White Rose Research Online URL for this paper:
http://eprints.whiterose.ac.uk/75165/
Other:
Arksey, H (2005) Access to health care for carers. National Co-ordinating Centre for NHS
Service Delivery and Organisation Research and Development, London.
eprints@whiterose.ac.uk https://eprints.whiterose.ac.uk/ Reuse
Items deposited in White Rose Research Online are protected by copyright, with all rights reserved unless indicated otherwise. They may be downloaded and/or printed for private study, or other acts as permitted by national copyright laws. The publisher or other rights holders may allow further reproduction and re-use of the full text version. This is indicated by the licence information on the White Rose Research Online record for the item.
Takedown
If you consider content in White Rose Research Online to be in breach of UK law, please notify us by
Access to Health Care for Carers:
Barriers and Interventions
Re p or t f or t h e N a t ion a l Co- or d in a t in g Ce n t r e f or
N H S Se r v ice D e liv e r y a n d Or g a n isa t ion
R & D ( N CCSD O)
D e ce m b e r 2 0 0 3
pr epar ed by
Hilary Arksey, Karen Jackson Social Policy Research Unit ( SPRU) Alison Wallace, Sally Baldwin
Depar t m ent of Social Policy & Social w or k ( SPSW) Su Golder
NHS Cent re for Reviews and Dissem inat ion ( CRD) Elizabet h Newbronner, Philippa Hare
Act on.Shapir o
Addr ess f or cor r espon den ce
Dr Hilary Arksey, Resear ch Fellow Soc ial Policy Research Unit Universit y of York,
Heslingt on York YO10 5DD
Cont ent s
Ack n ow le dge m e n t s 4
Ex e cu t iv e Su m m a r y
Background 5
Obj ect iv es of t h e st u dy 5
Resear ch m et h ods: lit er at u r e r ev iew 6
Resear ch m et hods: consult at ion 6
Ty pology of bar r ier s t o access t o h ealt h car e f or car er s 7
Key findings 7
Gaps and w eaknesses in t he ev idence base 11 Recom m en dat ion s f or f u r t h er r esear ch 12
Dissem inat ion 13
Th e Re por t
Ch a pt e r 1 I n t r odu ct ion 1 4
1 . 1 Access t o h ealt h car e 14
1. 2 Car er s and car e giv ing 15
1.3 Policy cont ext 17
1. 4 Aim s and obj ect iv es of st udy 18 1 . 5 St r u ct u r e of t h e r epor t 19
Ch a pt e r 2 Re se a r ch m e t h ods 2 0
2. 1 I nt r oduct ion 20
2 . 2 Th e r ev iew pr ot ocol 20
2 . 3 Refer ences r et r iev ed 28
2.4 Consult at ion 31
2.5 Dat a synt hesis 32
Ch a pt e r 3 Ba r r ie r s t o ca r e r s’ a cce ss t o h e a lt h ca r e 3 3
3. 1 I nt r oduct ion 33
3 . 2 Ty pology of bar r ier s t o access t o h ealt h car e f or car er s 33 3. 3 Nat ur e and or ganisat ion of ev idence 34 3. 4 Bar r ier s r elat ed t o pr of ession al ch ar act er ist ics 40 3. 5 Bar r ier s r elat ed t o ser v ice issues 45 3. 6 Bar r ier s r elat ed t o language or cult ur al issues 50 3 . 7 Bar r ier s r elat ed t o car er or car e r ecipien t ch ar act er ist ics 54 3.8 Bar r ier s r elat ed t o know ledge and infor m at ion issues 58
Ch a pt e r 4 I n t e r ve n t ion s t o im pr ov e a cce ssibilit y for ca r e r s 6 3
4. 1 I nt r oduct ion 63
4 . 2 Cur r ent policy and pr act ice in t he NHS 63 4 . 3 I n t er v en t ion s t o ov er com e bar r ier s t o h ealt h car e f or car er s 66 4.4 Ov er com ing bar r ier s r ela t ed t o pr of ession al ch ar act er ist ics 70 4. 5 Ov er com ing bar r ier s r elat ed t o ser v ice issu es 72 4 . 6 Ov er com ing bar r ier s r elat ed t o language or cult ur al issues 74 4 . 7 Ov er com in g bar r ier s r elat ed t o car er or c ar e r ecipient
ch ar act er ist ics 75
4. 8 Ov er com ing bar r ier s r elat ed t o infor m at ion and know ledge
issues 77
4.9 Conclusion 79
Ch a p t e r 5 D iscu ssion a n d con clu sion s 8 2
5. 1 I nt r oduct ion 82
5. 2 Sum m ar y of r esult s 82
5. 3 Concept ualising access t o h ealt h car e f or car er s 85 5 . 4 Recom m endat ions t o im pr ov e car er s’ access t o h ealt h car e 90 5.5 Gaps and weak nesses in t he ev idence base 94 5. 6 Recom m endat ion s f or f u r t h er r esear ch 99 5.7 Dissem inat ion and im plem ent at ion of r esear ch findings 102
Re fe r e n ce s 1 0 3
Ap p e n d ice s
Appe n dix 1 Ele ct r on ic se a r ch st r a t e gie s 1 1 0
Appe n dix 2 Re su lt s of d a t a b a se s se a r ch e d 1 2 4
Appe n dix 3 D a t a e x t r a ct ion for m 1 2 5
Appe ndix 4 N a t iona l a nd loca l or ga n isa t ion s con su lt e d 1 2 8
Appe n dix 5 I n t e r vie w sch e du le for n a t ion a l or ga n isa t ion s 1 2 9
Appe n dix 6 I n t e r vie w sch e du le for loca l or ga n isa t ions 1 3 1
Appe n dix 7 Su m m a r y of cor e st u die s 1 3 3
Appe ndix 8 Sum m a r y of in t e r m e dia t e st u die s 1 3 6
Appe n dix 9 Su m m a r y of su pple m e n t a r y st u die s 1 3 9
Appe n dix 1 0 Su m m a r y of r e spit e st u die s 1 4 1
Appe n dix 1 1 Su m m a r y of in t e r ve n t ion e va lu a t ion s 1 4 6
Acknowledgem ent s
The r esear ch w as funded by t he NHS Ser vice Deliver y & Or ganisat ion ( SDO) Research and Developm ent Program m e ( Proj ect reference SDO/ 24/ 2002) .
We ar e gr at eful t o all t hose indiv iduals w ho cont r ibut ed t heir t im e and ex per t ise t o t he consult at ion.
Colleagues hav e pr ov ided helpful adv ice and suppor t dur ing t he cour se of t he work, in part icular Karen Croucher, Michael Hirst , Em ily Holzhausen, Lisa
O’Malley and Julie William s. Em ese Mayhew ’s cont ribut ion t o t he ear ly st ages of t he review w as invaluable. We are grat eful t o librarians in t he J.B. Morrell Libr ar y at t he Univer sit y of Yor k for all t heir assist ance. Sally Pulleyn pr ovided v aluable secr et ar ial suppor t t hr oughout t he st udy .
Ex e cu t ive Su m m a r y
Background
The General Household Survey 2000 show s t hat approxim ately 6.8 m illion adult s in Brit ain provide care t o sick or disabled relat ives or friends, or t he elder ly. Car er s r epor t high levels of st r ess, anxiet y and depr ession, as w ell as general healt h problem s and physical inj uries such as st rained backs associat ed w it h lift ing. The m or e dem anding car e, t he less likely it is t hat car er s w ill have t im e t o at t end t o t heir ow n healt h car e needs. Cur r ent gov er nm ent policy put s an em phasis on support ing carers in t heir caring role, and ensuring t hat t he NHS and social ser v ices helps t hem m aint ain t heir healt h. The int ent ion t hat car er s obt ain qualit y healt h car e ser v ices is not necessar ily r ealised in pr act ice. Many car er s feel m ar ginalised by healt h car e pr ofessionals and
believ e t hat t heir ow n needs for healt h care ar e ov er look ed. Consequent ly , it is im por t ant t o ident ify t he bar r ier s t hat pr ev ent car er s fr om accessing, and ut ilising, effect iv e healt h car e ser v ices, as w ell as int er v ent ions t hat can im pr ov e accessibilit y .
Obj ect ives of t he st udy
The overall aim of t he w ork w as t o inform t he NHS Service Delivery and
Organisat ion ( SDO) R & D Program m e about t he t heory and evidence on carers’ access t o h ealt h car e. Th e t w o k ey obj ect iv es w er e:
• t o exam ine t he evidence from UK and int ernat ional research ( published and
unpublished) in order t o ident ify:
– t he pr oblem s and bar r ier s t hat car er s ex per ience in accessing healt h car e ser v ices, and any associat ed issues r elat ing t o equit y of access and level of unm et need
– ev idence of int er v ent ions designed t o im pr ov e car er s’ access t o h ealt h car e ser v ices, and how t hese v ar y accor ding t o age and cir cum st ances
• t o consult w it h k ey st ak eholder s w it h an int er est in car er s’ access t o healt h car e about t he findings fr om t he r eview and r ecom m endat ions for fur t her r esear ch.
The follow ing report docum ent s key t hem es from t he lit erat ure review and consult at ion. I n addit ion, it pr esent s a t y pology of bar r ier s t hat car er s encount er w hen accessing healt h car e, and dev elops a m odel of access t o healt h car e specifically for car er s. Det ailed infor m at ion about t he int er v ent ions r ev iew ed can be found in t he supplem ent ar y r epor t : Access t o Healt h Car e for
Research m et hods: lit erat ure review
A pr ot ocol w as dr aw n up t o guide t he r ev iew pr ocess. The aim of t he lit er at ur e r ev iew w as t o ident ify all st udies published since 1987 t hat could help answ er t he cent r al r esear ch quest ion: ‘What does t he r esear ch ev idence t ell us about w hat r est r ict s, w hat pr om ot es and w hat im pr ov es car er s’ access t o healt h car e ser v ices?’ Sear ches w er e m ade of k ey elect r onic dat abases and t he I nt er net . Ot her sear ch st r at egies included hand sear ching, sear ching w eb sit es of k ey or ganisat ions, and cont act ing k ey r esear cher s in t he field. Bibliogr aphies of st udies w er e check ed t o ensur e r efer enc ed st udies w er e included. Of t he 8775 init ial r efer ences, 46 w er e found t o be bot h applicable t o t he r esear ch quest ion and of sufficient qualit y t o ent er t he r ev iew ; 32 of t he r epor t s discussed bar r ier s t o car er s’ access t o healt h car e or r espit e ser v ices. Th e rem aining 14 were evaluat ions of int ervent ions designed t o im prove
accessibilit y . Ther e w er e t hr ee gr oups of int er v ent ions: pr im ar y car e init iat ives, hom e - based healt h car e pr oj ect s, and geogr aphical infor m at ion sy st em s ( GI S) soft w ar e. The 46 r esear ch r epor t s w er e classified in t er m s of t y pe of st udy design and st r engt h of ev idence. Som e of t he st udies w er e st ronger and m ore robust in com parison wit h ot hers which had im plicat ions for t he conclusions t hat could r easonably be dr aw n. Relev ant dat a w er e ext r act ed fr om each st udy and sy nt hesised t hr ough a nar r at iv e r ev iew .
Resear ch m et hods: consult at ion
Cont r ibut or s t o t he consult at ion included policy m ak er s and pr act it ioner s w it h an int er est in car er s’ access t o healt h car e. Tw o m ain st ak eholder gr oups w er e involved:
• nat ional st at ut or y and v olunt ar y sect or or ganisat ions ( n= 12)
• local or ganisat ions t hat had int r oduced int er v ent ions specifically t o im pr ov e car er s’ access t o healt h car e ( n= 8) .
Key aim s of t he consult at ion w er e:
• t o ex plor e per cept ions of t he bar r ier s t hat car er s confr ont w hen t r y ing t o gain access t o h ealt h car e ser v ices
• t o ident ify specific ex am ples of int er v ent ions, good pr act ice and ar eas of t he count r y t hat hav e m ade pr ogr ess in facilit at ing access for car er s
• t o com plem ent t he r ev iew findings, and help m ake recom m endat ions t hat
Typology of barriers t o access t o healt h care for
carers
Exist ing concept ual fram ew orks t o help underst and w hy people m ay or m ay not gain access t o healt h car e did not easily accom m odat e t he par t icular bar r ier s t hat car er s confr ont . A t y pology of bar r ier s, based on ex ist ing m odels and t he ev idence fr om t he lit er at ur e r ev iew , w as dev eloped specifically for car er s. I t provided t he organising framew or k for ex am ining access t o healt h car e for car er s, and com pr ised fiv e differ ent t y pes of bar r ier s r elat ing t o:
• pr ofessional char act er ist ics
• ser v ice issues
• language or cult ural issues
• car er or car e r ecipient char act er ist ics
• inform at ion and know ledge issues.
Key findings
Ba r r ie r s r e la t e d t o pr ofe ssion a l ch a r a ct e r ist ics
Key bar r ier s ident ified in t he lit er at ur e r eview and consult at ion r elat ing t o pr ofessional char act er ist ics included: lack of r ecognit ion of t he car ing r ole and aw ar eness of t he needs and issues inv olv ed; pr ofessional uncer t aint y about r oles and boundar ies; r eact iv e r at her t han pr oact iv e appr oaches; pr ior it ising t he car e r ecipient at t he ex pense of t he car er ; pr ofessional m odels,
concept ualisat ions or st er eot y pes of car er s t hat m ay n ot be con du civ e t o m eet ing t heir needs.
These ar e difficult issues t o addr ess, especially on a shor t - t erm basis. I n t erm s of int er v ent ions, t he ev idence indicat ed t hat car er suppor t w or k er s in pr im ar y care init iat ives provided t raining and helped raise aw ar eness of car er s’ issues. This could help det er pr ofessionals fr om allow ing pr econceived not ions and assum pt ions about car er s t o st and in t he w ay of r efer r als or t he offer of par t icular t r eat m ent s. Healt h car e pr ofessionals t ak ing on t he r ole of
‘cham pio ns’ could help t o change at t it udes and spr ead good pr act ice. Building up good r elat ionships bet w een car er s and pr ofessionals, and t r eat ing car er s as ‘par t ner s’ in t he pr ov ision of car e, could also facilit at e access for car er s.
r equir em ent s; incent iv es for pr im ar y car e pr ofessionals t o focus on car er s’ healt h and pr oact iv ely offer healt h check s.
Ba r r ie r s r e la t e d t o se r v ice issu e s
Wit h r egar d t o ser v ice issues, t he lit er at ur e r ev iew and consult at ion
consist ent ly ident ified t he follow ing bar r ier s: GP sur ger ies not ident ifying car er s and/ or ‘t agging’ carers’ r ecor ds; lack of t r aining in car er s’ issues; ‘gat
e-keeping’; inflexible appoint m ent syst em s; wait ing t im es; t ransport and car par k ing; cost s.
Wit h r efer ence t o int er v ent ions t o ov er com e ser v ice issue bar r ier s, a m ain feat ure of all prim ary care init iat iv es w as t o set in place sy st em s t o ident ify car er s, and t ag m edical r ecor ds. Ther e w as ev idence t hat hom e - based int er v ent ions helped t ack le t r anspor t and/ or subst it ut e car e pr oblem s; car er s w ho w er e housebound or lived in r ur al ar eas also gained. Massage t her apist s, for exam ple, t ook t heir t ables t o car er s’ hom es. Telephone- and com put er-based ser v ices pr ov ided dir ect access, on dem and, t o infor m at ion, educat ion and ‘in- hom e’ suppor t gr oups t her eby facilit at ing easier access t o pr ofessional support . Geographical infor m at ion sy st em s soft w ar e had t he pot ent ial t o infor m fut ur e dev elopm ent s r elat ing t o local pr ov ision of ser v ices t o suppor t car er s. Cont r ibut or s t o t he consult at ion em phasised t he use of non- healt h v enues, flexibilit y and sim ple referral procedure s ( including self - referral) .
Based on t he findings, r ecom m endat ions t o addr ess bar r ier s r elat ing t o ser vice issues include: ident ificat ion and t agging of car er s in m edical r ecor ds, including hospit al adm ission and dischar ge not es; inclusion of quest ions t o ident ify car er s in hospit al adm ission and dischar ge not es; inclusion of a car er quest ion at new pat ient r egist r at ion, on r egular ov er- 75s’ healt h check s and ot her st andar d healt h scr eenings, and on r epeat pr escr ipt ion for m s; pr ovision of healt h car e ser v ices in set t ings w hich ar e accessible and accept able t o car er s; low er ing t he t hr eshold of access t o ser v ices t o allow m or e ear ly , pr ev ent iv e w or k w it h car er s; ident ificat ion of a point of cont act or car er suppor t w or k er in each pr act ice or ser v ice; gr eat er r ecognit ion of t he needs and special
cir cum st ances of car er s in t he w ay in w hich appoint m ent s and ser v ices ar e offer ed and elect iv e pr ocedur es ar e ar r anged; m or e st r at egic and co- or dinat ed use of t he Car er s Special Gr ant ; incr ease in t he local availabilit y of flexible and appr opr iat e r espit e ser v ices; funding for t he ev aluat ion of local init iat iv es t o enable t hem t o dem onst r at e t heir effect iv eness; and r ecognit ion and
addr essing of t he t r anspor t needs of car er s, especially in r ur al ar eas, w hich could include m ore use of hom e visit s.
Ba r r ie r s r e la t e d t o la n g u a g e or cu lt u r a l issu e s
Language and cult ur al bar r ier s ident ified by t he lit er at ur e r eview and
Alt hough no int er v ent ions w er e found t hat specifically addr essed bar r ier s r elat ed t o language or cult ur al issues, t he im por t ance of r eaching out t o black and et hnic m inor it y car er s w as com m ent ed upon. The consult at ion suggest ed t hat healt h pr ofessionals w it h a posit iv e appr oach t o m inor it y car er s could en cou r age access.
Based on t he findings, recom m endat ions t o address barriers relat ing t o language or cult ur al issues include: assist ance w it h r eading, w r it ing and for m com plet ion; expansion of pr ofessional int er pr et ing and t r anslat ion ser vices w it hin pr act ices and ser v ices; cult ur al div er sit y t r aining for healt h car e professionals in cult ural and r eligious issues and appr opr iat e pr act ices.
Ba r r ie r s r e la t e d t o ca r e r or ca r e r e cipie n t
ch a r a ct e r ist ics
The ev idence indicat ed t hat k ey bar r ier s r elat ing t o t he char act er ist ics,
behav iour s and beliefs of car er s or car e r ecipient s t hat ser v ed t o inhibit access t o healt h car e included: car er s’ appr oach t o car e giv ing and/ or healt h
prom ot ion; carers; help- seeking behaviours; personal and/ or cult ural beliefs and pr efer ences; car e r ecipient s’ at t it ude.
The r ev iew of t he ev aluat ions of int er v ent ions show ed t hat m any car er s accept ed t heir sit uat ion and/ or did not ident ify t hem selv es as car er s, em phasising t he im port ance, not ed earlier, of GP surgeries ident ifying ( and r ecor ding) car er s. Car er s w er e offer ed infor m at ion and suppor t by
int erm ediaries, for exam ple recept ionist s, w hich helped ov er com e t heir lack of assert iveness. Carer support w orkers not only provided inform at ion but also adv ocacy ser v ices, enabling car er s t o t alk t hr ough issues and ident ify solut ions w it h an independent per son. Suppor t gr oups r educed feelings of isolat ion, incr eased confidence and influenced help- seeking behaviour. For carers unable t o j oin conv ent ional suppor t gr oups, t elephone- and com put er- based pr oj ect s offering ‘in- hom e’ suppor t gr oups w er e valuable. Such int er vent ions w er e especially useful t o car er s w ho valued anonym it y, and/ or w er e em bar r assed or lacked self - confidence t o t alk openly . Cont r ibut or s t o t he consult at ion
em phasised t he v alue of adopt ing a holist ic appr oach t o car er s, aim ed at addressing t heir em ot ional, psychological and spir it ual needs.
Based on t he findings, recom m endat ions t o address barriers relat ing t o carer or car e r ecipient char act er ist ics include: educat ion for car er s by healt h
Ba r r ie r s r e la t e d t o in f or m a t ion a n d k n ow le d g e
issu e s
The follow ing barriers relat ed t o inform at ion and know ledge issues w ere uncov er ed by t he lit er at ur e r ev iew and consult at ion: car er s not being giv en infor m at ion about av ailable ser v ices and how t o access t hem ; m edical confident ialit y .
The ev idence indicat ed t hat pr im ar y car e init iat iv es and t elephone- and com put er- based pr oj ect s helped address t hese barriers. Prim ary care
init iat ives, for exam ple, developed inform at ion packs and direct ories of nat ional and local car er suppor t facilit ies t o be used by bot h car er s and healt h car e professionals. Carer support w orkers also point ed care r s in t he dir ect ion of r elev ant agencies, and pr ov ided adv ocacy and benefit adv ice. Telephone- and com put er- based int ervent ions w ere useful in providing carers w it h inform at ion and educat ion. Resear ch show ed t hat car er s w ho w er e inex per ienced could nonet heless be quick ly t r ained t o use com put er- based sy st em s; in one st udy , t he av er age age of car er s w as 68 y ear s. Telephone gr oups w er e found t o be as effect iv e in pr ov iding access t o infor m at ion as on- sit e groups for rural and/ or isolat ed car er s. They also pr o v ed cost - effect iv e in suppor t ing r ur al car er s. Cont r ibut or s suggest ed t hat ser v ices t hat w er e w ell net w or k ed t hem selv es w er e in a good posit ion t o signpost car er s t o r elev ant agencies.
Gaps and w eaknesses in t he evidence base
Ga ps
The st udy ident ified clear gaps in t he lit er at ur e in r elat ion t o car er s’ access t o: hospit al- based car e; t er t iar y ser v ices; cont inuing access fr om pr im ar y t o secondar y car e; nat ional scr eening pr ogr am m es; chir opody ; dent al ser v ices; and opt ical car e.
Resear ch has concent r at ed on ser v ices and int er v ent ions aim ed specifically at car er s. Lit t le is k now n about t he im pact on car er s of gener ic ser v ices designed t o im pr ov e access for all pat ient gr oups, such as: NHS Dir ect ; NHS Dir ect online; Walk- I n Cent r es; Healt hy Liv ing Cent r es; Adv anced Access in pr im ar y care; and t he Nat ional Bo oking Program m e.
The lit er at ur e r ev iew did not uncov er any r esear ch t hat look ed at healt h car e access in r elat ion t o t he follow ing gr oups: y oung car er s; older car er s; black and et hnic m inorit y carers; carers from refugee and asylum- seeking
com m unit ies; rural car er s; and car er s of people w it h st igm at ising condit ions ( e.g. m ent al healt h, alcohol or drug- relat ed problem s; HI V/ AI DS) .
I n com par at iv e t er m s, t he ev idence base r elat ing t o how language or cult ur al issues could cr eat e bar r ier s, and in t ur n how t hese could be ov er com e, w as part icularly weak.
M e t h od olog ica l a n d q u a lit y issu e s
St udy designs
Most of t he st udies included in t he r ev iew dr ew on ev idence t hat w as cr oss-sect ional and t hat pr ov ided snapshot s of t he phenom enon under inv est igat ion at one point in t im e by w ay of eit her sur v ey or qualit at iv e int er v iew s. Ther e w as a deficit of pr ospect iv e st udies w it h long- t erm follow- up, collect ing qualit at iv e and quant it at iv e dat a and capt ur ing pr ocess and out com es inform at ion. St udy weaknesses included: sm all sam p le sizes; car er and car e r ecipient v iew s t hat w er e not dist inguished fr om one anot her ; failur e t o disaggr egat e infor m at ion about healt h car e ser v ices and social car e ser v ices; and lim it ed analy sis of t he audit and st at ist ical elem ent s of int er v ent ions. Very few st udies included an econom ic com ponent .
Th e or e t ica l fr a m e w or k s a n d ou t com e m e a su r e s
from all groups of professionals about appr opr iat e out com es t o dem onst r at e t heir effect iv eness and cost - ef f ect iv en ess.
Re por t ing
Ther e w er e inst ances of poor abst r act s and r epor t ing on r esear ch m et hods and dat a analy sis. These sor t s of inadequacies m ak e t he r ev iew pr ocess difficult , especially in r elat ion t o qualit y cont r ol issues.
Recom m endat ions for furt her research
On t he basis of t he lit er at ur e r ev iew and consult at ion, st udies should be com m issioned t hat inv est igat e:
• car er s’ access t o h ealt h car e in t h eir ow n r igh t – m ore work is needed
t hat focuses on t his ar ea, and t hat does not confuse issues in r elat ion t o t he healt h car e needs of car er s and t hose of t he car e r ecipient
• car er s’ access t o h ealt h car e in dif f er en t set t in g – fur t her r esear ch should
look at car er s’ ex per iences and v iew s abou t access t o h ealt h car e in set t ings ot her t han pr im ar y car e; such r esear ch should ev aluat e t he specific healt h out com es of helping car er s t o access healt h car e, and look at t he im pact of int r oducing special m easur es t hat addr ess access
problem s for carers
• car er s’ use of gener ic NHS ser v ices – t her e is a need t o inv est igat e
car er s’ use of gener ic ser v ices, such as NHS Dir ect , NHS Dir ect online; Walk- I n Cent r es; Healt hy Liv ing Cent r es; Adv anced Access in pr im ar y care; and t he Nat ional Booking Program m e
• local pr im ar y car e init iat iv es – local pr im ar y car e init iat ives need t o be
rigorously evaluat ed, in part icular from t he point of view of det erm ining long- t er m effect iv eness, and dev eloping t r ansfer able and/ or sust ainable appr oaches; t her e is scope for st udies aim ed at finding out w het her t hese sor t s of init iat iv es help ov er com e obst acles faced by par t icular car er gr oups, for inst ance y oung car er s
• cult ur ally sensit iv e ser v ices – r esear ch should be under t ak en t o find out
w hat it m eans t o hav e ‘cult ur ally sensit iv e’ healt h car e ser v ices for car er s and how such ser v ices can be im plem ent ed
• infor m at ion and com m unicat ion t echnology . – det ailed qualit at iv e
infor m at ion about car er s’ use of t he I nt er net and e- t echnologies is needed t o inform t he developm ent of lo cal, nat ional and int er nat ional e- healt h w eb sit es for car er s.; r esear ch ex plor ing t he scope for local pr im ar y car e init iat ives, GP sur ger ies, hospit als and car er s’ organisat ions t o j oint ly provide inform at ion on local, regional and nat ional services for c arers w ould also be useful
• specif ic car er gr ou ps. – c om par at iv e dat a show ing v ar iat ions bet w een
geogr aphical ar eas and am ong differ ent gr oups of car er s w ould be
w it h st igm at ising c ondit ions is needed, as is r esear ch int o t he special problem s of access in rural areas
• car er s fr om r efugee and asy lum - seeking com m unit ies. – r esear ch is
r equir ed t hat ex am ines access t o healt h car e ser v ices for car er s fr om refugee and asylum seeking com m unit ies
• ou t com e m easu r es. – r esear ch t o r each agr eem ent am ong differ ent
pr ofessional gr oups about appr opr iat e out com e m easur es t o gauge t he effect iv eness of int er v ent ions t o im pr ov e access w ould be v aluable
• econom ic ev aluat ions – econom ic ev aluat ions, especially of int er v ent ions
t o im pr ov e access for car er s, w ould be v aluable t o policy m ak er s t o k now t he financial im plicat ions of init iat iv es, and how m uch differ ence t hey m ight m ake
• concept ual fr am ew or k s – it w ould be valuable t o under t ake fur t her w or k
t o br ing t oget her differ ent concept ual m odels and fr am ew or ks int o a m or e coher ent fr am ew or k for concept ualising access for car er s m or e br oadly .; t he v alue of t he m odel should t hen be t est ed em pir ically .
Dissem inat ion
Th e Re por t
Chapt er 1 I nt roduct ion
1 .1 Acce ss t o h e a lt h ca r e
I n t he Whit e Paper , The New NHS: Modern, Dependable , t he gov er nm ent set s ou t a vision in which local healt h com m unit ies work in part nership t o plan and deliver im pr ovem ent s in healt h car e ser vices t o benefit t he com m unit y as a w hole ( Depar t m ent of Healt h, 1997) . The needs of pat ient s ar e cent r al; people are t o be offered prom pt high- qualit y t r eat m ent and car e w hen and w her e t hey need it . The NHS Plan t o m oder nise t he NHS r einfor ces t hese t hem es ( Depar t m ent of Healt h, 2000a) . Tw o of t he Plan’s cor e pr inciples ar e t hat ‘The NHS w ill shape it s ser v ices ar ound t he needs and pr efer ences of individual pat ient s, t heir fam ilies and t heir car er s’ ( p.4; par agr aph 3) and t hat ‘The NHS w ill r espond t o differ ent needs of differ ent populat ions’ ( p.4; par agr aph 4) . To help r ealise t his vision, new gener ic ser vices such as NHS Dir ect , NHS Dir ect online, Walk- I n Cent res, t he Nat ional Booking Program m e and ‘Advanced Access’ in pr im ar y car e hav e been int r oduced, init iat iv es t hat hav e t he pot ent ial t o im pr ov e accessibilit y t o healt h car e for all pat ient gr oups.
Opt im al access t o healt h car e has been defined as ‘pr oviding t he r ight ser vice at t he r ight t im e in t he r ight place’ ( Roger s et al., 1999) . How ever, w hile recent NHS policies ( Depart m ent of Healt h, 1997, 2000a) em phasise t he pr ov ision of equit able healt h ser v ices t o t he w hole populat ion of England, obt aining t he r ight suppor t at t he r ight t im e does not depend solely on t he availabilit y of healt h car e ser vices. Gullifor d et al. ( 2001) dist inguish bet w een ‘hav ing access’, w hich is w hen t her e is an adequat e supply of ser v ices and sy st em s in place t o facilit at e ut ilisat ion, and ‘gaining access’, w hich r elat es t o ent r y t o, or act ual ut ilisat ion of, ser v ices. Ev en w her e adequat e ser v ices do ex ist , issues r elat ing t o affor dabilit y , phy sical accessibilit y and accept abilit y can lim it t he ex t ent t o w hich pat ie nt s and car er s m ake use of t hem ; social or cult ur al obst acles can also r est r ict ut ilisat ion ( Gullifor d et al., 2001) .
I nt er act ions bet w een st r uct ur al v ar iables such as et hnicit y or pov er t y m ay int ensify access problem s. Gulliford et al. ( 2001) also point out t hat bar r ier s t o access can occur at differ ent point s on t he healt h car e pat hw ay fr om init ial cont act , t o ent r y and ut ilisat ion of effect iv e, appr opr iat e and accept able ser v ices, t hr ough t o t he at t ainm ent of t he desir ed or appr opr iat e out com es.
The I ndependent I nquiry int o I nequalit ies in Healt h found t hat individuals and com m unit ies m ost at r isk of ill healt h t ended t o exper ience t he least
For exam ple, people from black and et hnic m inorit y com m unit ies are less likely t o r eceiv e t h e ser v ices t h ey n eed.
1 .2 Ca r e r s a n d ca r e g iv in g
I nform al carers of ill and disabled people, and t he elderly, are anot her group t hat is v ulner able t o ex clusion fr om healt h and social car e ser v ices ( Beck er , 2000; How ar d, 2001) , in par t because t hey ar e isolat ed fr om t he r est of societ y as t heir car ing dut ies t ie t hem t o t heir hom es. Ther e is no sim ple definit ion of t he t erm ‘carer’, but generally speaking it refers t o t he provision of unpaid car e, help or suppor t t o a r elat ive or fr iend w ho cannot m anage on t heir ow n because t hey suffer from physical disabilit ies or m ent al healt h problem s, or difficult ies r elat ed t o old age ( Maher and Green, 2002) . This ( inform al) support enables t he car e r ecipient t o cont inue t o liv e in his or her ow n hom e. As far as per sonal car e is concer ned, car er s m ay pr ovide assist ance in m oving, handling, feeding, personal hygiene and adm inist ering m e dicat ion ( Pr incess Roy al Tr ust for Car er s, 2003) . Car er s can be m ale or fem ale, of any age, cult ur e and religion ( Nat ional Assem bly for Wales, 2000) ; t hey m ay com bine caring wit h full- or part - t im e w or k ( Pr incess Royal Tr ust for Car er s, 2003) . For t he
purposes of t his r epor t , w e ar e focusing on issues r elat ing t o t hose car er s w ho pr ov ide unpaid car e, help or suppor t t o anot her per son w ho cannot m anage on t heir ow n because of illness, frailt y or disabilit y. I n ot her w ords, our w orking definit ion of car er does not include par ent s w it h childcar e r esponsibilit ies ( unless t hey are caring for disabled children w ho place dem ands on t hem bey ond t hose r equir ed of par ent s of non- disabled children) , ‘form al’ carers who pr ovide paid car e, or car er s w ho ar e involved in c are giving on a volunt ary basis for a char it able or v olunt ar y or ganisat ion.
full- t im e w or ker s, 17 per cent of par t - t im e w or k er s and 15 per cent of t he unem ployed.
Half of t hose providing care for 20 hours a week or m ore report ed a long-st anding illness, and j ulong-st over one- t hird ( 35 per cent ) said t heir illness lim it ed t heir act ivit ies. Elderly carers in part icular report ed healt h problem s ( 47 per cent r epor t ed a limit ing long- st anding illness) . Carers looking aft er som eone who lived wit h t hem were m ore likely t han t hose caring for som eone living elsewhere t o report healt h problem s arising from t heir responsibilit ies ( 59 per cent com par ed w it h 29 per cent ) .
A subst ant ial body of lit er at ur e now ex ist s show ing t hat car er s believ e car ing has adv er se effect s on t heir ow n phy sical and em ot ional healt h. For ex am ple, car er s r epor t high lev els of st r ess, anx iet y and depr ession, gener al healt h problem s, loneliness and social isolat ion, as w ell as phy sical inj ur ies such as st r ained back s associat ed w it h lift ing ( Par k er , 1993; Tw igg and At k in, 1994; Warner, 1995; Brown and Mulley, 1997; Henwood, 1998; Arksey et al. , 2000; Keeley and Clar ke, 2002) . Near ly 40 per cent of car er s t aking part in t he GHS for 2000 r epor t ed t hat t heir phy sical or m ent al healt h had been affect ed as a r esult of car ing ( Maher and Gr een, 2002) . How ever , est ablishing a causal relat ionship bet ween caring and ill healt h in general is problem at ic ( Parker and Law t on, 1994) . Recent w or k in t he Social Policy Resear ch Unit ( Hir st , 2000) based on secondar y analy sis of t he Br it ish Household Panel Sur v ey r ev eals t hat car ing has gr eat er im pact on car er s’ em ot ional healt h r at her t han phy sical healt h, especially for car er s who provide 20 or m ore hours of care per week.
The w or k by Hir st ( 2000) also show s t hat t he healt h of car er s is m or e lik ely t o det eriorat e t han im prove over t im e com pared w it h healt h changes in non-car er s. This m ight r eflect t he fact t hat alm ost half t he non-car er s r esponding t o a large- scale quest ionnair e sur v ey by t he Pr incess Roy al Tr ust for Car er s
r epor t ed t hat car ing left t hem no t im e t o look aft er t heir ow n healt h ( Keeley and Clarke, 2002) , findings t hat have been report ed elsewhere ( Cunningham and Dick, 1995; Rogers et al., 1998) . Resear ch show s t hat t he m or e
dem anding t he car e is, t he less likely it is t hat car er s w ill have t im e t o seek help in r elat ion t o t heir ow n healt h ( Act on, 2002) . ‘Sym pt om cont ainm ent ’ can be a feat ur e of t he pr essing need t o fulfil t he r out ine t ask s associat ed w it h car e and dom est ic w or k ( Roger s et al., 1998) .
I t is k now n t hat car er s’ help- seek ing act iv it ies inv olv e act iv ely engaging w it h: inform al and form al ‘m ediat ors’ ( Cot rell and Engel, 1998; Rogers et al., 1998) ; com m unit y pharm acist s ( Harris et al., 1998) ; pr ofessionals inv olv ed w it h car e r ecipient s, such as day hospit al st aff ( Walder , 1995) ; t elephone adv ice lines ( Mahoney et al. , 2001) ; and com put er- based services providing inform at ion and ‘in- hom e’ support groups ( Gallienne et al., 1993; Magnusson et al., 2002) . These st udies confir m ev idence point ing t o t he im por t ance of t he social
1 . 3 Policy con t e x t
The closur e of long- st ay hospit als and t he gr ow ing pr essur e t o suppor t people wit hin t heir own hom es or in t he com m unit y has led t o increasing governm ent reliance on inform al care provided wit hin t he fam ily ( St alker, 2003) . Care in t he com m unit y has raised t he profile of unpaid, fam ily caring; fam ily caring is not new , but m ak ing it cent r al t o gov er nm ent policy focuses a spot light on it ( Brechin et al. , 2003) .
I n r ecognit ion of t he im por t ant cont r ibut ion car er s m ak e t o societ y , t he last t en year s has w it nessed a gr ow ing em phasis on suppor t ing car er s in t heir car ing r ole. This is im por t ant because r ecent t r ends indicat e t hat m or e individuals are likely t o be heavily involved in providing longer periods of care ( Hirst and Hut t on, 2000) . During a t ypical life span, six out of t en individuals are likely t o assum e ‘heavy’ caring responsibilit ies ( 20 hours or m ore per week) at som e point in t heir lives ( Hirst and Hut t on, 2000) . The governm ent is com m it t ed t o ensur ing t hat t he NHS and Social Ser v ices should help car er s m aint ain t heir healt h ( Depart m ent of Healt h, 1999a) . I n 1999, t he governm ent published it s nat ional st r at egy for car er s, Car ing about Car er s ( Depart m ent of Healt h, 1999a) . The st r at egy ident ifies infor m at ion, suppor t and car e as cr ucial t o car er s. I t addr esses t he possibilit y t hat car er s m ight neglect t heir ow n healt h because t hey ar e focusing on t he car e t hey pr ov ide r at her t han on t he car e t hey m ight need t hem selv es. I t st at es t hat ‘Car er s hav e a r ight t o see t heir ow n healt h needs m et . They need help t o m aint ain t heir ow n healt h, bot h physical and em ot ional’ ( Depart m ent of Healt h, 1999a: 55) . The Carers Special Grant , ring- fenced m onies t hat local aut hor it ies can apply for , aim s t o
st im ulat e t he pr ov ision of innov at iv e r espit e car e and shor t br eak s t o giv e carers t im e out from caring.
Mor e r ecent ly , t he Carers and Disabled Children Act 2000 st rengt hened carers’ r ight s under t he Car er s ( Recognit ion and Ser v ices) Act 1995 t o an assessm ent of t heir ow n abilit y t o pr ov ide car e w her e t hey pr ov ide ( or int end t o pr ov ide) subst ant ial am ount s of car e on a r egular basis. Th e pr act ice gu idan ce t o t h e new Act em phasises t he k ey r ole t hat GPs and ot her pr im ar y car e st aff play in suppor t ing car er s ( Depar t m ent of Healt h, 2000b) . St andar d Tw o of t he
Nat ional Ser vice Fr am ew or k for Older People st r esses t he im por t ance of good inform at ion for carers, point ing out t hat w it hout inform at ion carers are m ore lik ely t o suffer fr om st r ess and consequent ly be less able t o cont inue t o car e ( Depart m ent of Healt h, 2001) .
The int ent ion t hat car er s obt ain qualit y pr im ar y, secondar y and specialist healt h car e ser v ices is not necessar ily r ealised in pr act ice. Recent r esear ch int o car er s’ ex per iences of t he NHS suggest s t hat alt hough car er s ar e in r egular t ouch w it h t he NHS and v alue t he r ecognit ion and suppor t t h ey receive, m any st ill feel ‘ignored and invisible’ and t hat t heir ow n needs for healt h car e ar e over looked ( Henw ood, 1998) .
Giv en how v it al good healt h car e is for car er s, it is im por t ant t o ident ify obst acles t h at st an d in t h e w ay of car er s accessing and ut ilising effect iv e ser vices. To t his end, t he NHS Ser vice Deliver y and Or ganisat ion ( SDO) Research and Developm ent Program m e com m issioned research int o t he pr oblem s and bar r ier s t o access t o healt h car e for car er s, and effect iv e int er v ent ions t o r e m edy v ar iat ions. The r esear ch t eam w as led by t he Social Policy Resear ch Unit ( SPRU) at t he Univ er sit y of Yor k , w or k ing in conj unct ion w it h t he pr im ar y and com m unit y car e consult ancy Act on.Shapir o. This r epor t pr esent s t he st udy findings.
1 .4 Aim s a n d obj e ct iv e s of st u dy
The overall aim of t he st udy w as t o inform t he SDO program m e about t heory and ev idence on car er s’ access t o healt h car e. Under pinning t his aim w er e t w o k ey obj ect iv es:
• t o exam ine t he evidence from UK and int ernat ional research ( published and
unpublished) in order t o ident ify:
– t he pr oblem s and bar r ier s w hich car er s exper ience in accessing healt h car e ser v ices ( including healt h pr om ot ing and pr ev ent iv e ser v ices) , and any associat ed issues r elat ing t o equit y of access and lev el of unm et need
– ev iden ce of specific, pr act ical an d effect iv e in t er v en t ion s t h at can im pr ov e car er s’ access t o healt h car e ser v ices, and how t hese appr oaches v ar y accor ding t o t he car er ’s age and cir cum st ances.
• t o consult w it h k ey st ak eholder s, not ably car er s’ gr oups, m aj or volunt ary or ganisat ions and nat ional and local st at ut or y bodies w it h an int er est in access t o healt h car e, about bot h t he findings fr om t he lit er at ur e r ev iew and recom m endat ions for furt her research.
This r epor t docum ent s bot h t he findings fr om t he lit er at ur e r ev iew and t he consult at ion. We included a t ot al of 46 prim ary st udies and report s in t he r ev iew ; of t hese, 32 ident ified bar r ier s t o healt h car e for car er s w hile t he rem aining 14 com pr ised ev aluat ions of int er v ent ions designed t o ov er com e t hese obst acles. As w ill be seen, com m on t hem es and issues em erged from t he r ev iew and t he consult at ion ex er cise. Based on t he ev idence fr om t he r ev iew and t he account s collect ed dur ing t he consult at ion, w e pr ov ide insight s int o t he ar eas w her e t her e ar e gaps in k now ledge, com m ent on t he st r engt h of t he ev idence base, m ak e r ecom m endat ions for fut ur e r esear ch and suggest
st r at egies t o im pr ov e accessibilit y for car er s. We fur t her dev elop t he
r efined v er sion show s addit ional issues specifically r elat ing t o access t o healt h car e for car er s.
1 .5 St r u ct u r e of t h e r e p or t
The r epor t is or ganised as follow s.
• Ch apt er 2 discusses t he m et hods adopt ed for t he lit er at ur e r ev iew and consult at ion r espect iv ely .
• Chapt er 3 docum ent s t he ev idence fr om t he lit er at ur e r ev iew and t he consult at ion about obst acles t o car er s’ access t o pr im ar y car e, hospit al-based car e, scr eening program m es, respit e care and short breaks. I t m akes a st ar t on pr esent ing ideas about pr act ical solut ions and r em edial act ion t o im pr ov e access for car er s.
• Chapt er 4 pr esent s t he findings fr om t he r ev iew of t he lit er at ur e and t he consult at ions about int er v ent ions aim ed at helping car er s gain access t o healt h car e. The r ange of int er v ent ions com pr ises: pr im ar y car e init iat iv es; com m unit y- based init iat ives; hom e - based healt h car e pr oj ect s
( t elephone- and com put er- based t echnologies and com plem ent ar y t her apies) ; and geogr aphical infor m at ion syst em s ( GI S) soft w ar e.
Chapt er 2 Research m et hods
2 .1 I n t r od u ct ion
A t hor ough lit er at ur e r ev iew w as conduct ed w it h adv ance decisions m ade about how t he lit er at ur e w ould be found, appr aised and collat ed. A pr ot ocol guided t he review process, w hich aim ed t o m inim ise bias in t he present at ion of t he findings, and ensur e t hat our int ent ions w er e t r anspar ent and ex plicit . This chapt er set s out how t he st udies pr esent ed w er e chosen for inclusion in t he r ev iew . I t r epor t s on t he v ar ious st ages of t he pr ocess, fr om defining t he quest ion, sear ching for ev idence, apply ing t he inclusion cr it er ia, appr aising t he st r engt h of t he ev idenc e and sy nt hesising t he findings of t he final select ion of st udies. I t also set s out how t he com plem ent ar y consult at ion ex er cise w as con du ct ed.
2 .2 Th e r e v ie w p r ot ocol
2 .2 .1 The que st ion
The r ev iew quest ion w as ‘What does t he r esear ch ev idence t ell us abou t w h at r est r ict s, w hat pr om ot es and w hat im pr ov es car er s’ access t o healt h car e ser v ices?’ The r ev iew t eam spent t im e dev eloping an under st anding of t he quest ion as it infor m ed each st age of t he r ev iew pr ocess. The focus w as on car er s’ access t o ser v ices t hat ar e pr ov ided in any set t ing and dir ect ly addr ess t heir own physical and m ent al healt h needs as individuals, which m ay or m ay not r elat e t o t heir r ole as a car er s. These ser v ices m ay pr om ot e t he healt h of carers or play a role in prevent ing t heir ill healt h . I t w as an t icipat ed t h at clear boundar ies ar ound t he lit er at ur e w ould not alw ay s be possible, so int er t w ined is t he per son’s r ole as a car er w it h t heir ow n needs. The r ev iew t eam how ev er w or k ed on t he basis t hat , for ex am ple, st udies focusing on access t o ser v ices t hat pr ov ided educat ion t o t he car er on cor r ect lift ing t echniques t o pr ev ent back inj ur ies w ould be included, but st udies ex am ining access t o t hose ser v ices pr ov iding t r aining in t he cor r ect inser t ion of cat het er t ubes for t he car e r ecipient w ould not . Wit hin t his, it is ack now ledged t hat lack of
infor m at ion about t he car e r ecipient ’s healt h and cir cum st ances and how t o m anage t he car e pr ov ided adds t o car er st r ess and cont r ibut es t o car er s’ ill healt h ( Depart m ent of Healt h, 1999a) .
possible solut ions, since t her e is a paucit y of r igor ous ev idence dem onst r at ing posit iv e h ealt h- r elat ed out com es.
2 .2 .2 Se a r ch st r a t e gy
Resear ch ev idence w as ident ified using a num ber of channels, show n in Table 2.1.
Ta ble 2 .1 I de n t ifyin g r e se a r ch
• Sear ch es of ap p r op r iat e elect r on ic d at ab ases • Ref er en ce ch eck in g of ar t icles r et r iev ed • Sear ch in g f or pu blicat ion s of k ey au t h or s
• Cit at ion sear ch in g on Social Scien ce Cit at ion I n dex ( SSCI ) • Ch eck in g r elev an t I n t er n et sit es
• Con su lt at ion w it h k ey n at ion al an d local or g an isat ion s • Con t act w it h k ey r esear ch er s in t h e f ield
• Con t act in g lead r esear ch er s id en t if ied f r om t h e Nat ion al Resear ch Reg ist er • Con su lt in g specialist libr ar ies
• Op en r eq u est f or r ef er en ces on JI SCMail sit es
• Han d sear ch in g of j ou r n als ( Medical Jou r n al of Au st r alia, Healt h an d Social Car e in t h e Com m unit y , Jour nal of Pu blic Healt h Medicin e)
The r eview t eam included an infor m at ion scient ist fr om t he Cent r e for Review s and Dissem inat ion ( CRD) who was inst rum ent al in developing t he elect ronic sear ch st r at egies. The follow ing dat abases w er e sear ched for r efer ences for relev ant st udies w it h a r ange of k ey w or ds and sear ch st r at egies.
CD - ROM d a t a b a se s
• Cochrane Cont rolled Trials Regist er ( CCTR)
• Cochr ane Dat abase of Sy st em at ic Rev iew s ( CDSR)
• Nat ional Research Regist er ( NRR)
D a t a ba se s on Silv e r Pla t t e r
• Brit ish Nursing I ndex (BNI )
• CI NAHL
• EMBASE
• Healt h Managem ent I nform at ion Consort ium ( HMI C) ( HELMI S, DHdat a and
t he King’s Fund dat abases)
• MEDLI NE and PREMEDLI NE
• Syst em for I nform at ion on Grey Lit erat ure in Europe ( SI GLE)
Fr e e w e b d a t a b a se s
• Car edat a – ht t p: / / w w w . elsc. or g. uk / bases_ floor / car edat a. ht m
• Dat abase of Abst r act s of Rev iew s of Effect iv eness ( DARE)
ht t p: / / agat ha. y or k . ac. uk / w elcom e. ht m
• Healt h Technology Assessm ent Dat abase ( HTA)
ht t p: / / agat ha. y or k . ac. uk / w elcom e. ht m
• NHS Econom ic Evaluat ion Dat abase ( NHS EED)
ht t p: / / agat ha. y or k . ac. uk / w elcom e. ht m
• Social, Psychological, Educat ional and Crim inological Trials Regist er
( SPECTRE) – ht t p: / / 128.91.198.137/
Subscript ion- on ly w e b d a t a b a se s
• Planex – ht t p: / / w w w . planex . ndir ect . co. uk / v alidat e2.asp?url= / default .asp
D a t a b a se s on BI D S
• Psy chI NFO – ht t p: / / w w w . bids. ac. uk /
• I nt er nat ional Bibliogr aphy of t he Social Sciences ( I BSS) –
ht t p: / / w w w . bids. ac. uk /
D a t a ba se s on W e b of Scie n ce
• Social Science Cit at ion I ndex ( SSCI ) – ht t p: / / w os.m im as.ac.uk/
D a t a ba se s on OV I D W e b
• Allied and Com plem ent ary Medicine Dat abase ( AMED) –
ht t p: / / gat ew ay .uk .ov id.com /
Ta ble 2 .2 I n t e r n e t sit e s se a r ch e d
Healt h Dev elopm en t Agen cy ht t p: / / w w w .hda- online. or g. uk /
Car er s UK w w w . car er son lin e. or g. u k ,
Depar t m en t of Healt h Car er s sit e ht t p: / / w w w . car er s. gov . uk /
Car er s Nat ion al Associat ion Nor t h er n I r elan d ht t p: / / w w w . car er sni. or g/ suppor t . ht m l
Pr in cess Roy al Tr u st f or Car er s w w w . car er s. or g
Con t act- a- Fam ily w w w . cafam ily . or g. uk
Cr ossr oad s w w w . cr ossr oads. or g. u k ,
Alzh eim er s Societ y w w w . alzh eim er s. or g. u k
Nat ion al Pr im ar y Car e Dev elop m en t Team w w w .ndpt .or g
Nat ion al Pr im ar y Car e Resear ch an d Dev elopm en t Cen t r e
w w w . npcr dc. m an. ac. uk
Pr im ar y Car e at t h e Depar t m en t of Healt h w w w . doh. gov . uk / pr icar e/ index . ht m
Roy al College of Gen er al Pr act it ion er s w w w . r cgp. or g. uk /
Roy al College of Nu r sin g w w w . r cn. or g. uk
HAZ n et w w w . haznet . or g. uk
Doct or Pat ient Par t ner ship w w w . dpp. or g. uk
Ch ildr en ’s Societ y ht t p: / / w w w .t he- childr ens- societ y . or g. u k /
Ment al Aft er Car e Associat ion ( MACA) ht t p: / / w w w .m aca.or g.uk / int r o.ht m
Mak in g Space ht t p: / / w w w . m ak ingspace. co. uk /
Ret hink ht t p: / / w w w . r et hink . or g/
Healt h Car e f or Car er s w w w . h ealt h car efor car er s. co. u k
Relev ant I nt er net sit es, display ed in Table 2.2, w er e sear ched and pr ov ided em pir ical m at er ial and r epor t s t hat ser ved as useful background inform at ion. The r efer ences of all lit er at ur e r eceiv ed w er e check ed for cit at ions t hat had not appear ed in our init ial r efer ence set . Key r esear cher s in t he field,
subscr iber s t o online discussion boar ds, and t he local and nat ional
or ganisat ions cont act ed in t he consult at ion ex er cise w er e ask ed t o ident ify r elevant r esear ch r epor t s. This pr oved useful in ident ifying som e addit ional st udies, especially local ev aluat ions of pr oj ect s, and aided t he ident ificat ion of int er v ent ions for t he local consult at ion. The King’s Fund library w as also visit ed t o obt ain docum ent s and sour ce supplem ent ar y r efer ences, in addit ion t o t heir dat abase being sear ched. Cit at ion sear ches w er e car r ied out on SSCI for a handful of k ey r efer ences.
[image:24.596.69.537.85.465.2]2 .2 .3 St udy select ion
Ther e w er e t hr ee st ages for a st udy t o go t hr ough befor e it w as included in t he final lit er at ur e r ev iew :
• a check for pot ent ial r elev ance, so t hat only ar t icles w er e or der ed t hat had t he pot ent ial t o answ er t he r ev iew quest ion
• a check t hat t he r ev iew inclusion cr it er ia had been m et , so t hat t he st udy pr ov ided dir ect ev idence t o addr ess t he quest ions posed
• a check for qualit y , t o ensur e t hat t he resear ch findings w er e gener ally sound.
Tw o r ev iew er s scanned t he t ot al r efer ences t o check for pot ent ial r elev ance, double - check ing t he init ial 15 per cent t o ensur e consist ency in decision-m ak ing. Wher e t he abst r act or t it le indicat ed t hat it r elat ed br oadly t o car er s and healt h ser v ices, t he r epor t w as obt ained. I f it w as not possible t o
ascer t ain t he st udy ’s pot ent ial v alue t o t he r ev iew fr om t he t it le or abst r act , t he ar t icle w as st ill r et r iev ed and decisions m ade on t he full t ex t . Many
r efer ences w er e clear ly not appr opr iat e and had been br ought for w ar d because of t he soft nat ur e of t he t er m s used in social car e, but t he qualit y of
abst r act ing on som e dat abases w as poor , m eaning addit ional r esour ces w er e em ployed in obt aining st udies w hen st r uct ur ed abst r act s w ould hav e pr oduced m or e accur at e init ial decisions.
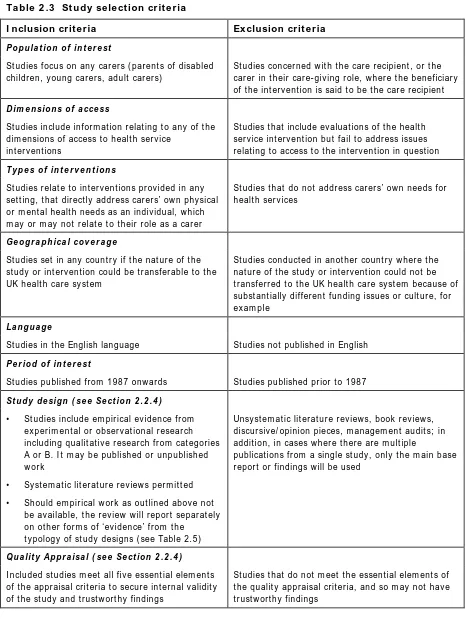
Tw o r ev iew er s t hen check ed all of t he r et r iev ed st udies against t he inclusion cr it er ia pr esent ed in Table 2.3. Of t hese decisions, 80 per cent w er e double check ed t o ensur e t hat t he r esear ch st udies w ere eligible for inclusion. The cr it er ia w er e found useful in placing boundar ies ar ound lit er at ur e t hat focused on answ er ing t he r ev iew quest ion, and ensur ed consist ent applicat ion acr oss t he m em bers of t he t eam . Any disagreem ent s regarding t hese decis ions w er e r esolved consensually in t he w ider t eam .
I nt er nat ional st udies w er e r et r iev ed and assessed for r elev ance t o t he UK healt h car e sy st em . St udies t hat addr essed aspect s of Medicar e or MediAid in t he Unit ed St at es, for exam ple, or r ur al healt h issues in developing count r ies, w er e not put for w ar d for r ev iew . Those t hat addr essed univ er sal issues of access t o healt h for car er s in dev eloped count r ies w er e put for w ar d. While no r est r ict ions w er e placed on t he sear ch, t r anslat ing non- English language st udies w as bey ond t he scope of t his r ev iew , alt hough w e ar e aw ar e of t he bias t his m ay int r oduce int o t he r epor t ed findings. Ver y few for eign- language r efer ences w er e pr oduced, but it r em ains unk now n w het her t hey m ay hav e affect ed t he findings of t he r ev iew .
Ta ble 2 .3 St u dy se le ct ion cr it e r ia
I nclusion crit eria Ex clusion cr it e r ia
P o p u la t io n o f in t e r e st
St u dies f ocu s on an y car er s ( par en t s of disabled ch ildr en , y ou n g car er s, adu lt car er s)
St udies concer ned w it h t he car e r ecipient , or t he car er in t h eir car e- giv in g r ole, w h er e t h e ben eficiar y of t he int er v ent ion is said t o be t he car e r ecipient
D im e n sio n s o f a cce ss
St udies include infor m at ion r elat ing t o any of t he dim en sion s of access t o h ealt h ser v ice
int er v ent ions
St udies t hat include ev aluat ions of t he healt h ser v ice in t er v en t ion bu t fail t o addr ess issu es r elat ing t o access t o t he int er v ent ion in quest ion
T y p e s o f i n t e r v e n t i o n s
St udies r elat e t o int er v ent ions pr ov ided in any set t ing, t hat dir ect ly addr ess car er s’ ow n phy sical or m ent al healt h needs as an indiv idual, w hich m ay or m ay n ot r elat e t o t h eir r ole as a car er
St u dies t h at do n ot addr ess car er s’ ow n n eeds for h ealt h ser v ices
Ge o g r a p h i ca l co v e r a g e
St udies set in any count r y if t he nat ur e of t he st udy or int er v ent ion could be t r ansfer able t o t he UK h ealt h car e sy st em
St udies conduct ed in anot her count r y w her e t he nat ur e of t he st udy or int er v ent ion could not be t r an sfer r ed t o t h e UK h ealt h car e sy st em becau se of subst ant ially differ ent funding issues or cult ur e, for ex am p le
La n g u a g e
St udies in t he English language St udies not published in English
P e r i o d o f i n t e r e st
St udies published fr om 1 9 8 7 onw ar ds St udies published pr ior t o 1987
St u d y d e sig n ( se e Se ct io n 2 . 2 . 4 ) • St u dies in clu de em pir ical ev iden ce fr om
ex p er im en t al or obser v at ion al r esear ch in clu din g qu alit at iv e r esear ch fr om cat egor ies A or B. I t m ay be pu blish ed or u n pu blish ed w or k
• Sy st em at ic lit er at u r e r ev iew s per m it t ed
• Sh ou ld em pir ical w or k as ou t lin ed abov e n ot be av ailable, t h e r ev iew w ill r epor t separ at ely on ot h er f or m s of ‘ev iden ce’ f r om t h e
t y pology of st u dy design s ( see Table 2 . 5 )
Un sy st em at ic lit er at u r e r ev iew s, book r ev iew s, discur siv e/ opinion pieces, m anagem ent audit s; in addit ion, in cases w her e t her e ar e m ult iple
publicat ions fr om a single st udy , on ly t h e m ain base r epor t or findings w ill be used
Q u a lit y Ap p r a isa l ( se e Se ct io n 2 . 2 . 4 ) I n clu ded st u dies m eet all fiv e essen t ial elem en t s of t he appr aisal cr it er ia t o secur e int er nal v alidit y of t he st udy and t r ust w or t hy findings
[image:26.596.65.531.74.709.2]2 .2 .4 St r e ngt h of e vide nce
I t is im por t ant t hat t he conclusions and r ecom m endat ions of t he pr esent r epor t ar e based on t he best ev idence av ailable, but t his does not m ean r epor t ing only ‘ideal t ype’ r esear ch. Em pir ical st udies w er e chosen in w hich t he r esear ch design and it s conduct could be assum ed t o offer a r easonable lev el of confidence in t he r esult s. These decisions ensur ed t he st udies m et a basic qualit y t hr eshold, and t hat t he st udies w er e designed in such a w ay as t o r epr esent good r esear ch inquir y.
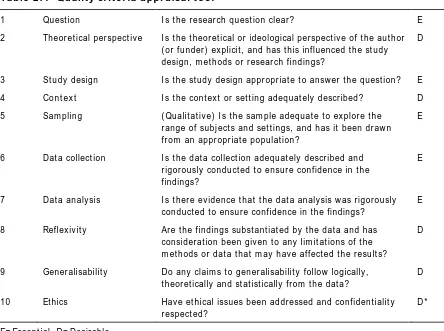
A qualit y cr it er ia t ool dev eloped by Cr oucher et al. ( 2003) w as chosen t o est ablish w het her a st udy m et t he qualit y t hr eshold. Ther e is lit t le consensus ov er t he use of appr aisal t ools in r ev iew s, and t his t ool w as adopt ed because r eview er and r eader s alike can r eadily under st and it ; it includes guidance on it s pr act ical applicat ion and is not r esour ce int ensiv e. The set of cr it er ia is
pr esent ed in Table 2. 4. One r ev iew er applied t hese cr it er ia t o each st udy t hat m et t he inclusion cr it er ia and t hose t hat m et t he ‘essent ial’ elem ent s w er e put for w ar d for t he final r ev iew . A second r ev iew er check ed 20 per cent of t hese decisions.
Ta ble 2 .4 Qu a lit y cr it e r ia a ppr a isa l t ool
1 Quest ion I s t h e r esear ch qu est ion clear ? E
2 Th eor et ical per spect iv e I s t h e t h eor et ical or ideological per spect iv e of t h e au t h or ( or funder ) ex plicit , and has t his influenced t he st udy design , m et h ods or r esear ch fin din gs?
D
3 St udy design I s t he st udy design appr opr iat e t o answ er t he quest ion? E
4 Con t ex t I s t he cont ex t or set t ing adequat ely descr ibed? D
5 Sam plin g ( Qu alit at iv e) I s t h e sam ple adequ at e t o ex plor e t h e r ange of subj ect s and set t ings, and has it been dr aw n f r om an appr opr iat e populat ion?
E
6 Dat a collect ion I s t h e dat a collect ion adequ at ely descr ibed an d r igor ou sly con du ct ed t o en su r e con fiden ce in t h e findings?
E
7 Dat a an aly sis I s t h er e ev iden ce t h at t h e dat a an aly sis w as r igor ou sly con du ct ed t o en su r e con fidence in t he findings?
E
8 Reflex iv it y Ar e t he findings subst ant iat ed by t he dat a and has
consider at ion been giv en t o any lim it at ions of t he m et h ods or dat a t h at m ay h av e affect ed t h e r esu lt s?
D
9 Gener alisabilit y Do an y claim s t o gen er alisabilit y follow logically , t heor et ically and st at ist ically fr om t he dat a?
D
10 Et hics Hav e et h ical issu es been addr essed an d con fiden t ialit y
r espect ed?
D *
E= Essen t ial, D= Desir able
* I n som e sen sit iv e fields, et h ical appr ov al an d con sider at ion s m ay be essen t ial.
[image:27.596.71.515.362.693.2]All r esear ch st udies t hat ent er ed t he r ev iew w er e t hen classified using a t y pology of st udy design ( Table 2.5 below ) adapt ed fr om t hat used in t he Nat ional Service Fram ework for Older People ( Depart m ent of Healt h, 2001) . This provided an indicat ion of w hat t y pe of ev idence infor m ed t he findings pr esent ed. I t w as int ended t hat r esear ch fr om cat egor ies A and B w ould be included in t he final r ev iew ed ar t icles because t hey w er e t he m ost r igor ous st udies, unless ot her st udies w er e able t o fill gaps found in t he ev idence base. The use of C1 t y pe ev idence w as used t o ex plor e gaps r elat ing t o t he bar r ier s faced by differ ent t y pes of car er s, and in t he r epor t ing of int er v ent ions, due t o t he lack of m or e r igor ous r esear ch in t hese ar eas.
I t w as appr opr iat e t o r ev iew differ ent t y pes of r esear ch t o infor m t he set of quest ions guiding t his r ev iew . The st udy t y pology classificat ion w as at t r act iv e, because of it s r ecognit ion of t he v alue of good qualit at iv e st udies. How ev er , it w as found t hat consider a t ion of t he st r engt h t hat a cer t ain st udy design can offer should r elat e t o t he par t icular quest ion and line of inquir y . St udies per ceived t o hold gr eat er int er nal validit y m ay have less ext er nal validit y, so reducing t heir ut ilit y t o t he review. For exam p le, ‘t reat m ent ’ groups in
ex per im ent al st udies w er e pr ov ided w it h specific int er v ent ions ( such as com put er- based t echnology or hom e - based m assage t r eat m ent s) designed specifically for t hat par t icular st udy . Conclusions fr om t hese st udies, alt hough pr ecise, can lim it t heir r elat ionship w it h cur r ent pr act ice. Also, t he
t r ansfer abilit y of t he st udies fr om an exper im ent al set t ing t o a nat ur al one m ay pose problem s. St udies w it h large convenience sam ples m ay be w holly
Ta ble 2 .5 Ty pology of st u dy de signs
Evide n ce fr om e m pir ica l r e se a r ch a n d ot h e r pr ofe ssion a l lit e r a t u r e
Ev id e n ce t y p e co d e Ex a m p l e s o f st u d y t y p e
A1 Sy st em at ic r ev iew s w h ich in clu de at least on e r an dom ised con t r olled t r ial ( RCT) ( e. g. Sy st em at ic Rev iew s f r om Coch r an e or Cen t r e f or Rev iew s an d Dissem in at ion )
A2 Ot her sy st em at ic and high- qu alit y r ev iew s w h ich sy n t h esise r ef er en ces
B1 I n div idu al RCTs
B2 I ndiv idual non- r andom ised, ex per im ent al/ int er v ent ion st udies
B3 I ndiv idual non- ex per im ent al st udies, cont r olled st at ist ically if
appr opr iat e; includes st udies using case cont r ol, longit udinal, cohor t , m at ch ed pair s, or cr oss- sect ion al r an dom sam ple m et h odologies, an d sound qualit at iv e st udies; analy t ical st udies including secondar y analy sis
C1 Descr ipt iv e an d ot h er r esear ch or ev aluat ion not in B
Evide n ce fr om e x pe r t opin ion ( in t h e a bse n ce of e m pir ica l r e se a r ch e vide n ce )
Ev id e n ce t y p e co d e Ex a m p l e s o f st u d y t y p e
C2 Case st u dies an d ex am ples of good pr act ice
D Su m m ar y r ev iew ar t icles an d discu ssion s of r elev an t lit er at u r e an d con fer en ce pr oceedin gs n ot ot h er w ise classified
E Pr ofession al opin ion based on pr act ice, or r epor t s of com m it t ees
U User opin ion f r om car er s or car er s or gan isat ion s
Sour ce: adapt ed fr om Nat ional Ser v ice Fr am ew or k for Older People ( Depar t m ent of Healt h, 2001)
An Access dat abase w as used t o m anage dat a ex t r act ion for m s, pr esent ed in Appendix 3. The dat abase r ecor ded a unifor m set of infor m at ion for each st udy t hat m et t he inclusion cr it er ia. All r ev iew er s used t he dat a ex t r act ion for m t o en su r e con sist ency and ease of com par ison bet w een st udies. The ex t r act ion of t he subst ant iv e cont ent of t he st udies w as based ar ound t he bar r ier s t hat hinder ed access t o healt h car e and t he possible solut ions and int er v ent ions designed t o ov er com e t hese. I t w as im por t ant t o consider t he applicabilit y of int er v ent ions t o ot her set t ings, and so ev idence r elat ing t o an int er v ent ion’s st r uct ur e, pr ocess and out com es w as ex t r act ed w it h a v iew t o ident ify ing t he st r engt hs and w eak nesses of t he int er v ent ions ( Wagner and Guild, 1989) .
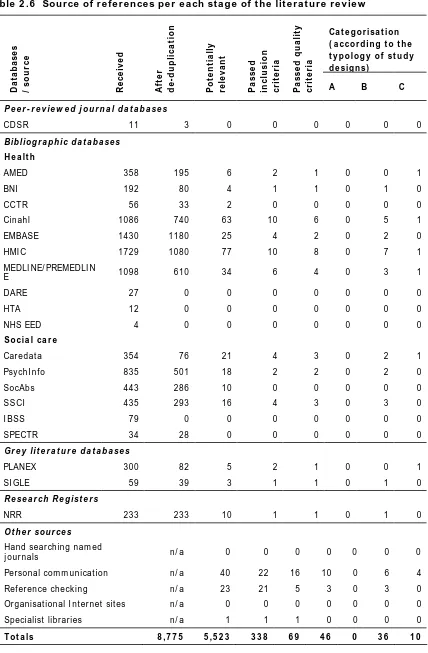
2 .3 Re f e r e n ce s r e t r ie v e d
Th e sear ch pr ocess pr oduced 8775 r efer ences. Once duplicat e r efer ences w ere rem oved, 5523 st udies rem ained and som e 338 of t hese w ere found t o be gener ally r elev ant t o t he r ev iew . Of t hese, 69 passed t he inclusion cr it er ia; 46 of t hese m et t he qualit y t hr eshold; 36 and 10 st udies r espect iv ely w er e cat egor ised as pr esent ing B- t y pe and C- t y pe ev iden ce accor din g t o t h e t y pology of st udy designs ( Table 2. 5) . Ther e w er e no st udies cont aining A-t y pe ev iden ce.
We felt t hat t he findings of t he r em aining 23 st udies, concent r at ed in t he C1 and C2 cat egor ies, w er e insufficient ly t r ust w or t hy . Ther e w er e a v ar iet y of r easons t o ex plain w hy t hey w er e ex cluded. For inst ance, t her e w er e ex am ples of poor ly focused st udies t hat w er e unclear about w hat r esear ch quest ions w er e being asked, w hich in t ur n cast doubt on t he appr opr iat eness of t he r esear ch m et hods and st udy sam ple. I n som e cases, t he r igour w it h w hich t he r esear ch had been conduct ed w as quest ionable. Ther e w as an inst ance, for exam ple, w her e r esear cher s ident ified lar ge discr epancies in ( quant it at iv e) dat a collect ed by st udy par t icipant s. Aut hor s t hem selv es r epor t ed w eak nesses in st udies, for exam ple pr oblem s w hen conduct ing int er view s; t he dynam ics of focus groups inhibit ing som e part icipant s from expressing t heir views; running ou t of t im e and not being able t o com plet e all t he int erviews planned; sm all and/ or unr epr esent at iv e sam ple sizes. I n ot her st udies, it w as not ev ident how t he analy sis had been car r ied out ; few , if any , det ails w er e included and it w as unclear w het her all of t he dat a had been included in t he analy sis, or w het her t he r esear cher s had been select iv e. Som e account s w er e sum m ar ies of pr im ar y r esear ch r epor t s w r it t en by a t hir d par t y , w ho in t ur n select ed w hat t o include and w hat t o ex clude ( oft en, det ails about r esear ch m et hods) in t he account , a pr ocess w hich led t o quest ions about t he aut hor it y of t he w or k . Effor t s t o obt ain t he pr im ar y r epor t s w er e gener ally unsuccessful; any w e did m anage t o obt ain w er e ent er ed int o t he r ev iew pr ocess independent ly . Ot her ar t icles w er e r epor t s of ear ly findings fr om st udies st ill t o be com plet ed.