Molecular Profiling of Appendiceal Epithelial Tumors
Using Massively Parallel Sequencing to Identify
Somatic Mutations
Xiaoying Liu,1Kabir Mody,2Francine B. de Abreu,1J. Marc Pipas,2Jason D. Peterson,1Torrey L. Gallagher,1
Arief A. Suriawinata,1Gregory H. Ripple,2Kathryn C. Hourdequin,2Kerrington D. Smith,3
Richard J. Barth, Jr.,3Thomas A. Colacchio,3Michael J. Tsapakos,4Bassem I. Zaki,5Timothy B. Gardner,6
Stuart R. Gordon,6Christopher I. Amos,7Wendy A. Wells,1and Gregory J. Tsongalis1*
BACKGROUND: Some epithelial neoplasms of the
appen-dix, including low-grade appendiceal mucinous neo-plasm and adenocarcinoma, can result in pseu-domyxoma peritonei (PMP). Little is known about the mutational spectra of these tumor types and whether mutations may be of clinical significance with respect to therapeutic selection. In this study, we identified so-matic mutations using the Ion Torrent AmpliSeq Can-cer Hotspot Panel v2.
METHODS: Specimens consisted of 3 nonneoplastic
reten-tion cysts/mucocele, 15 low-grade mucinous neoplasms (LAMNs), 8 low-grade/well-differentiated mucinous ad-enocarcinomas with pseudomyxoma peritonei, and 12 adenocarcinomas with/without goblet cell/signet ring cell features. Barcoded libraries were prepared from up to 10 ng of extracted DNA and multiplexed on single 318 chips for sequencing. Data analysis was performed using Golden Helix SVS. Variants that remained after the anal-ysis pipeline were individually interrogated using the In-tegrative Genomics Viewer.
RESULTS: A single Janus kinase 3 (JAK3) mutation was
detected in the mucocele group. Eight mutations were identified in the V-Ki-ras2 Kirsten rat sarcoma viral on-cogene homolog (KRAS) and GNAS complex locus (GNAS) genes among LAMN samples. Additional gene mutations were identified in theAKT1(v-akt murine thy-moma viral oncogene homolog 1),APC(adenomatous polyposis coli), JAK3, MET (met proto-oncogene), phosphatidylinositol-4,5-bisphosphate 3-kinase (PIK3CA), RB1(retinoblastoma 1),STK11(serine/threonine ki-nase 11), and tumor protein p53 (TP53) genes. Among the PMPs, 6 mutations were detected in theKRASgene and also in theGNAS,TP53, andRB1genes.
Appen-diceal cancers showed mutations in the APC, ATM (ataxia telangiectasia mutated),KRAS,IDH1 [isocit-rate dehydrogenase 1 (NADP⫹)], NRAS [neuro-blastoma RAS viral (v-ras) oncogene homolog],
PIK3CA, SMAD4 (SMAD family member 4), and
TP53genes.
CONCLUSIONS: Our results suggest molecular
heteroge-neity among epithelial tumors of the appendix. Next generation sequencing efforts have identified muta-tional spectra in several subtypes of these tumors that may suggest a phenotypic heterogeneity showing mu-tations that are relevant for targeted therapies. © 2014 American Association for Clinical Chemistry
Although cancer of the appendix is rare, representing ⬍1% of gastrointestinal tumors, it affects approxi-mately 2000 individuals annually in the US(1 ). Diag-nostically these tumors can be challenging due to the heterogeneity of the diverse histologic types. Carci-noids historically have been the most common histo-logic type of appendiceal tumors identified, but the dis-tribution of histology has changed with time, with adenocarcinomas representing 64% of appendiceal tu-mors and carcinoids representing 11% in one recent series(2 ). Adenocarcinomas (intestinal, colonic, and signet ring types), lymphomas, and mixed histology, are all examples of additional tumor types known to arise from the appendix.
The most frequent presenting symptoms of these tumors are those mimicking appendicitis, but they may also present with general abdominal pain, as-cites, or peritoneal spread and pseudomyxoma
peri-1Departments of Pathology,2Medicine–Section of Hematology/Oncology,3
Sur-gery,4Radiology,5Radiation Oncology,6Medicine—Section of
Gastroenter-ology and HepatGastroenter-ology,7Center for Genomic Medicine and Department of
Community and Family Medicine, Geisel School of Medicine at Dartmouth, Hanover, NH and Dartmouth Hitchcock Medical Center and Norris Cotton Cancer Center, Lebanon, NH.
* Address correspondence to this author at: Department of Pathology, Dartmouth Hitchcock Medical Center, Lebanon, NH 03756. E-mail gregory.j.tsongalis@ hitchcock.org.
Received April 2, 2014; accepted May 1, 2014.
Previously published online at DOI: 10.1373/clinchem.2014.225565 © 2014 American Association for Clinical Chemistry
Clinical Chemistry60:7 1004–1011 (2014)
tonei (PMP).8Carcinoids may occasionally present with symptoms of carcinoid syndrome (flushing, tachycardia, and diarrhea). In fact, cancers of the appendix are com-monly noted incidentally upon appendectomy.
In some instances, surgery alone is sufficient in the management of these tumors. However, for large car-cinoids, adenocarcinomas, or lymphomas, for exam-ple, more extensive surgery and/or chemotherapy are required. There is currently no standard treatment for these tumors, and which chemotherapy or targeted agent therapy is best used for these tumors remains a subject of debate. At present, adenocarcinomas of the appendix are frequently treated similarly to colon cancer.
Lack of standardized management strategies for these tumors has contributed to high mortality rates. The identification of biomarkers is necessary for the development and selection of more appropriate thera-peutic regimens contributing to more personalized
medicine. In this era of personalized medicine, in which therapeutic strategies can be based on genomic profiling of tumor cells, we sought to identify genomic profiles of various types of appendiceal tumors. In the current study we used massively parallel sequencing techniques to identify somatic mutations in the hot-spots of 50 known human cancer genes to identify mo-lecular profiles which may be clinically actionable with respect to currently available targeted therapies. Materials and Methods
SAMPLES
All samples were obtained from the Department of Pathology archives at the Dartmouth Hitchcock Medical Center (2003–2013). Formalin-fixed, paraffin-embedded (FFPE) specimens consisted of four groups: 3 nonneoplastic retention cysts/mucocele, 15 low-grade appendiceal mucinous neoplasms (LAMNs), 8 low-grade/well-differentiated mucinous adenocarci-nomas with PMP, and 12 adenocarciadenocarci-nomas with goblet cell/signet ring cell features (Fig. 1). The specimen types included FFPE surgical resections and FFPE cy-8Nonstandard abbreviations: PMP, pseudomyxoma peritonei; LAMN, low-grade
appendiceal mucinous neoplasm; FFPE, formalin-fixed, paraffin-embedded; EGFR, epidermal growth factor receptor; CRC, colorectal cancer.
Fig. 1. Histological subtype of appendiceal tumors (hematoxylin and eosin stain).
(A), Nonneoplastic retention cysts/mucocele; (B), LAMNs; (C), low-grade/well-differentiated mucinous adenocarcinoma with PMP; (D), adenocarcinoma with goblet cell/signet ring cell features; (E), appendiceal adenocarcinomas without goblet cell/signet ring cell features. Magnification as follows:⫻100 (A–D) and⫻200 (E).
tology samples (cell blocks) of peritoneal fluid. All tis-sues were deidentified in compliance with the Com-mittee for the Protection of Human Subjects. All samples were independently reviewed by two surgical pathologists who also determined the percentage of tu-mor cell content in each sample.
DNA EXTRACTION
FFPE tissue samples with more than 10% tumor con-tent were macrodissected from 8 unstained tissue sec-tions of 5 microns each. Macrodissection enriched for tumor cell content to⬎50%. Genomic DNA was ex-tracted using the Gentra Puregene kit (Qiagen) accord-ing to the manufacturer’s recommendations. Extracted DNA samples were quantified using the Quant-iTTM PicoGreen® dsDNA assay kit (Invitrogen) before li-brary preparation for sequencing.
AmpliSeq™ CANCER HOTSPOT PANEL v2
Libraries were generated using Life Technology’s Ion AmpliSeq Cancer Hotspot Panel v2 as previously de-scribed(3 ). This panel consists of 207 amplicons cov-ering over 20 000 bases of 50 genes with known cancer associations. Approximately 10 ng of genomic DNA from each sample was used to prepare barcoded librar-ies using IonXpress barcoded adapters (Life Technolo-gies). Libraries were combined to a final concentration of 100 pmol/L using the Ion Library Quantification Kit (Life Technologies), and emulsion PCR was performed using the Ion Torrent OneTouchTM2 System. Samples were sequenced on the Ion Torrent Personal Genome Machine (PGMTM) using Ion 318TMchips.
DATA ANALYSIS
Sequencing reads were first aligned to Human Genome version 19 (hg19) using Torrent Suite 3.4.2. The first step in the data analysis pipeline was to run the Variant Caller Plugin 4.0 provided by Ion Torrent using the high stringency thresholds for somatic variant
detec-tion. Variant annotation and prediction of functional significance was performed with the aid of Golden He-lix’s SVS software version 7.7.8. Remaining variants were assessed using the Broad’s Integrated Genome Viewer (IGV 2.2). Read depth and uniformity of cov-erage across individual amplicons was assessed using the Coverage Analysis Plugin 4.0 provided by Ion Torrent.
Results
HISTOLOGIC DISTRIBUTION OF CASES
Nonneoplastic appendiceal lesions, namely retention cysts/mucoceles, showed a dilated cystic appendix filled with mucinous material. Two out of 3 of the cysts were lined by benign columnar epithelium, while the other was without an epithelial lining, possibly a result of extensive epithelial denudation (Table 1).
All patients with LAMNs also had dilated cystic appendices. Five out of 15 LAMNs showed gross evi-dence of rupture with acellular mucin on the serosal sur-face. Microscopically, the cyst walls were lined by a low-grade adenomatous mucinous epithelium (Table 1).
Low-grade/well-differentiated mucinous adeno-carcinoma with PMP showed appendiceal rupture with mucin extravasation into the abdomen. Six of them revealed cellular mucin, while the other 2 presented with acellular mucin (Table 1).
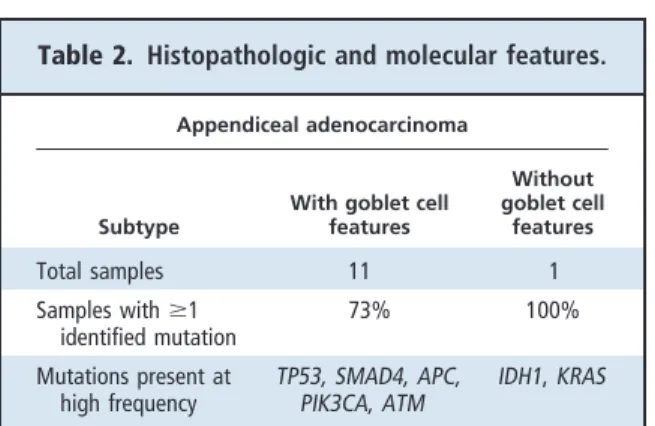
Of the appendiceal adenocarcinomas, 11/12 cases showed features of adenocarcinoma and admixed sin-gle and clusters of goblet- like mucinous cells/signet ring cells. The other case had adenocarcinoma with mucin production and serrated features, moderately differentiated morphology, and no overt goblet cell features (Table 2).
MUTATION PROFILING USING NEXT GENERATION SEQUENCING
A total of 38 samples were sequenced for the AmpliSeq Hotspot Cancer Panel v2 and only 9 did not show any
Table 1. Histopathologic and molecular features.
Benign nondysplastic
(mucocele) LAMNs
Low-grade/well- differentiated mucinous adenocarcinoma with PMP
Total sample number 3 15 8
Histology
Mucin extravasation without rupture 1/3 4/15 0
Mucin extravasation with rupture 0 4/15 8/8
Rupture with PMP 0 0 8/8
Molecular (mutation distribution)
Samples withⱖ1 identified mutation 33% 80% 75%
mutations in the 50 genes tested. Among the 3 muco-cele samples, 2 were wild type and the other had a mu-tation in the Janus kinase 3 (JAK3)9gene (c.2164G⬎A, p.V722I)(Fig. 2A).
Of the 15 LAMNs, 80% (n ⫽12) had at least 1 hotspot mutation identified and 20% (n⫽3) were wild type (Fig. 2B). The most common somatic mutations identified were in the V-Ki-ras2 Kirsten rat sarcoma viral oncogene homolog (KRAS) and GNAS complex locus (GNAS) genes. There were 6 KRAS mutations mapped to codon 12 (c.34G⬎T, p.G12V and c.35G⬎A, p.G12D), 1 to codon 13 (c.38G⬎A, p.G13D), and 1 to codon 61 (c.183A⬎C, p.Q61H). Mutations in the GNAS gene were identified in 8 samples, 2 with c.2531G⬎A, p.R844H and 6 with c.2530C⬎T, p.R844C. Six out of 8 LAMNs contained bothKRAS andGNASmutations. Additional mutations were iden-tified in the v-akt murine thymoma viral oncogene ho-molog 1 (AKT1) (n⫽1), adenomatous polyposis coli (APC) (n ⫽ 5), JAK3 (n ⫽ 1), met proto-oncogene (MET) (n⫽ 2), phosphatidylinositol-4,5-bisphosphate 3-kinase (PIK3CA) (n⫽1), retinoblastoma 1 (RB1) (n⫽ 2), and serine/threonine kinase 11 (STK11) (n⫽1) genes. Samples with mutations in theMETandAKTgenes did not show additional mutations. Three of the 4APC mu-tated cases also had mutations in bothKRASandGNAS genes. Two samples had the same mutations inKRAS, GNAS,RB1, andAPCgenes. These samples had a total of 8 and 5 variants each.
Two out of 8 (25%) low-grade/well-differentiated mucinous adenocarcinoma with PMP samples were wild type and 6/8 (75%) had 2 variants identified (Fig.
2C). All of the mutated samples had a mutation in the KRASgene mapped to codon 12 (c.35G⬎A, p.G12D; c.35G⬎T, p.G12V; c.34G⬎T, p.G12C). In addition, mutations were identified in the tumor protein p53 (TP53) (n⫽2),GNAS(n⫽1), andRB1(n⫽1) genes. Two tumor samples had the same mutations in the KRASandGNASgenes. Two other tumor samples had mutations in theKRASandTP53genes; however, the mutations were not similar. And one sample had a mu-tation in theKRASandRB1genes.
Nine out of 11 adenocarcinoma cases with goblet cell features (82%) had at least 1 hotspot mutation, and 2 (18%) were wild type (Fig. 2D). Five mutations were identified in the TP53 and SMAD family member 4 (SMAD4) genes. Additional mutations identified in this cohort were mapped to the following genes:APC (n⫽3),PIK3CA(n⫽2), ataxia telangiectasia mutated (ATM) (n⫽2), and neuroblastoma RAS viral (v-ras) oncogene homolog (NRAS) (n ⫽1). APCandATM mutations were similar among samples. The 1 adeno-carcinoma case without goblet cell features showed 2 unique mutations in the KRAS (c.37G⬎A, p.G13R) and isocitrate dehydrogenase 1 (NADP⫹) (IDH1) (c.394C⬎A, p.R132S) genes.
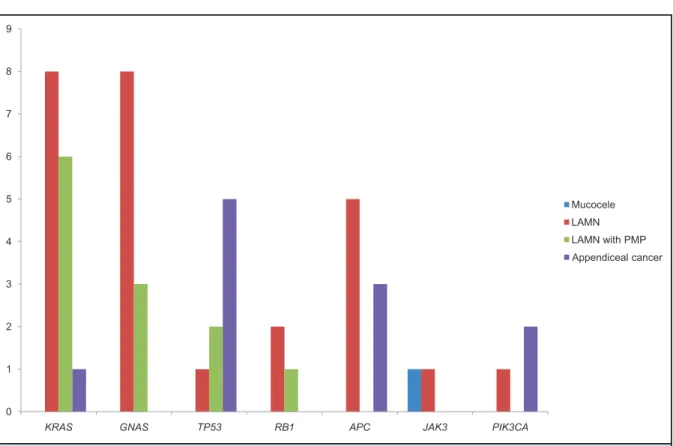
The genomic profiles across the 4 sample types identified mutations within 15 different genes. Com-paratively, only 7 of them (KRAS,GNAS,TP53,RB1, APC,JAK3, andPIK3CA) were mutated in more than 1 group (Fig. 3). Mutations identified in the KRAS,
GNAS, and APC genes were similar among samples
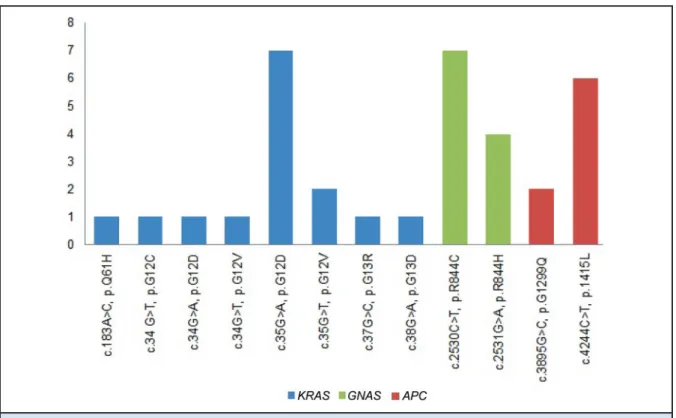
and groups (Fig. 4). WithKRAS, a total of 7 samples (LAMNs and low-grade/well-differentiated mucinous adenocarcinoma with PMP) had a G12D mutation and 2 samples had a G12V mutation. ForGNAS, the most common mutations were R844C and R844H, identi-fied in 7 and 4 samples, respectively. Of the 9 samples with a mutation in theAPCgene, 7 had the P1415L and 2 had the G1299Q mutation.
Discussion
Appendiceal carcinomas are quite rare, with an age-adjusted incidence of 0.12 cases per 1 million people per year. Although most discussions about appendiceal cancers have revolved around carcinoid tumors histor-ically, incidences of the noncarcinoid subtypes have been found to be higher as a whole, with rates per 1 million people per year of 1.3 for mucinous adenocar-cinoma, 0.95 for adenocaradenocar-cinoma, 0.5 for adenocarci-noid (goblet cell), and 0.15 for signet ring cell tumors (4 ). In an analysis of over 2500 cases from 1973 to 2001, it was noted that carcinoid and goblet cell tumors more often presented with localized disease, whereas muci-nous and signet ring cell types presented more fre-quently with larger tumors (⬎2cm) and distant dis-9Human genes:JAK3, Janus kinase 3; KRAS, V-Ki-ras2 Kirsten rat sarcoma viral
oncogene homolog;GNAS, GNAS complex locus; AKT1, v-akt murine thymoma viral oncogene homolog 1;APC, adenomatous polyposis coli; MET, met proto-oncogene;PIK3CA, phosphatidylinositol-4,5-bisphosphate 3-kinase; RB1, reti-noblastoma 1;STK11, serine/threonine kinase 11; TP53, tumor protein p53; SMAD4, SMAD family member 4; ATM, ataxia telangiectasia mutated; IDH1, isocitrate dehydrogenase 1 (NADP⫹);NRAS, neuroblastoma RAS viral (v-ras) oncogene homolog.
Table 2. Histopathologic and molecular features.
Appendiceal adenocarcinoma
Subtype
With goblet cell features Without goblet cell features Total samples 11 1 Samples withⱖ1 identified mutation 73% 100% Mutations present at high frequency TP53, SMAD4, APC, PIK3CA, ATM IDH1, KRAS Molecular Profiling in Tumors of the Appendix
ease. Tumors of the appendix tend to result in increased morbidity and mortality due to late or inci-dental detection. Mortality varies by histologic sub-type, with 5-year survival rates, despite aggressive sur-gical resections, being 83% for carcinoid, 76% for goblet cell, 46% for mucinous, 42% for adenocarci-noma, and 18% for signet ring cell.
Traditional systemic therapies have been extrapo-lated from treatment of colorectal cancer (CRC) and, although data are limited, there have been several re-ports noting benefit with FOLFOX [folinic acid (leuco-vorin), 5-FU (fluorouracil), and oxaliplatin] therapy. Molecular targeting agents, as used and currently un-der investigation in treatment of colorectal adenocar-cinoma, also might be worth evaluating as a treatment option for appendiceal adenocarcinoma, as similar molecular aberrations have been noted in colonic ade-nocarcinoma(5–9 ).
We have previously validated the AmpliSeq Can-cer Hotspot Panel for use in clinical assessment of hu-man cancers, including non–small cell lung cancer, melanoma, glioma, and colon cancer(3 ). In this study, we extended the application of this cancer gene panel to tumors of the appendix, for which there is little molec-ular profiling reported. The goal was to potentially identify clinically actionable mutations with respect to targeted therapy. We found thatKRASandGNAS muta-tions were the most common alteramuta-tions identified in pa-tients with LAMNs and low-grade/well-differentiated mucinous adenocarcinoma with PMP.
KRAS is a protooncogene that encodes proteins involved in cell growth, division, motility, differentia-tion, and apoptosis. Somatic mutations have been linked to the development of several types of cancer, but in CRC, they are detected in 35%– 45% of the pa-tients. The most common mutations result in amino
Fig. 2. Frequency of tissue samples without mutations [wild type (WT)] and frequency of mutant genes identified in each group.
(A), Nonneoplastic retention cysts/mucocele; (B), LAMNs. Genes identified in only one sample represent 15% and were included in “other.” (C), Low-grade/well-differentiated mucinous adenocarcinoma with PMP; (D), appendiceal adenocarcinomas with and without goblet cell/signet ring cell features.
acid substitutions at codons 12 and 13, leading to the activation of the MAPK (mitogen-activated protein ki-nase) pathway. Although these mutations are not prog-nostic, they are well established biomarkers associated with a lack of response to anti– epidermal growth factor receptor (anti-EGFR) monoclonal antibodies, such as cetuximab and panitumumab. According to the US Food and Drug Administration, only patients negative forKRASmutation (or wild type) should receive cetux-imab and panitumumab. Therefore, patients diag-nosed with CRC are screened forKRASmutations. Ac-cording to Patel and Karapetis, the discovery of these mutations as a biomarker allowed for personalized EGFR-targeted therapy for CRC patients(10 ). Among the appendiceal adenocarcinomas with goblet cell fea-tures, this study shows that this group does not have KRASmutations, in agreement with previous findings (11 ).
KRASmutations have been reported previously in appendiceal tumor studies that queried fewer genes. For example, Cuatrecasas and colleagues(12 ) demon-strated that 5 of 6 appendiceal tumors with PMP had a KRASmutation in codon 12. In 2002, Bazan and col-leagues reported that KRAS mutation in codon 12 might be involved in the regulation of mucins (13 ).
Zauber and colleagues demonstrated that 100% of low-grade mucinous tumors had aKRASmutation either in codon 12 or 13, with G12D and G12V being the most common (42% each)(14 ). These authors also studied 42 normal appendices without any neoplasms and all of them were wild type for theKRASgene. Recently, a group of researchers identified 58% of patients with PMP as positive forKRASmutation(15 ). In that study, 89% of the mutations were in codon 12 and 11% in codon 13. In 2013, Nishikawa and colleagues identified GNASmutations as common in LAMNs and suggested that mutantGNASmight play a direct role in mucin production(16 ).
Among the appendiceal adenocarcinoma cases with goblet cell features, we found no samples with KRASmutations. This observation confirms previous findings that these tumors lackKRASmutations(11 ). Our study also demonstrated that this group has mu-tations in theTP53andSMAD4genes. Rammani and colleagues showed that 25% of the appendiceal goblet cell carcinomas had aTP53mutation(17 ). According to Stancu and colleagues, goblet cell carcinoids did not show mutations in SMAD4 (18 ). However, a study with CRC samples performed in 2013 by Fleming and colleagues demonstrated that 9% of sporadic CRCs
0 1 2 3 4 5 6 7 8 9
KRAS GNAS TP53 RB1 APC JAK3 PIK3CA
Mucocele LAMN LAMN with PMP Appendiceal cancer
Fig. 3. Genes mutated in more than 1 sample type (KRAS, GNAS, TP53, RB1, APC, JAK3, and PIK3CA). Number of tumors with mutation (y axis).
had anSMAD4mutation(19 ). The authors demon-strated that one of the mutations identified (c.1082G⬎A, p.R361H) was a pathogenic mutation. None of the appendiceal adenocarcinomas with goblet cell features demonstratedKRASorGNASmutations. This may indicate that a different molecular pathway of carcinogenesis exists in this group of tumors.
GNASis a member of the G-protein family, which modulates signals from transmembrane receptors to the cAMP pathway. Mutations inGNASmay cause the activation of adenylyl cyclase and an increase of cAMP levels. If this pathway is dysregulated, it can increase cell proliferation and contribute to the development and/or progression of cancer. It has also been suggested that a mutated GNASgene is responsible for mucin production in LAMNs.
Conclusion
The next generation sequencing molecular profiling data presented in this study have identified mutation spectra in several subtypes of epithelial tumors of the appendix, suggesting substantial intertumor genomic heterogeneity which may contribute to phenotypic heterogeneity and which warrants further study. These
findings contribute to a better understanding of the molecular pathogenesis of these tumor types, whereas previous studies have focused on single or small num-bers of genes. This is the first study making use of a multigene panel using next generation sequencing technology in appendiceal cancers and may support the off-label use of targeted therapies.
Author Contributions:All authors confirmed they have contributed to the intellectual content of this paper and have met the following 3 re-quirements: (a) significant contributions to the conception and design, acquisition of data, or analysis and interpretation of data; (b) drafting or revising the article for intellectual content; and (c) final approval of the published article.
Authors’ Disclosures or Potential Conflicts of Interest:No authors declared any potential conflicts of interest.
Role of Sponsor:No sponsor was declared.
Acknowledgments:The authors thank the staff of the DHMC Mo-lecular Pathology Laboratory and the Translational Research Pro-gram. The data presented in this manuscript was in part generated through the Department of Pathology Translational Research Shared Resource Laboratory of the Geisel School of Medicine at Dartmouth, the Dartmouth Hitchcock Medical Center and the Norris Cotton Cancer Center.
Fig. 4. KRAS, GNAS, and APC genes shared similar mutations among samples. Number of tumors with mutation (y axis).
References
1.Connor SJ, Hanna GB, Frizelle FA. Retrospective clinicopathologic analysis of appendiceal tumors from 7,970 appendectomies. Dis Colon Rectum 1998;41:75– 80.
2.Turaga KK, Pappas SG, Gamblin T. Importance of histologic subtype in the staging of appendiceal tumors. Ann Surg Oncol 2012;19:1379 – 85. 3.Tsongalis GJ, Peterson JD, de Abreu FB, Tunkey
CD, Gallagher TL, Strausbaugh LD, et al. Routine use of the Ion Torrent AmpliSeqTMCancer
Hot-spot Panel for identification of clinically action-able somatic mutations. Clin Chem Lab Med 2014;52:707–14.
4.McGory ML, Maggard MA, Kang H, O’Connell JB, Ko CY. Malignancies of the appendix: beyond case series reports. Dis Colon Rectum 2005;48: 2264 –71.
5.Kabbani W, Houlihan PS, Luthra R, Hamilton SR, Rashid A. Mucinous and nonmucinous appen-diceal adenocarcinomas: different clinicopatho-logical features but similar genetic alterations. Mod Pathol 2002;15:599 – 605.
6.Tabernero J, Van Cutsem E, Diaz-Rubio E, Cer-vantes A, Humblet Y, Andre T, et al. Phase II trial of cetuximab in combination with fluorouracil, leucovorin, and oxaliplatin in the first-line treat-ment of metastatic colorectal cancer. J Clin Oncol 2007;25:5225–32.
7.Van Cutsem E, Kohne CH, Hitre E, Zaluski J, Chang Chien CR, Makhson A, et al. Cetuximab and
che-motherapy as initial treatment for metastatic colo-rectal cancer. N Engl J Med 2009;360:1408 –17. 8.Hurwitz H, Fehrenbacher L, Novotny W,
Cart-wright T, Hainsworth J, Heim W, et al. Bevaci-zumab plus irinotecan, fluorouracil, and leuco-vorin for metastatic colorectal cancer. N Engl J Med 2004;350:2335– 42.
9.Saltz LB, Clarke S, Diaz-Rubio E, Scheithauer W, Figer A, Wong R, et al. Bevacizumab in combination with oxaliplatin-based chemotherapy as first-line therapy in metastatic colorectal cancer: a random-ized phase III study. J Clin Oncol 2008;26:2013–9. 10.Patel GS, Karapetis CS. Personalized treatment
for advanced colorectal cancer: KRAS and be-yond. Cancer Manag Res 2013;5:387– 400. 11.Dimmler A, Geddert H, Faller G. EGFR, KRAS,
BRAF-mutations and microsatellite instability are absent in goblet cell carcinoids of the appendix. Pathol Res Pract 2014;210:274 – 8.
12.Cuatrecasas M, Matias-Guiu X, Prat J. Synchro-nous muciSynchro-nous tumors of the appendix and the ovary associated with pseudomyxoma peritonei. A clinicopathologic study of six cases with com-parative analysis of c-Ki-ras mutations. Am J Surg Pathol 1996;20:739 – 46.
13.Bazan V, Migliavacca M, Zanna I, Tuiolo C, Grassi N, Latteri MA, et al. Specific codon 13 K-ras mutations are predictive of clinical outcome in colorectal cancer patients, whereas codon 12 K-ras mutations are associated with mucinous
histotype. Ann Oncol 2002;13:1438 – 46. 14.Zauber P, Berman E, Marotta S, Sabbath-Solitare
M, Bishop T. Ki-ras gene mutations are invariably present in low-grade mucinous tumors of the vermiform appendix. Scan J Gastroenterol 2011; 46:869 –74.
15.Shetty S, Thomas P, Ramanan B, Sharma P, Go-vindarajan V, Loggie B. Kras mutations and p53 overexpression in psedomyxoma peritonei: asso-ciation with phenotype and prognosis. J Surg Res 2013;180:97–103.
16.Nishikawa G, Sekine S, Ogawa R, Matsubara A, Mori T, Taniguchi H, et al. Frequent GNAS muta-tions in low-grade appendiceal mucinous neo-plasms. Br J Cancer 2013;108:951– 8. 17.Ramnani DM, Wistuba II, Behrens C, Gazdar AF,
Sobin LH, Albores-Saavedra J. K-ras and p53 mu-tations in the pathogenesis of classical and gob-let cell carcinoids of the appendix. Cancer 1999; 86:14 –21.
18.Stancu M, Tsung-Teh W, Wallace C, Houlihan PS, Hamilton SR, Rashid A. Genetic alterations in goblet cell carcinoids of the vermiform appendix and comparison with gastrointestinal carcinoid tumors. Mod Pathol 2003;16:1189 –98. 19.Fleming NI, Jorissen RN, Mouradov D, Christie
M, Sakthianandeswaren A, Palmieri M, et al. SMAD2, SMAD3 and SMAD4 mutations in colorectal cancer. Cancer Res 2013;73:725– 35.