ARTICLE
Behavioral Problems and Cognitive Performance
at 5 Years of Age After Very Preterm Birth:
The EPIPAGE Study
Malika Delobel-Ayoub, MDa,b, Catherine Arnaud, MDa,b,c, Me´lanie White-Koning, PhDa,b, Charlotte Casper, MD, PhDd,
Ve´ronique Pierrat, MD, PhDe,f, Micheline Garel, MScf,g, Antoine Burguet, MD, PhDf,h, Jean-Christophe Roze, MD, PhDi, Jacqueline Matis, MDj, Jean-Charles Picaud, MD, PhDk, Monique Kaminski, MScf,g, Be´atrice Larroque, MD, PhDf,g, for the EPIPAGE Study Group
aInstitut National de la Sante´ et de la Recherche Me´dicale, U558, Research Unit on Perinatal Epidemiology, Child Health, and Development, Toulouse, France; bDepartment of Epidemiology, Universite´ Toulouse III Paul Sabatier, Toulouse, France;cEpidemiology Service anddDepartment of Neonatology, University Hospital of Toulouse (CHU), Toulouse, France;eDepartment of Neonatology, Jeanne de Flandres Hospital, Lille, France;fInstitut National de la Sante´ et de la Recherche Me´dicale, UMR S149, IFR 69, Epidemiological Research Unit on Perinatal Health and Women’s Health, Villejuif, France; ;gUniversite´ Pierre et Marie Curie, UPMC Univ Paris 06, UMR S149, Paris, France;hDepartment of Neonatology, University Hospital (CHU), Dijon, France;iDepartment of Neonatology, Children’s Hospital, Nantes, France;jDepartment of Neonatology, Hautepierre Hospital, Strasbourg, France;kDepartment of Neonatology, University Hospital (CHU) Montpellier, Arnaud de Villeneuve Hospital, Montpellier, France
The authors have indicated they have no financial relationships relevant to this article to disclose.
What’s Known on This Subject
Very preterm children are at risk of inattention and hyperactivity as well as emotional disturbance and poor social competence. Associations between behavioral problems and lower intellectual abilities, environmental factors, parental attitudes, and children’s chronic conditions have been reported for preterm children.
What This Study Adds
This study is one of the few that clearly explores the behavioral outcome of very preterm children while taking into account their cognitive performance. It shows the importance of maternal mental well-being and encourages early detection of these problems.
ABSTRACT
OBJECTIVES.We compared the frequency of behavioral problems in very preterm and term children at 5 years of age. We hypothesized that behavioral problems would be associated with cognitive impairment and environmental factors and that differences between the 2 groups would be reduced but persist after adjusting for cognitive performance and environmental factors.
PATIENTS AND METHODS.The Etude Epide´miologique sur les Petits Ages Gestationnels (EPIPAGE) study was a prospective population-based cohort study that included all births occurring between 22 and 32 weeks’ gestation and a control group of infants born at 39 to 40 weeks’ gestation in 1997 in 9 French regions. Neonatal and obstetrics data were collected at birth. At 5 years of age, sociodemographic status and neuro-developmental and cognitive development of the children, as well as maternal mental well-being, were assessed. The behavioral problems of 1102 very preterm and 375 term singletons without major impairments were studied by using the parent-completed Strengths and Difficulties Questionnaire.
RESULTS.Parents of very preterm children reported significantly more behavioral prob-lems, with a twofold higher prevalence compared with term children for hyperac-tivity/inattention, emotional symptoms, and peer problems. Behavioral problems were associated with low cognitive performance, developmental delay, hospitaliza-tions of the child, young maternal age, and poor maternal mental well-being. Very preterm children were still at higher risk of behavioral problems compared with term children after adjustment for cognitive performance and all others factors.
CONCLUSIONS.Behavioral problems were strongly related to cognitive impairment, but very preterm children were still at higher risk even after adjusting for cognitive performance. Early screening for behavioral problems should be encouraged for all
very preterm children, and maternal well-being should also be the focus of special attention.Pediatrics 2009;123: 1485–1492
A
DVANCES IN PERINATALcare have led to an increase in the survival rates of very preterm children1,2but have also increased the risk of long-term sequelae, such as neurodevelopmental impairment2,3 and behavioral or emo-tional disturbance. Most of the studies on behavioral problems among these children include children born beforewww.pediatrics.org/cgi/doi/10.1542/ peds.2008-1216
doi:10.1542/peds.2008-1216
Key Words
very preterm children, behavioral problems, cognition disorders, cohort study
Abbreviations
EPIPAGE—Etude Epide´miologique sur les Petits Ages Gestationnels
SDQ—Strength and Difficulties Questionnaire
K-ABC—Kaufman Assessment Battery for Children
MPCS—Mental Processing Composite Scale
OR— odds ratio CI— confidence interval
Accepted for publication Sep 25, 2008
Address correspondence to Catherine Arnaud, MD, Institut National de la Sante´ et de la Recherche Me´dicale (INSERM), U558, 37 Alle´es Jules Guesde, 31073 Toulouse Cedex, France. E-mail: [email protected].
1990.4–6However, in the late 1990s, important changes in perinatal care occurred that may also have influenced behavioral outcomes.
Very preterm children are at risk of inattention and hyperactivity,4,7,8and of emotional disturbance and poor social competence, although results for these disorders are less consistent.9–11 Cognitive impairment and poor educational achievement have consistently been re-ported in these children,4,6,9,12 and an association be-tween behavioral difficulties and lower intellectual abil-ities was found whatever the age of assessment.11,13–16 Therefore, cognitive development must be taken into account when studying behavioral disorders in very pre-term children. Associations between behavioral prob-lems and environmental factors, such as social charac-teristics of the family,17,18 parental attitudes,19 and children’s chronic conditions18,20have also been reported but without controlling for cognitive impairment.
We studied behavioral problems at 5 years of age in a large population-based cohort of very preterm children born in 1997 with no major impairment. Our aim was to compare the frequency of behavioral problems in very preterm and term children and to study the extent to which the differences could be explained by differences in cognitive level and the medical or social situation of the children. We hypothesized that differences between groups would persist after adjusting for cognitive perfor-mance and environmental factors would remain associ-ated with behavioral problems after taking into account cognitive performance.
METHODS
Participants
The Etude Epide´miologique sur les Petits Ages Gesta-tionnels (EPIPAGE) study is a population-based cohort study, which followed children from birth until 5 years of age. This study included all live-births occurring at ⬍33 weeks’ gestation and a control group of infants born at 39 to 40 weeks’ gestation in 1997 in 9 French regions. The follow-up was offered at hospital discharge for all infants, except in 2 regions where it was randomly of-fered for only 1 of 2 of those born at 32 weeks’ gestation. Parents were given written information and consent was obtained for the entire follow-up. The study was ap-proved by the Commission Nationale de l’Informatique et des Liberte´s.21
Follow-up was accepted by the parents for 2276 (96%) of 2382 very preterm infants and 557 (84%) of 666 term infants. It consisted of annual questionnaires sent to the parents. At 5 years of age, all children un-derwent medical and psychological examinations. Par-ents also completed a questionnaire that included an assessment of their child’s behavior. Between hospital discharge and the age of 5 years, 25 very preterm and 2 term children died. The questionnaire was completed by parents for 1690 (75%) preterm and 391 (70%) term children. We excluded multiple births (512 preterm and 6 term), because there could be differences in parental assessments of singletons and multiples, and there were too few multiple births in the control group. We
ex-cluded children with severe sensory impairment (blind-ness or deaf(blind-ness) or with severe neuromotor deficiency (63 preterm and 3 term children). In addition, 13 pre-term and 7 pre-term children were excluded, because they wereⱖ6 years of age at the time of assessment. The final sample consisted of 1102 very preterm and 375 term singletons.
Instruments and Measures
Gestational age was expressed in completed weeks of amenorrhea. During the neonatal period, cranial ultra-sound scans were performed in 98% of the very preterm infants and were classified as (1) major lesions: periven-tricular leukomalacia or perivenperiven-tricular parenchymal hemorrhage; (2) moderate lesions: intraventricular hemorrhage with ventricular dilatation or isolated ven-tricular dilatation or echodensity lasting ⬎14 days; (3) minor lesions: intraventricular hemorrhage without ventricular dilatation, germinal matrix layer hemor-rhage; and (4) none of these abnormalities.22
Maternal smoking during pregnancy was assessed at inclusion. Family characteristics were obtained at 5 years of age; social class of the family was assessed by the parents’ highest level of occupation or the mother’s if she lived alone.
The French version of the Strength and Difficulties Questionnaire (SDQ) was completed by the mother only (72%), mother and father (22%), father only (4%), or another caretaker (2%). The SDQ was designed for chil-dren aged 4 to 16 years. It contains 4 scales that assess psychiatric symptoms (hyperactivity/inattention, con-duct, emotional, and peer problems) and a scale that reflects prosocial behavior.23Scores for the 4-symptom scales are summed up to provide a “total difficulties” score ranging from 0 to 40, with higher scores indicating poorer mental health. Cut-offs were defined based on the 10th percentile of the observed scores in the control group (hyperactivityⱖ7, conduct problemsⱖ5, emo-tional symptomsⱖ5, peer problemsⱖ4, prosocial be-haviorⱕ6, and total difficultiesⱖ16). A total difficulties score was available for 1095 preterm and 371 term chil-dren. Behavioral problems in this cohort have already been assessed at the age of 3 years with an adapted version of the SDQ.24
Cognitive performance was assessed by using the French version of the Kaufman Assessment Battery for Children (K-ABC)25 administered by trained psycholo-gists. We used the Mental Processing Composite Scale (MPCS), considered as the equivalent of IQ, to classify cognitive performance into 3 categories: ⬎85, between 70 and 85, and⬍70.
Children’s treatments and hospitalizations since birth were obtained from medical charts. The children were medically examined to detect neurologic pathol-ogy or developmental delay. Parents completed 3 questions concerning the child’s health (excellent, good, or poor), his or her development (precocious, normal, or delayed), and the presence of speech dis-orders.
month: how they felt physically and morally (very good, fairly good, or fairly or very poor), did they feel tired (all the time, sometimes, or neither), and did they take tranquillizers, soporifics, or antidepressants.
Statistical Analysis
As 2 regions followed only 1 in 2 children born at 32 weeks’ gestation,2tests were weighted with Rao and Scott corrections26 and associations were quantified by using weighted odds ratios (ORs) with 95% confidence intervals (CIs). All numbers are those observed, whereas percentages are weighted.
Factors associated with a high total difficulties score in the very preterm children were assessed by using weighted multivariable logistic regression analysis. Co-variates were included in the initial model if they were associated at the 10% significance level in the univariate analysis. A backward procedure was used to remove variables (5% significance level).
To assess which part of the difference in behavioral problems between preterm and term children could be explained by differences in cognitive performance, we compared the rates of high total difficulties score in the 2 groups by using a weighted multivariable logistic re-gression analysis. We then adjusted for the MPCS and for all the variables significantly associated to the SDQ total difficulties score.
Because of missing data concerning maternal smok-ing dursmok-ing pregnancy, especially in the preterm group (14% vs 5% in the control group), separate multivariate analyses were performed.
Analyses were performed with Stata 8.0 software (Stata Corp, College Station, TX).
RESULTS
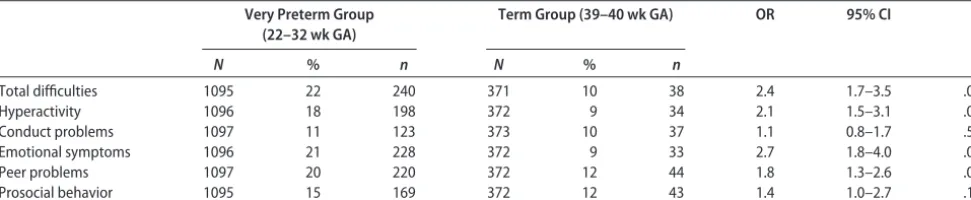
Preterm children were more likely to have high scores in the total difficulties, hyperactivity, emotional symptoms, and peer problems domains (Table 1), with a prevalence approximately twice that of the control group.
In the preterm children group, a strong association was found between behavioral problems and cognitive performance. The MPCS means were significantly lower among children with a high score for all scales of the SDQ (Table 2). Overall, 34% of children with an MPCS score of⬍70 had a high total difficulties score compared with 16% of those with normal cognitive performance (Table 3).
Tables 4 and 5 show factors associated with a high total difficulties score in univariate analyses. In the mul-tivariate model (Table 6), a MPCS score ⬍85, a young
TABLE 1 Proportion of Children With High Scores of Behavioral Problems for Each of the SDQ Domains and According to Gestational Age
Very Preterm Group (22–32 wk GA)
Term Group (39–40 wk GA) OR 95% CI P
N % n N % n
Total difficulties 1095 22 240 371 10 38 2.4 1.7–3.5 .001
Hyperactivity 1096 18 198 372 9 34 2.1 1.5–3.1 .001
Conduct problems 1097 11 123 373 10 37 1.1 0.8–1.7 .55
Emotional symptoms 1096 21 228 372 9 33 2.7 1.8–4.0 .001
Peer problems 1097 20 220 372 12 44 1.8 1.3–2.6 .001
Prosocial behavior 1095 15 169 372 12 43 1.4 1.0–2.7 .10
GA indicates gestational age.
TABLE 2 Mean Scores of Cognitive Performance (Mental Processing Composite) According to the Level of SDQ Scale Score Among Very Preterm Children
Cognitive Performance Score (K-ABC): Mental Processing Composite
Low SDQ Scale Score High SDQ Scale Score Mean Difference in
Scores
N Mean SD N Mean SD Mean 95% CI
Total difficulties score 770 96.4 19.7 207 87.5 18.4 8.9 6–12a
Hyperactivity 803 95.9 19.6 175 88.3 18.8 7.5 4–11a
Conduct problems 882 95.0 19.8 97 90.3 19.1 4.7 1–9b
Emotional symptoms 775 95.3 19.8 203 91.4 19.5 3.9 1–7b
Peer problems 787 95.3 19.9 192 91.1 18.5 4.2 1–7b
Prosocial behavior 837 95.1 19.7 141 91.1 19.9 4.0 0.5–8.0b
aP⬍.001. bP⬍.05.
TABLE 3 High Total Difficulties Score (SDQ) and Cognitive Performance (K-ABC) in Very Preterm Children
Cognitive Performance
(K-ABC)
N High Total Difficulties Score (SDQ)a
P
% n OR 95% CI
MPCS score⬎85 672 16 111 1.0 — ⬍.001
MPCS score⫽70–84 196 29 58 2.1 1.5–3.1 MPCS score⬍70 109 34 38 2.6 1.7–4.1
maternal age at birth, a delay in the development of the child as assessed by the parents, hospitalizations since birth, and poor maternal mental well-being during the previous month remained significantly associated with a high total difficulties score. When maternal smoking during pregnancy was added to the multivariate model, it was independently associated with a high total diffi-culties score (OR: 1.6 [95% CI: 1.1–2.4]). Results for the other covariates remained unchanged, except for hospi-talizations since birth which were no more significantly associated.
Multivariable analyses were performed to compare the risk of having a high total difficulties score in the preterm and the term cohorts (Table 7). The excess risk decreased slightly after adjusting for cognitive perfor-mance and others factors but remained significant.
When maternal smoking during pregnancy was added results remained unchanged (OR: 1.7 [95% CI: 1.1– 2.7]).
Evaluations at both 3 and 5 years of age were avail-able for 977 very preterm children. Of the 179 children who had a high total difficulties score at 3 years of age, 83 (46.3% [95% CI: 38.9%–53.8%]) still had a high score at 5 years. Of the 205 children who had a high score at 5 years of age, 83 (41.0% [95% CI: 34.4%– 48.0%]) already had a high score at 3 years of age. Children who had persistent behavioral problems tended to more frequently have cerebral lesions at neo-natal cranial ultrasound scans than children who were not identified until 5 years of age (40.7% vs 29.3%;P⫽
.10), but their cognitive performance did not differ sig-nificantly.
TABLE 4 Behavioral Problems (High Total Difficulties Score) Among Very Preterm Children According to Characteristics of the Child
N High Total Difficulties Score P
% n OR 95% CI
Gestational age, wk .73
24–26 76 24 18 1.2 0.7–2.1
27–28 180 24 44 1.2 0.8–1.8
29–30 310 21 64 1.0 0.7–1.4
31–32 529 21 114 1.0 —
Gender .005
Male 562 25 142 1.5 1.1–2.0
Female 533 18 98 1.0
Cerebral lesionsa .47
Major 25 16 4 0.7 0.2–2.1
Moderate 151 26 40 1.3 0.9–2.0
Minor 167 21 36 1.0 0.7–1.5
No lesions 736 21 157 1.0 —
Hospitalizations between birth and 5 y of age .002
No 373 16 63 1.0 —
Yes 677 25 169 1.7 1.2–2.3
Long-term treatment .13
No 976 21 210 1.0 —
Yes 82 29 23 1.5 0.9–2.5
Surgical intervention between birth and 5 y of age .04
No 745 20 151 1.0 —
Yes 302 26 78 1.4 1.0–1.9
Neurological pathology or development delayb ⬍.001
No 941 20 191 1.0 —
Yes 120 35 42 2.1 1.4–3.2
Health of the childc .001
Excellent 395 16 65 0.6 0.5–0.9
Good 608 24 145 1.0 —
Poor 90 33 30 1.6 1.0–2.5
Development of the childc ⬍.0001
Normal 877 20 176 1.0 —
Precocious 104 15 15 0.7 0.4–1.2
Delayed 113 43 49 3.1 2.1–4.6
Speech disorderc ⬍.0001
No 856 19 161 1.0 —
Yes 231 33 79 2.1 1.5–2.9
aCranial ultrasound scans in the neonatal period: major lesions, periventricular leukomalacia or periventricular parenchymal
hemor-rhagic involvement; moderate lesions, intraventricular hemorrhage with ventricular dilatation or isolated ventricular dilatation or echodensity lasting⬎14 days; minor lesions, intraventricular hemorrhage without ventricular dilatation, germinal matrix layer hemor-rhage.
DISCUSSION
In this study, parents of very preterm children reported significantly more behavioral problems for their 5-year-old children than did parents of term children. Behav-ioral problems were strongly associated with low cogni-tive performance of the child and environmental factors. Very preterm children were still at higher risk of behav-ioral problems after adjusting for these factors.
The strengths of this longitudinal study are its
gesta-tional age-based recruitment in a large population and a control group with the same follow-up.
One limitation is that some parents refused to partic-ipate or were lost to follow-up. In both the preterm and term groups, nonresponders were more often from lower social backgrounds, as noted elsewhere.27 This may have led to an underestimation of the rates of behavioral problems and cognitive impairment.
The SDQ is a well-validated questionnaire designed for the assessment of behavioral problems in children in the general population. It has been studied in a large nationwide epidemiologic sample of British children and showed satisfactory reliability.23 SDQ scores completed by parents correctly predicted the probability for chil-dren to be independently diagnosed as having psychiat-ric disorders. SDQ scores are strongly correlated with the Rutter questionnaire and the Child Behavior Check-list.28,29Furthermore the inclusion of positive items and
TABLE 5 Familial Characteristics of the Children and Health of the Mothers as Perceived by Themselves Among Very Preterm Children at 5 Years of Age
N High Total Difficulties Score
P
% n OR 95% CI
Maternal age at birth, y .02
⬍25 207 28 60 1.5 1.0–2.1
25–34 678 21 145 1.0 —
ⱖ35 202 17 34 0.7 0.5–1.1
No. of siblings .63
0 356 22 79 1.0 0.8–1.4
1–2 586 21 126 1.0 —
ⱖ3 86 26 22 1.3 0.8–2.2
Mother living alone .16
Yes 117 27 32 1.4 0.9–2.1
No 953 21 201 1.0 —
Secondary school diploma .001
No 713 25 178 1.8 1.2–2.5
Yes 344 16 53 1.0 —
Social class of the familya .006
High 478 18 83 1.0 —
Middle 405 22 93 1.3 1.0–1.9
Low 174 29 52 1.9 1.3–2.9
Mother’s occupation .15
No 455 24 111 1.2 0.9–1.7
Yes 611 20 123 1.0 —
Mother’s nationality .94
French 1000 22 217 1.0 —
Other 77 21 18 1.0 0.6–1.7
Maternal physical well-being .002
Very good 390 16 63 1.0 —
Fairly good 586 25 150 1.8 1.3–2.5
Fairly or very poor 75 25 20 1.7 1.0–3.1
Maternal mental well-being ⬍.0001
Very good 393 15 62 1.0 —
Fairly good 555 24 133 1.7 1.2–2.4
Fairly or very poor 93 40 37 3.6 2.2–6.0
Maternal fatigue ⬍.0001
All the time 278 32 89 2.3 1.5–3.6
Sometimes 539 19 105 1.2 0.8–1.8
Nether 212 17 36 1.0 —
Treatment with tranquillizers, soporifics, or
antidepressants
.003
No 919 21 193 1.0 —
Yes 111 33 36 1.9 1.2–3.0
Maternal smoking during the end of pregnancy
.002
No 656 19 124 1.0 —
Yes 292 28 83 1.7 1.2–2.3
aHighest occupational level of the parents, or occupation of the mother if she lived alone.
TABLE 6 Factors Associated With High Total Difficulties Score at Age 5 in the Very Preterm Groupa
High Total Difficulties Score
Adjusted ORa
95% CI P
Cognitive performance ⬍.0001
MPCS score⬎85 1.0 —
MPCS score⫽70–84 2.6 1.7–3.9
MPCS score⬍70 1.8 1.0–3.2
Maternal age at birth, y .006
⬍25 1.6 1.0–2.4
25–34 1.0 —
ⱖ35 0.6 0.4–1.0
Development of the child assessed by parents .005
Normal 1.0 —
Precocious 0.7 0.3–1.3
Delay 2.4 1.3–4.2
Hospitalizations between birth and 5 y of age 1.6 1.1–2.3 .02 Mental well-being of the mother during
previous month
⬍.001
Very well 1.0 —
Fairly well 1.8 1.2–2.7
Fairly or very poor 3.4 1.9–6.3
Multivariable logistic regression analysis (N⫽861).
aAdjusted for all variables in the table.
TABLE 7 Comparison of Total Difficulties Scale Between Very Preterm and Term Children After Adjustment for Cognitive Performance and Other Major Risk Factors
Very Preterm Children/ Term Children
N High Total
Difficulties Score
OR 95% CI P
Crude OR 1138 2.4 1.6–3.6 ⬍.001
OR adjusted for cognitive performancea 1138 2.0 1.3–3.1 .001 OR adjusted for cognitive performance and
other major risks factorsb
1138 1.8 1.2–2.8 .009
aMental processing composite.
bOther major risks factors: maternal age at birth, health of the child, and development of
the shortness of this instrument make it more acceptable for parents. One of the possible limitations could be that the appreciation of the parents may be influenced by their mental well-being. The absence of significant dif-ferences between the preterm and control group wom-en’s answers concerning their physical or mental well-being suggests that bias was avoided.
We found that, compared with term children, pre-term children had a twofold higher prevalence for inat-tention-hyperactivity, emotional problems, and peer problems but not for conduct problems. Whatever the age of assessment, studies of very preterm or very low birth weight children constantly report increased rates of inattention-hyperactivity problems4,10and in some stud-ies this is the only associated behavioral disorder.7,8,30,31 Emotional problems are also commonly described among these children.9,14,32,33For conduct problems, re-sults are more inconsistent, and only a few studies have found an increased risk among very preterm or very low birth weight children.14,34
Behavioral problems at 3 years of age and their evo-lution between 3 and 5 years of age have rarely been reported.5We found that 41% of the very preterm chil-dren who had a high total difficulties score at 5 years of age already had a high score at 3 years of age, and that 46% of those who had a high total difficulties score at 3 years of age still had a high score at 5 years of age. These results are consistent with those of a prospective study that found a 50% stability of behavioral problems be-tween 3 and 5 years of age.5
Very preterm or very low birth weight children gen-erally have lower IQ scores and more cognitive impair-ment than term children.4,6,9,12,35–37We found that poor cognitive performance in preterm children was strongly related to behavioral problems, a result consistent with previous findings.11,14,16 Moreover, we showed that the increased risk of behavioral problems persisted even af-ter adjusting for cognitive performance. Few studies clearly aimed to determine if differences in the rate of behavioral problems between very low birth weight or very preterm children and term children could be ex-plained by cognitive level. In a cohort of 194 extremely prematurely born children assessed at age 5, lower IQ was found to be associated with hyperactive behavior and poorer social skills, and extremely premature chil-dren were still at increased risk of hyperactive/inatten-tive behavior when controlling for intellectual ability.16 In line with our results, Indredavik et al13found that very low birth weight adolescents were at increased risk for attention-deficit/hyperactivity and anxiety disorder when compared with term controls, even when adoles-cents with low estimated IQ were excluded. Saigal et al15 observed that parents of extremely low birth weight adolescents reported higher scores for attention-deficit/ hyperactivity disorder and depression than parents of term controls even after controlling for developmental quotient and other risk factors.
We failed to find any association between cerebral lesions at neonatal cranial ultrasound scan and a high total difficulties score at 5 years. Some studies have found an association between cerebral lesions and
neu-rologic and cognitive impairment,32,38–40but few studies have specifically focused on the link between cerebral damage and behavior. Consistent with our results, 2 studies did not find any links between behavioral prob-lems and neonatal cerebral abnormalities at cranial ul-trasound scan.11,41However, 1 study reported an associ-ation between lesions suggestive of white matter injury on neonatal cranial ultrasound and psychiatric disorders (especially attention-deficit/hyperactive and anxiety dis-orders) among low birth weight children at 6 years of age.33Other studies have shown that behavioral prob-lems were related to abnormalities detected by MRI at adolescence.13,42It is now acknowledged that, in addi-tion to white matter injury and especially periven-tricular leukomalacia, immaturity is also responsible for a reduction in cerebral cortical gray matter, deep nuclear structures, and corpus callosum.32,38,39,43These cerebral lesions that could be associated with behav-ioral disorders are not easily detected with ultrasound scans while better detected with MRI. Our results may have been slightly different if cerebral lesions had been studied by using MRI.
We did not find any significant relationship between behavioral problems and the degree of immaturity, a result found in other studies.5,9,41
We found that behavioral problems were associated with a delay in the child’s development as assessed by the parents, which has also been described else-where.31,44Hospitalizations since birth were also related to behavioral problems at 5 years of age, an unsurprising result, because childhood illness and chronic physical conditions have been identified as significant risk factors for behavioral problems in very low birth weight chil-dren18,20and in the general population.45
Young maternal age at birth was associated with an increased risk of behavioral problems, a finding previ-ously reported in low birth weight children5and in the general population.45
Despite the large number of missing data, which re-quires prudence in the interpretation, smoking during pregnancy was associated with an increased risk of be-havioral problems, independently of the other risk fac-tors. The persistence of this association after adjustment on social factors and maternal well-being suggests an independent effect of smoking during pregnancy. Such an independent association has been shown among very low birth weight children.5
control-ling for gender, developmental quotient, and socioeco-nomic factors.15
These results underline the multifactorial origins of behavioral problems and have several implications for clinical practice. To reduce the incidence of such prob-lems, clinicians should be encouraged to focus their at-tention on maternal well-being and management of ma-ternal distress from neonatal hospitalization onward.47 Disturbance in parent-child interaction during the neo-natal period, which is not evaluated in this study, could also put very preterm children at higher risk of behav-ioral problems. Programs of developmental care such as the Newborn Individualized Developmental Care and Assessment Program have been shown to improve mother-child interaction48 and behavioral function-ing.48–50Such programs of developmental care were not available in France in 1997 but are now increasingly being put into practice and may help to improve behav-ioral outcomes in very preterm children.
CONCLUSIONS
Early detection of behavioral problems among very pre-term children should be encouraged to deal with these difficulties as early as possible and in the most appropri-ate manner, especially as it has been shown that very preterm or very low birth weight teenagers are also at increased risk for attention-deficit/hyperactivity, depres-sion, and anxiety disorders.13,15,51,52We found that even the less immature children had an increased risk of behavioral problems. Moreover, although behavioral problems were strongly related to cognitive impairment, very preterm children were still at higher risk of behav-ioral problems after adjusting for cognitive performance. These results should encourage early screening for these problems in very preterm children, including the less immature and those without cognitive impairment.
ACKNOWLEDGMENTS
Funding for this study was obtained from the Institut National de la Sante´ et de la Recherche Me´dicale (French National Institute of Health and Medical Research), la Direction Ge´ne´rale de la Sante´ du Ministe`re des Affaires Sociales (the Directorate General for Health of the French Ministry for Social Affairs), Merck-Sharp and Dohme-Chibret, la Fondation de la Recherche Me´dicale (the Medical Research Foundation), and the Programme Hospitalier de Recherche Clinique (the Hospital Program for Clinical Research) of the French Department of Health.
The EPIPAGE Study Group members include Institut National de la Sante´ et de la Recherche Me´dicale (INSERM) U149: B. Larroque (national coordinator), P. Y. Ancel, B. Blondel, G. Bre´art, M. Dehan, M. Garel, M. Kaminski, F. Maillard, C. du Mazaubrun, P. Missy, F. Sehili, K. Supernant, and L. Marchand; Alsace: M. Du-rant, J. Matis, J. Messer, and A. Treisser (Hoˆpital de Hautepierre, Strasbourg); Franche-Comte´: A. Burguet, L. Abraham-Lerat, A. Menget, P. Roth, J.-P. Schaal, and G. Thiriez (CHU St Jacques, Besanc¸on); Haute-Nor-mandie: C. Le´veˆque, S. Marret, and L. Marpeau (Hoˆpital
Charles Nicolle, Rouen); Languedoc-Roussillon: P. Bou-lot and J.-C. Picaud (Hoˆpital Arnaud de Villeneuve, Montpellier), A.-M. Donadio and B. Lede´sert (ORS Montpellier); Lorraine: M. Andre´, J. Fresson, and J. M. Hascoe¨t (Maternite´ Re´gionale, Nancy); Midi-Pyre´ne´es: C. Arnaud, S. Bourdet-Loube`re, and H. Grandjean (INSERM U558, Toulouse), M. Rolland (Hoˆpital des en-fants, Toulouse); Nord-Pas-de-Calais: C. Leignel, P. Lequien, V. Pierrat, F. Puech, D. Subtil, and P. Truffert (Hoˆpital Jeanne de Flandre, Lille); Pays de la Loire: G. Boog, V. Rouger-Bureau, and J.-C. Roze´ (Hoˆpital Me`re Enfants, Nantes); and Paris-Petite-Couronne: P.-Y. Ancel, G. Bre´art, M. Kaminski, and C. du Mazaubrun (INSERM U149, Paris), M. Dehan and V. Zupan-Simu-nek (Hoˆpital Antoine Be´cle`re, Clamart), and M. Vodo-var, M. Voyer (Institut de Pue´riculture, Paris).
We thank Dr He´le`ne Grandjean for invaluable assis-tance throughout this work.
REFERENCES
1. Schwartz RM, Luby AM, Scanlon JW, Kellogg RJ. Effect of surfactant on morbidity, mortality, and resource use in new-born infants weighing 500 to 1500 g. N Engl J Med. 1994; 330(21):1476 –1480
2. Wilson-Costello D, Friedman H, Minich N, Fanaroff AA, Hack M. Improved survival rates with increased neurodevelopmen-tal disability for extremely low birth weight infants in the 1990s.Pediatrics.2005;115(4):997–1003
3. Anderson PJ, Doyle LW. Executive functioning in school-aged children who were born very preterm or with extremely low birth weight in the 1990s.Pediatrics.2004;114(1):50 –57 4. Bhutta AT, Cleves MA, Casey PH, Cradock MM, Anand KJ.
Cognitive and behavioral outcomes of school-aged children who were born preterm: a meta-analysis.JAMA.2002;288(6): 728 –737
5. Gray RF, Indurkhya A, McCormick MC. Prevalence, stability, and predictors of clinically significant behavior problems in low birth weight children at 3, 5, and 8 years of age. Pediatrics. 2004;114(3):736 –743
6. Saigal S, den Ouden L, Wolke D, et al. School-age outcomes in children who were extremely low birth weight from four in-ternational population-based cohorts. Pediatrics.2003;112(4): 943–950
7. Breslau N, Brown GG, DelDotto JE, et al. Psychiatric sequelae of low birth weight at 6 years of age.J Abnorm Child Psychol. 1996;24(3):385– 400
8. Foulder-Hughes LA, Cooke RW. Motor, cognitive, and behav-ioural disorders in children born very preterm.Dev Med Child Neurol.2003;45(2):97–103
9. Anderson P, Doyle LW. Neurobehavioral outcomes of school-age children born extremely low birth weight or very preterm in the 1990s.JAMA.2003;289(24):3264 –3272
10. Chapieski ML, Evankovich KD. Behavioral effects of prematu-rity.Semin Perinatol.1997;21(3):221–239
11. Weisglas-Kuperus N, Koot HM, Baerts W, Fetter WP, Sauer PJ. Behaviour problems of very low-birthweight children.Dev Med Child Neurol.1993;35(5):406 – 416
12. Marlow N, Wolke D, Bracewell MA, Samara M. Neurologic and developmental disability at six years of age after extremely preterm birth.N Engl J Med.2005;352(1):9 –19
13. Indredavik MS, Skranes JS, Vik T, et al. Low-birth-weight adolescents: psychiatric symptoms and cerebral MRI abnormal-ities.Pediatr Neurol.2005;33(4):259 –266
Preva-lence of behaviour disorders in low birthweight infants.Arch Dis Child.1994;70(4):271–274
15. Saigal S, Pinelli J, Hoult L, Kim MM, Boyle M. Psychopathol-ogy and social competencies of adolescents who were ex-tremely low birth weight.Pediatrics.2003;111(5 pt 1):969 –975 16. Hoff B, Hansen BM, Munck H, Mortensen EL. Behavioral and social development of children born extremely premature: 5-year follow-up.Scand J Psychol.2004;45(4):285–292 17. Girouard PC, Baillargeon RH, Tremblay RE, Glorieux J,
Lefeb-vre F, Robaey P. Developmental pathways leading to external-izing behaviors in 5 year olds born before 29 weeks of gesta-tion.J Dev Behav Pediatr.1998;19(4):244 –253
18. McCormick MC, Workman-Daniels K, Brooks-Gunn J. The behavioral and emotional well-being of school-age children with different birth weights.Pediatrics.1996;97(1):18 –25 19. Forcada-Guex M, Pierrehumbert B, Borghini A, Moessinger A,
Muller-Nix C. Early dyadic patterns of mother-infant interac-tions and outcomes of prematurity at 18 months. Pediatrics. 2006;118(1). Available at: www.pediatrics.org/cgi/content/ full/118/1/e107
20. McGrath MM, Sullivan M, Devin J, et al. Early precursors of low attention and hyperactivity in a preterm sample at age four.Issues Compr Pediatr Nurs.2005;28(1):1–15
21. Larroque B, Breart G, Kaminski M, et al. Survival of very preterm infants: EPIPAGE, a population based cohort study. Arch Dis Child Fetal Neonatal Ed.2004;89(2):F139 –F144 22. Larroque B, Marret S, Ancel PY, et al. White matter damage
and intraventricular hemorrhage in very preterm infants: the EPIPAGE study.J Pediatr.2003;143(4):477– 483
23. Goodman R. Psychometric properties of the strengths and dif-ficulties questionnaire.J Am Acad Child Adolesc Psychiatry.2001; 40(11):1337–1345
24. Delobel-Ayoub M, Kaminski M, Marret S, et al. Behavioral outcome at 3 years of age in very preterm infants: the EPIPAGE study.Pediatrics.2006;117(6):1996 –2005
25. Kaufman AKN.Batterie Pour l’Examen Psychologique de l’Enfant. Paris, France: Editions du Centre de Psychologie Applique´e; 1993
26. Rao JN, Scott AJ. A simple method for the analysis of clustered binary data.Biometrics.1992;48(2):577–585
27. Wolke D, Sohne B, Ohrt B, Riegel K. Follow-up of preterm children: important to document dropouts. Lancet. 1995; 345(8947):447
28. Goodman R. The Strengths and Difficulties Questionnaire: a research note.J Child Psychol Psychiatry.1997;38(5):581–586 29. Goodman R, Scott S. Comparing the Strengths and Difficulties
Questionnaire and the Child Behavior Checklist: is small beau-tiful?J Abnorm Child Psychol.1999;27(1):17–24
30. McCormick MC, Gortmaker SL, Sobol AM. Very low birth weight children: behavior problems and school difficulty in a national sample.J Pediatr.1990;117(5):687– 693
31. Szatmari P, Saigal S, Rosenbaum P, Campbell D, King S. Psy-chiatric disorders at five years among children with birth-weights less than 1000g: a regional perspective.Dev Med Child Neurol.1990;32(11):954 –962
32. Peterson BS, Vohr B, Staib LH, et al. Regional brain volume abnormalities and long-term cognitive outcome in preterm infants.JAMA.2000;284(15):1939 –1947
33. Whitaker AH, Van Rossem R, Feldman JF, et al. Psychiatric outcomes in low-birth-weight children at age 6 years: relation to neonatal cranial ultrasound abnormalities.Arch Gen Psychi-atry.1997;54(9):847– 856
34. Ross G, Lipper EG, Auld PA. Social competence and behavior problems in premature children at school age.Pediatrics.1990; 86(3):391–397
35. Kilbride HW, Thorstad K, Daily DK. Preschool outcome of less
than 801-gram preterm infants compared with full-term sib-lings.Pediatrics.2004;113(4):742–747
36. Mikkola K, Ritari N, Tommiska V, et al. Neurodevelopmental outcome at 5 years of age of a national cohort of extremely low birth weight infants who were born in 1996 –1997.Pediatrics. 2005;116(6):1391–1400
37. Olse´n P, Vainionpaa L, Paakko E, Korkman M, Pyhtinen J, Jarvelin MR. Psychological findings in preterm children related to neurologic status and magnetic resonance imaging. Pediat-rics.1998;102(2 pt 1):329 –336
38. Peterson BS, Anderson AW, Ehrenkranz R, et al. Regional brain volumes and their later neurodevelopmental correlates in term and preterm infants. Pediatrics. 2003;111(5 pt 1): 939 –948
39. Inder TE, Warfield SK, Wang H, Huppi PS, Volpe JJ. Abnormal cerebral structure is present at term in premature infants. Pediatrics.2005;115(2):286 –294
40. Miller SP, Ferriero DM, Leonard C, et al. Early brain injury in premature newborns detected with magnetic resonance imag-ing is associated with adverse early neurodevelopmental out-come.J Pediatr.2005;147(5):609 – 616
41. Sommerfelt K, Troland K, Ellertsen B, Markestad T. Behavioral problems in low-birthweight preschoolers.Dev Med Child Neu-rol.1996;38(10):927–940
42. Stewart AL, Rifkin L, Amess PN, et al. Brain structure and neurocognitive and behavioural function in adolescents who were born very preterm.Lancet.1999;353(9165):1653–1657 43. Inder TE, Huppi PS, Warfield S, et al. Periventricular white
matter injury in the premature infant is followed by reduced cerebral cortical gray matter volume at term.Ann Neurol.1999; 46(5):755–760
44. Nadeau L, Boivin M, Tessier R, Lefebvre F, Robaey P. Me-diators of behavioral problems in 7-year-old children born after 24 to 28 weeks of gestation.J Dev Behav Pediatr.2001; 22(1):1–10
45. Gortmaker SL, Walker DK, Weitzman M, Sobol AM. Chronic conditions, socioeconomic risks, and behavioral problems in children and adolescents.Pediatrics.1990;85(3):267–276 46. Singer LT, Salvator A, Guo S, Collin M, Lilien L, Baley J.
Maternal psychological distress and parenting stress after the birth of a very low-birth-weight infant.JAMA.1999;281(9): 799 – 805
47. Melnyk BM, Feinstein NF, Alpert-Gillis L, et al. Reducing pre-mature infants’ length of stay and improving parents’ mental health outcomes with the Creating Opportunities for Parent Empowerment (COPE) neonatal intensive care unit program: a randomized, controlled trial.Pediatrics.2006;118(5). Available at: www.pediatrics.org/cgi/content/full/118/5/e1414
48. Kleberg A, Westrup B, Stjernqvist K. Developmental outcome, child behaviour and mother-child interaction at 3 years of age following Newborn Individualized Developmental Care and Intervention Program (NIDCAP) intervention.Early Hum Dev. 2000;60(2):123–135
49. Als H, Duffy FH, McAnulty GB, et al. Early experience alters brain function and structure.Pediatrics.2004;113(4):846 – 857 50. Westrup B, Bohm B, Lagercrantz H, Stjernqvist K. Preschool outcome in children born very prematurely and cared for according to the Newborn Individualized Developmental Care and Assessment Program (NIDCAP).Acta Paediatr.2004;93(4): 498 –507
51. Gardner F, Johnson A, Yudkin P, et al. Behavioral and emotional adjustment of teenagers in mainstream school who were born before 29 weeks’ gestation.Pediatrics.2004;114(3):676 – 682 52. Indredavik MS, Vik T, Heyerdahl S, Kulseng S, Brubakk AM.
DOI: 10.1542/peds.2008-1216
2009;123;1485
Pediatrics
Jacqueline Matis, Jean-Charles Picaud, Monique Kaminski and Béatrice Larroque
Véronique Pierrat, Micheline Garel, Antoine Burguet, Jean-Christophe Roze,
Malika Delobel-Ayoub, Catherine Arnaud, Mélanie White-Koning, Charlotte Casper,
Preterm Birth: The EPIPAGE Study
Behavioral Problems and Cognitive Performance at 5 Years of Age After Very
Services
Updated Information &
http://pediatrics.aappublications.org/content/123/6/1485
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/123/6/1485#BIBL
This article cites 49 articles, 18 of which you can access for free at:
Subspecialty Collections
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_ Fetus/Newborn Infant
al_issues_sub
http://www.aappublications.org/cgi/collection/development:behavior Developmental/Behavioral Pediatrics
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2008-1216
2009;123;1485
Pediatrics
Jacqueline Matis, Jean-Charles Picaud, Monique Kaminski and Béatrice Larroque
Véronique Pierrat, Micheline Garel, Antoine Burguet, Jean-Christophe Roze,
Malika Delobel-Ayoub, Catherine Arnaud, Mélanie White-Koning, Charlotte Casper,
Preterm Birth: The EPIPAGE Study
Behavioral Problems and Cognitive Performance at 5 Years of Age After Very
http://pediatrics.aappublications.org/content/123/6/1485
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.