RIT Scholar Works
Theses
Thesis/Dissertation Collections
6-30-1998
ABA/Lovaas treatment for autism and pervasive
developmental disorders in the Monroe County
area
Kelly Byrne
Follow this and additional works at:
http://scholarworks.rit.edu/theses
This Thesis is brought to you for free and open access by the Thesis/Dissertation Collections at RIT Scholar Works. It has been accepted for inclusion
in Theses by an authorized administrator of RIT Scholar Works. For more information, please contact
ritscholarworks@rit.edu.
Recommended Citation
ABA/-
Lo.w.a,s
1
ABA/ Lovaas Treatment for Autism and Pervasive Developmental
Disorders in the Monroe County Area
Master's Project
Submitted to the Faculty
of the School Psychology Program
College of Liberal Arts
ROCHESTER INSTITUTE OF TECHNOLOGY
By
Kelly
J.
Byrne
In
Partial Fulfillment of the Requirements
for the Degree of
Rochester, New York
June
30, 1998
Approved: _ _....;:.:Je:.:..;n:.:..:n~ife~r...;;;L~u~ko~m~s;.;.;k~i
:--
:--_
(Comm ittee.. Chair)
Nicholas DiFonzo
School Psychology Program
Permission to Reproduce Thesis
jf\
K
~
VY\v
f\
(cJ
£
(,{ )V\
V"\k-r----=:...!..:...~e...::.~~---I
k!
fld
J
~
A1<.1
Aff~
hereby grant permission to the
Wallace
Me~bra';ymhe
Rochester Institute of Technology to reproduce my
thesis in whole or in part. Any reproduction will not be for commercial use or profit.
Date:
tR
I
~
I
q
~
Signature of Author:
PERMISSION FROM AUTHOR REQUIRED
Title of thesis
_
I
prefer to be contacted
each time a
request for reproduction is made. I can be reached at the following address:
PHONE:
_
Date:
_
Signature of Author:
_
________________________________________________________________________________~~ O O__~"_._.Q~~Q_0 _
I
PERMISSION
DENIED
TITLE OF THESIS
_
I
hereby deny permission to theWallace
Memorial Library of the Rochester Institute of Technology to reproduce my
thesis in whole or in part.
ABA^
Lovaas 2
Table
ofContents
List
ofTables
andFigures
/
4
Abstract
/
5
literature
Review
/
6
Introduction
/
6
Autism
/Pervasive
Developmental Disorder
/
7
Description
ofLovaas
Therapy
/
8
History
ofLovaas
Therapy
/
11
Controversy Surrounding
Research
andLovaas Behavioral
Interventions/
15
Current Legal Issues
/
16
Introduction
to
Other Treatment
Approaches
/
17
Rational
for
Project
onABA/
Lovaas
Treatment
for
Children
withAutism/
19
Project
Overview
/
22
Community
Contribution
/
22
Project
Design
andReview
ofObjectives
/
24
Rptuilts/DiqnistJnrL
Section./
29
Sample Demographics
/
29
Applied Behavior Analysis Programs
/
31
Additional Treatment Methods
/
39
Making
the Decision to
Use ABA
/Lovaas
/
41
ABA
/Lovaas'Impact
onthe
Family
/
45
Positives
andNegatives
ofABA /Lovaas
/
45
What Parent's
Need From
the
Monroe
County
Community
/
46
Parent's Experiences
withFunding
ABA /Lovaas Programs
/
46
Summary
/
47
References^
49
Appendix A:
Letter
from
RACE
Group
/
54
Appendix B:
ABA/Lovaas Parent
Survey
/
56
ABA/
Lava
a^s4
List
ofTables
1.
Sample
Demographics
/
30
2.
Information
onApplied Behavior Analysis
Programs
/
32
3.
Reasons
for
Change in Program Hours
/
34
4.
Professional
Composition
ofABA
Teams
/
37
5.
Consultant Hours
/
38
6.
Other Treatment Programs
/
40
7-
Source
ofEirst
Laformation-
on-ABA
/
42
8.
Reasons
for
Choosing
ABA/
Lovaas Treatment
/
43
Abstract
The
purpose ofthis
project wasto
provide schoolpsychologists,
and otherprofessionals,
an overview ofthe
ABA/
Lovaas
programsbeing
implemented
in
the
Monroe
County
area(upstate
New York). Parents
weresurveyed,
in
orderto
gatherinformation
onthe
Applied Behavior
Analysis/
Lovaas
methodthey
areusing
to
treat
their child.To
provide additionalinformation
aboutthe
childrenparticipating
in
the project,
adirect
observation ofthe
child was conducted and arating
scale wascompleted
(Childhood
Autism
Rating
Scale). Ten families
participatedin
the
project,
with the child's agesranging
from
37
monthsto
66
months.Project
resultsindicate
that
parent's areinvesting
large
amounts oftime
andenergy
in
these
programs.
In
allcases,
parents reportedcombining
ABA/Lovaas
programs withother
forms
oftreatment
(i.e.,
preschool,
drug
therapy,
musictherapy,
dietary
treatments,
etc.).Parents
aregenerally reporting
positivefeelings
aboutthe
treatment,
althoughthey
areexperiencing
some concerns around programfunding,
ABA/
Lovaas
6
Literature
Review
Introduction
"Scarcely
a monthhad
passed sinceAnne-Marie's
first diagnosis [of
autism],
but
it
felt
morelike
six.Every
single nightMarc
andI
readbooks
and articles aboutautism,
racing
againstthe
days,
racing
to
find
someway
ofhalting
her
inexorable
progressionbackwards"(Maurice,
1993).
The
above words were writtenby
Catherine
Maurice,
author ofthe
book Let
Me Hear Your
Voice.
Ms.
Maurice
writes ofthestruggle she andher
family
faced
while
trying
to
find
away
to
help
their autisticdaughter. These
words couldhave
been
writtenby
any
parentfacing
the
struggle ofraising
andeducating
a child withautism.
The Maurices
optedto teach
Anne-Marie
using behavioral
principals,
specifically
the
behavioral
educational plandeveloped
by
O.
Ivar
Lovaas. In
her
book
she writes ofthe
success and gainsboth
ofher
autistic children made whentaught
by
this
method.In
additionto
Ms. Maurice's
descriptive
account ofher
children's
recovery,
casestudy
articleshave
been
printed onthe two
siblings(Perry,
Cohen,
&
DeCarlo,
1995b). Although
professionalsin
the
field
have
warnedthe
public notto
viewthe
Maurices'
progress as
typical,
her book has become
a catalystfor many
parentsto
research andemploy
Lovaas
methods withtheir
children(Shapiro
&
Hertiz, 1995; Ryan,
1995).
As
more and more children arediagnosed
with autism/Pervasive
Developmental Disorder
(PDD),
the
question ofhow
to
treat
the
disorder
becomes
more urgent.
In
the
Monroe
County,
located in
upstateNew
York,
parents and professionals areturning
to
treatments
based
onbehavioral
principles(Applied
treatment
methodsbecome
morepopular,
county
agencies and schooldistricts
arefaced
withthe
challenge offunding
the
programs anddeciding
whobenefits
from
such services.
This has
created muchcontroversy
and muchdiscussion
overthe
appropriateness and effectiveness of
Lovaas/
ABA
programs.Autism
/Pervasive Developmental
Disorder
Fifty
yearsago,
Leo Kanner identified
"autism" as a syndrome ofdisorders
characterized
by
socialisolation,
language
problems,
and a restricted range ofinterests
(Bauer,
1995a &
1995b;
Diagnostic
andStatistical Manual Fourth
Edition,
1994).
Autism
has been
misunderstood andclinically hard
to
define.
Historically
it
was considered a
"childhood
schizophrenia,"and
thought
to
be
causedby
poorparenting (Rutter
&
Schopler,
1987).
Other
theories
onthe
"single
coredeficit" of
autism are
that
it is
causedby
sensory
difficulties,
biological
problems,
language
andcognitive
deviances,
and socialimpairments
(Smith,
McEachin,
&
Lovaas,
1993).
Today,
autismis
seen asexisting
more on a spectrum(Rimland,
1993;
Wing
&
Gould,
1979).
The
term
Pervasive Developmental Disorder
(PDD)
is
frequently
usedto
describe
the
range andseverity
ofthe
"autistic
like"symptoms a child
displays
(Rutter
&
Schopler,
1992).
Many
researchersfeel
that
there
is
no singleetiology
for
autism,
and childrenmay
have different
impairments
that
arecausing
the
autisticcharacteristics
(Wing
&
Gould, 1979;
Phelps &
Grabowski, 1991;
"Interview
withIvar
Lovaas,
1994).
In
1980,
autism was recognized as adistinct developmental
disorder
in
the
DSM-III
(Bauer,
1995a & 1995b).
Initially,
autism was placed onAxis
II,
indicating
that
it
wasconsidered astable,
unchanging
conditionthat
had
a poorprognosis.In
ABA/
Lovaas
8
transient
conditions(Edelson).
This
movement,
along
withthe
acceptanceby
many
professionals ofthe"autism
spectrum"has
resultedin
more childrenbeing
diagnosed
as autistic orPDD
(Bauer,
1995a
&
1995b). Treatment
modalitieshave
been
revisedto
address abroader
range ofbehaviors
associated withautism,
but
nosingle
therapeutic
intervention has
yetbeen
identified
asthe
"cure"for
autism.As
aresult, the
professionalcommunity
andfamilies
of children with autism aregrappling
withthe
choice of whattreatment
strategiesto
use.Description
ofLovaas
Therapy
Behavioral
treatments,
such asthat
developed
by
Ivar
Lovaas,
arebased
ontheories
of operantconditioning
and appliedbehavior
analysis(ABA) (Lovaas,
1981). Rutter
describes
it
as"a
matter of ....encouraging
progressin
the
rightdirection
through the
use ofdifferential
reinforcement and ofdirect
teaching
that
providethe
skillsneeded"
(1985).
Techniques
such asshaping, prompting,
fading,
extinction,
andthe
use ofprimary
andsecondary
reinforcers are usedto
teach the
child a wide range ofbehaviors
and skills(Rutter,
1985; Lovaas,
1981). In
addition,
Lovaas
endorsedthe
use ofaversives,
particularly
to
end self-injuriousbehavior.
The ABA
approachto
teaching
children with autism stemsfrom
the
belief
that
they
do
not appearto
learn
from
their
environmentlike
typical
childrendo. While
the
average child
takes in information
continuously
(every
waking
minute,
365
days
ayear),
the
child with autism needsto
be
taught the
skillsto
learn
from
the
world aroundthem.
The
structure andintensity
ofthe
Lovaas
programis
an attemptto
teach them
basic
learning
principals,
andto
"make-up"for lost
learning
time
(Lovaas,
1987;
Lovaas,
1981).
philosophy,
techniques,
and educational programsthat
arethe
foundation
for
today's
Applied Behavior Analysis
(ABA)
approachto
treating
autism.The book
is
organized
into
five
sections,
which are asfollows:
(1)
Unit I
teaches
parents andteachers
the
basics
of appliedbehavior
analysistechniques,
(2)
Unit II
containsprograms
(of
individual
lessons)
that
preparethe
childto
learn,
(3)
Unit III
introduces
basic
verballanguage
andplay
skills,
(4)
Unit IV
teaches
self-help
skills,
(5)
Unit V
presents more advanced and complicated verballanguage,
(6)
Unit
VI
focuses
on abstract verballanguage,
and(7)
Unit
VII
teaches the
studenthow
to
function
in
school andcommunity
settings.Parents
are advisedto
order a series ofvideo
tapes,
to
help
supplementthe
instructions
containedin
the
training
manual(Lovaas,
1981).
Although
parents are consideredthe
main serviceproviders,
it is
recommended
that
they
develop
a"treatment
team"
of at
least
three
peopleto
help
provide services
to their
child("Lovaas
revisited: should wehave
everleft?,
1995;
Lovaas
1981). Parents
andtreatment teams
are guidedby
a consultanttrained
in
Lovaas
/ABA
therapy.
Each
programis
designed
to teach
suchthings
assitting,
receptivelanguage,
and verbal
imitation. Within
each program are smaller stepsthat
they
child mustmaster
before
the
skillis learned.
These
smaller steps are called"discrete trail
training,"
because
they
start with ateacher's
instruction
and end withthe
child'sresponse
(Lovaas,
1981).
A
well coordinatedteam
mustensure,
by
the
use of videotaping
orby
direct
observation, that
they
are allusing
the
same commands and samelanguage
whileteaching
the
child(Lovaas,
1981).
In his
originalstudies,
Lovaas
recommended
that
the
child receive a-minimum-of 40-hours-
ofdirect
one-oiv-Qneinstruction
per week(Lovaas,
1987).
As
willbe
discussed,
the
evolution ofABA
ABA/
Lovaas, 10
instruction is
appropriatefor
eachindividual
child.Discrete
trial
training
consists ofthree
components.They
are asfollows:
"
(1)
presentation of a
discriminative
stimulus(i.e.,
a request or acommand);
(2)
aresponse
(what
the
individual does
following
the
request orcommand);
and(3)
presentation of
reinforcing
stimulus,
defined
in
this
program as a rewardif
correct,
saying
"no"if
incorrect"("Lovaas
revisited: should we everhave
left?,"1995).
Although individual
needsvary from
childto child,
instruction
usually
consists of4
to
6
hours
perday,
5
to
7
days
perweek,
for
a minimum oftwo
years.Within
asession
the
child might workfor
2
to
5
minutes,
andthen
be
rewardedfor working
appropriately
anywherefrom
several secondsto two
minutes .After
eachhour,
the
child
is
generally
given a15 to
20
minutebreak
("Lovaas
revisited: should we everhave
left?/'1995^.
Lovaas^
L981X-
ba
orderto
makethismodel work,,it is.
essentiaLforparents and
teachers
to
identify
whattypes
ofthings
are "rewards"for
their
child.Some
children mightbe
willing
to
workfor
food,
while others will preferbeing
rewarded
for
the
opportunity
to
engagein
some physicalactivity
(Lovaas,
1981).
Another
emphasis ofthe
Lovaas
methodis
early
intervention. Lovaas
proposed
in
his first
study
(1973)
that
the
youngerthe
childwas,
the
better
progressthey
would make(Lovaas,
Koegel, Simmons,
&
Long,
1973).
Some
researchershave
suggested
that
thisis
true
because
the
brain
plasticity
of younger childrenis
greaterthan that
of older children(Perry,
Cohen,
&
DeCarlo,
1995a).
Early
intervention
is
successful
for
avariety
ofreasons,
such as:(1)
Early
development
is
a criticaltime
to
acquire communication
skills,
for both
the typical
child andthe
child withautism;
(2)
Younger
childrenhave limited
learning
histories,
andtheir
behaviors
areless
complex;
(3)
Since
younger children need much care andattention,
parents arechildren are easier
to
physically
control(Dunlap
&
Fox,
1996).
Although
Lovaas'book does
notdelineate
anideal
ageto
startbehavioral
intervention,
in
his 1987
study he limited his
subjectsto
children under the age of40
monthsif
mute,
and underthe
age of46
monthsif
echolalic.Most
childrenin
ABA
programs are aroundthe
age of3 1/2
years("Lovaas
revisited: should we everhave
left?,"1995).
As
willbe
discussed,
there
is
muchcontroversy
over what agethe
child stops
benefiting
from
intensive behavioral
intervention.
Although
it
wasthought
to
be
appropriateonly
for
young
children,
researchers arestarting
to
suggestit
may benefit
older autistic students as well("Intervention:
it
doesn't
needto
be
early,"
1995).
History
ofLovaas
Therapy
O. Ivar
Lovaas
had many
years of experienceworking
with children withautism
before
he
presentedthe
ABA
program asit
existstoday.
He
dedicated his
professional careerto
researching
andtreating
children with autism.When Lovaas
first
began his
research,
he
wasinterested in
learning
abouthow
acquiring language
effects a child's non-verbal
behavior
(Lovaas,
1993). While
searching
for
agroup
ofchildren who were
lacking
meaningfullanguage,
Lovaas
wasintroduced
to
childrenwith autism.
From
that
point onhis
careerfocused
ontreating
andresearching
this
population.
(Lovaas,
1993).
Using
his
training
as abehavioral
clinicalpsychologists,
Lovaas
workedto
establish empirical evidenceto
supporthis
claimthat
abehavioral
method ofintervention
wasthe
best way
to
improve
the
lives
ofthese
children
(Lovaas,
1993).
Using
behavioral
principalsto
educate childrenis
nota new concept.Researchers
have found
behavioral
techniques to
be
effective withtypical children,
ABA/
Lovaas,
12
revisited: should we ever
have
left?,"1995). Lovaas
acknowledgesthat
his
approachto
treating
autismis
notbased
on newlearning
techniques
(Lovaas,
1993).
As
willbe
discussed,
his
programis
most notablefor
its
intensity
and structureddelivery.
Various
treatments
have been developed
to
help
children with autism(i.e., "play
therapy,
operantconditioning,
specialdiets,
megadoses ofvitamins,
psychoactivedrugs,
electricshock,
signlanguage
training,
residentialtreatment,
perceptualtraining,
motortraining,
mainstreaming,
specialeducation,
andothers")
(Schopler,
Mesibov,
&
Baker,
1982).
However,
many
professionals agreethat
using
abehavioral
approachto
treating
autismholds
the
most promise(Rutter,
1985;
Lovaas,.
1987;
"Lovaas
revisited: should we everhave
left?,"199,5).
Lovaas'
first
attemptto
usebehavioral
principalsto treat
children withautism
had limited
success(Lovaas, Koegel, Simmons,
&
Long,
1973).
In 1973
Lovaas
designed
abehavioral
programto treat
20
children with autism.Specific
ages ofthe
children
involved in
the
study
were not reportedin
the
literature.
Students
wereidentified
onthe
basis
of apparentsensory
deficits,
affectiveisolation,
self-stimulatory
behavior,
mutism,
echolalicspeech,
and a poor receptivelanguage
(Lovaas,
Koegel, Simmons,
&
Long,
1973).
The
use of aversives(such
asspanking,
aslap
onthe
thigh,
or aloud
"no")
was usedto
eliminate self-injuriousbehavior
(Lovaas,
Koegel, Simmons,
&
Long, 1973; Lovaas,
1993).
The
children were placedin
four
treatment
groups.The
groups variedin
the
intensity
ofthe
treatment
delivered,
amount ofinstruction
they
received,
and whodelivered
the treatment
(therapist
vs. parents).Overall,
the
study
suggestedthat
whentaught
using behavioral
principles,
subjects made great gains
in
learning
appropriatebehavior
and communicationmade
during
treatment.
Lovaas
concludedthe
following:
(1)
Age
may
be
animportant
factor
in
determining
which childrenbenefit
from behavioral
treatment.
Lovaas
noted thatthe
older childrenin
his study
had
difficulty
withgeneralizing
new skillsto
different
environments.He
proposedthat
younger children would
"discriminate
less
wellthan
olderchildren,
hence
generalize and maintain
the therapeutic
gainsto
a more optimal degree"(Lovaas,
Koegel, Simmons,
&
Long, 1973);
(2)
The
treatment
is
most successfulif
it
nrnirsin
rhp rhild's nahiralenvironment.
The
childrenin
the
study
who returnedto
stateinstitutions
aftertreatment
regressedto
a greaterdegree
than
children who returnedhome
to
parentstrained
in
behavioral
techniques.
(Lovaas, Koegel,
Simmons,
&
Long,
1973).
Lovaas
concluded
that
the
environmentthe
childfunctions
in.
mustbe
structured sothat
it
maintains
the therapeutic
gains madeby
the
childduring
treatment;
and(3)
Parents
canbe
utilized astreatment therapists.
As
mentionedabove,
the
parents
trained
in behavioral
techniques
helped
their
children maintaintreatment
gains.
Lovaas identified
the
following
parent characteristics as essential:"A
willingness
to
usestrong
consequences...,
a willingnessto
deny
that
their
childrenare'ill'
[put
responsibility
onthe
child]...., the
willingnessto
commit a major part oftheir
lives
to their
children andto
exercise somedegree
of contingent managementthroughout
the
day"(Lovaas,
Koegel, Simmons,
&
Long,
1973).
Lovaas
appliedthis
knowledge
to
his
1987
study.The
Young
Autism
Project
began in
1970
atthe
University
ofCalifornia
atLos Angeles
(UCLA).
Subjects
wereassigned
to
an experimentalgroup
and a controlgroup,
onthe
basis
ofthe
availability
of staff members.Random
placement was not ethical or acceptableto the
ABA/Lovaas,
14
with autism
from
atreatment
program not connectedto
UCLA. Participants
had
achronological age of
less
than
40
monthsif
they
weremute,
andless
than
46
monthsif
they
possessed echolalic speech.Intelligence
was also afactor.
Participants
had
aprorated mental age
(deviation
IQ)
of11
months or more.The
childrenin
the
experimental
group (n
=19)
received over40
hours
ofintensive
behavioral
treatment
per weekin
the
home,
for
a minimum oftwo
years.An
emphasis wasplaced on parent
involvement
and parent education.The
childrenin
controlgroup
#1
(n
=19)
received10
hours
ofbehavioral
treatment
perweek,
and wereinvolved
in
community based
interventions
(special
education,
preschool).The
childrenin
control
group
#2
(n
=21)
were nottreated
by
any
professionals associated with theYoung
Autism Project
(Lovaas,
1987).
The
results ofthis
study
wereto
create muchcontroversy among
professionals who specialized
in
autism(Schopler,
Short,
&
Mesibov,
1989; Foxx,
1993;
Kazdin,
1993;
Mesibov,
1993;
Mundy,
1993
).
Lovaas
claimedthat
out ofthe
19
subjects
in
the experimentalgroup,
9
children,
or47%
ofhis
sample,
achievednormal
functioning. Normal
functioning
was measuredby
placementin
a regulareducation
first
gradeclassroom,
andby having
averageintellectual
functioning
(as
measured
by
a standardizedtest).
In
Control
Group
#1,
only
one student achievednormal
functioning.
In 1993
anotherstudy
was conductedto
look
atthe
long
term
effects,of
Lovaas'
method of
behavioral
intervention.
(McEarhin,.
Smith, &_Lavaas,
1993;
"Long
term
follow-up:
early
intervention
effectslasting,"
1993).
Approximately
six years after
the
participants ofthe
1987
study
achieved"normal
functioning,"they
were evaluated
to
assessif
the
gainsthey
made were permanent.Only
one studentfrom
the
best
outcomegroup
neededto
be
movedfrom
a regular education classto
aautism was successful and created permanent positive change
(McEachin,
Smith,
&
Lovaas, 1993;
"Long
term
follow-up: early
intervention
effects lasting,"1993).
Controversy
Surrounding
Research
andLovaas Behavioral
Interventions
Although
Lovaas'claim of a
47%
success rate generated muchexcitement,
it
also generated much controversy.Concerns
and additional explanations aboutLovaas'
research, andmethods si i rfa rpd
in
thrppmain areas:(a)
Assignment
to the
Experimental
Group
was notRandom. One
ofthe
major criticisms of
the
1987
study
wasthat
subjects were not assignedto
the
experimentalgroup
or controlgroup
in
a randomfashion
(Schopler,
Short &
Mesibov,
1989).
Schopler, Short,
andMesibov
(1989)
questioned whether or notthe
controlgroup
was comparableto
the
experimentalgroup, in
terms
of parentalinvolvement
andthe
amount of attentionthey
received.(b)
Subjects
Not
anAverage Sample
ofChildren
withAutism.
Schopler,
Short,
andMesibov
(1989)
madethe
argumentthat
Lovaas
choose agroup
of subjectsthat
had
abetter
prognosisthan
the
average population of children with autism.The
claimhas
been
madethat tests that
generally
yieldlow
scoresfor
children with autism were chosenfor
pretreatmentdata
collection.His
samplehad
an average
IQ
higher
than
the
average child with autism.The
older childrenin
the
study (40
monthsto
46
months)
were chosenonly
if
they
were echolalic(generally
considereda sign of abetter
prognosis).(c)
Follow-Up
Measures
Did
notMeasure "Normal
Functioning."
Several
professionals
have
questioned whether"school
placement,
standardizedIQ
measures^
andasranHarHi7pHsocial/
emotionalmeasure"
were
true
measures,of whether or notany
residual autistic characteristics remained(Schopler,
Short,
andABA /Lovaas
16
many
flaws,
because districts vary
in
their
inclusion
andmainstreaming
policies.In
addition,
many
ofthe
childrenin
the
"best
outcome"group had strong
parent andteacher
advocates(Foxx,
1993; Schopler, Short,
andMesibov,
1989).
Lovaas
was alsocriticized
for
overlooking
several elevated scores onthe
social/emotional
measurethat
suggestedthese
studentshad
some emotional and cognitive problems(Mundy,
1993).
In
various responsearticles,
Lovaas
has
answered each concern raisedby
other professionals
(Lovaas,
Smith,
&
McEachin, 1989; Lovaas,
1993). In
many
instances
he
refersback
to
his
original research as evidencethat
his
methodologieswere sound.
Although
there
is
controversy
over the47%
success rate ofthe
1987
study,
all professionals agreethat the
study
needsto
be
replicated andimproved.
As
of1993,
three
replication sites were established acrossthe
country
(Smith,
McEachin,
&
Lovaas,
1993).
There
aremany
concerns aboutreplicating,
such asthe cost, the
length
oftime that
mustbe
dedicated
to the
study,
andthe
lack
of professionals whohave
intensive
training
in
behavior
modification(Smith,
McEachin,
&
Lovaas,
1993).
In
a1993
article,
Alan
Kazdin
proposedthat
replication studies shouldhave
the
following
things:
(1)
Random
assignmentto the
experimentalgroup
and controlgroup;
(2)
A
larger
samplesize;
and(3)
Use
of a standarddiagnostic
battery
thatsamples a
full
range ofdisorders
and evaluatesthe
severity
ofthe
child's autisticfeatures.
(Kazdirv
1993).
Current
Legal Issues
As
was mentionedpreviously,
Lovaas
programshave
createdlegal issues
for
parents and school
districts.
According
to
PL94-142,
districts
are requiredto
provideall students with
"Free
andAppropriate Public
Education"
(FAPE)
("When
methodologies
collide,"
the
issue
of whatis
an "appropriate" and effective programfor
children withautism.
Due
to the
intensity
and specializedtraining
ofthe
Lovaas
consultants,
ABA
programs are costly.
It is
reportedthat
in
Maryland
programs can rangefrom
$20,000
to
$22,000
at year("Requests
for Lovaas
therapy,"1995). In California
services canrange
from $1,000
a monthto
$6,000
amonth,
depending
uponthe
expertise ofthe
consultant
("Requests for Lovaas
therapy,"1995). Although
the
decision
about whatconstitutes
FAPE
is
left up
to
state agencies andlocal
schooldistricts,
many
parentsare
initiating
due
process andentering
into impartial
hearings
("When
methodologies
collide,"
1995).
If
parents can convince ahearing
officerthat
the
Lovaas
methodis
superior and more effectivethan
programs providedby
the
district,
they
are awarded reimbursement and/or
funding
for
their
home-based
therapy
("When
methodologiescollide,"
1995). As
parents startto
winthese
hearings
(i.e.,
Delaware
County
Intermediate Unit
v.Martin
andMelinda
K.
andMA.
v.Vorhees
Township
Board
ofEducation),
districts
arefaced
withchoosing
between
costly
court expenses orfunding
an expensive program with unknowneffectiveness
("Requests
for
Lovaas
therapy,"
1995).
Introduction
to Other Treatment Approaches
As
was mentionedpreviously,
there
aremany
treatment
choicesfor
autismand
Pervasive Developmental Disorder.
Many
parents choose avariety
of strategiesto
addresstheir
children'sneeds.In
additionto
Lovaas/
ABA
therapy,
they
may be
utilizing
otherinterventions. The
following
is
adescription
of some ofthe
morepopular
treatment
choices:(A)
Psychopharmacology
(Drug
Treatment).
The
purpose ofusing drugs
to
control autistic
symptomology is
to
better
prepare the childto
respondto
specialABA/
Lovaas
18
Drugs
are usedto
increase
attention,
reduceself-stimulatory
behavior,
and reducetantrums
(Campbell,
Anderson, Deutsch,
&
Green,
1984).
The
drugs
most often prescribedinclude
the
following:
haloperidol,
fenfluramine,
naltrexone,
clomipramine, clonidine,
and various stimulants(Campbell,
Schopler, Cueva,
&
Hallin,
1996).
(B)
TEACCH. Treatment
andEducation
ofAutistic
and relatedCommunication
handicapped
Children. This
is
a program establishedby
Eric
Schopler
of theUniversity
ofNorth Carolina
atChapel Hill
(Campbell,
Schopler,
Cueva,
&
Hallin,
1996).
Schopler is
skeptical ofthe
dramatic
"recovery"claims
made
by
Lovaas
("Requests for
Lovaas,"1995).
The TEACCH
programis
acommunity
based
program,
located
in
public school classrooms.The
maintenants
ofthe
programinclude
high
amounts of parentparticipation,
on-going
evaluationand
diagnostic
work,
and structuredteaching (Schopler,
1987; Campbell,
Schopler,
Cueva,
&
Hallin,
1996).
(C) Auditory
andSensory
Integration Training. These
theories
arebased
onthe
premisethat
some people with autismhave
anover-sensitivity
orunder-sensitivity
to
sounds and/or
textures.
Through
variousinterventions
andactivities,
an attemptis
madeto
"desensitize"the child,
and makethem
better
ableto
handle
different
soundfrequencies
andtextures
(Campbell,
Schopler,
Cueva,
&
Hallin,
1996).
(D)
Greenspan Techniques.
Stanley
Greenspan
views autism as a"multi
systemdevelopmental
disorder,"
in
whichthe
child experiencesdelays
across allareas of
development
("Alternatives
to
behaviorism,"
1995).
He
advocatesfor
atherapy
called"floor
time,"
in
which the parent ortherapist
attemptsto
understandself-stimulatory
behavior)
("Alternatives
to
behaviorism,"1995).
The
childis
thought to
learn
through the
interaction,
andthrough
the
relationship
that
is
developed
during
time
spent withthe
adult("Alternatives
to
behaviorism,"1995).
(E)
Dietary
/Vitamin
Interventions. Of
allthe
areasdiscussed
thus
far,
this
area
is
the
mostcontroversial andlpast
rpsparrhpd,Most
ofthe
information
available on
this treatment is
found
onthe
internet
(Lewis,
1997). The
premisebehind
this treatment
is
that
one ofthe
causes of autismis
anallergy
to
gluten andcaseine.
These
two
substances arefound
in
many foods commonly
introduced
atthe
age of
approximately
18
months.Advocates
ofthis treatment
claimthat
whenfoods
with gluten and caseine are removed
from
the
child'sdiet,
many
oftheir
autisticsymptoms abate
(reduction
in tantrums
andself-stimulation,
improved
eye-contact,
better
attentionskills)
(Lewis,
1997). The
diet
is
often usedin
conjunction withvitamin
therapy.
Two
vitamin supplementscommonly
administeredin
large
amounts
include
B6
anddimethylglycine
(DMG) (Aman,
1995).
Rational
for
Project
onABA
/Lovaas
Treatment
for Children
withAutism
The
changing
definitions
for
autism andPervasive Developmental Disorder
(PDD)
have
resultedin
the
development
ofmany
treatment
options.Parents
ofpreschoolers
diagnosed
with autismface
the
challenging decision
of whatinterventions
to
use withtheir
child.As
indicated
by
the
aboveliterature
review,
O.
Ivar Lovaas has developed
a program whichis
based
on principals ofApplied
Behavior
Analysis,
consists of alarge
amount oftreatment
hours
(40+
perweek),
and
demands
intense
parentalinvolvement.
This
treatment
approachhas
createdmuch
controversy,
for
both
professionalsin
the
field
and schooldistricts.
With
the
increasing
number of childrenbeing
diagnosed
with autism/PDD,
it
ABA/
Lovaas,
20
over
the
course oftheir
career.In
orderto
serve as a consultant and source ofinformation
for
these
families,
professionals needknowledge
ofthe
history
andcurrent structure of
ABA
/Lovaas
programsin
the
Monroe
County
Area.
Due to
the
expense ofthese
intensive
programs,
schooldistricts
andcommunity
groups areraising
questions aboutthe
effectiveness and appropriateness ofthis treatment.
Community
groups and school professionalshave
startedto
collaborate onresearching
these
programs(i.e.,
Community
Task Force
onAutism:
Research
andEvaluation
Cnmmiftpp)
This
project was conductedin
orderto
provide professionalsin
the
field
anoverview of
both
the
composition ofthe
currentABA
/Lovaas
programsbeing
implemented
in
the
Monroe
County
area,
and asummary
ofthe
collective concernsof parents
implementing
such programs.The
literature
reportsthat
ABA/
Lovaas
programs aretime intensive
(40
hours+),
require much parentinvolvement,
and arebest
utilizedwith younger children.I
wantedto
assessif
these
characteristics aretrue
ofMonroe
County
families utilizing
these
programs.Parents
of children withautism
/PDD
weresurveyed,
using
asurvey
form developed
by
the
research student.The
children wereobserved,
and ratedin
terms
ofthe
severity
oftheir
autisticsymptoms
(Childhood
Autism
Rating
Scale).
The information
wasthen compiled,
in
orderto
get adescriptive
account ofthe
ABA/
Lovaas
programsin the
Monroe
County
area.In
addition,
as a school psychologistworking
in
this
community,
I
wantedto
have
abetter
understanding
ofthe
following:
(1)
What
sourcesdo
parents consultwhen
choosing
anABA/
Lovaas
treatment
programfor
their
child?;
(2)
What
professionals areincluded
onABA
/Lovaas
treatment
teams?;
(3)
What
otherdoes
ABA impact
family
life?;
(5)
What
do
parents needfrom
the
professionalcommunity?;
and(6)
What is
the
(approximate)
cost offunding
ABA/
Lovaas
programs?
This
knowledge
willhelp
schoolpsychologists,
and other professionalsABA/ Lovaas,
22
Project
Overview
Community
Contribution
With
the
rising
number of requestsfor
ABA
/Lovaas
treatments
for
autism,
professionals
in Monroe
County
have begun
to
ask questions aboutthe
efficacy
andcost-effectivenessof such programs.
Monroe
County
is
the
secondlargest county
in
upstate
New York. It's
populationis
approximately
750,000
people,
with aland
areaof
663.21
square miles.The
county
is
comprised of19
towns,
10
villages,
andthe
city
of
Rochester.
Rochester,
New York
is
famous for
its
exportindustry
(Eastman
Kodak,
Bausch
andLomb,
General
Motors, Xerox,
ITT Automotive).
On
a per capitabasis,
more products are exportedfrom
Monroe
County
than
any
othercommunity
in
the
United States
(above
information
located
athttp://www.co.monro.ny.us/
aboutmc
/
mchistory
.html).Through
professionalnetworking, in October
of1996 I
learned
of a committeeforming
to
addressthe
issue
ofABA
/Lovaas
servicesin
the
Monroe
County
area.A
group
ofprofessionals,
consisting
ofadministrators,
schoolpsychologists,
andspecial education
coordinators,
werecollaborating
to
gatherdata
and start somepreliminary
research onABA
/Lovaas
programs.The
chairpersonfor
this
committee was affiliated with
New
York's
Board
ofCooperative
Education Services.
In November
of1996 this
group
metto
formulate
their
purpose anddraft
up
asurvey.
They
intended to
look
at whattypes
of programs children whohad
receivedABA/
Lovaas
were placedin
uponentering
the
public school system.The
committeewanted
to
determine if
children who receivedABA
/Lovaas
as preschoolers weretypically
placedin
regular education or mainstreamedprograms,
ordid
they
stillThey
collectedthis
data
via a written survey.Each
committee member committedto
contacting
aMonroe
County
schooldistrict
andeliciting
their
cooperationin
providing
thedesired information.
As
willbe discussed
later,
some ofthe
questionsfrom
this
originalsurvey
were utilizedin
the
course ofthis
project.The
researchmethod and
survey
results were notutilized,
due
to the
fact
that
program placementcan
be
highly
subjective andinfluenced
by
many factors (such
asdistrict
policy
andthe
level
of parent advocacy).While
attending
this
November
24,
1996
meeting
I
learned
of anotherlocal
committee
forming
to
addressthe
issue
ofABA/
Lovaas. This
committee was calledthe
Community
Task Force
onAutism:
Research
andEvaluation
Committee. The
chairperson
for
this committee was affiliated withthe
University
ofRochester
/Strong
Hospital's Center
for
Developmental
Disabilities.
Although
the
make-up
ofthe
committee variedfrom meeting
to meeting, the
primary
memberswere as
follows:
two
parents of children withautism, two
pediatricians connectedto
the
Strong
Center
for
Developmental
Disabilities,
aNYS Board
ofCooperative
Educational
Services
(BOCES)
representative,
aCommittee
ofPreschool Special
Education
chairpersonfrom
aMonroe
County
schooldistrict,
and a schoolpsychologist
from
aMonroe
County
schooldistrict. I
attendedthree
meetings ofthis
committee
(December
20, 1996;
January
27, 1997;
January
31,
1997). The intent
wasto
work with
these
professionalsin
orderto
draft
up
a specific research questionthat
would
be
appropriatefor
a master's project onABA
/Lovaas
treatment
for
autism.This
provedto
be
achallenging
task.
The
long
term
objective ofthis
committee was
to
researchthe
effectiveness ofABA /Lovaas
programs asthey
compare
to
moretraditional
ways oftreating
autism(predominantly
specialABA/
Lovaas
24
limitations
in time
and personalresources, this
was not afeasible
researchtopic.
Through
much negotiation anddiscussion,
the topic
waslimited
and narrowed.It
was
decided
that
I
would conduct a series ofinterviews,
rating
scale observations(Child
Autism
Rating
Scale),
and recordreviews,
in
an attemptto
generate a generalidea
ofhow
much progress each childhas
made whilereceiving
Lovaas
therapy.
The
design
ofthe
final
project willbe discussed
at alater
point.In
orderto
gainthe
support ofMonroe
County
parents,
I
attended severalReaching
Autistic Children
Early
(RACE)
support groups.The
purpose ofthis
organization
is
to
promoteABA
/Lovaas
as a viabletreatment
optionfor
childrenwith autism.
They
provide support andinformation
to
families
implementing
ABA
programs.
The
long-term
goal ofRACE is
to
establish anApplied Behavior Analysis
school
for
children with autism.This
organization provided an excellent pool offamilies for
the
researchthat
wasto
be
conducted.On
February
1,
1997 1
presentedmy
projectdesign
to
the
parents present atthe
meeting.On
May
3,
1997
I
contactedthe
RACE
presidentfor
assistancein
promoting
my
project.The
president signed aletter
ofsupport,
andhad
parentssign-up
if
they
wereinterested in
participating
in
the
project(see
Appendix
A).
On
October
11,
1997
1
attended athird
RACE
meeting.At
this
meeting
I
scheduledfamilies
to
be
interviewed
and observed.Throughout
the
course ofthe
project,
close contact was maintained withthe
RACE
group
president and various members.
Project Design
andReview
ofObjectives
The
design
ofthis
project changed overthe
course ofits
completion.The
original
design,
mentionedabove,
was a series ofinterviews,
observations(CARS),
and recordreviews.
The
goal wasto
comparethe
length
oftime
the
child receivedmeasured
by
adifference
score,
obtainedby
comparing
the
child's score onthe
Childhood Autism
Rating
Scale
(CARS)
priorto
receiving
ABA
andto
the
child'sscore on the
CARS
afterbeing
in
anABA
program.Again,
due
to
limitations
oftime
andpersonal
resources, the
projectwas altered.During
the
period oftime
from
October,
1997
to
December, 1997,
interviews
and observations offamilies using
the
ABA
program were conducted.The information
gathered was usedto
develop
adescriptive
picture ofMonroe
County
ABA
programs.The
rating
scales were usedto
examine the
level,
orseverity,
ofthe
disability
demonstrated
by
this
particulargroup
of children with autism.
As
wasdiscussed
earlier, the
purpose ofthis
project wasto
give professionals and parents a "cross-section" or
description
ofthe
ABA
servicesbeing
delivered
to
children with autism/PDD
in
the
Monroe
County
Area.
The
Childhood
Autism
Rating
Scale
was administeredto
supplementthis
description,
and
to
provide some more specificinformation
aboutthis
sample of childrenreceiving
ABA
therapy.
The
originalintent
ofthe
project wasto
stay
withinthe
age range of3
to
5
years old.
After
consultation withprofessionals andparents,
it
wasdecided
that
amore appropriate age range was
birth
to
5
years old.Members
ofthe
Monroe
County
Committee,
The
Community
Task
Force
onAutism: Research
andEvaluation
Committee,
andthe
RACE
group
estimatedthat there
wereapproximately
50
children with
autism/
PDD
classifications withinMonroe County. It
wasthen
estimated
that
out ofthose
50
families,
approximately
30
ofthem
wereimplementing
ABA
programs.These
numbers were rough estimates.Due
to
thefact
that
there
are no centralizedrecordskept
onlocal
incident
rates of autism/PDD,
oron
the
enrollment of such childrenin
treatment programs,
estimations neededto
be
ABA/
Lovaas,
26
At
the
RACE
meetings(May
andOctober),
14
families
signedup
to
be
partofthe
project.Another 21
families
were contactedby
phone(personal
conversation orphone message).
For
various reasons(i.e.,
child wastoo
oldfor
the
study,
child wasno
longer
doing
ABA,
child wasmultiply
disabled,
parent never returnedthe
phonecall,
parentstoo
busy,
etc.),
only
11
families
wereinterviewed
and observed.Out
ofthese
11
families,
10
were usedto
calculatethe
descriptive
account ofABA
treatment
in
the
Monroe
County
area.One
childinterviewed
and observedby
the
researchstudent was out of
the
birth
to
5
age range.Interviews
and observationstypically
took
approximately
onehour
andfifteen
minutes.After
the parent(s)
completedthe
survey, the
research studentinterviewed
them
in
orderto
gather additionalinformation
to
accurately
scorethe
Childhood
Autism
Rating
Scale
(CARS).
The interview
wasdesigned
to
be filled
outby
the
parent whilethe
Childhood Autism
Rating
Scale
(CARS)
observation wasbeing
conductedby
the
research student.
The
average completiontime
ofthe
survey
was ahalf-an-hour
to
forty-five
minutes.The
questionnaire consisted oftwenty-four
questions,
withresponses
being
recordedin
narrativeform
andin
check-listform
(see
Appendix
B).
During
the
development
ofthe survey,
feedback
was collectedfrom
the
two
parentson
the
Community
Task
Force
onAutism: Research
andEvaluation
Committee.
As
previously
mentioned,
questions wereborrowed from
the
Monroe
County
survey
on program placement
for
preschoolers who receivedABA
treatment.
Care
wastaken
to
makethe
survey'slanguage
andformat
accessibleto the
parent.Questions
included the
following:
demographic information
onthe child,
number of monthsin
anABA
program,
number ofhours
ofABA
servicedelivered
weekly,
othertreatment
approachesbeing
utilized,
andthe
parentsimpression
ofdifferent facets
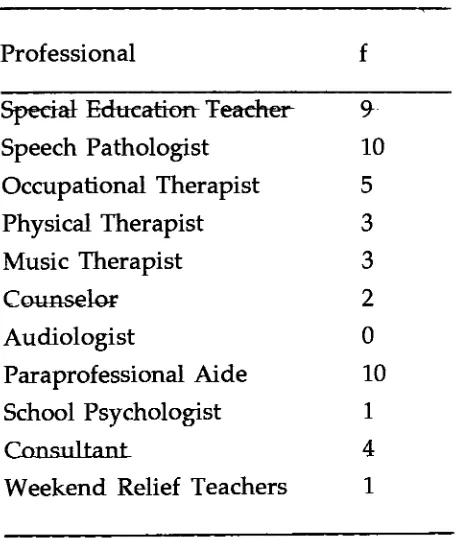
The Child Autism
Rating
Scale
(CARS)
was chosen as a measure ofthe
children's autistic symptoms.
The
scale consists of15
subscales:"relating
to
people;
imitation;
emotionalresponse;
body
use;
objectuse;
adaptationto
change;
visualresponse;
listening
response;
taste,
smell,
andtouch
response anduse;
fear
ornervousness;
verbalcommunication;
non-verbalcommunication;
activity
level;
level
andconsistency
ofintellectual
response;
and general impressions"(Van
Bourgondien,
1992;
Schopler,
1995). The
scale wasdeveloped
to
assistin
evaluating
children-referred
to the
Treatment
andEducation
ofAutistic
and relatedCommunication
handicapped
Children
(Division
TEACCH; Schopler,
1995).
The
CARS is
a compilation of several accepteddefinitions
anddescriptions
of autism.Schopler
drew
from
the
following
existing
criteria:"Kanner
(1943)
criteria,
the
Creak
(1961)
points, the
definition
ofRutter
(1978),
that
ofthe
National
Society
for
Autistic
Children
(NSAC,
1978),
andthe
DSM-IV
(1994)"(Schopler,
1995).
The
scale wasoriginally
createdin
1973,
andthen
revisedin 1988
(Schopler,
1995). The
manualused
for
this
projectwas reprintedin 1995.
The
norm samplefor
the
Childhood
Autism
Rating
Scale
(CARS)
was1,606
children,
reflecting
the
economic and racialmake-up
ofthe
North Carolina
population
that
TEACCH
services(Schopler,
1995).
As
reportedin
the manual,
theCARS has
adequatelevels
ofinternal
consistency
(.94),
interrater
reliability
(.71),
test-retest
reliability
(.88),
and criterion-relatedvalidity
(.80) (Schopler,
1995).
The
scale was
intended to
be
used as part of afull
evaluationfor
the
TEACCH
program.The
scale was scored after a cliniciandirectly
observed a child withinthe
laboratory
setting
(Schopler,
1995).
In
orderto
determine
if
the
scale was valid and reliableunder other circumstances,
further
studies were conducted.It
wasfound
that ratingsABA/
Lovaas,
28
and after record review
(r=.82),
adequately
correlated with ratingsdone
atTEACCH
Centers
(Schopler,
1995). For
thisproject, the
scale was scored afterdoing
adirect
observation of
the
childin
the
home
andinterviewing
the
parent.The CARS
was notthe
only
instrument
availableto
ratethe
severity
ofautistic symptoms.
Other
measures usedfor
this
purposeinclude
the
Autism
Behavior Checklist
(ABC)
andthe
Real Life
Rating
Scale
(RLRS).
A
pilotstudy done
by
Sevin
et al.(1991)
analyzedthese three scales, in terms
ofinterrater
reliability,
correlations
between
the
instruments,
accuracy
of cut-off scoresfor
classification,
and
the
relationship
ofthese
scalesto
adaptivebehavior
measures.Sevin
et al.(1991)
reportedthat
the
interrater
reliability
they
achievedfor
the
CARS
wasslightly
less
than
originally
reportedby
Schopler
(1995).
The
CARS
alsodid
not correlatewell with
the
adaptivebehavior
measure(Vineland).
The
authors attributedthese
discrepancies
to
a small sample size and adifference
in
behaviors
assessedby
the
Vineland
andthe
CARS. As
for
correlationsbetween
the, scales, the.
CARS
correlatedwith
the
RLRS,
but
notthe
ABC. The
cut-off scorefor
the
CARS
appearsto
be
appropriate,
asindicated
by
the
fact
that
92%
ofthe
subjects werecorrectly
identified.
The
authors conclude thatthe
CARS
andthe
RLRS
are adequatescreening
measurefor
identifying
children with pervasivedevelopmental
disorders
(Sevin,
1991). The
ABC fared less
well,
and wasconsideredless
"technically
sound"
than
the otherscales
(Sevin,
1991).
This CARS
was chosenfor
this
projectbecause,
when comparedto
otherinstruments,
it
is time
efficient andtechnically
superiorto
other autismDiscussion/Results
Section
Sample
Demographics
The
original goal of this project wasto
interview
and observe30 families.
Due
to
personallimitations
and parentavailability, the
final
sample size was10. This
sample size
is inadequate
to
make generalizations aboutthe
entireMonroe
County
area population of childrenwith autism.
Observations
willbe limited
to
this
uniquesample of
families
and children withautism/
PDD.
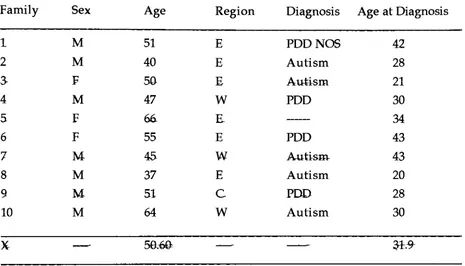
As
shownin Table
1, 30%
ofthis
sample was
female,
and70%
was male.Pervasive Developmental Disorders
mostfrequently
occurin
males(75%),
asis
reflectedin
this
particular sample(Schopler,
1995). Another
factor
I
attemptedto
look
at was wherein
Monroe
County
these
services are
being
delivered
withthe
mostfrequency.
Sixty
percent ofthe
families
live in
the
eastern part ofthe county,
30%
ofthe
families live
in
the
western part ofthe
county,
and10%
ofthe
families live
in
the
city
ofRochester.
The
average age ofdiagnosis
for
this
sample was31.9
months(with
a range of22
months;
youngest =21
months and oldest =43
months).The
average ageis in
accordancewith
the
DSM-IV
criteriafor
diagnosing
autism/PDD
before
the
age of3
years
(DSM-IV).
Two
childrenin
the
sample werediagnosed
afterthat
cut off point.As
for
the
specificdiagnoses
assignedto these
children,
they
included Pervasive
Developmental Disorder Not Otherwise
Specified,
(PDD
NOS),
Pervasive
Developmental Disorder
(PDD),
andAutism.
This
mostlikely
reflectsthe
"autism
spectrum,"
and
broadening
ofthe
definition
for
autism(Rimland,
1993; Bauer,
1995a
& 1995b).
The different
classifications reflectthe
heterogeneous
nature ofthis
population and
the
overalldifficulty
withdiagnosis.
Lovaas
(1973)