FOCUSED NURSING INTERVENTIONS ON
KNOWLEDGE AND FUNCTIONAL HEALTH
PROBLEMS AMONG OLDER ADULTS AND
THEIR CAREGIVERS AT SELECTED
RURAL COMMUNITY SETTING
THESIS
Submitted to
THE TAMIL NADU Dr.M.G.R MEDICAL UNIVERSITY, CHENNAI
for the award of the degree of
DOCTOR OF PHILOSOPHY
IN
NURSING
By
Mrs.M.SUMATHI, M.Sc(Nursing)
FOCUSED NURSING INTERVENTIONS ON
KNOWLEDGE AND FUNCTIONAL HEALTH
PROBLEMS AMONG OLDER ADULTS AND
THEIR CAREGIVERS AT SELECTED
RURAL COMMUNITY SETTING
THESIS
Submitted to
THE TAMIL NADU DR.M.G.R MEDICAL UNIVERSITY, CHENNAI
for the award of the degree of
DOCTOR OF PHILOSOPHY
IN
NURSING
By
Mrs.M.SUMATHI, M.Sc(Nursing)
Under the Guidance of
Dr. REVATHY VIJAYALAKSHMI, M.D., Ph.D.,
COMMUNITY HEALTH NURSING DEPARTMENT
OMAYAL ACHI COLLEGE OF NURSING
CHENNAI – 600 066
FOCUSED NURSING INTERVENTIONS ON
KNOWLEDGE AND FUNCTIONAL HEALTH
PROBLEMS AMONG OLDER ADULTS AND
THEIR CAREGIVERS AT SELECTED
RURAL COMMUNITY SETTING
THESIS
Submitted to
THE TAMIL NADU DR.M.G.R MEDICAL UNIVERSITY, CHENNAI
for the award of the degree of
DOCTOR OF PHILOSOPHY
IN
NURSING
By
Mrs.M.SUMATHI,
M.Sc(Nursing)
Guided By
Dr. REVATHY VIJAYALAKSHMI, M.D., Ph.D.,
Ph.D RESEARCH GUIDE
COMMUNITY HEALTH NURSING DEPARTMENT
OMAYAL ACHI COLLEGE OF NURSING
I wish to express my deep sense of gratitude to the Vice Chancellor and Research Department of the Tamil Nadu Dr.M.G.R.Medical University, Guindy, Chennai, for giving me an opportunity to undertake my Ph.D. in Nursing at this esteemed University.
I greatly value and express my deep sense of gratitude to Mrs.Valli Alagappan, Managing Trustee & Chairperson Governing Council, Mr.A.R.Kasiviswanathan, Member Trustee and Mrs.Seetha Subbiah, Member Trustee for giving me an opportunity to pursue the study and for extending the needed help.
I extend my sincere gratitude to Dr.Revathy Vijayalakshmi, MD, Ph.D., Research Guide, Omayal Achi College of Nursing, for her untiring support, scholastic suggestions and constant encouragement in the completion of my thesis. She has been instrumental in inspiring me throughout my Ph.D pursuit. Her thought provoking ideas, academic & clinical brilliance and honest approach molded me to gain confidence for the completion of my study.
Doc., Principal and Research Director, ICCR, Omayal Achi College of Nursing, for giving me an opportunity to pursue the Ph.D.Nursing, for being a backbone for my research study. She contributed and enriched my knowledge with research. A special bouquet of thanks for contributing her time, effort and ideas for developing this research study from womb to tomb stage, for permitting and sponsoring me to attend various national and international conference on geriatric care, providing forum for presenting my research study report in International Conferences. Each and every step of my research study is mended with her thought provoking ideas. She provided untiring support, motivation, suggestion and encouragement in the completion of this thesis.
I am immensely grateful to the Advisory Committee Members Dr.A.Judie, M.Sc(N), Ph.D., and Dr.Susila, M.Sc(N), Ph.D., for their efficient guidance, thought provoking ideas and untiring spirit which capacitated me to execute this study.
I extend my deep sense of gratitude to the Dr.D.Celina, M.Sc(N), Ph.D., Vice Principal, Omayal Achi College of Nursing for rendering her invaluable ideas, support, guidance, suggestion throughout my study. I also thank her for validating my content and suggesting the necessary changes to refine the data collection instrument. I also thank her for her creativity and excellence in preparing the flashcards for the research study through the IEC department.
Nursing for efficient guidance and ethical approval for conducting the research study.
My deepest gratitude to Dr. Venkatesan, M.Sc., M.Phil., Ph.D Biostatistician, for his efficient guidance and assistance which has meant more to me than I could ever express.
My sincere thanks to Dr.V.S.Natarajan, Geriatric Physician, Madras Medical College, Dr.Priya Vijayakumar and Dr.Sunil K.Senan, Professors, Dept., of Geriatrics, Amrita Institute of Medical Sciences, Experts in the field of General Medicine, Nursing, and Physiotherapist who validated my content and provided suggestion necessary to enhance my tool that was perfectly tailored to fit the objectives of my study.
I am extremely thankful to Prof.V.Balchandar M.P.T Principal, Jeya college of Physiotherapy for his valuable guidance and also for providing No Harm certificate which helped me to execute the study successfully.
I would like to place on record my deep sense of gratitude to Dr.K.Surendran M.D., Surveillance Medical Officer, World Health Organisation and Dr.Esther Lydia, Professor in Nutrition for the efficient guidance in constructing my research tool.
their care givers without whose cooperation and support the timely and successful completion of this endeavor would have still remained a dream.
My deepest gratitude to Mr.N.Nadarajan M.A(His), M.A.,(Pol) M.A.,(I.R) , M. Ed, Head Master (Retd), Govt. Hr. Sec. School, Nandivaram, and Mrs.B.Manimala B.Sc., M.A(Pub.Adm), M.A(Eng) IELTS Trainer for editing the tool and thesis in English and Mrs.Kalaimani M.A., M.Phil., Professor for editing the tool in Tamil.
I am extremely thankful to Mrs. Mythili, M.Sc (N) Asst.Prof, IEC department for her effort and help in preparing flash cards for executing my study.
A sincere and whole hearted gratitude to Ms.M.Sheeba Suvitha, M.Sc. (N) Incharge of Community Health Centre Arakambakam, Ms.S.Florence, Ms.D.Thilagam M.Sc(N) and Staff of OACHC for their kindness and helping hearts toward my need.
I submit my sincere thanks to the Village leaders, Trained Research Assistants, Village Health Nurse, local volunteers and self help group members who provided support for the entire study.
HOD of Community Health Nursing Dept., Mrs. R Vijayalaksmi, M.Sc(N) HOD of Obstetrics and Gynaecological Nursing Dept., and Mrs.Jeyanthi.P, M.Sc(N) Asst. Prof of Mental Health Nursing Department for their peer valuation, moral support, motivation and guidance for successful completion of this study.
I also express my heartfelt thanks to my friend Ms.Jolly Ranjith, M.Sc(N) Assot. Professor, Medical Surgical Nursing Department for her timely help in peer valuation of my manuscript and support for the curriculum management during my study period.
I thank Mrs.Bhagavathi, M.Sc(N), Ms.J.Beulah, M.Sc(N), Assot. Prof, Mrs. RuthRani Princely, M.Sc(N) HOD of Child Health Nursing Department, Mrs. Nandhini.S, M.Sc(N) Nurse Researcher, all Faculty and Staff of Omayal Achi College of Nursing (since 2011 to till now) for their kindness and helping hands in successful conduct of this study.
My special thanks to my friend Mr.Yayathee, M.Sc (N) ICMR Research fellow, who motivated and helped me in publishing my pilot study report in online journal and also I thank him for his guidance relation to copy right and plagiarism.
successful completion of my study.
I extend my thanks to the librarians Ms.F.S.Judith and Mr.T.M.Asokan, and Mr.N.Muthukumaran for their co-operation extended to me in retrieving the related literature.
I deeply thank Mr. Suresh, former System Administrator, for his support and help during my Ph.D programme.
I express my profound gratitude and heartfelt thanks to my Seniors Ms.Sathyalatha Sarathy, Ms.A.Lakshmi, Mr.S.Dinesh Selvam, Ms.R.Padmavathy, and Ms.Hemavathy for their creative minds, helping hearts, guidance and mighty hands in successful conduct of this thesis and special thanks to Mrs.Sathyalatha Sarathy for her timely help in peer valuation of my manuscript.
I am also thankful to B.Sc (N) and M.Sc (N) Medical Surgical Nursing Students of Omayal Achi College of Nursing for their timely help and encouragement and support from the conception of this study.
mother Mrs.Lakshmi, Father in Law Mr.Dakshinamoorthy, Mother in Law Mrs.Kuppammal, brothers Mr.Satheesh Kumar, Mr.Sudhakar, brother in law Mr.Baskar, Mr.Asok, Sister in law Mrs. Gomathi for their encouragement, support, adjustment and lifetime support.
My special thanks to my husband Mr.D.Ganapathy B.E, Proprietor MDM Engineering Works for his financial support, adjustment, commitment and untiring spirit of work and to my lovable children Master.G.Surya and Baby G.Harshini, for his and her adjustment, kindness and support during the period of my study.
Above all, with reverence and serenity I thank my EVER LOVING, EVER LIVING LORD ALMIGHTY for his richest heavenly blessings and abundant grace which encircled me through every minute step of my attempt to transform this execution into a reality and I accord this as the corner stone of all the help I received for my thesis.
ANOVA - Analysis of Variance
BBS - Berg Balance Scale
CI - Confidence Interval
CINHAL - Cumulative Index to Nursing & Allied Health Literature
CD - Compact Disk
ESS - Epworth Sleepiness Scale
FFNI - Family Focused Nursing Intervention
FHP - Functional Health Problem
GDP - Gross Domestic Product
GHQ - General Health Questionnaire
ICD-10 - The Tenth Revision of International Classification of Disease
ICCR - International Centre for Collaborative Research
IMRAD - Introduction, Method, Results and Discussion
KAS - Kerala Aging Survey
MOSE - Mobility and Safety for Elderly
NCDs - Non-Communicable Diseases
NICE - National Institute for Health and Care Excellence
NIMHANS - National Institute of Mental Health and Neurosciences
NSS - National Sample Survey
PMRT - Progressive Muscle Relaxation Therapy
POMA - Performance Oriented Mobility Assessment
PSQI - Pittsburgh Sleep Quality Index
SAFE - Screening Assessment for Fall Evaluation
SLR - Senior Living Residence
SPICES - Sleep Disturbance, Problem with Eating, Incontinence, Evidence
of fall and Skin breakdown
SRD’s - Sleep Related Disorders
TN - Tamil Nadu
TV - Television
UN - United Nations
UNFPA - United Nation Fund for Population Activities
UNPD - United Nation Population Division
UNPFD` - United Nation Population Fund Collaboration
USA - United States of America
USD - U.S Dollar
USPSTF - United State Preventive Services Task Force
WASO - Wake after Sleep Onset
WHO - World Health Organization
S.No. Symbols
1 χ2 Chi square
2 p Probability value
3 t Test of significance
4 N Number
5 N Total Population
6 n Sub set of population
7 % Percentage distribution
8 ≥ Greater than or equal to
9 ≤ Less than or equal to
10 df Degree of freedom
11 r Correlation
CHAPTER
NO. TITLE
PAGE NO.
1. INTRODUCTION 1 – 34
1.1 Background of the study 3 – 18
1.2 Significance and need for the study 18 – 27
1.3 Conceptual framework 27
1.3.1 Conceptual framework -General Concepts 27 – 31
1.3.2 Application of conceptual framework 31 – 33
2. AIMS AND OBJECTIVES 35 – 41
2.1 Title 35
2.2 Statement of the Problem 35
2.3 Objectives of the Study 35 – 36
2.4 Null Hypotheses 36
2.5 Operational Definitions 37 – 40
2.6 Assumptions 40 – 41
2.7 Delimitations 41
3. REVIEW OF LITERATURE 42 – 66
3.1. Part I: General concepts of functional health problem.
(Fall and sleep disturbances). 43 – 49
3.2 Part II: Research studies related to
3.2.1 Prevalence of fall among older adults 49 – 53
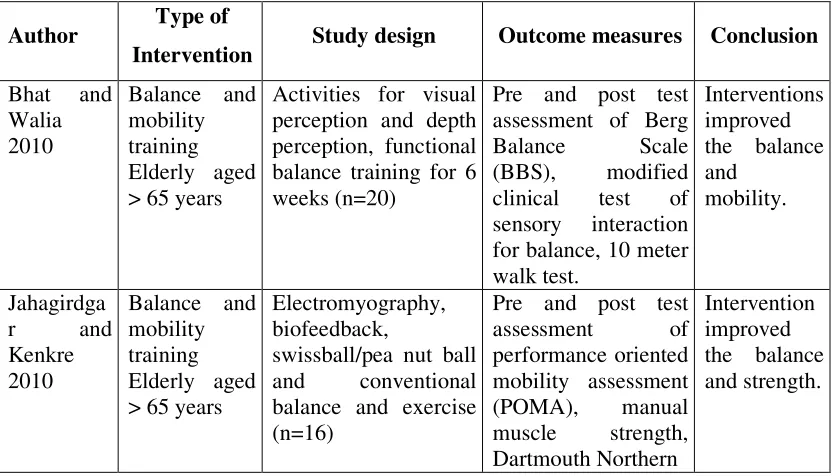
3.2.2 Effectiveness of fall prevention programme among older
adults. 53 – 58
3.2.3 Prevalence of sleep disturbances among older adults 58 – 62 3.2.4 Various interventions to reduce the sleep disturbances 62 – 65
3.2.5 Role of caregivers in care of older adults 65 – 66
4. MATERIALS AND METHODS 67 – 100
4.1 Research Approach 67
4.2 Research Design 68
NO. NO.
4.4 Research Setting 69 – 70
4.5 Population 70 – 71
4.6 Sample and Sample size 71 – 72
4.7 Sample selection criteria 72 – 74
4.8 Sampling Technique 74 – 75
4.9 Data Collection Instrument 77 – 84
4.10 Interventions 85 – 87
4.11 Content validity 87
4.12 Reliability of the tool 88
4.13 Ethical Considerations 89 – 90
4.14 Pilot Study 90 – 92
4.15 Data Collection Procedure 93 – 98
4.16 Data Analysis Procedure 100
5. RESULTS AND ANALYSIS 101–198
5.1 Description of the background variables of the older adults in
the experimental and control group. 109
5.2 Description of demographic variable of caregivers in the
experimental and control group. 115
5.3
Assessment and comparison of pre-test and post test level of functional health problem and knowledge among older adults in experimental and control group.
119
5.4
Assessment and comparison of pre test and post test level of knowledge among caregivers in experimental and control group.
132
5.5
Effectiveness of family focused nursing interventions on level of functional health problems and knowledge among older adults in experimental and control group.
136
5.6
Effectiveness of family focused nursing interventions on level of knowledge regarding functional health problems among
NO. NO.
5.7
Effectiveness of family focused nursing interventions on level of functional health problems and knowledge among older adults between experimental and control group.
168
5.8
Effectiveness of family focused nursing interventions on knowledge on functional health problems among caregivers between experimental and control group.
183
5.9
Correlation of post test level of knowledge with functional health problems among older adults in experimental and control group.
185
5.10
Correlation of post test level of knowledge of caregivers with knowledge and functional health problems among older adults in experimental and control group.
188
5.11
Association of selected background variables with level of functional health problems and knowledge gained score among older adults in experimental group
192
5.12
Association of selected demographic variables with level of knowledge gained score among caregivers in experimental group.
198
6. DISCUSSION 199–227
7. SUMMARY, CONCLUSION, IMPLICATIONS,
RECOMMENDATIONS AND LIMITATIONS 228–241
REFERENCES 242–250
S. No. Title Page No.
1.1.1 Global scenario of aged 1995-2150 5
1.1.2 Expectation of life at birth in WHO Region, 2008 6 1.1.3 Total population of elderly in various countries in the year 2008 6 1.1.4 Total Aged population in India (As per India Census 2011) 7 1.1.5 Expected number of Centenarians in the world in 2050 8 1.1.6 The life expectancy at birth in India as per census (2011) 9 1.1.7 Prevalence and risk factors for fall related injury in older adults in
low income countries
12
1.1.8 Fall related mortality and morbidity in India 13
1.1.9 Living arrangement of the older adults 17
3.1.1 Study related to fall prevention intervention for older adults 54
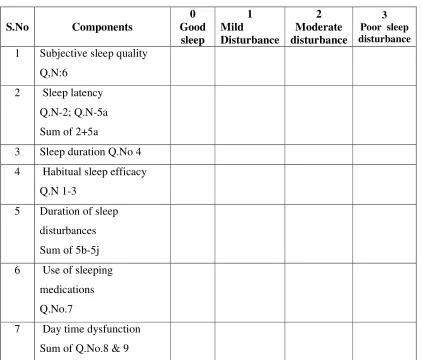
4.9.1 Domains of PSQI tool 81
4.10.1 Sleep Hygiene Schedule 86
4.12.1 Reliability values of the data collection tool 88
4.15.1 Drop out analysis 97
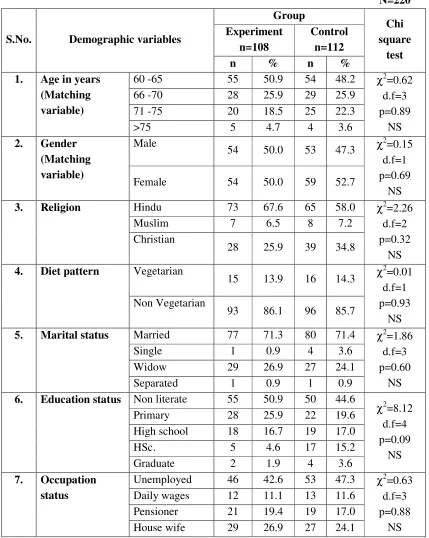
5.1.1(a)
Frequency and percentage distribution of demographic variables of older adults like age, gender, religion, diet pattern, marital status, educational status and occupation among experimental and control group
109
5.1.1(b)
Frequency and percentage distribution of demographic variables of older adults like type of family, income status, family size and family support system in experimental and control group.
111
5.1.1(c)
Frequency and percentage distribution of clinical variables of older adults such as history of chronic illness, activities of daily living, type of recreational activity and previous history of fall in experimental and control group.
113
5.2.1(a)
Frequency and percentage distribution of demographic variables of caregivers like age, gender, educational status and occupation
5.2.1(b)
Frequency and percentage distribution of demographic variables of caregivers like duration of time spending with older adults, duration of experience in caring older adults, history of chronic illness in experimental and control group
117
5.3.1
Comparison of pre test level of risk for fall, sleep disturbances and level of knowledge among older adults in the experimental and control group
119
5.3.2 Comparison between pre test and post test level of risk for fall
among older adults in experimental and control group 121
5.3.3 Comparison of pre test and post test level of risk for fall among
older adults among older adults experimental and control group 122
5.3.4 Comparison between pre test and post test level of sleep
disturbance among older adults in experimental and control group 124
5.3.5 Comparison of pre test and post test level of sleep disturbances
among older adults in experimental and control group 126
5.3.6
Comparison between pre test and post test level of knowledge regarding functional health problems among older adults in the experimental and control group
128
5.3.7
Comparison of pre test and post test level of knowledge regarding functional health problems among older adults in experimental and control group
130
5.4.1 Comparison between pre test and post test level of knowledge
among caregivers in experimental and control group 132
5.4.2 Comparison of pre test and post test level of knowledge among
caregivers in experimental and control group 134
5.5.1
Comparison of overall level of risk for fall related to personal factor score among older adults within experimental and control group
136
5.5.2
Comparison of overall level of risk for fall related to environmental factor score among older adults within
5.5.3 Comparison of overall level of risk for fall score of older adults at
the level of post test 1 within the experimental and control group 140
5.5.4 Comparison of overall level of risk for fall score of older adults at
the level of post test 2 within experimental and control group 141
5.5.5 Comparison of overall level of risk for fall scores of older adults
at the level of post test 3 within experimental and control group 142
5.5.6 Comparison of overall level of risk for fall score of older adults
within experimental and control group 143
5.5.7
Overall Comparison of pre test and post test level of risk for fall cumulative mean score among older adults in experimental and control group
145
5.5.8
Comparison of level of sleep disturbances in relation to subjective sleep quality, sleep latency and sleep duration among older adults within experimental and control group
146
5.5.9
Comparison of level of sleep disturbances in relation to habitual sleep efficacy, duration of sleep disturbance and day time dysfunction among older adults within experimental and control group
148
5.5.10
Comparison of overall level of sleep disturbances score of older adults at the post test1 level within experimental and control group
150
5.5.11
Comparison of overall level of sleep disturbances score of older adults at the post test 2 level within experimental and control group
151
5.5.12
Comparison of overall level of sleep disturbances score of older adults at the post test 3 level within experimental and control group
152
5.5.13 Comparison of overall level of sleep disturbances score of older
adults within experimental and control group 153
5.5.14
Comparison of overall level of knowledge score of older adults at
5.5.15 Comparison of overall level of knowledge score of older adults at
the level of post test 1 within the experimental and control group 156
5.5.16 Comparison of overall level of knowledge score of older adults at
the level of post test 2 within experimental and control group 157
5.5.17 Comparison of overall level of knowledge score of older adults at
the level of post test 3 within experimental and control group 158
5.5.18 Comparison of overall level of knowledge score of older adults
within experimental and control group 159
5.5.19
Overall Comparison of pre test and post test level of knowledge cumulative mean score among older adults in experimental and control group
161
5.6.1 Comparison of overall level of knowledge score of caregivers at
the level of post test 1 within experimental and control group 162
5.6.2 Comparison of overall level of knowledge score of caregivers at
the level of post test 2 within experimental and control group 163
5.6.3 Comparison of overall level of knowledge score of caregivers at
the level of post test 3 within experimental and control group 164
5.6.4 Comparison of overall level of knowledge among caregivers
within experimental and control group 165
5.6.5
Overall Comparison of pre test and post test level of knowledge cumulative means score among caregivers in experimental and control group
167
5.7.1 Comparison of level of risk for falls related to personal factors
among older adults between experimental and control group 168
5.7.2
Comparison of level of risk for falls related to environmental factors among older adults between experimental and control group
170
5.7.3 Comparison of overall level of risk for falls among older adults
between experimental and control group 171
5.7.4
Comparison of level of sleep disturbances related to subjective sleep quality and sleep latency among older adults between experimental and control group
5.7.5
Comparison of level of sleep disturbances related to sleep duration and sleep efficacy among older adults between experimental and control group
175
5.7.6
Comparison of level of sleep disturbances related to duration of sleep disturbances, use of sleep medication and day time dysfunction among older adults between experimental and control group
177
5.7.7 Comparison of overall level of sleep disturbance among older
adults between experimental and control group 179
5.7.8 Comparison of overall level of knowledge among older adults
between experimental and control group 181
5.8.1
Comparison of overall level of knowledge on functional health problems among caregivers between experimental and control group
183
5.9.1 Correlation of post test level of knowledge with risk for fall
among older adults in experimental and control group 185
5.9.2 Correlation of post test level of knowledge with level of sleep
disturbance among older adults in experimental and control group 186
5.9.3 Correlation of post test level of sleep disturbance with risk for fall
among older adults in experimental and control group 187
5.10.1 Correlation of post test level of knowledge of caregivers with
knowledge of older adults in experimental and control group 188
5.10.2
Correlation of post test level of knowledge of caregivers with level of risk for fall of older adults in experimental and control group
190
5.10.3
Correlation of post test level of knowledge of caregivers with level of sleep disturbance among older adults in experimental and control group
191
5.11.1
Association of selected demographic variables like age, educational status and type of family of older adults with the level
5.11.2
Association of selected clinical variables like activities of daily living, medication history of older adults with the level of risk for fall reduction score in the experimental group
193
5.11.3
Association of selected demographic variables like age, educational status and family income of older adults with the level of sleep disturbances in the experimental group
194
5.11.4
Association of selected clinical variables like activities of daily living, medication history of older adults with the level of sleep disturbances (quality of sleep) reduction score in the experimental group
195
5.11.5
Association of selected demographic variables like age, educational status and family monthly income of older adults with the level of knowledge gained score among older adults in the experimental group
196
5.11.6
Association of selected clinical variables like activities of daily living of older adults with the level of knowledge gained score among older adults in the experimental group
197
5.12.1
Association of selected demographic variables like age, gender, educational status and previous experience in caring older adults with the level of knowledge gained scores among caregivers in experimental group
Fig. No. Title 1.1.1 Population Pyramid in 2005 and 2025
1.1.2 Prevalence of self reported problems with falling sleep
1.3.1 Conceptual framework based on Integrated Robert Carkhuff Helping and Human Relations theory and Stuffle Beams CIPP Evaluation Model
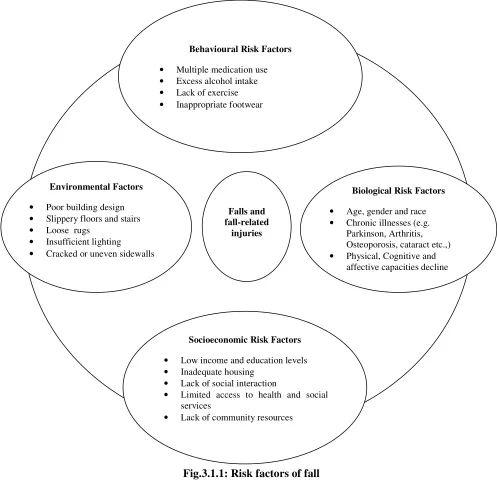
3.1.1 Risk factors of fall
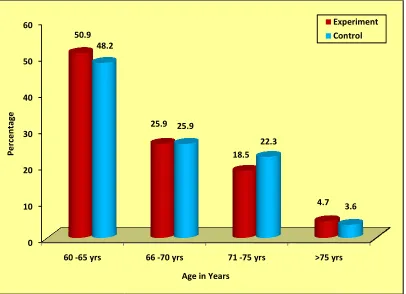
5.1.1(a) Percentage distribution of age among older adults in the experimental and control group
5.1.1(b) Percentage distribution of gender among older adults in the experimental and control group
5.1.1(c) Percentage distribution of educational status among older adults in the experimental and control group
5.1.1(d) Percentage distribution of type of family among older adults in the experimental and control group
5.1.1(e) Percentage distribution of family support system among older adults in the experimental and control group
5.1.1(f) Percentage distribution of history of chronic illness among older adults in experimental and control group
5.1.1(g) Percentage distribution of activities of daily living among older adults in experimental and control group
5.1.1(h) Percentage distribution of previous history of fall among older adults in experimental and control group
5.4.2 Overall comparison of pre test and post test level of knowledge cumulative mean score among caregivers in experimental and control group
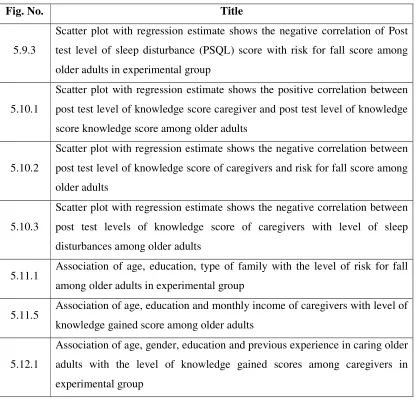
5.9.1
Scatter plot with regression estimate shows the negative correlation of post test level of knowledge score with risk for fall score among older adults in experimental group
5.9.2
5.9.3
Scatter plot with regression estimate shows the negative correlation of Post test level of sleep disturbance (PSQL) score with risk for fall score among older adults in experimental group
5.10.1
Scatter plot with regression estimate shows the positive correlation between post test level of knowledge score caregiver and post test level of knowledge score knowledge score among older adults
5.10.2
Scatter plot with regression estimate shows the negative correlation between post test level of knowledge score of caregivers and risk for fall score among older adults
5.10.3
Scatter plot with regression estimate shows the negative correlation between post test levels of knowledge score of caregivers with level of sleep disturbances among older adults
5.11.1 Association of age, education, type of family with the level of risk for fall among older adults in experimental group
5.11.5 Association of age, education and monthly income of caregivers with level of knowledge gained score among older adults
5.12.1
[image:24.612.110.527.64.473.2]S.No. Title
A Provisional Registration for PartTime Ph.D Degree B Part Time Ph.D Research Programme Proforma C Advisory Committee Certificate
D Gantt chart ( Ph.D Research Execution Plan) E Ethical Clearance Certificate
F Information, Education, Communication (IEC) Approval Certificate G Permission letter for conducting the study in the Data Collection Setting H Permission letter for utilizing PSQI tool
I Certificate for Exercise Training
J No Harm Certificate for Balance and Strengthening exercises and Breathing Exercise (Pranayama).
K List of Experts for Content Validity L Related Research Work Executed M English and Tamil Editing Certificates
N Informed consent form (English and Tamil) O Tool in English and Tamil
P Intervention Tool – English & Tamil Q Plagiarism report
R Ph.D Synopsis Submission Application Form S Ph.D Thesis Submission Application Form
T Photos
An experimental study to assess the effectiveness of family focused nursing
interventions on knowledge and functional health problems among older adults and their
caregivers at selected rural community was undertaken. The abstract for the same is
presented in (IMRAD) Introduction, Methods, Results and Discussion format of writing.
INTRODUCTION
India is an aging society with the rate of ageing population exceeding the growth
of the general population. Prevalent problems experienced by the older adults include
sleep disorder, problems with eating or feeding, incontinence, confusion, depression,
evidence of fall and skin break down.
Falls are a leading cause of death in older adults. Falls lead to 20% to 30% of
mild to severe injuries and major cause of 10% to 15% of all emergency department
visits. Fall related injuries typically occur in the home. Sleep problems can also have
serious medical consequences. Insomnia is a strong predictor of mortality and morbidity.
Sleep loss may exacerbate medical and psychiatric illnesses. Inadequate sleep (poor
quality of sleep) (or) insufficient duration (or) both may result in difficulty with
concentration, memory, confusion, increased risk of fall, and decrease the overall quality
of life. Falls in community dwelling older adults are often preventable and sleep
disturbances are manageable.
There is a need for developing a comprehensive care of providing preventive,
to reduce the burden of fall and sleep disturbance and problem of caregiver burden
existing among older adults and their caregivers.
The objectives of the study were
1. To assess and compare the pre and post test level of functional health problems
and knowledge on functional health problems among older adults in experimental
and control group.
2. To assess and compare the pre and post test level of knowledge on functional
health problems among caregivers in experimental and control group.
3. To determine the effectiveness of family focused nursing interventions on level of
functional health problems and knowledge on functional health problems among
older adults.
4. To determine the effectiveness of family focused nursing interventions on level of
knowledge on functional health problems among caregivers.
5. To correlate the post test level of knowledge with the level of functional health
problems among older adults in experimental and control group.
6. To correlate the post test level of knowledge on functional health problems of
caregivers with the level of knowledge and functional health problems among
older adults in experimental and control group.
7. To associate the selected background variables with mean differed functional
health problems score and knowledge score among older adults in experimental
and control group.
8. To associate the selected demographic variables with mean differed knowledge
NH1: There is no significant difference in the pre and post test level of functional
health problems and knowledge on functional health problems among older
adults between experimental and control group at p<0.05 level.
NH2: There is no significant difference in the pre and post test level of knowledge on
functional health problems among caregivers between experimental and control
group at p<0.05 level.
NH3: There is no significant correlation between the post test level of knowledge with
level of functional health problems among older adults in experimental and
control group at p<0.05 level.
NH4: There is no significant correlation between the post test level of knowledge of
caregivers with post test level of functional health problems and knowledge
among older adults in experimental and control group at p<0.05 level.
NH5: There is no significant association of selected background variable with mean
differed functional health problems score and knowledge score among older
adults in experimental and control group at p<0.05 level.
NH6: There is no significant association of selected demographic variable with mean
differed knowledge score among caregivers in experimental and control group at
p<0.05 level.
The conceptual frame work for the present study was based on the Integrated
theory of Robert R. Carkhuff helping and human relations theory and Stuffle Beam
CIPP evaluation model which guided the investigator through a systematic approach to
approach the older adults functional health problems and improve the knowledge of
A true experimental two group pretest and post test design was undertaken for the
study. The independent variable for the study was family focused nursing interventions
and the dependent variable was the knowledge on functional health problems and
functional health problems among older adults, knowledge on functional health problems
among caregivers. The study was conducted at adopted villages (community) of Omayal
Achi Community Health Centre. The samples for the study were older adults who had
functional health problems such as risk of fall and sleep disturbances and their
caregivers. The total sample size was 220 older adults (108 in experimental group and
112 in control group) and 220 caregivers of older adults (108 in experimental group and
112 in control group). Simple random sampling technique (random number table
method) was used to collect the samples.
The data collection instrument for screening of older adults with functional health
problem was modified Fulmer SPICES tool and level of function health problem such as
risk for fall using modified SAFE tool, and sleep disturbances (Sleep quality -Insomnia)
using Pittsburg sleep quality index tool and structured knowledge questionnaire to assess
the level of knowledge of older adults and their caregivers.
The investigator conducted the study in three phases. In the first phase, screening
was done for all the older adults with functional health problems and in second phase,
pre test assessment of level of functional health problems in older adults and level of
knowledge among older adults and their caregivers was done. In the third phase, the
investigator administered family focused nursing interventions which included family
sleep hygiene with breathing exercise for reduction of sleep disturbances. Reinforcement
of information and adherence of exercise was administered by direct visit using
flashcards and video show and post test was done at 1st, 3rd and 6th months.
RESULTS AND DISCUSSION
The data analysis findings at the end of the 6th month (Post test 3) on risk for fall,
sleep disturbances and knowledge among older adults and knowledge among care givers
after administering Family Focused Nursing Interventions (FFNI) revealed the following
results.
With regard to the risk for fall among older adults in experimental group, the
overall mean score was 3.37 with the SD 1.21, whereas in control group, it was 7.35 with
the SD 1.93. The unpaired ’t’ test value of t=18.26 proved that there was a high
statistical significant difference between the experimental and control group at p<0.001
level. FFNI such as education on fall, balance and strengthening exercise, modification
of possible home environment had significantly reduced the risk for fall among older
adults in the experimental group (29.7%) than in the control group (1.6%).
With regard to the level of sleep disturbances among older adults in experimental
group, the overall mean score was 4.71 with the SD 3.79, whereas in control group, it
was 8.92 with the SD 0.48. The unpaired ’t’ test value of t=11.66 proved that, there was
a high statistical significant difference between the experimental and control group at
group (23.7%) than in the control group (0.6%).
With regard to the level of knowledge among older adults in the experimental
group, the overall mean score was 17.38 with the SD 1.34, whereas in control group, it
was 9.20 with the SD 2.87. The unpaired ‘t’ test value of t= 27.14 proved that, there was
a high statistical significant difference in the level of knowledge among older adults
between the experimental and control group at p<0.001 level. FFNI such as family
focused education had significantly improved the level of knowledge of older adults in
the experimental group (44.8%) than in the control group (0%).
With regard to the level of knowledge among caregivers in the experimental
group, the overall mean score was 17.82 with the SD 1.59, whereas in control group, it
was 9.10 with the SD 2.87. The unpaired ‘t’ test value of t=7.14 proved that, there was a
high statistical significant difference between the experimental and control group at
p<0.001 level. FFNI such as family focused education had significantly improved the
level of knowledge of caregivers in the experimental group (42.7%) than in the control
group (1.1%).
Thus the family focused nursing intervention had significantly reduced the
functional health problem and improved the knowledge among older adults and their
The research phenomena focused on family focused nursing intervention for
older adults and care giver, in which the knowledge and functional health problems
among older adults and knowledge of care givers were assessed. The research
investigator utilized the FFNI which included family focused education, balance and
strengthening exercise, possible modification at home environment, sleep hygiene and
breathing exercise. The study concluded that there was a significant reduction of risk for
fall rate by 29.7%, reduction of sleep disturbances rate by 23.7% and improvement of
knowledge among older adults and their caregiver’s rate by 44.8%, and 42.7%
respectively. The study result proposes and the research investigator also recommends
CHAPTER – 1
INTRODUCTION
Living is a process of continual change which consists of three phases in a
human’s life. They are childhood, middle age and old age. Every person has to face the
reality of old age because it is a natural phenomenon. Elderly (or) Geriatrics (or) older
adults consist of age nearing (or) surpassing the average life span of human being. The
boundary of old age cannot be defined exactly because it does not have the same
meaning in all societies. The Government of India adopted National policy on older
person in January 1999. The National policy defines senior citizen (or) elderly (or) older
adults as a person who is of age 60 years (or) above1.
Over the past century, humanity has been adding years to life. The overall
reduction in general and infant mortality rates and the steady increase in average age of
death have resulted in the growth of elderly population around the world. These are great
triumphs. Globally “ageing” is growing in both developed and developing countries. The
dream of human being is to live longer and free from all sufferings. Population ageing
presents both challenges and opportunities.
Health, in the older person, is a product of the life experiences of the individual.
As age advances, biological and physical nature of the body is likely to deteriorate which
leads to physical and sensory impairment and increasing disability. There are many
causes for declining function in old age, but in general, these can be divided into four
Normal aging brings about inevitable and irreversible changes. These normal
ageing changes are partially responsible for the increased risk of developing health
related problems within the elderly population. The prevalent problems experienced by
the older adult includes sleep disorders, problems with eating or feeding , incontinence,
confusion, depression, evidence of fall and skin break down. Falls and sleep disorder are
the major problems among the older adults. These are the important causes of morbidity
and mortality among older adults and predictor of poor physical and cognitive status2.
Many of the health problems faced by older persons are the result of risk factors
such as smoking, lack of physical activity and unhealthy diets. Maintaining an active
lifestyle is one of the most cost effective ways to stay healthy. An active lifestyle means
older persons continue to participate in social, economic, cultural, spiritual and civic
affairs. Longer life is a benefit to individual and community only if the quality of life is
maintained3.
The focus of geriatric care services is on preservation of function and improving
the quality of life rather than on investigating, diagnosing, treating and curing specific
diseases because many diseases in the elderly are chronic in nature. This means the
geriatric nurse must deal with the patient’s social, psychological, physical and medical
problems in participation with their family or caregivers who are assisting the older
adults
1.1 BACKGROUND OF THE STUDY
The aging of population and extension of life is an important end product of the
process of demographic transition. “Normal ageing” refers to inexorable and universal
physiological changes that occur with ageing. “Usual aging includes age related disease
which results from the interaction between genetic, environmental and behavioral
factors. “Successful aging is defined as a low risk of disease and disease related
disability, high mental and physical function, and active engagement with life”4.
Geriatrics & Geriatric Nursing
The word Geriatrics was derived from the Greek word “Gerios” meaning old age
and “iatros” meaning medicine. The terminology was coined by an American Doctor
Nascher in 1914. The British Geriatric Society defined Geriatrics as “The branch of
general medicine concerned with the clinical, preventive, medical and social aspects of
illness in the elderly”. The specialty of geriatric nursing plays a vital role in the care of
elderly in the community5.
Gerontology and Gerontological Nursing
Gerontology is the scientific study of the ageing process and problems of ageing.
Geriatric medicine is a specialty which deals with the health care and social welfare
aspects of the elderly. The American Geriatric Society was established in 1942. The first
geriatric specialty department was established in Britain in 1947 by Dr.Marger Warren6.
The first geriatric specialty ward in India was started in 1978 at the Government General
Hospital, Chennai by Padmashree. Natarajan.V.S. The aim of gerontologic nursing is to
safeguard and improve the health of the aged to the greatest extent possible and to
World Health Organization (WHO) had chosen 1999 as the International Year of
the Elderly”. The World Health Day (April 7th) theme of the Year 1999 was “Active
aging make the difference” which is recognized that it is the key for older people to go
on playing a major part in the society. Every year, 1st October is celebrated as the “The
International Day of Older Persons”. Active aging involves every dimensions of life, viz
physical, mental, social and spiritual8.
Globally, the number of people aged 60 years and above is growing faster than
any other age group. It is estimated that by 2050, for every one child there will be two
elderly people. The percentage of elderly in the world population is expected to increase
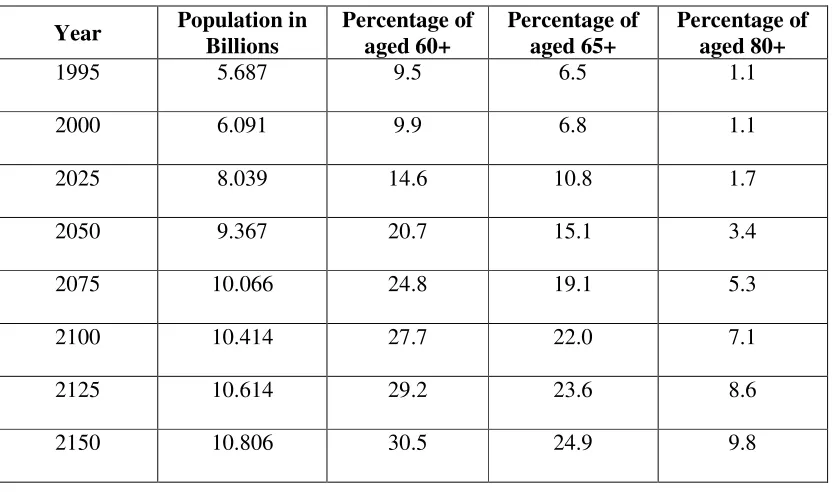
rapidly from 9.5 in 1995 to 20.7 in 2050 and 30.5 in 2150. In 2006 almost 500 million
people worldwide were 65years and older. By 2030 the total is projected to increase to 2
billion. This phenomenon is referred to as “Population aging”. “Population aging is a
triumph of humanity but also a challenge to society”9.
Fig1.1.1: Population Pyramid in 2005 and 2025
It highlights the growing proportion of older population in parallel with a
decreasing proportion of younger population. The triangular population pyramid 2005
[image:37.612.110.526.195.441.2]will be replaced with a more cylinder like structure in 20253.
Table 1.1.1: Global scenario of aged 1995-2150 10
Year Population in
Billions
Percentage of aged 60+
Percentage of aged 65+
Percentage of aged 80+
1995 5.687 9.5 6.5 1.1
2000 6.091 9.9 6.8 1.1
2025 8.039 14.6 10.8 1.7
2050 9.367 20.7 15.1 3.4
2075 10.066 24.8 19.1 5.3
2100 10.414 27.7 22.0 7.1
2125 10.614 29.2 23.6 8.6
2150 10.806 30.5 24.9 9.8
Based on the demographic views, population ageing is a result of decline in both
mortality and fertility, i.e. fewer children are born and more people live in old age. Over
the last five decades mortality rate in developing countries has markedly declined, and
dramatically raised the average life expectancy at birth, from 41 years in the early 1950’s
to almost 62 years in 1990. By the year 2020 it is projected to reach 70 years. The
number of elderly worldwide will reach more than 1000 million with over 700 million of
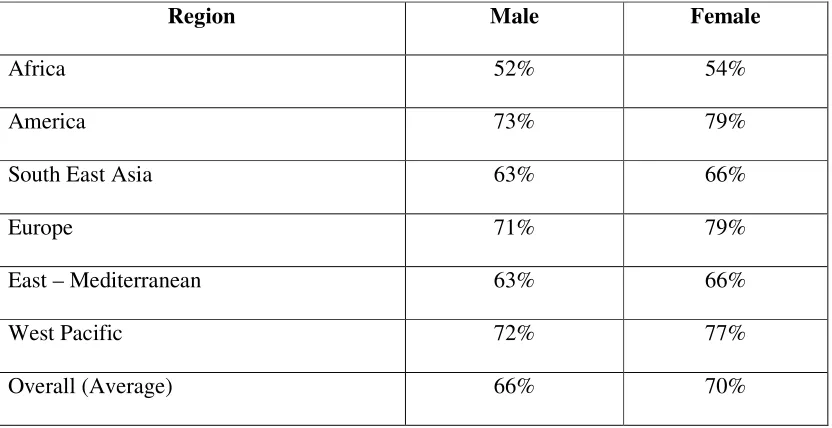
Table 1.1.2: Expectation of life at birth in WHO Region, 200812
Region Male Female
Africa 52% 54%
America 73% 79%
South East Asia 63% 66%
Europe 71% 79%
East – Mediterranean 63% 66%
West Pacific 72% 77%
Overall (Average) 66% 70%
More than half of the world’s elderly population lives in the Asia – Pacific
region. The largest number of elderly persons in Asia is in Japan, followed by India and
[image:38.612.110.526.93.307.2]other countries12.
Table 1.1.3: Total population of elderly in various countries in the year 200813
Country Elderly population
China 12%
European Region 19%
Indonesia 9%
Italy 26%
Japan 29%
China 12%
South East Asia 8%
India which is the second largest population in the world and is the world’s
largest democracy is also undergoing demographic transition. India is an aging society
with the rate of ageing population exceeding the growth of the general population. In
India, there has been sharp increase in the number of elderly between 1991 & 2001 from
57 million to 77 million and 137 million by 20 2114. By the year 2050, the number of
elderly people would rise to 324 million. India has gained the label of “an aging nation”
with 7.7% of its population being more than 60 years and is expected to reach 12.6 in
202515.
Table 1.1.4: Total Aged population in India (As per India Census 2011)15
YEAR TOTAL AGED POPULATION
1961 24 millions
1981 43 millions
1991 57 millions
2001 77 millions
2011 90 millions
2050 (Estimated) 315 millions.
SOURCE: United Nation Population Fund Collaboration and Help age India 2012.
In 1997, the number of people aged 60 years and above was 63.64 million. As of
1st March, 2012, the projected number stands at 98.5 million. The number of elderly
people in India (60 years and above) has increased by 54.77% in the last 15 years16.
The report, which was released in Tokyo on the International Day of Older
per cent are elderly. According to the report, by 2050, India and China will have about
80 per cent of the world's elderly living there, and India is likely to overcome China in
the number of centenarians17.
Table.1.1.5: Expected number of Centenarians in the world in 205017
Country At present Expected numbers
China 14,300 2,62,500
Japan 49,500 617,000
India 151,000 620,000
Ageing of population is affected due to downward trends in fertility and
mortality. Low birth rates coupled with long life expectancies, push the population to an
ageing humanity. It is observed that percentage of person aged 60 (or) more is rapidly
increasing and the percentage of person above age 80 is going up over the years. The
total fertility rate in overall India has declined18.
Expectation of life at birth for males and female has increased more in recent
years. In India the expectation of life at birth for male has shown increase from 42 years
in 1951 1960” to 58 years in 1986 1990” and it is projected to 67 years by 2011
-2016 for males and 69 years for females. This shows an increase of about 9 years for
Table 1.1.6: The life expectancy at birth in India as per census (2011)
Life
Expectancy
(In years)
199120 201115
M F M F
58.6 59 65 65
The decision of rural and urban population is one of the important socio
demographic factors. As per the National Census in India 2011, 833 million people
currently live in rural areas. Only 31.99% of population live in urban areas. The
distribution of rural population in India declined by more than 3 percentage from 72.99%
(2001) to 68.84% (2011). Though majority of them are older adults and they still reside
in rural India21.
In India, three fourth of the elderly live in rural areas, of which 48% are women
and 55% of them are widows. Nearly 70% rural elderly depend on others as their health
problems increase with age. The percentage of older adult population will gradually
increase in Tamil Nadu and Kerala and will have more than 13% of population in the age
group of 60 plus by the year 201622.
In Tamil Nadu, the total population as per census (2011) was 7,21,38,958. Total
aged population in Tamil Nadu is 4.16 million. Among them 2.4 million are women.
68% of elderly people are living in rural area. Urban aged population is equal among
men and women. In rural areas 1.51 million are male which is slightly higher than female
Older adults in the rural community face special challenges because of
geographical isolation, high poverty level and declining of self care abilities and less
access to health care providers. Majority of the older adults are less engaged in health
promoting activities and often under served by health care personnel. The rural older
adults face medical indifference, not only in hospital care, but elder nursing homes,
recreation facilities and old age centers are over whelming us presently in the urban
areas. With such a huge mismatch in the urban rural population and health care system,
elderly in India faces an uphill task.
Normal aging brings about inevitable and irreversible changes. These normal
ageing changes are partially responsible for the increased risk of developing health
related problems within the elderly population. Prevalent problems experienced by the
older adult includes sleep disorders, problems with eating or feeding , incontinence,
confusion, depression, evidence of fall and skin break down. Falls and sleep disorder are
the major problems among the older adults. These are the important cause of morbidity
and mortality among older adults and predictor of poor physical and cognitive status2.
Falls are a common public health problem among the older adults in many
communities. Falls are a significant threat to the safety, health and independence of older
citizens. Around 30% of community dwelling elderly fall each year and some fall
repeatedly. Every 17 seconds an adult over 65 years of age will fall and subsequently
The Center for Disease Control and Prevention reported that 1 in 3 adults aged 65
years and older will experience a fall in a year. 20% to 30% of those who fall will sustain
a moderate to severe injury25.
The global burden of Years Lived with Disability (YLD’s) due to fall in adults
aged 50 and 69 years was 66% in developing countries compared with 34% in developed
countries. In 2010, falls accounted for over 77% and 85% of YLD’s resulting from
unintentional injuries than traffic accidents in adults aged 50 to 69 years and 70 and over.
People aged 65 and older have the highest risk for falling with 30% and 50% of people
older than 80 falling at least once in a year26.
WHO study on Global Aging and Adult Health report on prevalence and
risk factors for fall related injury in older adults in low and middle income
countries-2013 (China, Ghana, India, Mexico, the Russian Federation and South
Africa)26
• Prevalence of fall injuries among older adults was highest in India (6.6%) and
lowest in South Africa (0.9%).
• Fall related injury was more prevalent among women than men in all countries
except South Africa.
• Unintentional fall related injuries were most common type (91.4%) and
intentional (inflicted by another person) the least common type (2.6%).
• Fall related injuries typically occurred in the home.
• Depression, arthritis, grip strength and insufficient intake of fruits and vegetables
severe or extreme sleep problem, water source outside the home were identified
as risk factors for fall related injury in China and India.
Table 1.1.7: Prevalence and risk factors for fall related injury in older adults in low
income countries26
Countries China Ghana India Mexico Russian
Federation
South
Africa
Prevalence of fall
related injury in
last 12 months
372 118 430 101 107 31
% 60.6 44.4 72.3 67.2 73.0 66.9
Age group (in years)
50 -59 2.2 2.0 6.2 1.4 2.4 0.2
60-69 3.4 2.8 6.6 3.8 3.0 1.3
70-79 4.7 3.0 7.4 4.5 1.7 0.8
80+ 4.4 3.2 7.8 4.3 3.0 5.5
Gender
Male 2.4 1.6 4.4 1.9 2.0 1.3
Female 3.9 3.6 8.8 3.6 2.7 0.6
Place of fall
Home 46 41.3 69.6 85.3 46.0 70.5
Work 31.7 44.6 14.7 13.6 14.0 12.0
Others 20.9 11.1 15.0 0.0 0.0 1.0
Falls are a leading cause of death in older adults. Falls lead to 20% to 30% of
mild to severe injuries and major cause of 10% to 15% of all emergency department
visits. The duration of hospital stay after fall injuries ranges from 14 to 15 days and may
be longer when associated with hip fractures, advancing age and frailty27.
Among older adults, falls are the number one cause of fractures (hip, pelvis,
spine arm hand or ankle), most common reason for hospital admissions for trauma, loss
of independence, need long term care and deaths. 20% to 30% of traumatic brain injuries
Table 1.1.8: Fall related mortality and morbidity in India29
Authors Location
Fall history criteria
Consequences of fall in older adults
Jaganoor
et al, 2011
28 states and 7 union
territories covered by the sample registration
system
- Mortality Injuries Psychological
impact
Death in 2001 2003 65%, high death rates above 70
years of age.
- -
Dsouza et al, 2008
Manipal, Udupi, Karnataka Falls in the previous year _ Injuries (59%), fractures (16%), physician consultation(4 7%), hospital admission (19%)
Fear of fall (53%), activity restriction(31%) Cardona et al, 2008 Andhra Pradesh
- Fall
injuries(86%)
Non fatal
injuries (34%) -
Kaushik and Desouza 2008 Not specified - - -
40% of elderly with fall history reported decreased balance confidence. World Health Organizati on 2004,
India - Death 53% - -
The economic impact of falls is critical to family, community, and society. Fall
incurred costs are categorized as direct and indirect cost. Direct costs include health care
costs such as medications and other services such as consultation and rehabilitation
services. Indirect costs include loss of income due to inability of individuals or family
SLEEP:
Sleep complaints are common among all age group. The most frequent sleep
complaints in older adults is “sleep maintenance insomnia that is difficulty in initiating
(or) maintaining sleep ,early morning wakening and frequent nocturnal awakenings,
obstructive sleep apnea syndrome, restless leg syndrome, rapid eye movement and sleep
behavior disorder”. Approximately 50% of the population aged 65years or above have
problems with sleep; it does not mean elders should encounter sleep disorders30.
Warwick Medical School (2012) evaluated the sleep quality among 24,434
women and 19,501 men aged 60 years and above in eight rural global locations like
Ghana, Tanzania, South Africa, India, Bangladesh, Vietnam, Indonesia and Kenya. The
epidemic of sleeplessness affected 150 million older adults in developing world. The
[image:46.612.118.524.401.681.2]number is projected to increase to 200 million by 203031.
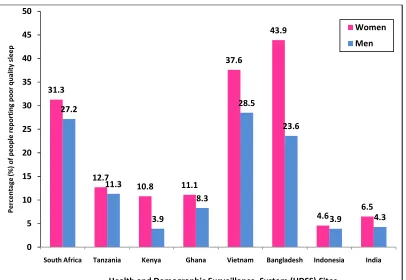
Fig.1.1.2: Prevalence of self reported problems with falling sleep31 31.3 12.7 10.8 11.1 37.6 43.9 4.6 6.5 27.2 11.3 3.9 8.3 28.5 23.6 3.9 4.3 0 5 10 15 20 25 30 35 40 45 50
South Africa Tanzania Kenya Ghana Vietnam Bangladesh Indonesia India
P e rc e n ta g e ( % ) o f p e o p le r e p o rt in g p o o r q u a li ty s le e p
Health and Demographic Surveillance System (HDSS) Sites
Women
Bangladesh had the highest prevalence of sleep problem (Insomnia) 43.9% for
women, and 23.6% in men. Vietnam too had very high rate of sleep problem 37.6% for
women and 28.5% for men. In African countries, Tanzania, Kenya and Ghana the rate of
sleep problem was between 8.3% and 12.7%. South Africa had double the rate of African
countries 31.3% for women and 27.2% for men31.
Nearly 5% of Indians aged 50 years and above suffered from sleep disorders, of
which 6.5% women and 4.3% men suffered with sleep disturbance. Around 4% of the
men who reported severe or extreme sleep problem suffered from severe depression and
3% reported severe anxiety32.
Many studies reported about sleep complaints in older people. Study conducted
in a sample of over 3000 people aged 18 to 79 years reported that the one year
prevalence of insomnia was 14% in the aged 18 to 34 years, but rose to 25% in the 65 to
79 years old. A recent survey in community dwellers older than 65 years showed the
prevalence insomnia was 36% in men and 54% in women. A study of 8500 people aged
16 to 74 years found that 37% older people had insomnia33.
Longitudinal follow up study for 13 to 15 years from 1997-1999 through 2012,
reported that insomnia was associated with a threefold increase in mortality. In relation
to gender, male insomniacs had 4 times higher risk of mortality than sleepers and
compared with those sleeping 6.5 hrs or more34.
Sleep problems can also have serious medical consequences. Insomnia is a strong
illnesses. Inadequate sleep (poor quality of sleep) (or) insufficient duration (or) both
may result in difficulty with concentration, memory, confusion, increased risk for fall,
and decrease the overall quality of life. Sleep maintenance insomnia, that is early
morning wakening and frequent nocturnal awakenings are often distressful to the elderly
and their caregivers and frequently precipitate crises in care giving35.
Older adults are in need of conservative and non pharmacologic therapies like
simple sleep hygiene, diet, balance and strengthening exercises, cognitive behavioral
therapy and lifestyle changes than medications because elderly are more likely to have
medication side effects (or) complications36. The Pittsburgh Sleep Quality Index is easily
used to assess the quality and pattern of sleep in older adults37.
Sleep hygiene is an important first line treatment strategy of managing insomnia.
The other strategies include stimulus control (control sleep environment), behavioral
interventions, sleep restriction therapy (strict sleep wake cycle), paradoxical intention
(not voluntarily making oneself go to sleep), patient education and relaxation therapy
(deep breathing, progressive muscle relaxation, meditation, yoga, tai chi etc) 38.
Caregivers
Social support for the older adult occurs at three levels. Family and kinship
relations are the first and preferred providers of social support. Second, a semiformal
level of support is found in clubs, churches, neighbourhoods, and senior citizen centers.
Last the older adults may be linked to social welfare agencies, health facilities, and
National Family Health Survey in India found that more than four out of five
(78%) Indians aged 60 years and older live in the same household with their children,
while about 14% lived with only a spouse and 5 percent lived alone40.
Table 1.1.9: Living arrangement of the older adults 40
Living arrangement of older
adult
Male Female
Rural Urban Rural Urban
Institute 0.65 0.74 0.54 0.20
Alone 11.78 0.69 8.98 0.60
With Family 87.19 98.42 90.08 98.77
No relation 0.33 0.16 0.40 0.43
Source: 60thNSS Report (1990-1994)
The UNFPA in its study in India, which was conducted in seven states, found that
around one-fifth of the elderly lived alone or with spouses only in both rural and urban
areas. 70 per cent of the elderly population was illiterate and their earning capacity in the
past (during their adult years) was limited and they depended upon some productive
labour work outside home for their survival. “Nearly 60-75% of all elderly are
economically dependent on other, usually their children. Even though they receive
pension they find their economic status lower after retirement”40.
Caregiver is someone who provides supervision, direct care and coordinates
services. Family care giving activities include assistance with day-to-day activities,
illness-related care, care management, and invisible aspects of care. Day-to-day activities
include personal-care activities (e.g., bathing, eating, dressing, mobility, transferring
from bed to chair, and using the toilet) and IADLs (e.g., meal preparation, grocery
include managing symptoms, coping with illness behaviors, carrying out treatments, and
performing medical or nursing procedures that include an array of medical
technologies39.
The caregiver spending more time in care of older adults often experiences stress,
depression and physical illness as they have to care the other members of the family.
Nursing research must accelerate our efforts to identify the best practice for providing
quality care for older adults and for supporting their families and other caregivers.
1.2 SIGNIFICANCE AND NEED FOR THE STUDY
In recent years, several countries such as Thailand, Indonesia, and India have
taken steps to improve services for