Suspicion and Persistence: A Case of
Pediatric Brugada Syndrome
Brynn E. Dechert, MSN, CPNP,aMartin J. LaPage, MD, MS,aMitchell I. Cohen, MDb
abstract
This is the case of a 9-year-old girl who initially presents with episodes of syncope and potentially concerning family history. An extensive evaluation is unrevealing, and she appears to have simple benign autonomic dysfunction. Eventually, a rare and life-threatening disease is uncovered, and she receives appropriate treatment. The case report highlights the persistence and suspicion of the managing providers that ultimately allowed the diagnosis to be revealed as well as some of the key features of the underlying disease.
Suspicion is the feeling or thought that something is possible. Persistence is the continuance in a course of action despite difficulty or opposition. Frequently, the art of medicine requires the provider to make conclusions with incomplete information; investigation into the patient’s ailment must be based on experience and suspicion. A diagnosis is not always immediately clear even with comprehensive testing and only reveals itself with persistence and time. In the case to follow, the patient’s ongoing signs and symptoms continued to stack evidence against any serious underlying disease, and it was only the persistence and suspicion of the managing providers that ultimately allowed the diagnosis to be revealed.
CASE REPORT
The patient presented at age 9 to a pediatric electrophysiologist (M.I.C.) after experiencing 4 episodes of syncope, occurring during various daily activities but not during exercise or with fever. Occasionally, these were associated with palpitations or tonic-clonic–type movements and an ashen appearance. Her initial hospital evaluation, including neurology, gastroenterology, and infectious disease
consults and EEG and head computed tomography, was unremarkable.
Her father had been evaluated 7 years before for reported Brugada pattern on electrocardiogram during fever. He had also had several syncopal episodes diagnosed as vasovagal. Evaluation at that time led to a reported
recommendation for an implantable cardioverter defibrillator (ICD), but he declined. The father’s
electrocardiogram result, at the time of the subject patient’s presentation, was normal. He was referred to adult cardiology, which did not suspect a diagnosis of Brugada syndrome. The patient’s 4 siblings were asymptomatic with normal electrocardiogram results.
The patient’s cardiac evaluation included normal echocardiogram and Holter monitor results. Her
electrocardiogram result was normal, including placement of V1 and V2 at a high intercostal space. Procainamide challenge caused some mild changes in the V1 and V2 ST segments but was not diagnostic for Brugada. An implantable loop recorder (ILR) was implanted to clarify any future syncope episodes.
Three months later, the family
relocated, and she established care with another pediatric electrophysiologist (M.J.L.). Aside from electrocardiogram,
aDepartment of Pediatrics, University of Michigan, Ann Arbor, Michigan; andbInova Fairfax Children’s Hospital, Falls Church, Virginia
Ms Dechert and Dr LaPage cared directly for the presented patient, drafted the initial case report, and reviewed and revised the manuscript; Dr Cohen cared directly for this presented patient and critically reviewed and revised the article for intellectual content; and all authors approved the
final manuscript as submitted and agree to be accountable for all aspects of the work.
DOI:https://doi.org/10.1542/peds.2018-3296 Accepted for publication Jan 11, 2019
Address correspondence to Brynn E. Dechert, MSN, CPNP, Division of Pediatric Cardiology, Department of Pediatrics, University of Michigan, 1540 E Hospital Dr, Ann Arbor, MI 48109. E-mail: [email protected] PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2019 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have nofinancial relationships relevant to this article to disclose.
FUNDING:No external funding.
POTENTIAL CONFLICT OF INTEREST:The authors have indicated they have no potential conflicts of interest to disclose.
FIGURE 1
no testing was repeated at that time. Over the following year, she
continued to have frequent, weekly symptoms, including episodes of dizziness, chest pain, and near syncope; hundreds of ILR recordings showed sinus rhythm. At the annual follow-up, the family inquired about removing the ILR. The provider recommended leaving the ILR in place because of the low risk and potential benefit of ongoing monitoring.
Serendipitously, 5 months later (20 months after ILR implant), a sustained wide complex arrhythmia was documented by her ILR (Fig 1) during a febrile illness. At the time of arrhythmia, she was transiently lightheaded but not syncopal. Full evaluation was repeated, including echocardiogram and exercise tests, which had normal results.
Electrocardiogram obtained after the fever resolved did not show
a diagnostic Brugada pattern. Genetic testing was sent. Procainamide
challenge was repeated, resulting in T-wave inversion in V1 and V2 but insufficient ST elevation to qualify as a positive test result. A ventricular stimulation study without
isoproterenol using single and double premature ventricular extrastimuli from the apex resulted in occasional couplets and triplets of ventricular ectopy. A more aggressive approach using S4 premature ventricular extrastimuli induced monomorphic ventricular tachycardia, which progressed abruptly to polymorphic ventricular tachycardia and
ventricular fibrillation necessitating defibrillation. Thesefindings, in light of the previous history, were discussed with the family as well as several colleagues who varied widely in their opinions on whether to implant an ICD. It was decided to implant a subcutaneous implantable cardioverter defibrillator (S-ICD).
Just 2 days before her scheduled S-ICD implantation, the patient became febrile. She was immediately
treated with antipyretics and instructed to present to the clinic to attempt to obtain an
electrocardiogram during fever. The result from afebrile
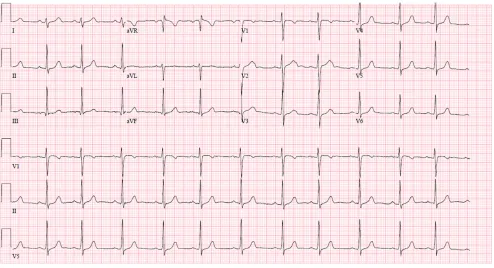
electrocardiogram on arrival was normal (Fig 2). Six hours later, she remanifested a temperature of 39.3ºC while in the clinic. Electrocardiogram then performed with high V1-V2 lead placement was diagnostic of the Brugada sign (Fig 3). She was promptly treated with ibuprofen and admitted for observation.
She underwent successful
implantation of a S-ICD 2 days later. Her genetic test eventually returned with a positive result for a pathologic mutation inSCN5A(c.384011G.A) as well as a variant of unknown significance identified inPKP2 (c.974C.T) also potentially affiliated with Brugada syndrome. The genetic testing facility reported theSCN5A mutation to be likely pathogenic, having been previously reported multiple times in association with FIGURE 2
Brugada syndrome and absent in large population cohorts. Familial cascade screening revealed only 1 genotype-positive sibling who harbored both mutations. TheSCN5A mutation was inherited from the father, and the variation of uncertain significance inPKP2was inherited from the mother.
DISCUSSION
Brugada syndrome is a rare, autosomal-dominant, inherited channelopathy that predisposes patients to ventricular arrhythmias and sudden cardiac death.1,2The hallmark of the disease is a specific pattern of ST segment elevation in the precordial leads (V1–V3). The Brugada pattern may be intermittently present and only revealed during fever, which also increases the likelihood of lethal arrhythmias.3–6It is therefore recommended that patients with known or suspected Brugada syndrome aggressively treat fever
with antipyretic therapy. This case report highlights the impact of fever inducing both ventricular
arrhythmias and the Brugada sign, identifies differing management approaches among pediatric electrophysiologists, and illustrates the role of suspicion and persistence, which may be critical to accurate diagnosis.
The majority of presenting and early evidence in this case did not support the ultimate diagnosis. Brugada syndrome typically presents in adult men, is more often seen in those of Asian descent, and rarely manifests in children. The diagnosis can be difficult because of the inconsistent presence of the Brugada sign on baseline electrocardiogram.3–7The procainamide challenge may not be reliable in pediatric patients, as shown by a large study on asymptomatic children evaluated because of family history in which 23% of patients had a negative drug challenge result before puberty that
eventually became positive after puberty, indicating that Brugada can become unmasked with age.8The difficulty in diagnosis is important to overcome because Brugada is thought to be the cause of sudden cardiac death in 4% to 12% of children and young athletes.9
The patient’s frequent symptoms were repeatedly correlated with benign rhythms, and the suspected diagnosis appeared more unlikely with each passing month. Although there had been initial suspicion of her father having a Brugada pattern during a fever, the diagnosis of Brugada pattern had never been confirmed, and subsequent
evaluations had been unremarkable.
Brugada syndrome in a 10-year-old with documented ventricular arrhythmias would be a class 1 indication for an ICD implantation. In this case, however, a definitive diagnosis of Brugada syndrome had not yet been established, and mildly symptomatic, well-tolerated, FIGURE 3
self-terminating ventricular tachycardia would not be an appropriate indication for an ICD. Repeat testing, including procainamide challenge, was again unrevealing in clarifying a diagnosis, and induced polymorphic ventricular tachycardia at electrophysiology study was not specifically diagnostic. Additionally, there are significant complication risks of ICDs in children, including the high rate of inappropriate shocks.
Before a clear diagnosis of Brugada being established by
electrocardiogramfindings or genetic testing, the provider (M.J.L.) had decided to implant an ICD in this patient. This decision came to be after extensive discussion with the patient and her family as well as with multiple colleagues. The case was discussed with 4 additional pediatric electrophysiologists, 2 of whom stated they would implant an ICD and 2 whom stated they would not in this case. These opinions were openly shared with the family, who ultimately agreed with S-ICD implantation, which is
recommended to mitigate the long-term complications of
a transvenous system. The diagnosis was ultimately confirmed by the febrile electrocardiogramfindings and shortly thereafter by the genetic testing results. The case is illustrative of the wide variation in treatment strategies for nonspecific diagnosticfindings even a life-threatening disease is potentially present.
CONCLUSIONS
The diagnosis of Brugada syndrome, or any rare disease, in children may be difficult. Pediatric diseases can evolve over time. Suspicion and persistence are important qualities for a provider to apply judiciously and may even be critically important in life-threatening diseases, such as Brugada syndrome. The early markers of Brugada syndrome in pediatric patients and the best treatments are yet to be discovered, and future effort should be directed at developing pediatric
electrocardiogram standards as well as management recommendations for pediatric patients.
ABBREVIATIONS
ICD: implantable cardioverter defibrillator
ILR: implantable loop recorder S-ICD: subcutaneous implantable
cardioverter defibrillator
REFERENCES
1. Brugada P, Brugada J. Right bundle branch block, persistent ST segment elevation and sudden cardiac death: a distinct clinical and
electrocardiographic syndrome. A multicenter report.J Am Coll Cardiol. 1992;20(6):1391–1396
2. Priori SG, Wilde AA, Horie M, et al. HRS/ EHRA/APHRS expert consensus statement on the diagnosis and management of patients with inherited primary arrhythmia syndromes:
document endorsed by HRS, EHRA, and APHRS in May 2013 and by ACCF, AHA, PACES, and AEPC in June 2013.Heart Rhythm. 2013;10(12):1932–1963 3. Bayés de Luna A, Brugada J, Baranchuk
A, et al. Current electrocardiographic criteria for diagnosis of Brugada pattern: a consensus report [published correction appears inJ Electrocardiol. 2013;46(1):76].J Electrocardiol. 2012; 45(5):433–442
4. Dumaine R, Towbin JA, Brugada P, et al. Ionic mechanisms responsible for the electrocardiographic phenotype of the Brugada syndrome are temperature dependent.Circ Res. 1999;85(9): 803–809
5. Porres JM, Brugada J, Urbistondo V, García F, Reviejo K, Marco P. Fever unmasking the Brugada syndrome.
Pacing Clin Electrophysiol. 2002;25(11): 1646–1648
6. Kum LC, Fung JW, Sanderson JE. Brugada syndrome unmasked by febrile illness.Pacing Clin
Electrophysiol. 2002;25(11):1660–1661 7. Probst V, Denjoy I, Meregalli PG, et al.
Clinical aspects and prognosis of Brugada syndrome in children.
Circulation. 2007;115(15):2042–2048 8. Conte G, de Asmundis C, Ciconte G, et al.
Follow-up from childhood to adulthood of individuals with family history of Brugada syndrome and normal electrocardiograms.JAMA. 2014; 312(19):2039–2041
DOI: 10.1542/peds.2018-3296 originally published online June 12, 2019;
2019;144;
Pediatrics
Brynn E. Dechert, Martin J. LaPage and Mitchell I. Cohen
Suspicion and Persistence: A Case of Pediatric Brugada Syndrome
Services
Updated Information &
http://pediatrics.aappublications.org/content/144/1/e20183296
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/144/1/e20183296#BIBL
This article cites 9 articles, 3 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/cardiology_sub Cardiology
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2018-3296 originally published online June 12, 2019;
2019;144;
Pediatrics
Brynn E. Dechert, Martin J. LaPage and Mitchell I. Cohen
Suspicion and Persistence: A Case of Pediatric Brugada Syndrome
http://pediatrics.aappublications.org/content/144/1/e20183296
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.