Open Access
Research
Quantification of functional weakness and abnormal synergy
patterns in the lower limb of individuals with chronic stroke
Nathan Neckel*
1,3, Marlena Pelliccio
1,2, Diane Nichols
1,2and
Joseph Hidler
1,3Address: 1Center for Applied Biomechanics and Rehabilitation Research(CABRR), National Rehabilitation Hospital, 102 Irving Street, NW,
Washington, DC 20010, USA, 2Physical Therapy Service, National Rehabilitation Hospital, 102 Irving Street, NW, Washington, DC 20010, USA
and 3Department of Biomedical Engineering, Catholic University, 620 Michigan Ave., NE, Washington, DC 20064, USA
Email: Nathan Neckel* - [email protected]; Marlena Pelliccio - [email protected]; Diane Nichols - [email protected]; Joseph Hidler - [email protected]
* Corresponding author
Abstract
Background: The presence of abnormal muscle activation patterns is a well documented factor limiting
the motor rehabilitation of patients following stroke. These abnormal muscle activation patterns, or synergies, have previously been quantified in the upper limbs. Presented here are the lower limb joint torque patterns measured in a standing position of sixteen chronic hemiparetic stroke subjects and sixteen age matched controls used to examine differences in strength and coordination between the two groups.
Methods: With the trunk stabilized, stroke subjects stood on their unaffected leg while their affected foot
was attached to a 6-degree of freedom load cell (JR3, Woodland CA) which recorded forces and torques. The subjects were asked to generate a maximum torque about a given joint (hip abduction/adduction; hip, knee, and ankle flexion/extension) and provided feedback of the torque they generated for that primary joint axis. In parallel, EMG data from eight muscle groups were recorded, and secondary torques generated about the adjacent joints were calculated. Differences in mean primary torque, secondary torque, and EMG data were compared using a single factor ANOVA.
Results: The stroke group was significantly weaker in six of the eight directions tested. Analysis of the
secondary torques showed that the control and stroke subjects used similar strategies to generate maximum torques during seven of the eight joint movements tested. The only time a different strategy was used was during maximal hip abduction exertions where stroke subjects tended to flex instead of extend their hip, which was consistent with the classically defined "flexion synergy." The EMG data of the stroke group was different than the control group in that there was a strong presence of co-contraction of antagonistic muscle groups, especially during ankle flexion and ankle and knee extension.
Conclusion: The results of this study indicate that in a standing position stroke subjects are significantly
weaker in their affected leg when compared to age-matched controls, yet showed little evidence of the classic lower-limb abnormal synergy patterns previously reported. The findings here suggest that the primary contributor to isometric lower limb motor deficits in chronic stroke subjects is weakness. Published: 20 July 2006
Journal of NeuroEngineering and Rehabilitation 2006, 3:17 doi:10.1186/1743-0003-3-17
Received: 01 December 2005 Accepted: 20 July 2006
This article is available from: http://www.jneuroengrehab.com/content/3/1/17
© 2006 Neckel et al; licensee BioMed Central Ltd.
Background
Muscle weakness, or the inability to generate normal lev-els of force, has clinically been recognized as one of the limiting factors in the motor rehabilitation of patients fol-lowing stroke [1,2]. In the lower limbs, this muscle weak-ness can be attributed to disuse atrophy [3] and/or the disruption in descending neural pathways leading to inadequate recruitment of motorneuron pools [1,4-6]. It has also been reported that weakness following stroke may be the result of co-contraction of antagonistic mus-cles [7-9]. Spasticity has also been proposed as an alterna-tive explanation for lower limb impairments in hemiparetic stroke [10,11], but more recent studies have found that spasticity may not play a significant role in gait abnormalities [12,13].
A well documented factor limiting the motor rehabilita-tion of patients following stroke is the presence of abnor-mal muscle activation patterns. Following stroke, some patients lose independent control over select muscle groups, resulting in coupled joint movements that are often inappropriate for the desired task [14,15]. These coupled movements are known as synergies and, for the lower limb, have been grouped into the extension synergy (internal rotation, adduction, and extension of the hip, extension of the knee and extension and inversion of the ankle) and the flexion synergy (external rotation, abduc-tion, and flexion of the hip, flexion of the knee, and flex-ion and eversflex-ion of the ankle) [16,17] with varying levels of completeness [18] and dominance [19].
Much of the literature attempting to quantify these abnor-mal muscle synergies is focused on the paretic upper limb of stroke patients. In isometric conditions, it has been shown that stroke patients have a limited number of upper limb synergies available to them due to abnormal muscle coactivation patterns [20]. In dynamic tasks, abnormal synergy patterns exist in the paretic upper limb between shoulder abduction with elbow flexion as well as shoulder adduction with elbow extension [21]. These, and other inappropriate upper limb muscle synergy pat-terns were attributed to abnormal torque generation about joints secondary to the intended, or primary, joint axis during maximal voluntary isometric contractions [22].
This analysis technique of quantifying torques at joints secondary to the intended joint axis was applied to the lower limbs of cerebral palsy patients in a seated position, where abnormal secondary joint torques were expressed during maximal hip and knee extension [23]. However, it has been shown that gravity can influence the control of limb movements by affecting sensory input [24] and alter-ing task mechanics [25,26]. When acute (<6 weeks post-injury) stroke subjects were placed in a functionally
rele-vant weight-bearing anti-gravity standing position, no such abnormal secondary joint torque patterns during maximal voluntary isometric contractions were found, even though primary joint torques deficits were observed [27].
The goal of this study was to quantify lower limb weak-ness and coordination in chronic (> 1 year post-injury) stroke patients in a functionally relevant standing posi-tion. Subjects were asked to generate maximum isometric contractions about a given joint while torques at joints secondary to the desired exertion were simultaneously cal-culated and recorded. This allowed us to quantify weak-ness as a torque deficit and coordination as the generation of any synergy patterns in the lower limbs of hemiparetic stroke patients. Additionally, EMG activity of relevant muscles was simultaneously recorded to quantify the presence of abnormal muscle activation patterns.
Methods
SubjectsSixteen subjects (9 male, 7 female) with hemiparesis resulting from a single unilateral cortical or sub-cortical brain lesion at least one year prior to testing participated in this study along with sixteen (9 male, 7 female) neuro-logically intact age-matched controls. Subjects were excluded from the study if they were too severely impaired to voluntarily move about the ankle, knee, and hip joints, measured by a Fugl-Meyer lower limb score below 10 out of 34. Subjects with a Fugl-Meyer lower limb score greater than 30 out of 34 were deemed very highly functional and excluded. The synergy control sub-score of the Fugl-Meyer assessment was also used to characterize subjects. This clinical score (0–22) reflects the ability to move within (0–14), to combine (15–18), or to move out of (19–22) classically defined dynamic synergy patterns. Although some subjects scored high on the Fugl-Meyer lower limb and synergy control sub-score, all subjects exhibited diffi-culty in walking typical of hemiplegic stroke subjects. Sub-jects were also screened for cognitive and communication impairments and only those with Mini Mental State Examination scores greater or equal to 22 were tested. All subjects were excluded for any uncontrolled cardiovascu-lar, neurological, or orthopaedic conditions, such as high blood pressure, arthritis, or history of seizure, that would inhibit exercise in a standing position. Informed consent was obtained before testing and all protocols were approved by the local institutional review boards. The clinical characteristics of each subject group is shown in Table 1.
Instrumentation
affected foot was securely placed inside a custom foot retainer which in turn was connected to a 6-axis load cell (JR3, Woodland CA). The foot retainer was angled down 30 degrees with respect to the horizontal so that all sub-jects had an ankle angle of 100 degrees and a knee angle of 135 degrees. Large foam bumpers were used to support the subject's trunk during the exertions. Because the tests were done with the subject in a standing posture, a har-ness was placed around the subject's abdomen and attached to an over-head body-weight support system in order to prevent falls. No support was provided by the sys-tem during the tests. Some subjects did, however, sit down in the harness between trials to rest their support leg. Additionally, a heart rate monitor was placed around the subject's chest which was repeatedly checked during test-ing by a physical therapist to ensure the exertions did not elevate the subject's heart rate to unsafe levels. A monitor
for biofeedback was placed in front of the subjects to rein-force exertions along each joint axis.
Electromyographic (EMG) recordings were collected using a Bagnoli-8 EMG system (Delsys, Inc., Boston, MA) with surface electrodes placed above the muscle belly's of the tibilias anterior, gastrocnemius, biceps femoris, vastus medialis, rectus femoris, gluteus maximus, gluteus medius, and adductor longus, and a common reference electrode placed on the patella. Electrode sites were abraded with a rough sponge and cleaned with isopropyl alcohol. The Ag-AgCl electrodes (contact dimension 10 mm × 1 mm, contact spacing 10 mm) were prepped with adhesive stickers and electrode gel. The preamplifiers pro-vided a gain of ×10+-2%, the amplifiers a gain selectable from ×100 to ×10,000 with a bandwidth of 20–450 Hz. Experimental Set-up
Figure 1
Experimental Set-up. A. Subjects were secured in a standing position with foam bumpers pinching the hips from four sides
and a safety harness prevented subjects from slipping down. The subject's foot was attached to a boot that was fixed to a six DOF load cell that would measure joint torques about the hip, knee and ankle. A monitor provided feedback on the torque generated in the primary joint direction. EMG activity was recorded from eight muscles. B. Photograph of experimental setup.
The common mode rejection ratio was >80 dB at 60 Hz
and the input impedance was >1015//0.2 ohm//pF.
EMG data, along with the forces and torques from the load cell, were anti-alias filtered at 500 Hz prior to sam-pling at 1000 Hz using a 16-bit data acquisition board (Measurement Computing, PCI-DAS 6402, Middleboro, MA) and custom data acquisition software written in Mat-lab (Mathworks Inc. Natick, MA) and stored for later anal-ysis.
Protocol
Subjects were asked to generate maximum voluntary tor-ques (MVTs) about eight different joint directions (ankle, knee, and hip flexion and extension, as well as hip abduc-tion and adducabduc-tion). For each joint direcabduc-tion, the subject was allowed to practice until they understood the task, after which three trials were recorded. Subjects were watched closely to make sure that they maintained their legs in the proper geometry. Trials were discarded and re-collected if subjects attempted to change leg geometry in order to achieve maximum torques. A minimum of one minute rest period was given between each trial. The sub-jects would start in a relaxed state and slowly ramp up to a maximum which was held for approximately 4 seconds. Visual feedback of the torque generated only along the desired direction was provided by a speedometer style dis-play on the monitor. The order of joint movements was selected to minimize subject fatigue (hip adduction, knee
flexion, hip extension, ankle flexion, hip abduction, knee extension, hip flexion, ankle extension). All subjects fol-lowed the same order of selected joint torques. Verbal encouragement and instructions were provided through-out the experiment.
Data analysis
For each trial the MVT, or primary torque, as well as the three secondary torques were measured along with the EMG data from the eight selected muscles. The different joint torques were computed by taking the forces and tor-ques measured by the load cell (denoted frame {o}) and transforming them back to the different joints using a homogeneous transformation matrix [28]. From the load cell, ankle torques can be calculated from:
where is a 3 × 3 rotation matrix from {o} to {a},
is a 3 × 3 skew matrix from {o} to {a}, and Fi
and Ti denote force and torque in each respective frame.
Ankle forces and moments can then be transformed back to the knee as:
F T
R
P R R
F T
a a
a
a a a
⎡ ⎣
⎢ ⎤
⎦ ⎥ =
× ⎡
⎣ ⎢ ⎢
⎤
⎦ ⎥ ⎥ ⎡ ⎣
⎢ ⎤
⎦
⎥ ( )
×
0
o o o o o
0
1 3 3
oaR a
o oa
P × R
Table 1: Clinical Characteristics of Subjects
Group Gender Age (years) Paretic Leg Tested Months Post-Stroke Synergy Control (max. = 22)
Fugl-Meyer Score %
Stroke Survivors F 30 R 39 13 79
F 36 R 26 21 88
F 48 R 13 21 68
F 51 L 54 21 91
F 53 L 36 6 53
F 57 L 26 20 53
F 64 R 14.5 9 88
M 44 R 149 17 71
M 50 R 194 16 53
M 50 R 29 14 56
M 55 R 34 10 68
M 56 R 30 15 47
M 59 L 13.5 16 44
M 63 L 23 11 47
M 68 L 20 19 47
M 69 R 18.5 11 76
Stroke 9 male 53.31 10 right leg 44.97 15 64.34
Average 7 female (+/-10.68) 6 left leg (51.18) (4.72) (16.46)
Control Average 9 male 7
female
57.13 (+/-8.85)
10 right leg 6 left leg / / /
And from the knee to hip as:
The skew and rotation matrices are formed from anatom-ical measurements while the subject is in the setup (shank and thigh lengths, knee and shank angles).
A MVT was defined as the peak torque sustained for 200 ms observed across any one of the 3 trials for that primary joint direction. The corresponding secondary torques exerted along the other joint axes during the 200 ms MVT window were also identified. For example, during maxi-mum voluntary knee flexion exertions, secondary torques consisted of those generated along the ankle flexion-extension axis, hip flexion-flexion-extension axis, and hip abduc-tion-adduction axis. Secondary torques generated during all trials were normalized to the MVT measured for that particular joint direction. Cases where a secondary torque exceeded 100% MVT indicated that the subject generated less torque while attempting to maximize that particular direction than when they were trying to maximize a differ-ent direction.
The EMG activity from the eight selected muscle groups was band-pass filtered (20–450 Hz), full-wave rectified, and then smoothed using a 200-point RMS algorithm. Each EMG trace was then normalized to the maximum EMG value observed across all trials for the respective muscle. This allowed for muscle activity demonstrated during the 200 ms MVT window to be expressed as the percentage of peak activity observed in each muscle.
Statistical analysis
A single factor ANOVA was used to compare the means of the chronic stroke subjects to the control subjects for each of the eight primary joint torque directions. A single factor ANOVA was used to compare the mean secondary tor-ques, as well as the mean EMGs, between the stroke and control groups. An independent Student's t-test was used to identify secondary torques that were significantly greater than zero (P < 0.05). Correlations (Pearson's, 2-tailed) between joint torque were found by grouping all data from the eight primary torque directions and com-paring all instances of one torque direction with the activ-ity at the other three joints. For example, all instances of hip abduction were compared with the torques of the hip, knee and ankle, regardless if it was flexion or extension.
Statistical analyses was performed with the software pack-age SPSS (SPSS Inc, Chicago, IL) and a confidence level of 0.05 was used for all comparisons.
The role of co-activation of antagonistic muscles on observed joint weakness was investigated by computing a co-contraction index (CI) for each primary torque direc-tion as follows:
where PCSA is the physiological cross sectional area of the healthy adult muscle [29]. The total activity demonstrated in the agonist muscle groups divided by the total muscle activity demonstrated in the antagonistic muscle groups results in the CI for that primary torque direction. One or more of the eight muscles recorded from were regarded as agonist/antagonist muscles for each primary torque direc-tion (ankle flexor – tibilias anterior, ankle extensor – gas-trocnemius, knee flexors – gastrocnemius and biceps femoris, knee extensors – vastus medialis and rectus fem-oris, hip flexor – rectus femoris and adductor longus, hip extensors – gluteus maximus and biceps femoris, hip abductor – gluteus medius, hip adductor – adductor lon-gus and gluteus maximus). It was important to scale the muscle activity by the PCSA since activity in large muscle groups generated significantly higher forces than activity in muscles with smaller cross-sectional area. The CI is a simple numerical measure of how much co-activation of antagonistic muscle groups subjects exhibit. Low CI occurs when subjects simultaneously activate agonist and antagonist muscle groups, whereas high CI is indicative of low levels of co-contraction. High levels of co-contraction (Low CI) would result in decreasing levels of torque exerted at the joint. A single factor ANOVA test was used to compare the mean CI values of the chronic stroke sub-jects to the control subsub-jects with a significance level of p < 0.05.
Results
Maximum voluntary torque
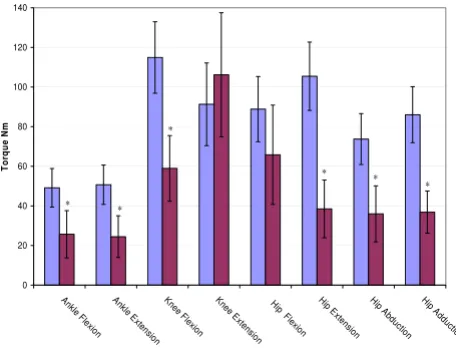
The maximum voluntary primary torques for the eight joint directions are shown in figure 2. The stroke group was significantly weaker (p < 0.05) for all joint directions except for knee extension and hip flexion. The average stroke hip flexion torque was less than the control group, but with a higher variability. The average stroke knee extension torque was actually larger than the control group, but again, with a higher variability.
Secondary torque and EMG patterns
Figures 3 through 6 show the normalized secondary torque patterns as well as the normalized EMG activity for all control subjects and all but one stroke subject during
F T
R
P R R
F T
k k
k
k k k
⎡ ⎣
⎢ ⎤
⎦ ⎥ =
× ⎡
⎣ ⎢ ⎢
⎤
⎦ ⎥ ⎥ ⎡ ⎣
⎢ ⎤
⎦
⎥ ( )
×
a
a a a a a
0
2 3 3
F T
R
P R R
F T
h h
h
h h h
⎡ ⎣
⎢ ⎤
⎦ ⎥ =
× ⎡
⎣ ⎢ ⎢
⎤
⎦ ⎥ ⎥ ⎡ ⎣
⎢ ⎤
⎦
⎥ ( )
×
k
k k k k k
0
3 3 3
CI PCSA EMG
PCSA EMG
i agonist i j antagonist j
= ∗
∗ ( )
∑
∑
,,the eight different primary directions. EMG data for one stroke subject was improperly collected and has hence been omitted. The stick figure diagrams illustrate the sec-ondary torque generation that was significantly greater than zero (P < 0.05). A more detailed discussion of the dif-ferent joint directions is presented below.
Ankle flexion/extension
As illustrated in Figure 3, during ankle flexion, both con-trols and stroke subjects generated knee extension and hip flexion secondary torques. While generating maximal ankle flexion, the stroke subjects had significantly less tibilias anterior activity but significantly greater gastrocne-mius, biceps femoris, gluteus maximus, and gluteus medius activity. During maximal ankle extension exer-tions, the stroke subjects generated a knee flexion second-ary torque that was significantly higher than the control subjects (p < 0.05). The EMG pattern on the right side of figure 3 shows that the stroke subjects had significantly less gastrocnemius muscle activity and significantly greater tibilias anterior, biceps femoris, vastus medialis, rectus femoris, gluteus maximus, and adductor longus muscle activity during maximal ankle extension exertions.
Knee flexion/extension
During maximal knee flexion exertions, both groups gen-erated ankle extension, hip extension and hip adduction secondary torques that were not different from each other (Figure 4). Interestingly, the stroke subjects had signifi-cantly greater gluteus maximus, and gluteus medius
activ-ity during maximum knee flexion exertions despite the fact that they did not produce larger hip extension second-ary torque. For knee extension, both groups produced ankle flexion, hip flexion and hip abduction secondary torques however the ankle flexion secondary torque was significantly larger in the stroke group, and significantly greater than 100%. The hip flexion secondary torque was also greater than 100% in the control group but not signif-icantly different than the stroke group. The EMG pattern illustrates that the stroke group had a greater gastrocne-mius and biceps femoris activity during knee extension MVT.
Secondary Torques During Ankle Flexion/Extension Figure 3
Secondary Torques During Ankle Flexion/Extension.
The top graphs show the secondary joint torques for the stroke (red) and control (blue) groups expressed in %MVT for ankle flexion (left) and ankle extension (right). The stick figures show the primary joint direction (green) as well as the secondary torques of the control (blue) and stroke (red) for the secondary joint torques that are significantly greater than zero. Abduction is denoted as a circled dot (out of the page), adduction is denoted a circled X (into the page). The bottom graph shows the EMG activity for the stroke (red) and con-trol (blue) groups expressed in % maximum value during ankle flexion MVT (left) and ankle extension MVT (right). Error bars represent 95% confidence interval. Significant dif-ferences between groups (p < 0.05) are denoted *. Tib Ant – tibilias anterior, Gas – gastrocnemius, Bi Fem – biceps femo-ris, Vast Med – vastus medialis, Rect Fem – rectus femofemo-ris, Glut Max -gluteus maximus, Glut Med – gluteus medius, Add Long – adductor longus.
Ankle Flexion Ankle Extension 0 10 20 30 40 50 60 70 80 90 Tib A nt Ga s Ham S tr Vas t M ed Re ct Fem Gl utM ax Gl ut M ed Add Lon g Tib A nt
Gas Ham S tr Vas t M ed Re ct F em Gl utM ax Gl ut M ed Add Lon g
Ankle Flexion Ankle Extension
% Ma xi mu m * * * * * Ti b A nt Ga
s Bi Fe m Va st M ed Rec t Fe m Gl ut M ax Gl ut M ed Ad d Long Tib An
t Ga
s Bi FemVast M ed Rec t F em G lu t Ma x Gl ut M ed Ad d Long
* * * * * * * -150 -100 -50 0 50 100 150 Ank le K
nee Hip Hip Ankl e
K ne
e Hi
p Hip
Ankle Flexion Ankle Extension
% M
V
T
Extension Flexion Flexion Extension Flexion Abduction
Flexion Abduction
*
Maximum Voluntary Torques Figure 2
Maximum Voluntary Torques. The maximum voluntary
joint torques for the stroke (red) and control (blue) groups expressed in Newton meters for the eight primary directions ankle flexion through hip adduction. Error bars represent 95% confidence interval. Significant differences (p < 0.05) are denoted *. 0 20 40 60 80 100 120 140 An kle Fl
ex ion
An kle Ex
ten sion Kn ee F lexi on Kn ee E xt ensi on H
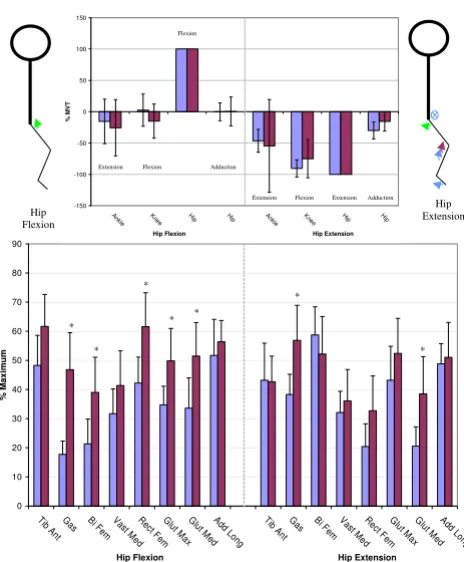
Hip flexion/extension
Figure 5 illustrates the secondary torques generated during hip flexion, where it can be seen that neither group gener-ated significant secondary torques. However the stroke group produced greater activity in the gastrocnemius, biceps femoris, rectus femoris, gluteus maximus, and glu-teus medius muscles. During hip extension MVT, both groups produced a secondary knee flexion torque and the control group produced additional ankle extension and
hip adduction secondary torques that were not signifi-cantly different from the stroke. The EMG pattern in figure 5 shows that the stroke group had greater gastrocnemius and gluteus medius activity during hip extension MVT.
Hip abduction/adduction
During hip abduction, the control group produced a hip extension secondary torque while the stroke group pro-duced a hip flexion secondary torque, the difference being significantly different (Figure 6). During hip abduction MVT, the stroke subjects had significantly greater gastroc-Secondary Torques During Hip Flexion/Extension
Figure 5
Secondary Torques During Hip Flexion/Extension.
The top graphs show the secondary joint torques for the stroke (red) and control (blue) groups expressed in %MVT for hip flexion (left) and hip extension (right). The stick fig-ures show the primary joint direction (green) as well as the secondary torques of the control (blue) and stroke (red) for the secondary joint torques that are significantly greater than zero. Abduction is denoted as a circled dot (out of the page), adduction is denoted a circled X (into the page). The bottom graph shows the EMG activity for the stroke (red) and con-trol (blue) groups expressed in % maximum value during hip flexion MVT (left) and hip extension MVT (right). Error bars represent 95% confidence interval. Significant differences between groups (p < 0.05) are denoted *. Tib Ant – tibilias anterior, Gas – gastrocnemius, Bi Fem – biceps femoris, Vast Med – vastus medialis, Rect Fem – rectus femoris, Glut Max -gluteus maximus, Glut Med – -gluteus medius, Add Long – adductor longus. Hip Extension Hip Flexion 0 10 20 30 40 50 60 70 80 90
Tib An t G
as Ham Str Va st Med R ect Fe m Gl ut M ax G lut M ed A dd Long Ti b An t Ga
s Ham Str
V ast Me
d R ect Fe m G lut M ax Gl ut M ed Add Lon g
Hip Flexion Hip Extension
% Max imum * * * * * * * Ti b A nt Ga
s Bi F em
Va st M
ed Rec t F em Gl ut M ax Gl ut M ed
Add L ong
Ti b A
nt Ga
s Bi F em
Va st M
ed Rec t F em Gl ut Ma x Glu t Me d Ad d L ong -150 -100 -50 0 50 100 150 Ankl e Kn
ee Hip Hi p Ankle
Kn
ee Hip Hip
Hip Flexion Hip Extension
% M
V
T
Extension Flexion Extension Adduction Flexion
Extension Flexion Adduction
Secondary Torques During Knee Flexion/Extension Figure 4
Secondary Torques During Knee Flexion/Extension.
The top graphs show the secondary joint torques for the stroke (red) and control (blue) groups expressed in %MVT for knee flexion (left) and knee extension (right). The stick figures show the primary joint direction (green) as well as the secondary torques of the control (blue) and stroke (red) for the secondary joint torques that are significantly greater than zero. Abduction is denoted as a circled dot (out of the page), adduction is denoted a circled X (into the page). The bottom graph shows the EMG activity for the stroke (red) and con-trol (blue) groups expressed in % maximum value during knee flexion MVT (left) and knee extension MVT (right). Error bars represent 95% confidence interval. Significant dif-ferences between groups (p < 0.05) are denoted *. Tib Ant – tibilias anterior, Gas – gastrocnemius, Bi Fem – biceps femo-ris, Vast Med – vastus medialis, Rect Fem – rectus femofemo-ris, Glut Max -gluteus maximus, Glut Med – gluteus medius, Add Long – adductor longus.
0 10 20 30 40 50 60 70 80 90
Tib An t G
as Ham Str Va st M ed R ect Fe
m Gl ut M ax G lut M ed A dd Long Ti b An t Ga
s Ham Str
V ast Me
d R
ect Fe m G lut M ax Gl ut M ed Add Lon g
Knee Flexion Knee Extension
% Max imum * * * * Knee Flexion Knee Extension Ti b A nt Ga
s Bi F em
Va st M
ed Rec t F em Gl ut M ax Gl ut M ed
Add L ong
Ti b A
nt Ga
s Bi F em
Va st M
ed Rec
t Fem Gl ut Ma x Glu t Me d Ad d L ong -150 -100 -50 0 50 100 150 200 250 300 350 An
kle Knee Hip Hip An kle Knee
Hip Hip
Knee Flexion Knee Extension
% M
V
T
Extension Flexion Extension Adduction
nemius and biceps femoris activity than the control sub-jects. For hip adduction MVT, none of the secondary torques were significantly different. The EMG pattern on the right side of figure 6 illustrates how the stroke group had greater gastrocnemius, vastus medialis, rectus femo-ris, gluteus maximus, and gluteus medius activity than the control subjects during hip adduction MVT.
Summary of secondary torques
For each group the secondary torques significantly greater than zero for the eight primary joint directions (figures 3
through 6) are summarized in Table 2. For each primary joint direction listed on the left, the secondary torques sig-nificantly greater than zero are marked with an 'X'. Addi-tionally, significant correlations (p < 0.05) between joint torques within each group are marked with an 'O'. To find these correlations all instances (primary or secondary) of a torque were pooled and compared to the other three joint torques. For example, all trials where ankle flexion was present were pooled and ankle flexion was compared to knee flexion/extension, hip flexion/extension, and hip abduction/adduction. The arrangement of rows and col-umns in Table 2 leads to the grouping of the primary joint directions into synergies. These synergies are based on the direction of the moment arm of the joint torque in the sagittal plane. Ankle flexion, knee extension, and hip flex-ion secondary torques are grouped as the Anterior Synergy while ankle extension, knee flexion, and hip extension are grouped as the Posterior Synergy. The frontal plane joint torques of hip abduction and adduction are differently grouped. Hip adduction is part of the posterior synergy in the control group but not part of any synergy in the stroke group. Hip abduction is part of the anterior synergy in the stroke group but part of the posterior synergy in the con-trol group.
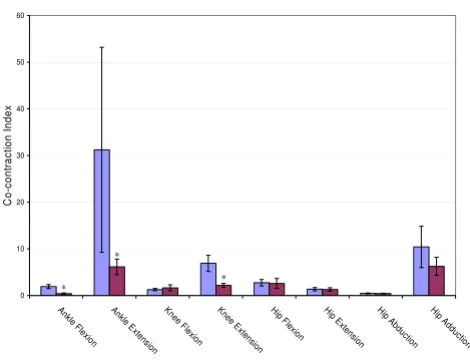
Co-contraction index
Figure 7 shows the co-contraction index for the eight pri-mary torque directions. The stroke group produced a sig-nificantly lower index, and thus greater co-contraction of antagonistic muscle groups during ankle flexion, ankle extension and knee extension. This was especially true during ankle extension where the stroke subjects exerted significantly higher tibialis anterior activity than the con-trol subjects.
Discussion
Primary joint torques
As expected, stroke subjects were weaker than age-matched controls for ankle flexion and extension, hip extension, abduction and adduction, and knee flexion. Surprisingly there were no significant differences in hip flexion and knee extension. Even more surprising was that the stroke subjects were, on average, stronger than the control group in knee extension. Median analysis con-firms that this is not just the result of a few exceptional stroke subjects. The median stroke knee extension torque was 90.60 Nm while the median control knee extension torque was 81.01 Nm. A closer inspection of the stroke subjects that generated large knee extension or hip flexion torques reveals that these stroke subjects were only stronger in one joint direction, and often generated below average MVT in the other joint directions tested. It is not unreasonable for an ambulatory, active stroke subject to use knee extension as part of a compensatory strategy, and Secondary Torques During Hip Abduction/Adduction
Figure 6
Secondary Torques During Hip Abduction/Adduc-tion. The top graphs show the secondary joint torques for the stroke (red) and control (blue) groups expressed in %MVT for hip abduction (left) and hip adduction (right). The stick figures show the primary joint direction (green) as well as the secondary torques of the control (blue) and stroke (red) for the secondary joint torques that are significantly greater than zero. Abduction is denoted as a circled dot (out of the page), adduction is denoted a circled X (into the page). The bottom graph shows the EMG activity for the stroke (red) and control (blue) groups expressed in % maximum value during hip abduction MVT (left) and hip adduction MVT (right). Error bars represent 95% confidence interval. Signifi-cant differences between groups (p < 0.05) are denoted *. Tib Ant – tibilias anterior, Gas – gastrocnemius, Bi Fem – biceps femoris, Vast Med – vastus medialis, Rect Fem – rec-tus femoris, Glut Max -gluteus maximus, Glut Med – gluteus medius, Add Long – adductor longus.
Hip Abduction
Hip Adduction
0 10 20 30 40 50 60 70 80 90
Tib An
t Ga
s Ham S
tr V
ast M ed
Rect Fem
G lut
M ax
Gl ut
M ed
Add Lon
g Ti
b A nt
Ga s Ham
S tr
Va st M
ed Rect
F em
G lut
M ax
Gl ut
Me d
Add L on
g
Hip Abduction Hip Adduction
% M
a
ximum
* *
*
* *
* *
Ti b A
nt Ga
s Bi Fe m
Va st M
ed Rec
t Fe m
Gl ut M
ax Gl
ut M ed
Add L ong
Tib An
t Ga
s Bi FemVast M ed
Rec t F
em Glu
t Ma x Gl
ut M ed
Ad d L
ong
-150 -100 -50 0 50 100 150
An
kle Knee Hip Hip An
kle Knee Hip Hip
Hip Abduction Hip Adduction
% M
V
T
Extension Flexion Extension Adduction Flexion Extension Flexion Abduction
over time, have it be as strong, or stronger, than an age-matched control.
Other factors influencing MVT, such as age, sex, or time post stroke were checked, but no significant correlation
was found. However such conclusions are somewhat lim-ited due to our sample size.
Secondary joint torque patterns
Abnormal coordination patterns in the upper limbs of hemiparetic stroke subjects have been quantified as the generation of torque in joints secondary to the primary joint axis [22]. When this analysis of secondary joint tor-ques was applied to the lower limbs of cerebral palsy sub-jects, abnormal secondary torques were produced at the hip and knee [23] which were consistent with the classi-cally defined extension synergy [15,16,30]. Presented here is evidence that such classically defined extension and flexion synergy patterns are not present in the lower limbs of chronic stroke subjects while in a functionally relevant standing, weight bearing position.
Torque patterns of healthy subjects
When asked to generate MVTs along the hip, knee, and ankle flexion and extension axes, the healthy control sub-jects produced secondary torques in the directions that were consistent with both the mechanical demands of the task and the physical properties of the musculature of the legs. For instance, when asked to generate a maximum knee extension torque, healthy subjects produced second-ary hip and ankle flexion torques. So the presence of pos-itive secondary torques of hip and ankle flexion are consistent with mechanical demands of the task. Not sur-prisingly healthy subjects had a high level of rectus
femo-Table 2: Secondary Torque Synergies
Control Ankle
Flexion
Knee Extension
Hip Flexion Hip
Abduction
Hip Adduction
Ankle Extension
Knee Flexion
Hip Extension
Primary Torque
Ankle Flexion X X
Knee Extension X O X O X
Hip Flexion O
Hip Abduction X O X O
Hip Adduction X O X O O
Ankle Extension X
Knee Flexion X O X O X O
Hip Extension X O X O X O
Stroke
Ankle Flexion X O X O
Knee Extension X O X O X
Hip Flexion O O
Hip Abduction O O X O
Hip Adduction
Ankle Extension X
Knee Flexion X O O
Hip Extension O X O
Anterior Synergy Posterior Synergy
Co-contraction Index Figure 7
Co-contraction Index. Cocontraction index for the eight
primary joint torques. Larger values represent lower levels of cocontraction. Error bars represent 95% confidence interval. Significant differences between groups (p < 0.05) are denoted *.
0 10 20 30 40 50 60
Ank le F
lexion Ankl
e E xtens
ion Knee
F lexi
on Kne
e E xt
en sion
Hip F lexi
on Hip
E xt
ens ion
Hip Ab
du ctio
n Hip
Ad du
ctio n
C
o
-c
ont
ra
ct
ion I
nde
x
* *
ris activity during knee extension MVT. The rectus femoris is known as both a knee extensor and hip flexor so the generation of secondary hip flexion during knee extension is consistent with the physical properties of the leg muscu-lature. This led to the grouping of the sagittal plane tor-ques into two synergies. The posterior synergy consisted of hip extension, knee flexion, and ankle extension while the anterior synergy consisted of hip flexion, knee exten-sion, and ankle flexion.
When asked to generate MVTs in the frontal plane joint directions of hip abduction and adduction, healthy sub-jects produced secondary torques that were not necessarily consistent with the physical properties of the musculature of the legs. The adductor longus is known as a hip flexor as well as adductor, but during high levels of adductor longus activity there was no production of significant hip flexion torque. However, the lower fibers of the gluteus maximus are known to adduct the hip [31] and during high gluteus maximus activity, there were significant sec-ondary hip adduction torques. To further classify the torque patterns of healthy subjects in the frontal plane (joint exertions of hip abduction and adduction) a sum-mary chart of significant secondary torques and correlated joint moments was constructed. Table 2 shows that hip adduction torque was correlated to knee flexion torque (marked 'O'), whereas hip adduction secondary torques were present during knee flexion and hip extension MVTs (marked 'X'). This led to classifying hip adduction as part of the posterior synergy. Even though hip abduction sec-ondary torques were produced during a MVT of an ante-rior synergy component (knee extension) it has been classified as part of the posterior synergy because hip abduction torque was correlated to knee flexion and hip extension. The presence of hip abduction secondary tor-ques during ankle extension MVT further justifies the pos-terior synergy classification.
Torque patterns of chronic stroke subjects
During MVTs in the sagittal plane, chronic stroke subjects showed no evidence of the classic extensor and flexor syn-ergies and behaved similarly to the healthy subjects. The torque patterns of the chronic stroke subjects differed from the healthy subjects only during hip abduction MVT. While healthy subjects produced significant hip extension torques, chronic stroke subjects produced significant hip flexion torque. This abnormal coupling of hip abduction and hip flexion is consistent with the classically defined flexion synergy.
A closer investigation into the secondary torque patterns generated during knee extension revealed that secondary torques were sometimes larger than the torques generated voluntarily. While we cannot conclude this origin for cer-tain, we postulate that a strategy used to generate a MVT
may unknowingly involve certain levels of co-contraction that would reduce the net torque. That is, it could be that the agonist muscles may be more active and the antago-nistic muscles more relaxed during a strategy used to gen-erate a MVT about a different joint. This would result in a net secondary torque that is larger than a net primary torque. This is not too unusual in the case of chronic stroke subjects generating secondary ankle flexion moments twice as large as their voluntary maximums. The majority of the stroke subjects had poor control at their ankle and often struggled to produce substantial ankle flexion torque. However while concentrating on knee extension exertions, any small increase in a synergistic ankle flexion exertions would be a rather large percentage. The slight increase in tibilias anterior activity from 35.32 % maximum during ankle flexion MVT to 38.78% maxi-mum during knee extension MVT further supports this. Unfortunately this phenomena gets a little more unusual when the levels of co-contraction are compared. A recalcu-lation of ankle co-contraction index during knee exten-sion MVT generation shows that there is a similar amount of co-contraction about the ankle during both voluntary ankle flexion (0.393 +/- 0.279 stdv) and voluntary knee extension (0.396 +/- 0.378 stdv), although recordings of the superficial leg muscles were made. It is likely that had more muscles been recorded from (e.g. soleus) a better understanding for the observed behavior could be explained.
The interesting finding that in control subjects, hip flexion secondary torques were greater than 100% MVT might be explained by the activity of the rectus femoris. During hip flexion MVT control subjects seamed to rely on moderate levels of both rectus femoris (42% maximum) and adduc-tor longus (52% maximum) to achieve hip flexion adduc- tor-ques. But during knee extension MVT the rectus femoris activity of the control subjects was higher (54% maxi-mum). A recalculation of hip co-contraction index during knee extension MVT shows that there is less co-contrac-tion about the hip during voluntary knee extension (3.58 1.39 stdv) than during voluntary hip flexion (2.73 +/-0.68 stdv). However these findings are not significantly different and had more muscles been recorded from a bet-ter understanding for the observed behavior could be explained.
Weakness in chronic stroke
chronic stroke subjects produced significantly more co-contraction during ankle flexion and ankle extension which may partially explain the joint torque deficits in those directions. But the stroke subjects produced signifi-cantly more co-contraction during knee extension even though they produced a similar level of torque. While inadequate recruitment of motorneuron pools can not be ruled out, it does appear that the co-contraction of antag-onistic muscle groups may at least contribute to the observed weakness in the chronic stroke subjects tested. This is consistent with our previous work that demon-strated significant co-activation of antagonistic muscle groups in acute stroke subjects [27].
Conclusion
Presented here for the first time is a quantitative analysis of lower limb weakness and synergy patterns of chronic stroke subjects in a functionally relevant standing weight-bearing position. In a standing position with added ves-tibular inputs, stroke subjects showed little evidence of the classic abnormal synergy patterns in seven of the eight directions tested. The findings here suggest that the pri-mary contributor to lower limb motor deficits in chronic stroke subjects is weakness, which is at least partially due to co-contraction of antagonistic muscles.
Declaration of competing interests
The author(s) declare that they have no competing inter-ests.
Authors' contributions
NN carried out the experiments, collected and analyzed the data, and drafted the manuscript. MP prepared jects and assisted with the experiments. DN prepared sub-jects and assisted with the experiments. JH designed the experiment, developed data collection software, and helped draft the manuscript. All authors read, edited, and approved the final manuscript.
Acknowledgements
We would like to extend our sincere thanks to the subjects who partici-pated in the study. This work was funded by the Whitaker Foundation (Arlington, VA; PI: J. Hidler).
References
1. Bourbonnais D, Vanden Noven S: Weakness in patients with hemiparesis. Am J Occup Ther 1989, 43(5):313-9.
2. Duncan PW, Badke MB: Stroke Rehabilitation: The Recovery of Motor Control Chicago, Year Book Medical Pub; 1987.
3. Scelsi R, Lotta S, Lommi G, Poggi P, Marchetti C: Hemiplegic atro-phy. Morphological findings in the anterior tibial muscle of patients with cerebral vascular accidents. Acta Neuropathol
1984, 62(4):324-31.
4. McComas AJ, Sica RE, Upton AR, Aguilera N: Functional changes in motoneurones of hemiparetic patients. J Neurol Neurosurg Psychiatry 1973, 36(2):183-93.
5. Newham DJ, Hsiao SF: Knee muscle isometric strength, volun-tary activation and antagonist co-contraction in the first six months after stroke. Disability and Rehabilitation 2001, 23:379-386.
6. Tang A, Rymer WZ: Abnormal force-EMG relations in paretic limbs of hemiparetic human subjects. J Neurol Neurosurg Psychi-atry 1981, 44(8):690-8.
7. Chae J, Yu DT: Neuromuscular electrical stimulation for motor restoration in hemiparesis. Top Stroke Rehabil 2002, 8(4):24-39. Winter
8. Knuttson E, Richards C: Different types of disturbed motor con-trol in gait of hemiparetic patients. Brain 1979, 102:405-430. 9. Knutsson E, Martensson A: Dynamic motor capacity in spastic
paresis and its relation to prime mover dysfunction, spastic reflexes and antagonist co-activation. Scand J Rehabil Med 1980, 12(3):93-106.
10. Bobath B: Adult Hemiplegia: Evaluation and Treatment London, William Heinnemann; 1978.
11. Corcos DM, Gottlieb GL, Penn RD, Myklebust B, Agarwal GC: Movement deficits caused by hyperexcitable stretch reflexes in spastic humans. Brain 1986, 109(Pt 5):1043-58.
12. Dietz V, Quintern J, Berger W: Electrophysiological studies of gait in spasticity and rigidity. Evidence that altered mechan-ical properties of muscle contribute to hypertonia. Brain
1981, 104(3):431-49.
13. Yelnik A, Albert T, Bonan I, Laffont I: A clinical guide to assess the role of lower limb extensor overactivity in hemiplegic gait disorders. Stroke 1999, 30(3):580-5.
14. Brunnstrom S: Movement Therapy in Hemiplegia New York, Harper and Row; 1970.
15. Twitchell TE: restoration of motor function following hemiple-gia in man. Brain 1951, 74(4):443-80.
16. Brunnstrom S: Associated reactions of the upper extremity in adult patients with hemiplegia; an approach to training. Phys Ther Rev 1956, 36(4):225-36.
17. Waters RL, Frazier J, Garland DE, Jordan C, Perry J: Electromyo-graphic gait analysis before and after operative treatment for hemiplegic equinus and equinovarus deformity. J Bone Joint Surg Am 1982, 64(2):284-8.
18. Michels E: Synergies in hemiplegia. Clin Manag 1982, 1:9-16. 19. Sawner K, LaVigne J: Brunnstrom's movement therapy in hemiplegia : a
neurological approach 2nd edition. Philadelphia, JB Lippincott;
1992:276.
20. Dewald JP, Pope PS, Given JD, Buchanan TS, Rymer WZ: Abnormal muscle coactivation patterns during isometric torque gener-ation at the elbow and shoulder in hemiparetic subjects.
Brain 1995, 118(Pt 2):495-510.
21. Beer RF, Given JD, Dewald JP: Task-dependent weakness at the elbow in patients with hemiparesis. Arch Phys Med Rehabil 1999, 80(7):766-72.
22. Dewald JP, Beer RF: Abnormal joint torque patterns in the paretic upper limb of subjects with hemiparesis. Muscle Nerve
2001, 24(2):273-83.
23. Thelen DD, Riewald SA, Asakawa DS, Sanger TD, Delp SL: Abnor-mal coupling of knee and hip moments during maxiAbnor-mal exer-tions in persons with cerebral palsy. Muscle Nerve 2003, 27(4):486-93.
24. Young LR: Perception of the body in space: mechanisms. In
Handbook of Physiology, Sect 1 Volume 3. Issue Pt 2 Edited by:
Brookhart JM, Mountcastle VB, Darian-Smith. Bethesda: American Physiological Society; 1984:1023-66.
25. McMahon TA: Muscles, reflexes, and locomotion Princeton, Princeton University Press; 1984.
26. Davis BL, Cavanagh PR: Simulating reduced gravity: a review of biomechanical issues pertaining to human locomotion [Review]. Aviat Space Environ Med 1993, 64(6):557-66.
27. Hidler J, Carroll M, Federovich E, Lacsamana C: Loss of differential muscle control leads to weakness and discoordination in individuals with acute hemiparetic stroke. IEEE Engineering in Medicine and Biology Society, Cancun, Mexico; 2003.
28. Craig JJ: An Introduction to Robotics: Mechanics and Control 1989. 29. Friederich JA, Brand RA: Muscle fiber architecture in the human
lower limb. J Biomech 1990, 23(1):91-5.
30. Sutherland DH, Davids JR: Common gait abnormalities of the knee in cerebral palsy. Clin Orthop Relat Res 1993:139-47. 31. Hollinshead WH, Rosse C: Textbook of Anatomy 4th edition.