A COMPARATIVE STUDY TO PROVE THE EFFECTIVENESS OF
TYLER TWIST EXERCISE WITH DIAMOND TAPING TO IMPROVE
WRIST EXTENSOR MUSCLE STRENGTH AND DECREASE PAIN IN
LATERAL EPICONDYLITIS
Reg. No. 271410225
MADHA COLLEGE OF PHYSIOTHERAPY
(AFFILIATED TO THE TAMIL NADU DR. M.G.R MEDICAL UNIVERSITY) GUINDY, CHENNAI, TAMIL NADU – 600 032
A COMPARATIVE STUDY TO PROVE THE EFFECTIVENESS OF
TYLER TWIST EXERCISE WITH DIAMOND TAPING TO IMPROVE
WRIST EXTENSOR MUSCLE STRENGTH AND DECREASE PAIN IN
LATERAL EPICONDYLITIS
ADVISOR
Prof. S. Mercy Clara, MPT. (Ortho),
Professor,
Madha College of Physiotherapy, Kundrathur,
Chennai – 600 069.
EXAMINERS
1.
2.
A Dissertation submitted to The Tamil Nadu Dr. MGR Medical University in partial fulfilment of the requirements for the award of the degree of
MASTER OF PHYSIOTHERAPY
CERTIFICATE
This is to certify that the project title “A comparative study to prove the effectiveness of Tyler twist exercise with diamond taping to improve wrist extensor muscle strength and decrease pain in lateral epicondylitis” is a bonafide record done under my guidance supervision in the partial fulfilment for the degree ofMASTER OF PHYSIOTHERAPY (MPT II YEAR APRIL- 2016) by Mrs. S. SUGANYA (Register Number: 271410225)
Post Graduate Student of Madha College of Physiotherapy.
GUIDE: PRINCIPAL
Prof. S. MERCY CLARA, MPT. (Ortho) Prof. V. VIJAI KRISHNA, MPT., MIAP
ACKNOWLEDGEMENT
I express my gratitude to MY GOD ALMIGHTY for his abundant grace and mercy that has made me success in my life.
I would like to dedicate this project to my beloved parents.
I express my heartfelt thanks to my dear father, mother, brother and husband, for their astounding support sacrifice and prayers that has enabled me to spell success in life.
I am grateful to the chairman and management of the Madha Educational Trust for providing me an opportunity to do my Post-Graduate study.
I very sincerely thank our beloved Principal Prof. V. VIJAI KRISHNA, MPT. (Cardio) MIAP for his support and valuable suggestions.
I wish to thank my guide Prof. S. MERCY CLARA, MPT. (Ortho) for her support and valuable knowledge for completing my work.
I also wish to thank Prof. S. NAGARAJ, MPT. (Cardio) MIAP, PG CDE.V.P,. for his ideas and support.
I also wish to thank my dear friends for their ideas and support in completing this work.
TABLE OF CONTENTS
CHAPTER
TITLE
PAGE NOS.
1 INTRODUCTION
1-5
2 REVIEW OF LITERATURE
6-9
3 DESIGN AND METHODOLOGY
10-19
4 DATA ANALYSIS
20-30
5 RESULTS AND DISCUSSION
31-34
6 LIMITATIONS ANDSCOPE FOR FURTHER STUDY
35
7 CONCLUSION
36
LIST OF TABLES
TABLE
NO.
TITLE
PAGE NO.
4.1
COMPARISON OF PRE TEST AND POST TEST VALUES OF NPRS, GRIP STRENGTH AND DASH IN GROUP A
21
4.2
COMPARISON OF PRE TEST AND POST TEST VALUES OF NPRS, GRIP STRENGTH AND DASH IN GROUP B
22
4.3 PAIRED T-TEST ANALYSIS OF GROUP A AND B 23
4.4 COMPARISON OF POST TEST SCORES OF NPRS IN
GROUP A AND GROUP B
25
4.5 COMPARISON OF POST TEST SCORES OF NPRS IN
GROUP A AND GROUP B
27
4.6 COMPARISON OF POST TEST SCORES OF DASH IN
GROUP A AND GROUP B
LIST OF FIGURES
FIGURE NO. TITLE PAGE NO.
Figure 1 APPLICATION OF DIAMOND TAPE 1 16
Figure 2 APPLICATION OF DIAMOND TAPE 2 17
Figure 3 TYLER TWIST EXERCISE 1 18
Figure 4 TYLER TWIST EXERCISE 2 19
Graph 1 COMPARISON OF PRE AND POST TEST FOR NPRS 26 Graph 2 COMPARISON OF PRE AND POST TEST FOR GRIP
STRENGTH
28
[image:7.595.59.537.116.366.2]1
INTRODUCTION
Upper limb plays an important role in everyone‟s daily life and hand is the effector organ of the upper limb, which supports it mechanically and allows it to adopt the optional position for any given action from the functional point of view1. Among the upper limb conditions, tennis elbow is one of the most significantly occurred condition2. According to Ebenezer, a painful elbow syndrome comprises lateral, medial and posterior elbow symptoms; among them the one significantly noticed is the lateral tennis elbow which results from repetitive stress3
It is generally a work-related or sport-related pain disorder usually caused by excessive quick, monotonous, repetitive eccentric contractions and gripping activities of the wrist4.
Tennis elbow affects 1% to 3% of the adult population 4 and only 5% of people related to tennis suffer from tennis elbow6. It is a misnomer, often seen in non tennis players5, although elbow pain is found in up to 50% of tennis players, where tennis elbow is encountered in 75–80% of cases and the incidence in general practice is 4–7 per 1000 per year, with 15% of workers involved in highly repetitive jobs reporting the condition6.
Several intervention for the management of lateral epicondylitis have been described, including Corticosteroid injection, NSAIDs, Muscle stretching and Strengthening exercise, Sports Taping techniques, Cryotherapy, use of orthotic device, Manipulative technique(Mulligan‟s MWM), Acupuncture, Ultrasound, LASER, TENS, ESWT, Electromagnetic field and Ionization. Although conservative treatment of this condition has been the subject of numerous studies, there is no agreement as to the most effective management strategy.
Eccentric exercises have been utilized successfully in chronic painful tendinosis like Achilles, supraspinatus and patellar tendinosis7. Since the different types of tendinosis show similarities in clinical behaviour and in their histological appearance, eccentric training may help in giving pain relief and functional improvements in patients with tennis elbow8.
2
equipment used for strengthening. Once the patient learned this simple exercise, they could easily perform this exercise at home independently without direct supervision or regular physiotherapy visits. Thus it helps to maintain the muscle performance and reduce the risk of re-injury and enhance the functional activities9.
It is proposed that the application of tape is a means, aims to alleviate pain, improve muscle function, and restore functional movements. Taping facilitates the compliance to exercise rehabilitation programs by minimizing the aggravation of symptoms during performance of therapeutic exercise 10.
3
AIM OF THE STUDY
The aim of the study is to prove the improvement in grip strength and pain reduction with the combination treatment of Tyler twist exercise and diamond tapping in Tennis elbow.
NEED OF THE STUDY:
There are articles, which support Diamond taping for pain free grip strength and indicates that it may be an useful adjunct in the management of tennis elbow. Recent articles state that the patients who used the Thera-Band flex bar has significant effect in reducing pain, improving grip strength and enhanced functional status, in patients with lateral epicondylitis.
But there is lack of experimental data regarding the comparative effects of Tyler twist exercise and Diamond taping in patients with lateral epicondylitis. Hence, here a need was identified to compare the effectiveness with diamond taping in patients with lateral epicondylitis. Hence there is a need to compare both and provide an effective and inexpensive treatment for tennis elbow.
OBJECTIVE OF THE STUDY
1. To find out effectiveness of Tyler Twist exercise alone in reducing pain and improving grip strength and hand function, in-patients with tennis elbow.
2. To find out the effectiveness of Tyler twist exercise along with diamond taping in reducing pain and improving grip strength and hand function in patients with tennis elbow.
4
OPERATIONAL DEFINITIONS
Tennis elbow:
Tennis elbow or lateral epicondylitis is a clinical condition characterized by pain and tenderness over the lateral side of elbow, difficulties in functional activities and with positive Mill‟s test, Cozen test or resisted middle finger extension test when examined clinically.
Taping
:Taping is a therapeutic procedure, performed by using tape, attached to the skin, to physically keep the muscles in place or joints in certain position, aims to reduce pain, enhance recovery, prevent overuse and further injury.
Grip strength:
Grip strength is the force applied by the hand to pull on or suspend from objects and is a specific part of hand strength. Optimum sized objects permit the hand to wrap around a cylindrical diameter from one to three inches.
Eccentric exercise:
An exercise in which there is overall lengthening of the muscle in response to external resistance.
Thera-Band Flexbar
5
HYPOTHESIS:
(i) Null Hypothesis:
There will be no significant difference with the combination treatment of Tyler twist exercise with diamond tapping for Tennis elbow.
(ii) Alternative Hypothesis:
6
REVIEW OF LITERATURE
1.
Mani L. Gerr F. (2000):
Pain at the wrist extensor muscles at (or) near their lateral epicondyle origin (or) pain directly over the lateral epicondyle is termed as lateral epicondylitis12.
2.
Magee D, Nischl R. et al (2008):
Lateral epicondylitis is a chronic overuse injury causing damage to the extensor muscles tendons of the forearm. The tendon which is most commonly involved are the extensor carpi radialis brevis, extensor digitorum and extensor carpi radialis longus13.
3.
Norris C (1998):
Many individuals may experience pain at the head of the radius during pronation which is due to irritation of the underlying bursa14.
4.
Bisset L et al (2009):
There is an annual incidence of 4-7 cases per 1000 patients in general practice and 1-3% within general population. It is a common condition that significantly impacts on the individual and society. It occurs primarily between the ages of 35 and 54 and typically affects the dominant arm in men and women, alike in activities15.
5.
Alam (2008):
7
6.
Zeisig (2008):
Microtrauma can occur due to fatigue after repetitive loads and can even occur if the loads are within the strength limits. Puranik (2009) stated that the possible etiologies are inflammation of the radial humeral bursa, synovium, periosteum and the annular ligament16.
7.
Hutson (2001):
In case of tennis players overload relates to the shake frequency, incorrect technique, particularly on the backhand and muscle imbalance or loss of flexibility17.
8.
Tyler T F et al(2010):
Assessed the efficacy of a novel eccentric wrist extensor exercise added to standard treatment for chronic lateral epicondylosis or tennis elbow. All outcome measures for this condition were markedly improved with the addition of an eccentric wrist extensor exercise to standard physical therapy. This novel exercise, using an inexpensive rubber bar, provides a practical means of adding isolated eccentric training to the treatment of chronic lateral epicondylosis9.
9.
Phil Page(2010)
Developed a novel exercise and has shown promise with patients with lateral epicondylitis. In his prospective, randomized, Quasi-control study. 22LE patients were assigned to either a standard physical therapy treatment group or a group that received standard PT with addition of novel flex bar exercise. He concluded that, this clinical suggestion demonstrated an excellent example of true “evidence-based practice” in physical therapy18.
10.
Gretchen Reynolds (2009) and Crystal Phend (2009):
8 .11 Bill Vicenzino et al(2003):
Did a study, on initial effects of elbow taping on pain-free grip strength and pressure pain threshold and found effectiveness of diamond taping technique on pain free grip strength in individuals with chronic lateral epicondylitis10.
12 Jones (2009):
Taping is used in associate with exercise program by many physiotherapists in the purpose of restoring functional movement patterns by relieving pain2.
13.
Lillian Albert Zaky (2013)
This study also noted the immediate effect of Diamond taping on wrist extensor strength, and pain in patients with tennis elbow and has concluded that this method of treatment may be useful in the management of this condition during exercise and functional rehabilitation20.
14 Boonstra M(2008):
Did a study to determine the reliability and validity of the Visual Analogue Scale for disability in patients with chronic musculoskeletal pain and they concluded that reliability of the VAS for disability is moderate to good and a strong correlation with the VAS for pain21.
15. Bohannon RW(1988):
In his study, he measured the validity of hand-grip dynamometry for upper extremity strength impairment in home care patients and the findings support the construct validity of hand-grip dynamometry for characterizing upper extremity strength impairment22.
16. Takasaki et al (2007):
9 .
17.
Isam Atroshi et al (2000):
Did a study on 176 patients to determine the reliability and validity of DASH scale and concluded that DASH is a reliable and valid region – specific outcome measure. It should be a valuable test in clinical research of upper extremity musculoskeletal disorders and for clinicians managing patients with such disorders24.
10
DESIGN AND METHODOLOGY
STUDY DESIGN:
Randomized controlled clinical trial.
STUDY SET UP:
Madha Medical college and Hospital Prema Physiotherapy Clinic.
POPULATION:
All the well oriented and well co-operative lateral epicondylitis subjects who fulfilled the inclusion criteria were included in the study.
SAMPLE SIZE:
30 subjects from the population were selected through the lottery method and they weredivided into two groups (Each fifteen)
GROUP A Tyler twist exercise.
GROUP B Tyler twist exercise with Diamond taping.
INCLUSION CRITERIA
o Mill‟s test positive.
o Cozens test positive.
o Patients who had pain over the lateral epicondyle with one of the following test. a. Extensor carpi radialis test [i.e. resisted middle finger extension].
11
o Participant who don‟t involve in any other form of treatment during their involvement in the study.
o Patient reporting unilateral involvement.
o Patient who have pain more than six weeks.
EXCLUSION CRITERIA
o Allergies to adhesive tape.
o Any upper limb neurological abnormalities on physical examination (Ex: Cervical neuropathy)
o A concomitant upper limb orthopaedic condition or any concurrent treatment.
o Limitation in ROM in the involved hand.
VARIABLES OF THE STUDY
i.
INDEPENDENT VARIABLE
o Tyler twist exercise
o Diamond tapping.
ii.
DEPENDENT VARIABLE
o Pain
o Grip Strength
MEASUREMENT TOOLS
o Visual Analog Scale – Pain
o Subjective disability (DASH) – Questionnaire
o Hand held dynamometer (Wrist and finger strength)
DURATION OF THE STUDY
12
METHODOLOGY
MATERIALS USED
Thera Band Flex Bar
Mc Connell‟s Rigid tape
Sand Bags and Dumbbells‟
NPRS
Hand Held Dynamometer
DASH Questioner
Patients who fulfilled the inclusion criteria after an initial assessment and informed consent, were assigned in to two groups A and B, based on simple random sampling .Pre-test and Post–.Pre-test evaluation were done before and after treatment, which includes pain assessment using NPRS , grip strength using hand held dynamometer DASH questioner.
Group A
Group A subjects received Tyler twist exercise.
TYLER TWIST EXERCISE PROTOCOL (10 min)
The Tyler twist exercise is performed using a Thera –band Flex Bar which consist of different resistance.
Yellow takes 6 lb of force Red - 10 lb Green - 15 lb Blue - 25 lb
13
Each subject for the Tyler Twist protocol will be given 3 sets of 15 repetitions of eccentric strengthening provided with a Thera-band Flex Bar to perform the exercise.
The strengthening exercise will be performed in a seated or a standing position.
The elbow will be flexed at 900 and forearm will be neutral (mid prone).
Subject will hold one end of rubber bar in involved hand with maximum wrist extension and grasp the other end of rubber bar by non-involved hand.
Then twist the rubber bar by flexing the non-involved wrist while holding the involved wrist in extension.
Bring arms in front of the body with elbows in extension while maintaining the twist in rubber bar by holding with non-involved wrist in full flexion and involved wrist in full extension
Slowly allow rubber bar to untwist by allowing involved wrist to move in to flexion (i.e., eccentric contraction of the involved wrist extensors).
Each eccentric wrist extensor contraction lasted for 4 sec (i.e., slow reversal).
Both upper extremities reset for subsequent repetition.
Subjects in the Tyler Twist exercise group perform 3 sets of 15 repetitions, with 30 sec rest period between each set.
Intensity will be increase by giving the patient a thicker rubber bar if the patient reported no longer experiencing discomfort during the exercise.
3 sets of 15 repetitions will be given 5 times a week, for 4 weeks.
14 Group B
In addition to Tyler Twist exercise, Group B subjects received Diamond taping Diamond taping was followed by Tyler Twist exercise to allow proper pain free exercise program.
DIAMOND TAPING:
The elbow region (from lower end of humerus till mid-forearm) has to be shaved and the part should be dry. Now a skin toughner spray is sprayed on the skin to avoid the direct contact with the tape. The diamond taping technique consisted of 4 pieces of approximately 80-100mm long, 38mm wide, non-elastic, McConnel‟s tape. These were laid on skin distal to proximal in a diamond shape, applying a tractional force on soft tissues towards lateral epicondyle and perpendicular to line of the tape.
The strips overlapped at their ends and were secured with an additional 4 tape strips, giving the bulging tissue an orange peel appearance. The tape will be removed after 24 hrs of application.
TYLER TWIST EXERCISE PROTOCOL (10 min)
Each subject for the Tyler Twist protocol will be given 3 sets of 15 repetitions of eccentric strengthening provided with a Thera-band Flex Bar to perform the exercise.
The strengthening exercise will be performed in a seated or a standing position.
The elbow will be flexed at 900 and forearm will be neutral (mid-prone).
Subject will hold one end of rubber bar in involved hand with maximum wrist extension and grasp the other end of rubber bar by non-involved hand.
15
Bring arms in front of the body with elbows in extension while maintaining the twist in rubber bar by holding with non-involved wrist in full flexion and involved wrist in full extension.
Slowly allow rubber bar to untwist by allowing involved wrist to move in to flexion (i.e., eccentric contraction of the involved wrist extensors).
Each eccentric wrist extensor contraction lasted for 4 sec (i.e., slow reversal).
Both upper extremities reset for subsequent repetition.
Subjects in the Tyler Twist exercise group perform 3 sets of 15 repetitions, with 30 sec rest period between each set.
Intensity will be increase by giving the patient a thicker rubber bar if the patient reported no longer experiencing discomfort during the exercise.
16
17
18
19
TYLER TWIST EXERCISE 2
20
DATA ANALYSIS
Statistical analysis was done using SPSS version 17.00
STATISTICAL DATA ANALYSIS TECHNIQUE
In Group A, Group B all data was expressed as mean ± SD and was statistically analyzed using paired „t‟ test and independent „t‟ test to determine the statistical difference among the parameters at 0.5% level of significance by employing the statistical tools as given below
Mean ; Standard deviation SD =
Paired t-test =
Where, = mean difference; Sd = Standard deviation of difference
Independent t – test =
SE= s
Where, s = SE =
21
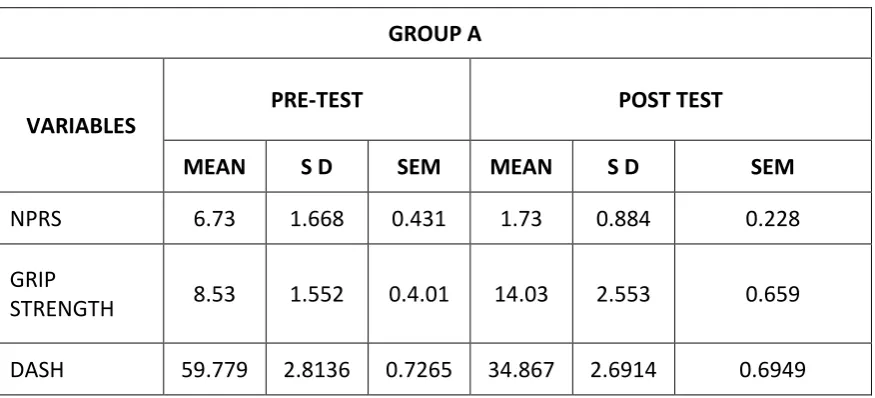
Table 4.1
COMPARISON OF PRE-TEST AND POST-TEST VALUES OF NPRS
DASH AND GRIP STRENGTH IN GROUP A
GROUP A
VARIABLES
PRE-TEST POST TEST
MEAN S D SEM MEAN S D SEM
NPRS 6.73 1.668 0.431 1.73 0.884 0.228
GRIP
STRENGTH 8.53 1.552 0.4.01 14.03 2.553 0.659
DASH 59.779 2.8136 0.7265 34.867 2.6914 0.6949
Table 4.1 shows descriptive measures of pre-test and post-test values of NPRS, grip strength and DASH in group A.
The mean value of NPRS in post-test is 1.73 with SD of 0.884 and SEM of 0.228, which is less than the mean value of pre-test 6.73 with a SD of 1.668 and SEM of 0.431.
The mean value of grip strength in post-test is 14.03 with SD of 2.553 and SEM of 0.659, which greater than the mean value of pre-test 8.53 with SD of 1.552 and SEM of 0.401.
22
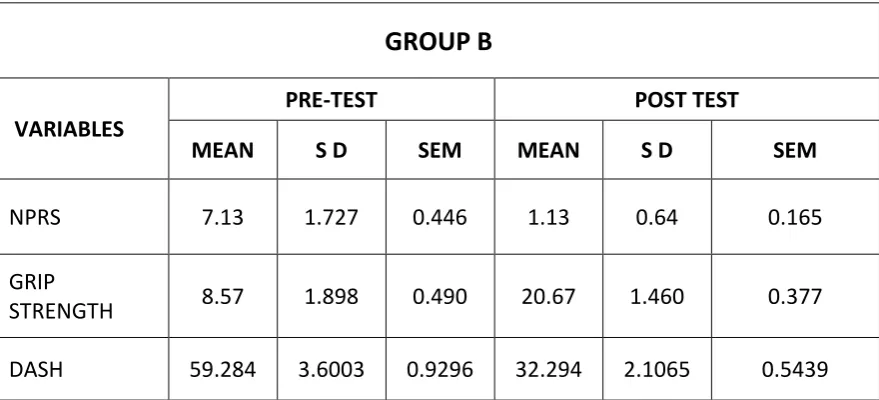
Table 4.2
COMPARISON OF PRE-TEST AND POST-TEST VALUES OF NPRS,
DASH, AND GRIP STRENGTH IN GROUP B.
GROUP B
VARIABLES
PRE-TEST POST TEST
MEAN S D SEM MEAN S D SEM
NPRS 7.13 1.727 0.446 1.13 0.64 0.165
GRIP
STRENGTH 8.57 1.898 0.490 20.67 1.460 0.377
DASH 59.284 3.6003 0.9296 32.294 2.1065 0.5439
Table 4.2 shows descriptive measures of pre-test and post-test values of NPRS, grip strength and DASH in group B.
The mean value of NPRS in post-test is 1.13 with SD of 0.640 and SEM of 0.165, which is less than the mean value of pre-test 7.13 with SD of 1.727 and SEM of 0.446.
The mean value of grip strength in post-test is 20.67 with SD of 1.460 and SEM of 0.377, which is greater than the mean value of pre-test 8.57 with SD of 1.898 and SEM of 0.490.
23
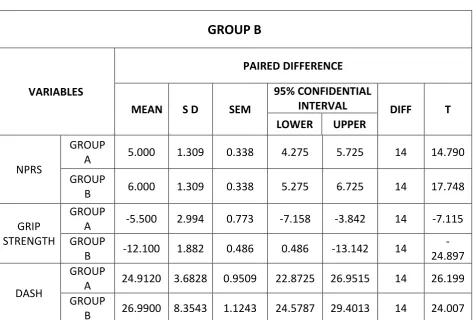
Table 4.3
PAIRED T-TEST ANALYSIS OF GROUP A AND GROUP B
GROUP B
VARIABLES
PAIRED DIFFERENCE
MEAN S D SEM
95% CONFIDENTIAL
INTERVAL DIFF T
LOWER UPPER
NPRS
GROUP
A 5.000 1.309 0.338 4.275 5.725 14 14.790
GROUP
B 6.000 1.309 0.338 5.275 6.725 14 17.748
GRIP STRENGTH
GROUP
A -5.500 2.994 0.773 -7.158 -3.842 14 -7.115 GROUP
B -12.100 1.882 0.486 0.486 -13.142 14
-24.897
DASH
GROUP
A 24.9120 3.6828 0.9509 22.8725 26.9515 14 26.199 GROUP
B 26.9900 8.3543 1.1243 24.5787 29.4013 14 24.007
The above table shows the statistical outcome of paired “T” test analysis of NPRS, grip strength, and DASH in group A and B.
The mean value of NPRS in group A is 5.000 with SD of 1.309 and SEM of 0.338, when compared to Group B, the mean value of group B is 6.000, which is increased, but the SD of 1.300 and SEM of 0.338 shows the same value as group A.
The change in 95% of confident interval in group A is 4.275 – 5.725 and group B is 5.275 – 6.725.
24
The change in 95% confident interval in group A is 7.158 3.842 and 0.486 to -13.142 in group B.
The mean of DASH in group A is 24.9120 with SD of 2.994, which is greater than group B with a mean value of 26.990 and SD 3.6828, but the SEM of group A is 0.9509 which is lesser than group B with SEM of 1.1243.
25
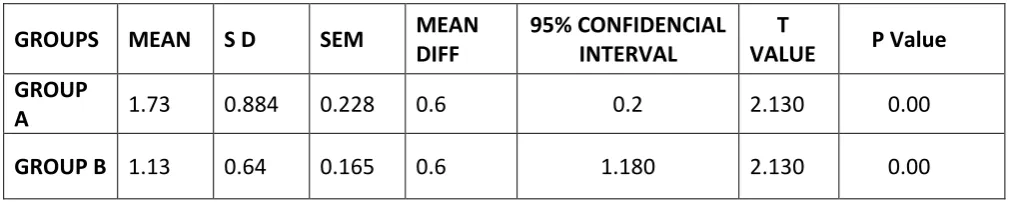
Table 4.4
COMPARISION OF POST SCORE OF NPRS OF GROUP A AND GROUP B
GROUPS MEAN S D SEM MEAN
DIFF
95% CONFIDENCIAL INTERVAL
T
VALUE P Value GROUP
A 1.73 0.884 0.228 0.6 0.2 2.130 0.00
GROUP B 1.13 0.64 0.165 0.6 1.180 2.130 0.00
The above table shows the statistical scores outcome measures of post-test scores of NRPS group A and group B.
The NRPS of group A has a mean value of 1.73 and group B has a mean value of 1.13 with mean difference of 0.600.
26
GRAPH 1
COMPARISION OF PRE AND POST TEST FOR NRPS
0 2 4 6 8 10
GROUP A GROUP B
M
E
A
N
±
SD
NPRS
27
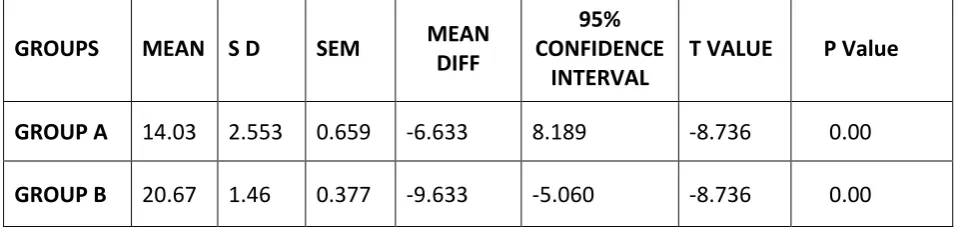
Table 4.5
COMPARISON OF POST SCORE OF GRIP STRENGHT IN
GROUP A AND B
The above table shows the statistical score outcome measures of post-test scores of grip strength of group A and group B.
The grip strength of group A has a mean value of 14.03 and group B has a mean value of 2.553 with a mean difference of -6.633.
The 95% of confident interval is 8.189 - -5.060 with a T-value of -8.736, which is statistically significant with P (<0.005).000..
GROUPS MEAN S D SEM MEAN
DIFF
95% CONFIDENCE
INTERVAL
T VALUE P Value
GROUP A 14.03 2.553 0.659 -6.633 8.189 -8.736 0.00
28
GRAPH 2
PRE AND POST TEST COMPARISION 0F GRIP STRENGTH
0 5 10 15 20 25
GROUP A GROUP B
M
E
A
N
±
SD
GRIP STRENGTH(Kg)
29
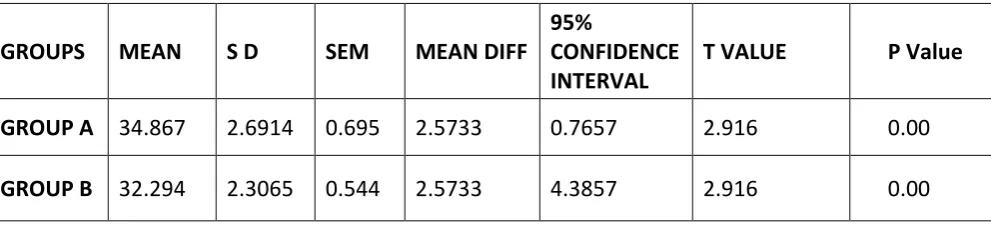
Table 4.6
COMPARISION OF POST TEST SCORES OF DASH OF GROUP A AND B
GROUPS MEAN S D SEM MEAN DIFF
95%
CONFIDENCE INTERVAL
T VALUE P Value
GROUP A 34.867 2.6914 0.695 2.5733 0.7657 2.916 0.00
GROUP B 32.294 2.3065 0.544 2.5733 4.3857 2.916 0.00
The above table shows the statistical score outcome measure of post-test scores of DASH of group A and B.
30
GRAPH 3
PRE AND POST TEST COMPARISION OF DASH
0 20 40 60 80
GROUP A GROUP B
M
E
A
N
±
SD
DASH
31
RESULT AND DISCUSSION
RESULTS:
The post test score of NPRS, Grip Strength and DASH shows, improvement in both the groups
The post scores in case of NPRS in both groups A and B show almost same state of improvement with a minimal difference.
The post test score of Grip Strength and DASH shows good improvement in Group B when compared to group A
Statistical supports also state that Tyler twist exercise with Diamond taping would be more beneficial when compared to Tyler twist alone.
32
DISCUSSION
Lateral epicondylitis is one of the conditions which can be treated by a wide variety of physiotherapy methods. It is still difficult to formulate all proof guidelines for the management of lateral epicondylitis. Various methods of treatment exist with own claims of success without any attempts of comparing the maximal effective methods. The objective of this study was to compare the effectiveness of Tyler twist exercise with diamond taping in the treatment of chronic lateral epicondylitis.
D' Stasinopoulos, in his study has mentioned that there are three forms of musculotendinous contractions (i) Isometric (ii) Concentric, and (III) Eccentric. Most therapists agree that the eccentric contractions appear to have the most beneficial effects for the treatments of LET. In case of LET, eccentric training should be performed for the extensor tendons of the wrist, including the ECRB tendon, which LET most commonly affects.
The three principles of eccentric exercises are (i) Load, (ii) Speed and (III) Frequency: Increase in load according to the patient‟s symptoms clearly subjects the tendons to greater stress and forms the bases for the progression of the program.
Increase in speed, thus increase the load of tendon to better stimulate the mechanism of injury23
.Phil Page, in his study, has mentioned that eccentric exercise effectively “lengthened” the muscle tendon complex resulting in structural remodelling of the tendon with hypotrophy and increased tensile strength of the tendon15.
Clinicians understanding the positive effects of eccentric exercise on tendinopathies used an existing clinical tool (the Flex Bar) to develop an “evidence – led” intervention that could be applied in today‟s outpatient physical therapy environment.
33
through central adaptations of both agonist and antagonist muscles; therefore, tennis elbow exercise may provide both structural and functional benefit during tendinopathy rehabilitation9 Research published in the journal of shoulder and elbow surgery found that the Tyler twist exercise using the Thera-band FlexBar is effective at reducing pain associated with tennis elbow.
The Tyler twist exercise promote an emphasis on home based inexpensive treatment as compared to clinically based use of more expensive devices.
Bill Vicenzino, in his study has suggested that clinically in musculoskeletal conditions, by minimizing the aggravation of symptoms during the performance of therapeutic exercise, use of taping technique may facilitate the compliance to exercise rehabilitation programs. He also suggested that diamond taping may be a useful adjunct in management of lateral epicondylitis where it would serve to optimize the imposed loads on the forearm muscles during exercise and functional rehabilitation10.
Lilian Albert Zaky has proved in his study that the application of taping technique(diamond tape)improved wrist extension isometric strength and pain immediately after application in patients with lateral epicondylitis13.
Today‟s internet based society will continue to challenge rehabilitation provider to support and practice in an evidence – based practice, as patients learn about successful treatment and look to their physical therapist to provide them.
Hence, this study has focused on a combination treatment of diamond taping along with Tyler twist exercise to enhance the rehabilitation program for tennis elbow and to formulate an evidence based practice.
34
In this study, it was found that Tyler Twist Exercise alone and Tyler twist exercise along with Diamond Tapping were effective in reducing pain and improving Grip Strength in patients with Chronic Lateral Epicondylitis.
Although both groups show a significant reduction of pain, the Tyler twist group with diamond taping was more effective in improving grip strength in patients with Chronic Lateral Epicondylitis. This difference in improvement could be because taping disperses stresses generated by muscle contraction, thereby reducing painful inhibition and allowing the subject to contract more forcefully. Further, a possible model of mechanism of action for taping may relate to its neurophysiologic effects on the nervous system .In this neurophysiologic model, the tape may exert an effect on grip strength by primarily altering the pain perception, either locally at the elbow by inhibiting nociceptors, facilitating large afferent fibre input into the spinal cord and/or possibly stimulating endogenous process of pain inhibition as stated by Alireza Shamsoddini5.
In the study conducted by Shamsoddini, he used a modified taping technique, where patient alone and without the help of the therapist, pasted tapes on their elbows. In this study the whole procedure of Tyler-twist exercise and Diamond taping was done under the supervision of the therapist. But if the patient been trained the technique of Diamond taping as proposed by Shamsoddini5 ,it would be purely a cost effective treatment, with minimal assistance of the therapist.
35
LIMITATION OF THE STUDY
1. The study consists of a small quantity of patients. 2. No long term follow up was done.
3. No blinding was done.
SCOPE FOR FURTHER STUDY:
1. Further study can be done with larger sample size. 2. Study can be done with long term follow up.
3. The same study can be done on acute lateral epicondylitis patients.
36
CONCLUSION
BIBLIOGRAPHY
1. Puranik VKC, 2009, A comparative study to analyze the effect of low level laser therapy and ultrasound therapy in patients with lateral epicondylitis,
2. Ebnezar J, 2003, Essentials of Orthopedics for Physiotherapists, Jaypee Brothers Medical Publishers, New Delhi.
3. Jones VAL, 2009, Physiotherapy in the management of tennis elbow: a review, British Elbow and Shoulder Society. Shoulder & Elbow, 1: 108–113.
4. D Stasinopoulous, K Stasinopoulou and M I Johnson, An exercise programme for the management of lateral elbow tendinopathy. British Journal of Sports Medicine2005;39:944-947
5. Shamsoddini A, Hollisaz MT and Hafezi R, 2010, Initial effect of taping technique on wrist extension and grip strength and pain of individuals with lateral epicondylitis, Iranian Rehabilitation Journal, 8(11): 24-28.
6. Sharath UR, 2005, combined effect of wrist manipulation and tennis elbow taping in patients with tennis elbow, Rajiv Ghandi University of Health Sciences, Bangalore. 7. Ian G Macintyre. Heavy eccentric loading for a recalcitrant case of lateral
epicondylosis in a hockey player: A case report. July 2007.
8. Kraushaar B, Nirschl R. Concepts review-tendinosis of the elbow (tennis elbow),Clinical features and findings of histological, immunohistochemical and electron microscopy studies. J Bone Joint Surg.1999; 81; 259-85.
9. Tyler T F et al, A new exercise for tennis elbow that works, s: 2010;5(3):189-192 10. Vicenzino B, Brooksbank J, Minto J, Offord S and Paungmali A, 2003, Initial effects
of elbow taping on pain-free grip strength and pressure pain threshold, Journal of Orthopedic & Sports Physical Therapy, 33(7):401-407.
11.Alam N, 2008, A study on the effectiveness of Mc Connell’s taping with cyriax approach & mulligan mobilization on chronic lateral epicondylitis, Rajiv Ghandhi University of Health Sciences, Bangalore.
12.Macdonald R, 1994, Taping Techniques-Principles and Practice, Butterworth- Heinemann, Oxford.
13.Lilian Albert Zaky, Imitate effect of diamond taping technique in treatment of tennis elbow.vol.18,no.(1)Jan:2013.
15.Phil Page, clinical suggestion, A new exercise for tennis elbow that works, 2010 volume 5.
16.Magee D, Orthopedic physical assessment. 5th edition St. Louis, Mo.: Saunders Elsevier.
17.Norris C. Sports injuries. 3rd edition. Oxford: Butterworth-Heinemann; 1998.
18.Zeisig E, 2008, Tennis elbow: sonographic findings and intratendinous injection treatment, Umea University, Sweden.
19. Hutson M, 2001, Sports Injuries Recognition and Management, Oxford University Press, New York. )
20. Bohannon RW. Hand-grip dynamometry provides a valid indication of upper extremity strength impairment in home care patients. J Hand Ther. 1998; 11(4): 258-60.
21.Boonstra AM, SchiphorstPreuper HR, Reneman MF. Reliability and validity of the visual analogue scale for disability in patients with chronic musculoskeletal pain. Int J Rehabil Res. 2008; 31(2): 165-9.
22.Isam Atroshi, Christina Gummesson, Bodil Anderssion,Elsa Dahlgren & Anita Johansson The Disabilities of the arm ,shoulder and hand (DASH)outcome questioner :Reliability and validity of the Swedish version evaluated in 176 patients.08 july 2009.71:6, 613 - 618.
23.Stasinopoulos Dimitrius and Manias Pantelis Comparing tow exercise programs for the management of lateral elbow tenopathy(Tennis elbow or Lateral epicondylitis) A comparative study 26 may 2013.
24.www.google.com
25.www.centralpubmed.com 26.www.apta.org
27.www.jospt.org
PROFORMA
Name :
Age :
Gender : Male/Female
Occupation :
Marital Status :
Chief Complaints :
Past Medical History :
Present History :
Personal History :
Socio-economic History :
VITAL SIGNS
I. Heart Rate :
II. Pulse :
III. Blood Pressure :
IV. Respiratory Rate :
PAIN ASSESSMENT
Site :
Side :
Duration :
Type :
Nature :
Aggravating Factors :
Severity :
Visual Analog Scale (VAS) :
ON OBSERVATION
General Observation :
Local Observation :
PALPATION
Swelling :
Tenderness :
Warmth :
EXAMINATION
Muscle Power :
Muscles Right Left
Special Tests :
Mill’s Test Cozen’s Test
INVESTIGATION
1. X-Ray :
2. MRI :
VARIABLES PRE
TEST
POST TEST NPRS
GRIP STRENGTH DASH
PHYSIOTHERAPY MANAGEMENT PLAN OF TREATMENT
Short Term Goal
Long Term Goal
INFORMED CONSENT FORM
I ………..………. agree to participate in the research study conducted by Mrs S. SUGANYA, II year, MPT (Ortho), Madha College of Physiotherapy entitled “A comparative study to prove the effectiveness of Tyler twist
exercise with diamond taping to improve wrist extensor muscle strength and decrease pain in management of lateral epicondylitis”
I acknowledge that the research study has been explained to me and I understand the agreeing to participate in the research means I am willing to,
1. Provide information about my health status to the researcher(s)
2. Allow the researcher(s) to have access to my professional records pertaining to the purpose of the study.
3. Participate in training program for duration of 6 weeks 4. Make myself available for follow up.
5. Understand and follow the home advice(s) that will be provided.
I have been informed about the purpose; procedure(s), measurement(s) and risk(s) involved in the research and my queries towards the research have been clarified.
I provide consent to the researcher to use the information, video recording(s), for research and educational purpose only.
I understand that my participation is voluntary and can withdraw at any stage of the research project.
Name of the Participant Date
APPENDICES
The Numeric Pain Rating Scale (NPRS)
THE DISABILITY OF ARM SHOULDER AND HAND QUESTIONER
(DASH)
The disability of arm, shoulder and hand (Dash) questioners is a self-administered region specific outcome instrument, develop to measure upper extremity disability and symptoms. The dash consists of 30 – item disability / symptom scale.
1. The items (table-I) ask about the degree of difficulty in performing various physical activities because of an arm, shoulder and hand problems (21 items).
2. Dash also consists of 2 optional 4 items scale concerning the ability to perform sports and /or to play a musical instruments (sports/musical scale) and ability to work (works scale).
3. Each item has 5 response choice ranging from no difficulty to ranging from unable to perform the activity or very severe symptoms, and is scored on a 1- 5point scale.
DASH scale is calculated by
DASH disability/symptoms score =[(sum of n response) -1] x 25 n
Mill’s Test:
Purpose: To determine the presence of a lateral epicondylitis.
Test Position: Standing.
Performing the Test: Palpate the lateral epicondyle while passively pronating the forearm, flexing the wrist and extending the elbow. A positive test is reproduction of lateral elbow pain.
Diagnostic Accuracy: Unknown.
Cozen's Test
Purpose: To determine the presence of lateral epicondylitis.
Test Position: Standing or sitting.
Performing the Test: Stabilize the patient’s forearm and instruct the patient to make a fist, pronate the forearm, radially deviate, and extend the wrist. Next the clinician palpates the lateral epicondyle with the stabilizing hand and applies a flexion force against the patient’s resistance. A positive test is reproduction of lateral elbow pain.
Diagnostic Accuracy: Unknown.
D
ISABILITIES OF THE
A
RM
, S
HOULDER AND
H
AND
DA SH
INSTRUCTIONS
This questionnaire asks about your symptoms as well as your ability to perform certain activities.
Please answer every question, based
on your condition in the last week, by circling the appropriate number.
If you did not have the opportunity to perform an activity in the past
week, please make your best estimate
on which response would be the most accurate.
It doesn’t matter which hand or arm you use to perform the activity; please answer based on your ability regardless of how you perform the task.
Please rate your ability to do the following activities in the last week by circling the number below the appropriate response.
NO MILD MODERATE SEVERE
UNABLE DIFFICULTY DIFFICULTY DIFFICULTY DIFFICULTY
1. Open a tight or new jar. 1 2 3 4 5
2. Write. 1 2 3 4 5
3. Turn a key. 1 2 3 4 5
4. Prepare a meal. 1 2 3 4 5
5. Push open a heavy door. 1 2 3 4 5
6. Place an object on a shelf above your head. 1 2 3 4 5
7. Do heavy household chores (e.g., wash walls, wash floors).1 2 3 4 5
8. Garden or do yard work. 1 2 3 4 5
9. Make a bed. 1 2 3 4 5
10. Carry a shopping bag or briefcase. 1 2 3 4 5
11. Carry a heavy object (over 10 lbs). 1 2 3 4 5
12. Change a lightbulb overhead. 1 2 3 4 5
13. Wash or blow dry your hair. 1 2 3 4 5
14. Wash your back. 1 2 3 4 5
15. Put on a pullover sweater. 1 2 3 4 5
16. Use a knife to cut food. 1 2 3 4 5
17. Recreational activities which require little effort
(e.g., cardplaying, knitting, etc.). 1 2 3 4 5
18. Recreational activities in which you take some force or impact through your arm, shoulder or hand
(e.g., golf, hammering, tennis, etc.). 1 2 3 4 5
19. Recreational activities in which you move your
arm freely (e.g., playing frisbee, badminton, etc.). 1 2 3 4 5
20. Manage transportation needs
(getting from one place to another). 1 2 3 4 5
21. Sexual activities. 1 2 3 4 5
NOT AT ALL SLIGHTLY MODERATELY QUITE EXTREMELY A BIT
22. During the past week, to what extenthas your arm, shoulder or hand problem interfered with your normal social activities with family, friends, neighbours or groups?
(circle number) 1 2 3 4 5
NOT LIMITED SLIGHTLY MODERATELY VERY
UNABLE
AT ALL LIMITED LIMITED LIMITED
23. During the past week, were you limited in your work or other regular daily activities as a result of your arm,
shoulder or hand problem? (circle number) 1 2 3 4 5 Please rate the severity of the following symptoms in the last week. (circle number)
NONE MILD MODERATE SEVERE EXTREME
24. Arm, shoulder or hand pain. 1 2 3 4 5
25. Arm, shoulder or hand pain when you
performed any specific activity. 1 2 3 4 5
26. Tingling (pins and needles) in your arm, shoulder or hand. 1 2 3 4 5
27. Weakness in your arm, shoulder or hand. 1 2 3 4 5
28. Stiffness in your arm, shoulder or hand. 1 2 3 4 5
NO MILD MODERATE SEVERE
SO MUCH
DIFFICULTY DIFFICULTY DIFFICULTY DIFFICULTY
DIFFICULTY THAT I CAN’T SLEEP
29. During the past week, how much difficulty have you had sleeping because of the pain in your arm, shoulder or hand?
(circle number) 1 2 3 4 5
STRONGLY NEITHER AGREE STRONGLY
DISAGREE DISAGREE NOR DISAGREE AGREE AGREE
30. I feel less capable, less confident or less useful because of my arm, shoulder or hand problem.
(circle number) 1 2 3 4 5
D
ISABILITIES OF THE
A
RM
, S
HOULDER AND
H
AND
A DASH score may not be calculated if there are greater than 3 missing items.
DASH DISABILITY/SYMPTOM SCORE= [(sum of n responses) - 1] x 25, where n is equal to the number of completed responses.
WORK MODULE (OPTIONAL)
The following questions ask about the impact of your arm, shoulder or hand problem on your ability to work (including home-making if that is your main work role).
Please indicate what your job/work is: _________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
❐ I do not work. (You may skip this section.)
Please circle the number that best describes your physical ability in the past week. Did you have any difficulty:
NO MILD MODERATE SEVERE
UNABLE DIFFICULTY DIFFICULTY DIFFICULTY DIFFICULTY
1. using your usual technique for your work? 1 2 3 4 5
2. doing your usual work because of arm,
shoulder or hand pain? 1 2 3 4 5
3. doing your work as well as you would like? 1 2 3 4 5
4. spending your usual amount of time doing your work? 1 2 3 4 5
D
ISABILITIES OF THE
A
RM
, S
HOULDER AND
H
AND
© INSTITUTE FOR WORK & HEALTH 2006. ALL RIGHTS RESERVED.
SPORTS/PERFORMING ARTS MODULE (OPTIONAL)
The following questions relate to the impact of your arm, shoulder or hand problem on playing your musical instrument or sport or both. If you play more than one sport or instrument (or play both), please answer with respect to that activity which is most important to you.
Please indicate the sport or instrument which is most important to you: ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
❏ I do not play a sport or an instrument. (You may skip this section.)
Please circle the number that best describes your physical ability in the past week. Did you have any difficulty:
NO MILD MODERATE SEVERE UNABLE
DIFFICULTY DIFFICULTY DIFFICULTY DIFFICULTY
1. using your usual technique for playing your
instrument or sport? 1 2 3 4 5
2. playing your musical instrument or sport because
of arm, shoulder or hand pain? 1 2 3 4 5
3. playing your musical instrument or sport
as well as you would like? 1 2 3 4 5
4. spending your usual amount of time
practising or playing your instrument or sport? 1 2 3 4 5
SCORING THE OPTIONAL MODULES: Add up assigned values for each response; divide by 4 (number of items); subtract 1; multiply by 25.
MASTER DATA
S.No. GROUP A
PRE – TEST POST TEST
NPRS
GRIP
STRENGTH(Kg) DASH NPRS
GRIP
STRENGTH(Kg) DASH
1 5 10 53.3 1 18 32.2
2 9 6 60.8 2 15 35.00
3 8 8 57.5 2 20 33.3
4 6 9 62.5 0 11 36.67
5 4 11 60.84 1 15 37.5
6 7 8 62.5 2 12 35.84
7 8 9 63.64 3 13 34.16
8 8 10 60.83 1 14 35.00
9 7 6 56.57 2 16 32.5
10 5 10 60.84 1 12 34.16
11 4 8 58.53 0 11 38.34
12 9 7 58.34 1 12 40.83
13 6 10 63.00 2 13.5 31.67
14 8 9 60.00 1 15 30.84
15 7 7 57.5 1 13 35.00
GROUP B
PRE – TEST POST TEST
NPRS
GRIP
STRENGTH DASH NPRS
GRIP
STRENGTH(Kg) DASH
7 8 57.5 1 22 30.8
9 5 61.6 2 20 30.00
6 9 60.00 1 21 34.3
10 7.5 61.67 2 19 34.16
5 10 52.5 1 21 34.67
7 8.5 60.00 1 23 32.5
9 9.5 62.5 2 18 36.67
8 4 56.67 2 19 30.84
6 10 61.67 1 23 34.1
4 9 65.13 0 20 28.33
7 9.5 57.5 2 21.5 35.00
9 8 62.5 1 20 33.34
5 11 53.34 0 22 31.67
8 10 60.84 1 20 36.67