randomized controlled study has not been performed to definitively address this concern, subse-quent reports have failed to demonstrate an increased risk of retinopathy with insulin lispro use in preg-nancy.25–27The incidence or progression of retinopathy was not specifically addressed in this retrospective review. Prospective, randomized controlled trials are necessary to further address the incidence and progres-sion of diabetic retinopathy as well as incidence of macrosomia in association with various insulin analogues during pregnancy. To achieve adequate power, these studies will need between 100 to 300 patients per treatment arm.25
Although this study presents important infor-mation regarding insulin glargine use during preg-nancy, it is limited by its retrospective nature. Blood sugar records and hemoglobin A1C data were limited. Unfortunately, blood sugar records were too limited to comment on the incidence of nighttime hypoglycemia in patients treated with insulin glargine versus NPH insulin. As this is one benefit of insulin glargine in
nonpregnant patients, future studies need to be per-formed to investigate whether insulin glargine use also decreases the frequency of nighttime hypoglycemia in pregnant patients as this can be an especially difficult problem during pregnancy given the stringent recom-mendations for glycemic control. Devlin et al have published a case report detailing the use of insulin glargine specifically for a patient who had been plagued by nighttime hypoglycemia with excellent blood glucose control and resolution of hypoglycemia.11
From this study, one can conclude that the level of glycemic control achieved during pregnancy with insulin glargine is comparable to that achieved with NPH insulin. In addition, maternal and fetal/neonatal out-comes appear to be similar whether a pregnant diabetic patient uses NPH insulin or insulin glargine as the long-acting insulin analogue in their regimen. A single daily dose of insulin glargine may be effective for management of gestational diabetes. Large prospective, randomized studies are needed to confirm the safety and efficacy of insulin glargine during pregnancies complicated by both pregestational and gestational diabetes.
REFERENCES
1. Boney CM, Verma A, Tucker R, Vohr BR. Metabolic syndrome in childhood: association with birth weight, maternal obesity, and gestational diabetes mellitus. Pediatrics 2005;115:e290–e296
2. Silverman BL, Rizzo TA, Cho NH, Metzger BE. Long-term effects of intrauterine environment. The Northwestern University Diabetes in Pregnancy Center. Diabetes Care 1998;21:B142–B149
3. Rosenstock J, Dailey G, Massi-Benedetti M, Fritsche A, Lin Z, Salzman A. Reduced hypoglycemia risk with insulin glargine: a meta-analysis comparing insulin glargine with human NPH insulin in type 2 diabetes. Diabetes Care 2005; 28:950–955
4. Wang XL, Lu JM, Pan CY, et al. Evaluation of the superiority of insulin glargine as basal insulin replacement by continuing glucose monitoring system. Diabetes Res Clin Pract 2007;76:30–36
5. Manini R, Forlani G, Moscatiello S, Zannoni C, Marzocchi R, Marchesini G. Insulin glargine improves glycemic control and health-related quality of life in type 1 diabetes. Nutr Metab Cardiovasc Dis 2007;17:493–498
6. Dolci M, Mori M, Baccetti F. Use of glargine insulin before and during pregnancy in a woman with type I diabetes and Addison’s disease. Diabetes Care 2005;28:2084–2085 7. Graves DE, White JC, Kirk JK. The use of insulin glargine
with gestational diabetes mellitus. Diabetes Care 2006;29: 471–472
8. Woolderink JM, van Loon AJ, Storms F, de Heide L, Hoogenberg K. Use of insulin glargine during pregnancy in seven type I diabetic women. Diabetes Care 2005;28:2594– 2595
10. Holstein A, Plasche A, Egberts EH. Use of insulin glargine during embryogenesis in a pregnant woman with type I diabetes. Diabet Med 2003;20:779–780
11. Devlin JT, Hothersall L, Wilkis JL. Use of insulin glargine during pregnancy in a type I diabetic woman. Diabetes Care 2002;25:1095–1096
12. Torlone E, Gennarinia A, Ricci NB, Bolli GB. Successful use of insulin glargine during entire pregnancy until delivery in six Type 1 diabetic women. Eur J Obstet Gynecol Reprod Biol 2007;132:238–239
13. Price N, Bartlett C, Gillmer MD. Use of insulin glargine during pregnancy: a case-control pilot study. BJOG 2007;114: 453–457
14. Gallen IW, Roland JM, Chirayath HH. Survey of glargine use in 115 pregnant women with type I diabetes. Diabet Med 2008;25:165–169
15. Hofmann T, Horstmann G, Stammberger I. Evaluation of the reproductive toxicity and embryotoxicity of insulin glargine (LANTUS) in rats and rabbits. Int J Toxicol 2002; 21:181–189
16. Chatterjee S, Jarvis-Kay J, Rengarajan T, Lawrence IG, McNally PG, Davies MJ. Glargine versus NPH insulin: efficacy in comparison with insulin aspart in a basal bolus regimen in type 1 diabetes—the glargine and aspart study (GLASS) a randomised cross-over study. Diabetes Res Clin Pract 2007;77:215–222
17. Kurtzhals P, Schaffer L, Sorenson A, et al. Correlations of receptor binding and metabolic and mitogenic potencies of insulin analogues designed for clinical use. Diabetes 2000;49: 999–1005
18. Ciaraldi TP, Carter L, Seipke G, Mudaliar S, Henry RR. Effects of the long-acting insulin analog insulin glargine on cultured human skeletal muscles: comparisons to insulin and IGF-I. J Clin Endocrinol Metab 2001;86:5838–5847
19. Berti L, Kellerer M, Bossenmaier B, Seffer E, Seipke G, Haring HU. The long acting human insulin analog HOE 901: characteristics of insulin signalling in comparison to Asp (B10) and regular insulin. Horm Metab Res 1998; 30:123–129
20. Ba¨hr M, Kolter T, Seipke G, Eckel J. Growth promoting and metabolic activity of the human insulin analogue [GlyA21, ArgB31, ArgB32]insulin (HOE 901) in muscle cells. Eur J Pharmacol 1997;320:259–265
21. Stammberger I, Bube A, Durchfeld-Meyer B, Donaubauer H, Troschau G. Evaluation of the carcinogenic potential of insulin glargine (LANTUS) in rats and mice. Int J Toxicol 2002;21:171–179
22. Lauszus FF, Klebe JG, Bek T, Flyvbjerg A. Increased serum IGF-1 during pregnancy is associated with progression of diabetic retinopathy. Diabetes 2003;52:852–856
23. Loukovarra S, Immonen I, Teramo KA, Kaaja R. Pro-gression of retinopathy during pregnancy in type 1 diabetic women treated with insulin lispro. Diabetes Care 2003;26: 1193–1198
24. Kitzmiller JL, Main E, Ward B, et al. Insulin lispro and the development of proliferative diabetic retinopathy during pregnancy. (Letter) Diabetes Care 1999;22:874–876 25. Buchbinder A, Miodovnik M, McElvy S, et al. Is insulin
lispro associated with the development or progression of diabetic retinopathy during pregnancy? Am J Obstet Gynecol 2000;183:1162–1165
26. Garg SK, Frias JP, Anil S, et al. Insulin lispro therapy in pregnancies complicated by type I diabetes: glycemic control and maternal and fetal outcomes. Endocr Pract 2003;9:187– 193