White Rose Research Online URL for this paper: http://eprints.whiterose.ac.uk/1722/
Article:
Sloper, P., Greco, V., Webb, R. et al. (1 more author) (2006) Key worker services for disabled children: the views of staff. Health & Social Care in the Community. pp. 445-452. ISSN 1365-2524
https://doi.org/10.1111/j.1365-2006.00617.x
eprints@whiterose.ac.uk
Reuse
Items deposited in White Rose Research Online are protected by copyright, with all rights reserved unless indicated otherwise. They may be downloaded and/or printed for private study, or other acts as permitted by national copyright laws. The publisher or other rights holders may allow further reproduction and re-use of the full text version. This is indicated by the licence information on the White Rose Research Online record for the item.
Takedown
If you consider content in White Rose Research Online to be in breach of UK law, please notify us by
Key worker services for disabled children: the views of staff
Short title: Views of staff in key worker services
Authors: Veronica Greco, D. Phil., Social Policy Research Unit, University of York;
Patricia Sloper, PhD, Social Policy Research Unit, University of York;
Rosemary Webb, PhD, Department of Educational Studies, University of York;
Jennifer Beecham, PhD, Personal Social Services Research Unit, University of Kent
at Canterbury.
This is the authors’ version of the article published as Greco, V., Sloper, P., Webb, R.
and Beecham, J. (2006) Key worker services for disabled children: the views of staff,
Health and Social Care in the Community, 14, 6, 445-52.
The definitive version is available at www.blackwell-synergy.com
Author to whom correspondence can be addressed:
Veronica Greco, Social Policy Research Unit, University of York, YO10 5DD
Tel: 01904 321950
Fax: 01904 321953
Abstract
Provision of ‘key workers’ for disabled children and their families, working across
health, education, and social services, has been recommended in the Children’s
National Service Framework. This study investigated the views of staff of key worker
services concerning the organisation and management of the services. Interviews
were carried out with key workers (N=50), managers (N=7) and members of
multi-agency steering groups (N=32) from seven key worker services in England and
Wales. A response rate of 62% was obtained. Major themes emerging from the
interviews were identified, a coding framework was agreed upon, and data were
coded using the qualitative data analysis programme Max QDA. Results showed that
although the basic aims of the services were the same, they varied widely in the key
workers’ understanding of their role, the amount of training and support available to
key workers, management and multi-agency involvement. These factors were
important in staff’s views of the services and inform recommendations for models of
service.
Key workers: key workers, care coordination, disability, children, multi-agency
working.
Introduction
Families with disabled children are in contact with many different agencies and
professionals. Many families report problems in understanding what services are
available and how to access them, understanding the roles of the different agencies
and professionals, getting professionals to understand their situation, and delays in
receiving services (Sloper, 1999). An answer to these problems, recommended in
official reports from the Court Report (1976) onwards, is that families should have
one person who acts as their main point of contact, collaborates with professionals
from their own and other services and ensures that access to and delivery of services
from the different agencies and professionals is co-ordinated. This person has been
termed a 'key worker', 'named person' or 'care coordinator. In this paper, the term key
worker is used.
Research has shown that less than a third of families with a disabled child has a key
worker (Beresford, 1995; Chamba et al., 1999) and when this does occur, it is often a
professional who takes on the role on their own initiative. Until recently, the
development of key working as part of a multi-agency system has been rare.
However, with the implementation of the Early Support Programme (Department for
Education and Skills/Department of Health, 2004) for families with young disabled
children, there has an upsurge of interest in key worker services.
A review of evidence on the effects of having a key worker (Liabo et al., 2001) has
shown that families with key workers report better relationships with services,
reduced stress, improvements in receipt of information and access to services, fewer
have reported that the role of the key worker encompasses: providing information
and advice to the family, identifying and addressing needs, accessing and
coordinating services for the family, providing emotional support, and acting as an
advocate for the family (Mukherjee et al., 1999; Tait & Dejnega, 2001).
A few studies have investigated views of staff in key worker services. Two studies
(Prestler, 1998; Tait & Dejnega, 2001) showed that there was an increase in job
satisfaction for those who acted as key workers. Other studies have looked more
broadly at professionals' views of the key worker service and their role in it. Appleton
et al. (1997) reported that key workers felt that they needed more time to dedicate to
care coordination and specific training for the role. In an evaluation of two key worker
schemes, Mukherjee et al. (1999) found that half the key workers saw no differences
between the key worker role and their everyday work. Key workers felt that the role
produced benefits in multi-agency working and improved relationships with parents.
However, difficulties were also encountered: not having enough time for the role,
confusion for staff and families about the key worker's role and, in one site, a lack of
training and supervision for key workers.
In a recent study exploring the impact of multi-agency working on professionals
supporting disabled children (Abbott et al., 2005), professionals from six care
coordination schemes, four of which provided key workers to families, were
interviewed. Results showed that overall, working with families as part of a
multi-agency team was felt to be enjoyable and rewarding. Professionals enjoyed better
relationships with families and could be more effective in supporting them.
to meet families’ needs, and they had broadened their own sense of role and identity,
although this sometimes raised concerns about erosion of expertise, and some
experienced uncertainty about the key worker role. Staff also reported that
multi-agency work did not appear to have a detrimental impact on their workload, although
there did not seem to be clear guidelines for staff on how much time commitment
should be made available to the care coordination service.
The aim of the study reported here was to investigate the views of staff from seven
key worker services which differed in their management and operation. This was part
of a larger project evaluating key worker services, involving parents, children and
staff in the services, and exploring the effectiveness of different models of service
(Greco et al., 2005).
Methods
Selection of key worker schemes
Seven key worker services were selected from 30 that were identified from a national
survey (Greco & Sloper, 2004). The rationale for selection of the seven services was
to represent variation in terms of models of service and types of locality covered.
Results of the survey indicated that an important difference between services was
the type of key workers employed, with non-designated key workers (who key work
for a few families on top of their ordinary role) being the most common (21 services),
and five services employing designated (full-time) key workers and three using both
types of workers. Thus, services were selected to reflect these different models: four
used only non-designated key workers, two used only designated key workers, and
funding to no dedicated funding; two services were longstanding and five were more
recently set up. Four of the catchment areas were predominantly rural, two were
predominantly urban, and one encompassed both urban and rural areas. Four of the
services were in England and three in Wales. The study aimed to investigate the
selected services as cases viewed from the perspectives of key workers, service
managers, and members of the steering group.
Procedure
The study was approved by a Multi-Centre Research Ethics Committee. Packages,
each containing a cover letter, information sheet, response form and postage-paid
return envelope, were sent to managers of the services, who distributed these to key
workers and all members of steering groups. The project aimed to interview all
managers, up to 10 key workers and up to 8 members of steering groups in each
service. Where services included a large number of key workers, managers were
asked to send packages to 20 key workers from a variety of professional
backgrounds. Where services included large steering groups (over ten), packages
were sent to ten members, selected to cover a variety of backgrounds, including
parents. If willing to take part, recipients provided contact details on the response
form, and were contacted by researchers to arrange an interview. Interviews lasted
approximately one hour and, with participants' consent, were tape-recorded.
Interview schedules
The interview schedules set out a list of questions and possible prompts to guide
interviewers but were used flexibly in order to respond to the issues raised by the
interviewees.
Key workers were asked questions about: their professional background, typical day,
training and supervision received, and problems encountered.
Interviews with steering group members included questions about their role on the
steering group; procedures for steering group meetings; multi-agency involvement;
involvement of parents and children in setting up and overseeing the service; and
funding for the service.
Interviews with service managers covered: their professional background and role in
the service; history of the service; multi-agency involvement; parent and child
involvement in the service; and funding of the service. All interviewees were asked
about the role of key workers, advantages and disadvantages of the service and
suggested improvements.
Data analysis
The interviews were analysed following established qualitative analysis procedures
(Taylor & Bogdan, 1984). This involved three researchers each reading a set of
transcripts to identify major themes emerging from the interviews. A coding
framework was agreed and themes were coded, employing the qualitative analysis
and views of the different models of services and then comparing these. Initially, a
report on the interviews for each service was produced, and these were checked by
another researcher and sent to the service manager in the appropriate site for further
checking. These reports were then drawn together, identifying differences and
similarities between views in the different services for a full report on the study
(Greco et al., 2005).
Results
Sample
One hundred and fifty-five packages were handed out to service managers.
Ninety-six responses were received. This represents a response rate of 62%. However, in
two services, it was not clear whether all packs were distributed to staff. In addition,
eight respondents were not included as they exceeded the number of interviews
planned for their services. In one interview, the tape was faulty and could not be
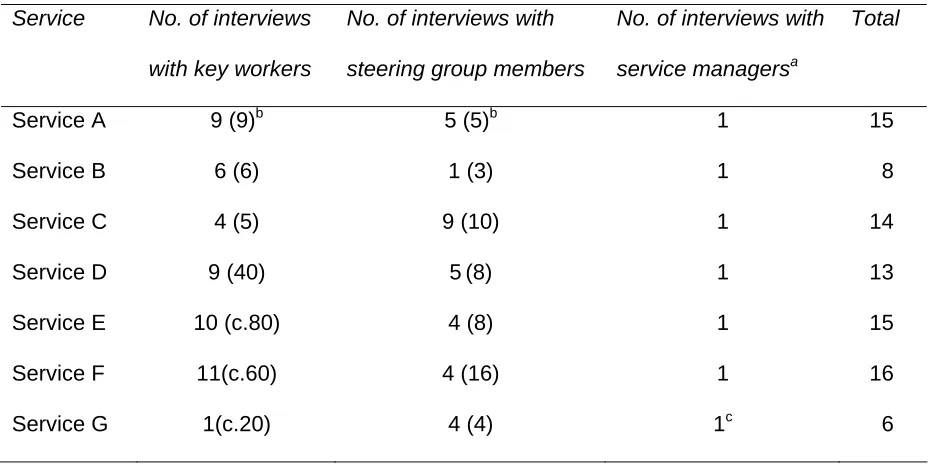
transcribed. Eighty-seven interviews, between six and 16 per site, were analysed
Table 1: Interviews conducted with staff
Service No. of interviews
with key workers
No. of interviews with
steering group members
No. of interviews with
service managersa
Total
Service A 9 (9)b 5 (5)b 1 15
Service B 6 (6) 1 (3) 1 8
Service C 4 (5) 9 (10) 1 14
Service D 9 (40) 5(8) 1 13
Service E 10 (c.80) 4 (8) 1 15
Service F 11(c.60) 4 (16) 1 16
Service G 1(c.20) 4 (4) 1c 6
a
In all sites except E, there was one service manager.
b
( ) = no. of key workers/steering group members in service
c
Joint interview with service manager and administrator who carried out much of the day to day running of the service.
Key workers came from a range of professional backgrounds. Social workers, health
visitors and community nurses were the most common professions, but therapists,
teachers, workers with voluntary agencies, Portage workers, nursery nurses, youth
workers, paediatricians and a dietician were also represented. In one service, a few
parents acted as key workers for themselves, supported by the service manager.
Service managers had professional backgrounds in health or social services.
Members of the steering groups included parents as well as representatives from all
Aims of the services
The basic aims of the services were similar across all seven services. These were:
identifying the needs of the child; providing key workers as a main point of contact for
the child and family; drawing up and reviewing a multi-agency care plan; working with
other professionals; providing information to families; and providing support for
families and helping them to access services.
Understanding of the key worker’s role
In four services, interviews with all staff showed clear agreement about what the key
worker role encompassed. These services defined the role as being the main source
of information, advice and support for families, enabling and empowering families,
overseeing and coordinating the implementation of the care plan and information
sharing between professionals. These services all had a clear written job description
for key workers. However, in the other three services different key workers
interpreted their role in different ways. Many key workers felt that the role was not
clear to them or they did not see any difference between the key worker role and
what they had always done. Some key workers expressed uncertainty about how
families and other professionals understood the role.
…and the key worker role I think is, is a little bit fuzzy, well I think
in everybody’s mind, certainly in mine.
In services where there were problems understanding the role, considerable
were clearly undertaking the role defined in earlier research (Mukherjee et al., 1999;
Tait & Dejnega, 2001) but others saw their role as more limited. Some did not feel
that they should be proactive in contacting families or that liaising with other
professionals on behalf of the family was part of their role. The following contrasting
accounts from workers in the same service illustrate this diversity in understanding:
I suppose my main idea of it is that it’s my responsibility to communicate
with all other professionals involved and make sure everyone’s up-to-date
…..and you’d like to feel that you’re the first person the family would turn to
if they’ve got worries. And I’d also feel a responsibility in getting the
problem sorted, even if it wasn’t in my area I would feel that was my job to
be acting as an advocate really for the family.
I’m not checking up on other professionals and their involvement in
families, that’s not my role.
Training
Three services had induction and regular ongoing training for key workers. Two
currently had no initial or ongoing training, although one of these had training
sessions in earlier years and plans were being made to reintroduce them. In another
service, some induction training was provided, consisting of one workshop when the
service first started; in the seventh service, each new key worker met the service
manager who explained the aims and nature of the service and what was expected
of them. This service manager also ran occasional sessions to explore key working in
In services with regular training, a wide range of topics was covered, including: law
relating to children, disability rights legislation, child protection, direct work, life story
work, charging policy, presentation skills, housing grants and benefits, Disability
Living Allowance, Motability, direct payments, statementing, the roles and working of
different agencies, what services are available and where to get information, and
team building. In addition to topics identified by service managers, key workers often
identified issues on which they required training and they spoke very positively about
the training received.
The training we've been given has been wonderful, it really has,
we've learnt a lot from it.
In services where key workers did not receive regular training, views were mixed.
Some felt that the training they received in their every day professional role was
sufficient; others expressed a need for training.
Supervision
The three services with regular training also had regular supervision specific to key
working. This was provided by the service managers between fortnightly and
six-weekly and was highly valued by the key workers.
It's excellent, you know. So...there are issues we go through,
issues about key working generally and, you know, the team, the
I need to, you know, I can go through every one of them and it's
really useful to say look I'm at loggerheads here, which she'll say
well have you tried doing that, you know.
In the other services, most key workers found that the supervision they received from
their line managers in their day-to-day professional role and support from other
professional colleagues was sufficient. However, some wanted more support and
guidance that related specifically to their key worker role.
Regular supervision was provided in services with between five and nine key
workers. In the larger services (40-80 key workers) the managers' contact with key
workers was more erratic. In some services, supervision was limited to the possibility
of telephoning the manager when a crisis occurred.
Peer support
In the three services that had key worker-specific training and supervision, there
were also regular opportunities for peer support. Members of two designated key
worker teams shared accommodation with each other, and one service with
non-designated key workers arranged regular training and group support meetings. Key
workers in these services particularly valued opportunities to meet and share
information and support. Key workers said having a diversity of professional
backgrounds in the team was an asset in providing a range of expertise. However
this synergy was possible only when key workers were given the opportunity to meet
Nobody knows everything and everybody has their weaknesses,
and that is the advantage of a true team where people are aware of
the weaknesses of others but they have their own strengths, which
compensate. So I think that’s the advantage of having people from
different disciplines…
Caseloads and contact with families
There was considerable variation in caseload size. Designated key workers
commonly worked with 20 to 40 families. In four of the services, non-designated key
workers worked with between one and five families in addition to their usual role and
caseload. In the other service, workers spent a greater proportion of their time on the
key worker part of their role and caseloads ranged from two to 25 families.
Key workers emphasised that the amount of time they spent on the key worker role
varied according to families’ levels of need at the time. Both designated and
non-designated key workers could struggle to cope if more than one family had a crisis at
the same time. Key workers found it difficult to estimate how much time they spent in
direct contact with families. Those who did make an estimate suggested that contact
with families took up about 25 to 50 per cent of their time, with related administration
and contacts with other services taking up the remainder.
Funding
Service managers and members of the steering group expressed that lack of funding
experiencing the most difficulties, there was no dedicated multi-agency funding for
the service. Managers and steering group members saw this as meaning that there
was no ownership of the service:
…but the problems have always been because no-one owns it,
there’s no money. I don’t know what it’s like in other areas but I
think my own view is that unless everyone’s on board with it then
it’s a very lopsided service…
Even where there was some multi-agency funding, problems could still arise over
which agency should fund resources or equipment needed by families. This was
frustrating for key workers who felt that these problems still needed to be sorted out
at strategic levels.
Where funding was committed from the three statutory agencies, inequities in
funding and the separation of funding streams, rather than pooled budgets, were
seen as barriers to good collaboration.
Role of the service manager
All services but one had a service manager who was responsible for the key worker
service. In three services, the role of the manager was to lead and develop the
service, supervise, support and organise training for key workers. In some cases,
managers also chaired planning and review meetings for children and families. Two
of these services had teams of designated key workers and one had both designated
related roles, however, it did not appear that these detracted from their management
of the key worker service. Supervision from these managers was highly valued.
They also saw developing a strong team spirit and motivating key workers as part of
their role and key workers valued this.
In one service with 40 non-designated key workers, the manager’s role included
organising planning and review meetings for families, chairing meetings, taking
minutes and preparing and distributing reports. She also provided support for key
workers and was regarded by them as very accessible and helpful. However, the
manager felt that it was not possible to provide regular supervision for such a large
number of key workers.
Service managers in the two remaining services had somewhat different roles. Both
had a role in overseeing the service but neither supervised, trained or had regular
contact with key workers. Both services had large numbers of non-designated key
workers (60-80). In one case, the manager chaired and coordinated planning and
review meetings for children, and some key workers felt that if a problem arose they
could contact the service manager. In the other case, one manager was responsible
for the implementation of four key worker teams in four areas of the county. Each
team had a manager, but responsibility for supervision of key workers rested with line
managers in their own agencies. Some key workers in this service felt that the team
managers were too busy to be contacted.
It was clear from interviews with key workers that accessibility of the service manager
was an important aspect of the service, but in non-designated key worker services
provide support or supervision and organise training.
Roles of the steering groups
In the initial stages of developing the services, multi-agency steering groups had
been instrumental in defining criteria and finding funding for the service. Most
continued to have a role in monitoring the service, reviewing and developing policies
and practices, and finding funding for new developments or expansion of the service.
A number of members highlighted the role of the group in ensuring a multi-agency
focus, raising awareness of the service in other agencies and addressing barriers to
multi-agency working.
All groups met regularly, varying between quarterly and once every two weeks.
However, in two areas there were concerns about poor attendance. Replacing
agency representatives who had left their agencies was identified as problematic in
both areas. In one area, poor attendance was also attributed to the fact that the
service was well established so people did not feel the need to prioritise the
meetings. In the other, there were concerns about lack of representation from some
agencies which meant that decisions could not be made, and it was felt that there
was a need for involvement from higher levels of management so that decisions
could be acted upon. In two areas, the groups' responsibilities were much wider than
the key worker service and the service was only a small part of the agenda.
Parent and child involvement
Five steering groups had between two and eight parent members per group, one
parent members but was planning to have parent representation. Nine parents were
interviewed in their capacity as steering group members. In all services, parents were
seen as an important force in keeping the group ‘grounded’, focussing on things that
affect families most, and providing a user perspective on the service. Generally,
parents felt that their views were listened to and respected, but a few suggested that
in reality they had little power and those who ‘hold the purse strings’ are the real
decision makers. None of the groups had children or young people involved,
although in one scheme young people had been involved when initially planning the
service. In one scheme, children were too young to be involved in consultation. In the
others, the high level of expertise and the considerable amount of time and effort
required to involve disabled children and young people in consultation meant that this
had not yet taken place. However, four groups were currently looking at ways for this
to happen.
Constraints and problems of the key worker role
A consistent theme among non-designated key workers was having insufficient time
to devote to the role. Many did not have dedicated key working time, and some felt
they were not doing justice to either role. Other constraints were engendered by gaps
in the provision of services in the areas and lack of resources. Problems in making
contact with other professionals, both to pass on and to obtain information, were
common. Some key workers felt that it was difficult to get other professionals to
understand their role and liaise with them.
Where key workers did not have regular supervision in their key worker role, lack of
support was at times problematic. Lack of relevant information and knowledge was a
confusion about the role of the key worker was cited as a problem in three areas.
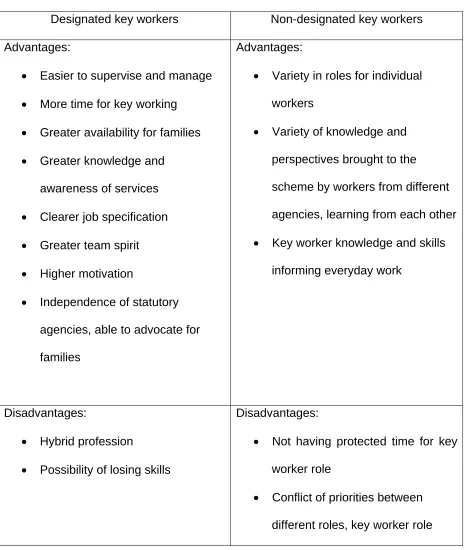
Type of key worker: designated or non-designated
Views on the advantages and disadvantages of designated and non-designated key
[image:20.595.67.535.225.775.2]workers are summarised in Table 2.
Table 2: Advantages and disadvantages of different types of key workers
Designated key workers Non-designated key workers
Advantages:
• Easier to supervise and manage
• More time for key working
• Greater availability for families
• Greater knowledge and
awareness of services
• Clearer job specification
• Greater team spirit
• Higher motivation
• Independence of statutory
agencies, able to advocate for
families
Advantages:
• Variety in roles for individual
workers
• Variety of knowledge and
perspectives brought to the
scheme by workers from different
agencies, learning from each other
• Key worker knowledge and skills
informing everyday work
Disadvantages:
• Hybrid profession
• Possibility of losing skills
Disadvantages:
• Not having protected time for key
worker role
• Conflict of priorities between
taking second place
• Not being 'an expert in everything'
• Not using key worker skills all the
time
• Uncertainty about role
• Little contact with other key
workers
• Juggling two roles
• Failure to know difference
between two roles
The disadvantages identified for designated key workers were seen as a risk of the
role but had not been experienced by the key workers interviewed. Some of the
disadvantages identified for non-designated workers may be overcome by better
management of the services, for example, by having a clear job description, training
and supervision, and agreements on protected time for key working with line
managers.
Advantages, disadvantages and suggested improvements to the service
Key workers identified a number of advantages for themselves: opportunities to build
good relationships with families; being able to 'make a difference' for families;
learning new skills and increased knowledge about children and families and other
services; and developing effective frameworks for information exchange with other
Perceived advantages for families of having a key worker were centred around
having one person to contact about any concerns, someone who was in charge of
coordinating services and making sure needs were met, and not having to keep
telling their story to different professionals. Respondents felt that this resulted in
greater consistency and continuity of care and thus stress was alleviated.
Advantages of the service for other professionals also centred around having one
point of contact regarding a family, being a source of information and knowing what
all agencies were doing with regard to a family. Key workers were seen as ‘lightening
the load’ and reducing pressure on other professionals.
Most of the disadvantages mentioned for key workers themselves concerned
non-designated key workers (see above). It was also acknowledged that key working is a
demanding role, key workers were at risk of becoming too emotionally involved and
having appropriate support in the role was important.
Improvements needed in some services were already valued features of other
services. These include:
• Clear description of the role of the key worker
• Administrative support
• Regular training and supervision for key workers
• Register of information about services for key workers and families
• Opportunities for key workers to exchange information and experiences
• A manager who can devote time to supervising the service.
There were some improvements that none of the services had fully managed to
achieve. Non-designated key workers wanted protected time for key working and, in
some cases, more negotiation with their line managers about how much time they
could spend on their key worker role and reductions in case loads in their main jobs
to allow this. Some services recognised the need to involve children and young
people in planning the service but none had done this as yet, and key workers
wanted guidance on consulting with disabled children and young people.
Discussion
The research is timely given the recent emphasis on providing key workers for
families with disabled children in the Early Support Programme (Department for
Education and Skills/Department of Health, 2004), the Children's National Service
Framework (Department of Health/Department for Education and Skills, 2004) and
Improving the Life Chances of Disabled People (Cabinet Office, 2005).
Findings show similarities with Abbott et al's. (2005) study on the impact of
multi-agency working on professionals. For example, Abbott et al. showed that clear
guidelines on the nature of the key worker role were often not available and having
peer support with key workers from other professional backgrounds was helpful.
However, that study found that key workers did not report a detrimental impact on
their ability to manage their workload. On the contrary, staff in this study found key
working required extra time and effort, and lack of time to perform this role was a
The findings of the study must be viewed in the context. The study is limited to a
snapshot in time and some of the services will already have changed by expanding
their staff or instituting training. The services in this study were focused on disabled
children with complex needs and we are not able to comment on issues concerning
key working for other groups of children. In addition, interviewees were self-selecting
and interviews with steering group members were difficult to achieve in one service
and in another only one key worker agreed to be interviewed. Potentially a more
varied perspective might have been obtained in services where a higher proportion of
staff was interviewed. However, overall there was a wide range of views within and
between staff in the different services.
The study showed that although the basic aims of the services were very similar, the
processes used to achieve those aims were different. Many staff were positive about
the advantages of the services for families and for themselves. However, there were
some crucial differences between services affecting how well they were viewed and
the problems encountered by staff. Services varied in the understanding of the key
workers’ role, the amount of training key workers received, whether they received
supervision or not, their opportunities to meet other key workers, level and stability of
funding, and the roles of the service manager and steering group.
Based on these findings, a number of recommendations can be made. Having a
clear, written job description for key workers helps to clarify the key worker role for
key workers themselves and other professionals. Key workers also need to have a
clear understanding of their role in order to explain it to parents, so that families know
showed that in services where there was confusion among key workers about the
role, parents were equally confused and different parents had very different
experiences of the same service (Greco et al., 2005).
Key working crosses the boundaries of different agencies and disciplines. The key
worker is the main point of contact for families, and needs to have a broad
knowledge of disability, other agencies' and professionals' roles, what services are
available locally and nationally, and where to find information. The role can also be
very demanding, and support structures need to be in place for key workers. These
include specific and ongoing training focused on the key worker role; supervision
specific to the role; opportunities for contact with other key workers; and agreement
on time for key workers to undertake the role. The findings suggested that the service
manager plays a central part in leading and developing the service and supporting
key workers, and needs sufficient time for running the service.
Staff in services with no dedicated funding spoke of the problems of lack of
ownership of the service and it is clear that dedicated funding, at least for a manager
and a training budget, is crucial. Steering groups could provide strong multi-agency
backing for the service and facilitate collaboration. However, managers on these
groups should be senior enough to make decisions, and able to prioritise steering
group meetings. Efforts must be made to ensure that parent representatives on the
steering group have a say in decision-making and do not feel powerless when
The findings indicate that staff in services where the above factors were in place
were most positive about the service. Where they were not in place, they were
identified as improvements needed in the service. Professionals interviewed in this
research generally felt that, as indicated in earlier research (Liabo et al., 2001), key
working was a way of providing a better and more effective service. However, with
the recent growth in key worker services (Care Coordination Network UK, 2005) it is
References
Abbott D., Townsley R., & Watson D. (2005) Multi-agency working in services for
disabled children: what impact does it have on professionals? Health and Social Care
in the Community 13, 155-163.
Appleton P., Boll V., Everett J.M., Kelly A.M., Meredith K.H. & Payne T.G. (1997)
Beyond child development centres: care coordination for children with disabilities.
Child: Care, Health and Development 23, 29-40.
Beresford B. (1995) Expert Opinions: a national survey of parents caring for a
severely disabled child. Policy Press, Bristol.
Cabinet Office (2005) Improving the Life Chances of Disabled People. Prime
Minister's Strategy Unit, London.
Care Coordination Network UK (2005) Survey of care coordination schemes.
www.ccnuk.org.uk
Chamba R., Ahmad W., Hirst M., Lawton D. & Beresford B. (1999) On the Edge:
minority ethnic families caring for a severely disabled child. Policy Press, Bristol.
Court Report (1976) Fit for the Future: The Report of the Committee on Child Health
Department for Education and Skills/Department of Health (2004) Early Support:
Professional Guidance. DfES Publications, Nottingham.
Department of Health/Department for Education and Skills (2004) National Service
Framework for Children, Young People and Maternity Services: Disabled Children
and Young People and those with Complex Health Needs. Department of Health,
London.
Greco V. & Sloper P. (2004) Care coordination and key worker schemes for disabled
children: results of a UK-wide survey. Child: Care, Health, and Development 30,
13-20.
Greco, V., Sloper, P., Webb, R. & Beecham, J. (2005) An Exploration of Different
Models of Multi-Agency Key Worker Services for Disabled Children: Effectiveness
and Costs. DfES Publications, Nottingham.
Liabo K., Newman T., Stephens J. & Lowe K. (2001) A Review of Key Worker
Systems for Disabled Children and the Development of Information Guides for
Parents, Children and Professionals. Office of R&D for Health and Social Care,
Cardiff, Wales.
Mukherjee S., Beresford B. & Sloper P. (1999) Unlocking Key Working. Policy Press,
Prestler B. (1998) Care coordination for children with special health needs,
Orthopaedic Nursing March/April (Supple.)
Sloper P. (1999) Models of service support for parents of disabled children: What do
we know? What do we need to know? Child: Care, Health and Development 25,
85-99.
Tait T. & Dejnega S. (2001) Coordinating Children’s Services. Mary Seacole
Research Centre, De Montfort University, Leicester.
Taylor S. & Bogdan R. (1984) Introduction to qualitative research methods: The
Acknowledgements
The study was funded by the Department of Health, Department for Education and
Skills, HM Treasury, and Welsh Assembly Government. The views expressed here
are those of the authors and not necessarily those of the funders. We would like to
thank all the staff who gave their time to participate in interviews, Sheila Sudworth
who carried out some of the interviews, and the project advisory group who provided