Q U A L I T A T I V E
Conceptualization of physical exercise and keeping fit by child
wheelchair users and their parents
Jane Noyes, Llinos Haf Spencer, Nathan Bray, Hans-Peter Kubis, Richard P. Hastings, Matthew Jackson
& Thomas D. O’Brien
Accepted for publication 28 October 2016
Correspondence to J. Noyes: e-mail: [email protected]
Jane Noyes MSc DPhil RN
Professor of Health and Social Services Research and Child Health
School of Social Sciences, Bangor University, UK
@jane_noyes
Llinos Haf Spencer PhD Research Officer
School of Healthcare Sciences, Bangor University, UK
Nathan Bray MSc PhD Research Officer
Centre for Health Economics and Medicines Evaluation, Bangor University, UK
Hans-Peter Kubis PhD Senior Lecturer
School of Sports and Exercise Science, Bangor University, UK
Richard P. Hastings BSc PhD CPsychol Chair of Family Research
Centre for Educational Development, Appraisal Research, Warwick University, Coventry, UK
Matthew Jackson
Department of Health Sciences, Liverpool Hope University, UK
Thomas D. O’Brien
School of Sport and Exercise Science, Liverpool John Moores University, UK
N O Y E S J . , S P E N C E R L . H . , B R A Y N . , K U B I S H . - P . , H A S T I N G S R . P . , J A C K S O N
M . & O ’ B R I E N T . D . ( 2 0 1 7 ) Conceptualization of physical exercise and keeping fit by child wheelchair users and their parents. Journal of Advanced Nursing 73(5), 1111–1123.doi:10.1111/jan.13209
Abstract
Aim. To gain a better understanding of how children aged 6–18 years who use wheelchairs and their families conceptualized physical exercise and keeping fit. Background. Disabled children with reduced mobility are commonly overweight and unfit. Nurse-led health screening programmes in schools commonly exclude disabled children if they cannot use standard weighing scales or stand against height measuring sticks.
Design. Qualitative interview study at two time points over 6 months with children who use wheelchairs and their families.
Methods. Framework analysis using the theory of planned behaviour.
Findings. Mainly physically active participants were recruited (24 children and 23 parents) 2013–2014. Despite engaging in high levels of physical exercise, children were assessed as fit but had elevated body fat and did not realize how fit they were or that they were slightly overweight and nor did their parents. Children enjoyed the social benefits of exercise. Unlike their parents, children confused the purpose and outcomes of physical exercise with therapy (e.g. physiotherapy) and incorrectly understood the effects of physical exercise on body function and strength, preventing stiffness, increasing stamina and reducing fatigue. A new model was developed to show children’s misconceptions.
Conclusions. Proactive parents can overcome barriers to enable their children to benefit from physical exercise. Professionals need to increase communication clarity to improve children’s understanding of therapy compared with physical exercise outcomes. Inclusion of children who use wheelchairs in health education policy; routine health screening; physical education classes and teacher training requires improvement. Body composition measurement is recommended, for which nurses will need training.
Keywords: conceptualization, disabled children, health promotion, nursing, physi-cal exercise therapy, public health, qualitative, school health screening, wheelchair
©2016 The Authors.Journal of Advanced NursingPublished by John Wiley & Sons Ltd 1111
Introduction
There is concern about increasing obesity among children in high-income countries (Department of Health 2011, WHO 2015). Children who use wheelchairs are at higher
risk of being unfit, overweight or obese (Public Health Eng-land 2014). In EngEng-land, 45% of children age 8–13 years with a life-limiting illness and learning disability were obese or overweight in 2011 compared with 22% of children who had neither condition (ChiMat 2011). Being over-weight has a severe impact on health and well-being in childhood and adulthood by exacerbating underlying condi-tions and increasing the risk of type 2 diabetes, heart and liver disease and some cancers (PHE 2014).
Despite the greater prevalence of obesity and overweight in disabled children, policy has primarily focussed on typically developing children. Neither the United Kingdom, guidance on exercise for children (National Institute for Health and Clinical Excellence (NICE) 2009) or the American Academy of Pediatrics Committee Statement on Nutrition (AAP 2003) mentioned disabled children. A balanced healthy diet tailored to each disabled child and regular physical exercise to keep-fit has been shown to be safe with the same benekeep-fits as for typically developing children (O’Brienet al.2014, 2016).
An effective keep-fit physical exercise involves the child feeling hot and sweaty with an increased heart and respira-tory rate (thereby indicating an increased metabolic rate) that subsequently returns to normal. Keep-fit exercise also induces a pleasant feeling of well-being. In contrast, thera-pies such as physiotherapy are designed to maintain, regain or improve strength, mobility or function of a specific ele-ment of the musculoskeletal system and children rarely experience pleasant feelings or social benefits (Scianniet al. 2009). Having regular therapy facilitated by a therapist does not replace the need for frequent physical exercise as they serve different purposes.
Background
The linked study protocols outline in greater depth that nurses have a vital health promotion, motivational and monitoring role in optimizing the health and well-being of disabled children (O’Brien et al. 2014, 2015). In England, children are weighed and measured by nurses as part of the National Child Measurement Programme at age 4–5 years and 6–10 years. Guidance recommends exclusion of chil-dren who are ‘not able to stand unaided on the scales or under the height measure’ (DoH 2010, p. 9). The trigger for intervention (such as a letter to the parents or exercise referral) is the outcome of the child’s weight and height measurements. Parents and children also need to recognize that the child is overweight and unfit and to acknowledge that this situation is unhealthy.
Little research has been conducted to understand why disabled children have lower participation in physical Why is the research needed?
Children’s health policy on exercise and healthy eating and national school weight screening programmes frequently exclude disabled children and they are often not screened if they cannot use standard weighing scales and height sticks.
Disabled children and particularly those with reduced mobility who use wheelchairs are at high risk of being unfit, overweight or obese.
It is not known how children who use wheelchairs and their parents conceptualize physical exercise, keeping fit or obesity.
What are the key findings?
Children who use wheelchairs were assessed as fit but had elevated body fat and did not realize how fit they were or that they were slightly overweight and nor did their par-ents.
Children who use wheelchairs confused the different pur-poses and outcomes of therapy (such as physiotherapy) compared with physical exercise, whereas parents were clear about the differences.
The study attracted self-selecting wheelchair using child participants who generally engaged in high levels of physi-cal exercise, which is useful feasibility information for the future design of interventions and research.
How should the findings be used to influence policy/ practice/research/education?
Findings show that child participants who used wheel-chairs were commonly excluded from nurse-led school screening programmes as the measuring equipment was commonly not accessible and an alternative accessible method was not available. This requires addressing urgently to comply with Equality Legislation.
Professionals in the multi-disciplinary team and especially nurses, need to clarify the language shared with children who use wheelchairs to ensure that they are clear about the difference between the purpose and outcomes of therapy (such as physiotherapy) compared with physical exercise.
exercise and are generally less fit (Scott 2010). Although there is increasing understanding of how typically develop-ing children and their parents conceptualize fitness and obe-sity (Thomas et al. 2014), there is no clear understanding of how children who use wheelchairs conceptualize these issues. The purpose of this paper is to report the first find-ings on how children who use wheelchairs and their parents conceptualize exercise and keeping fit.
Theoretical framework
The Theory of Planned Behaviour (Ajzen 1991) was used to conceptually link attitudes towards behaviours, subjective norms and perceived behavioural control as shaping an individual’s behavioural intentions and actual behaviours. (See Data S1 in Online file 1).
The study
Aim
To gain a better understanding of how children aged 6– 18 years who use wheelchairs and their families, conceptu-alize physical exercise and keeping fit and the impact of physical exercise on children’s bodies.
Research question
How do children (and their parents), conceptualize physical exercise and keeping fit and the impact of physical exercise on children’s bodies?
Design
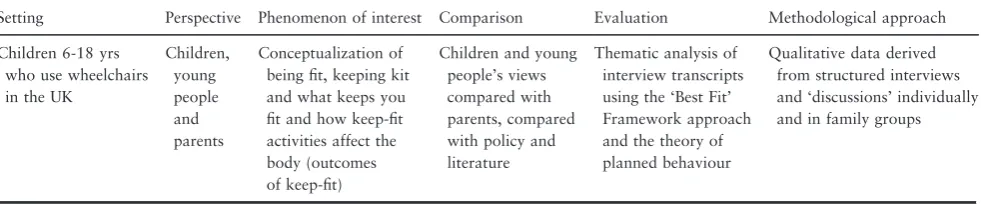
The SPICE framework (Setting, Perspective, Phenomenon of Interest, Comparison, Evaluation; Booth 2006) was used to determine the study focus (Table 1). This generic qualitative study informed by Framework analysis (Spencer et al. 2003, Carroll et al. 2011) was a component of a larger mixed-method study exploring and measuring well-being, health and fitness in children who use wheelchairs (O’Brien et al.2014).
Participants
Twenty-four children and 23 family members took part in one-to-one interviews at time point 1 in study stage 1 and 16 of these children and 15 parents took part in subsequent family-based discussions at time point 2 around 6 months later in study stage 3 (Figure 1).
(See Tables 2 and 3) for sample characteristics for each time point. Letters of invitation were sent via wheelchair
services, not-for-profit organizations and snowball sam-pling. A purposive sampling frame (Table 4) was designed to capture maximum variation of conditions and equal number of children per age group (6–10, 11–15, 16– 18 years).
Data collection
Data were collected on two occasions between October 2013 - September 2014. Structured interviews were con-ducted face-to-face or by telephone with children and their parents to elicit experiences and opinions and to explore their understanding of ‘keeping fit’. Parent and child inter-views were conducted separately, apart from when parental assistance was required to enable participation. Interviews were audio recorded and transcribed verbatim. Around 6 months later, ‘structured discussions’ were conducted at a ‘family day’ at a child-centred meeting venue in a country park. We termed these structured ‘discussions’ and not ‘in-terviews’ as the purpose was to elicit feedback and check out our understanding of findings from previous episodes of data collection and to further explore specific issues of interest for further clarification. Key information from dis-cussions was recorded on pro-forma sheets in real time.
Ethical considerations
See the study protocol for full details about child safeguard-ing, consent procedures and data protection (O’Brien et al. 2014). In brief, written informed consent and proxy con-sent for children (6–15 years) to participate was obtained from parents; and assent to participate was established with children and recorded on an assent form. Children over 16 years with mental capacity provided written informed consent. Research Ethics committee approval was obtained on 23 August 2013.
Data analysis
and developed maps and charts to display analytical findings.
Validity and rigour
None of the researchers had any prior relationship with the children and their families and disengaged at the end of the study. Rigour was enhanced by prolonged engagement with participants with opportunities to check meaning of initial analyses. The multi-disciplinary team included nursing, physiology, psychology and sports science expertise, which enabled interpretation through different discipline-specific lenses. An advisory group including a young adult chair user, exercise/sports facilitators, therapists and wheel-chair services representatives supported and advised the research team and provided feedback on findings.
Findings
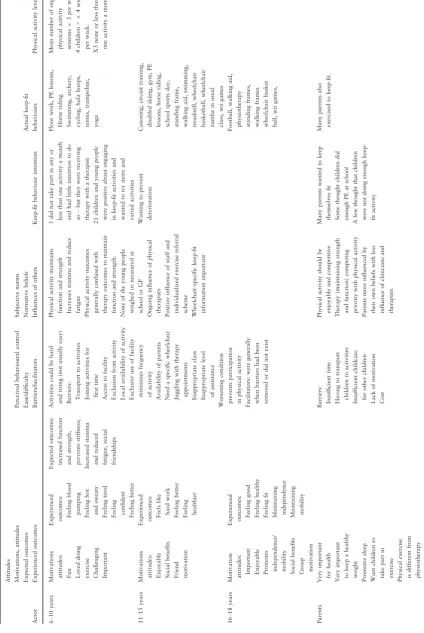
Mapping findings against the theory of planned behaviour Descriptive level findings are mapped against the theory of planned behaviour in Table 5.
Behavioural intention and actual behaviour
Twenty-one of 24 children reported that they regularly par-ticipated in a wide range of sports and physical exercise. The mean number of organized physical exercise sessions per week was three, with four children reporting at least four physical exercise sessions a week. Only three children reported none or less than one physical exercise session a month. Of the three children that did not regularly partici-pate in physical exercise, their parents were all keen for them to engage in more keep-fit activities. Overall, the very high physical exercise and fitness levels that we measu-red were not typical of the general population of wheelchair using children. We will return to this issue in the discussion.
Attitudes
Enjoyment and loving the activity was a key motivator. A girl aged 9 years (W22) said: ‘Now, we’ve got a topic in PE (physical education class at school), which is tennis–and I . . .absolutely love doing that’. A girl, aged 12 (W13)
Table 1 Spice Framework.
Setting Perspective Phenomenon of interest Comparison Evaluation Methodological approach
Children 6-18 yrs who use wheelchairs in the UK
Children, young people and parents
Conceptualization of being fit, keeping kit and what keeps you fit and how keep-fit activities affect the body (outcomes of keep-fit)
Children and young people’s views compared with parents, compared with policy and literature
Thematic analysis of interview transcripts using the ‘Best Fit’ Framework approach and the theory of planned behaviour
Qualitative data derived from structured interviews and ‘discussions’ individually and in family groups
Well mi study
N = 22 children and young people
N = 24 children and young people
N = 16 children and young people
N = 22 parents N = 1 grandmother
N = 21 parents
N = 15 parents Stage 1
Stage 2
Stage 3
described her experiences of using the Wii fit: Girl: ‘Because like, one it’s really fun and like, two it makes me feel better to know that I’m doing something’.
Older children were particularly motivated by the indi-vidualization of some schemes and the social aspects of par-ticipation. For example, A young man aged 18 (W17) said: ‘There are quite a few people my age and then there are various adults of various ages as well. . .. it’s mostly men. . .there are only two or three women or girls that go. . .’. Researcher ‘But it’s the social thing that keeps you going?’. Young man: ‘That’s the primary motivator’.
Similarly, a young woman aged 18 talked about the bene-fits of exercising with friends: ‘Making friends with people and keeping fit with each other because sometimes, it’s nice to have a friend, if you’re doing exercises with them, to look at them and see what they achieved and you kind of like achieve something together’. And a boy aged 14 (W06) said:’. . .because we all like train once a week and you get to build up some really good strong bonds, so it’s really good’.
Parents all said that physical exercise to keep-fit was very important along with enjoyment. For example, a mother of a girl, aged 9 (W24) said that she would like her daughter to take part in exercise for the joy of doing it: ‘I want her to do it for the love of doing it. . ... Not for competition or matches. . .’. Likewise parents of severely disabled children were motivated to enable their children to experience physi-cal exercise: A mother of a girl aged 8 (W24) said: ‘(daugh-ter) is very limited in what she can do, but she goes to a private swimming lesson every week’.
Expected outcomes
In addition to social contacts and friendships, children of all ages generally expected increased function and strength, prevention of stiffness and increased stamina and reduced fatigue from physical exercise.
Experienced outcomes of keep-fit activities
Children age 6–10 experienced increased tiredness and con-fidence. A 9-year-old girl (W22) said: ‘I get worn out’ (do-ing exercise). Later she went on to explain that exercise had also given her the confidence to do other things.
Children age 11–15 commonly experienced increased effort and hard work associated with exercise and felt bet-ter and healthier afbet-terwards. Although a boy aged 14 (W10) did not define what he meant by ‘keeping healthy’ he said: ‘I would just do it [physical exercise] to keep healthy, because the alternative to that is just sitting at home, doing nothing’.
The older 16–18 group experienced increasing confi-dence, stamina and reducing aches, fatigue and stiffness and some said they maintained their independence. Some young people who did not have degenerative conditions also increased their mobility. For example, A young woman
Table 2 Child demographic characteristics (n=24) at time point 1.
Gender 12 (50%) Male
12 (50%) Female
Aged 6–10 8
Aged 11–15 8
Aged 16–18 8
Condition
Achondroplasia/Pseudoachondroplasia 2
Cerebral palsy 14
Down’s syndrome 2
Encephalitis 1
Osteoporosis 1
Pallister–Killian syndrome 1
Spina bifida 2
Other unknown cause of mobility impairment 1 Education
In special education 11
Not in special education 13
Ethnicity
White British 20
Other white background 1
Mixed race 1
Black African background 1
Mixed Asian background 1
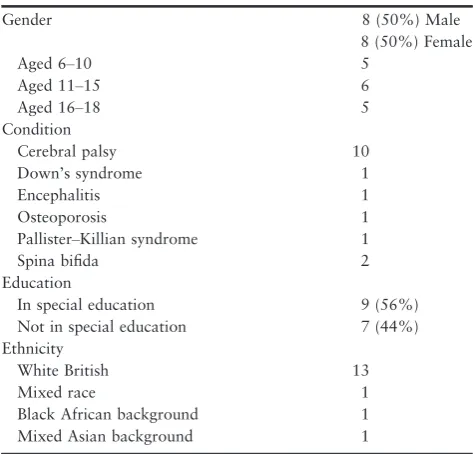
Table 3 Child demographic characteristics (n=16) at time point 2 (phase 3).
Gender 8 (50%) Male
8 (50%) Female
Aged 6–10 5
Aged 11–15 6
Aged 16–18 5
Condition
Cerebral palsy 10
Down’s syndrome 1
Encephalitis 1
Osteoporosis 1
Pallister–Killian syndrome 1
Spina bifida 2
Education
In special education 9 (56%)
Not in special education 7 (44%)
Ethnicity
White British 13
Mixed race 1
Black African background 1
aged 18 years (W23) said she swam because: ‘The reason is. . . to keep myself mobile and stop me, because of my cerebral palsy, to stop my legs getting stiff because if they were stiff I wouldn’t be able to do anything and I would class myself as an independent person because I do like loads of arm stretches, to help with my personal care and things’. This quote also illustrates how therapy-type activi-ties were prioritised to achieve daily functioning outcomes such as reduced stiffness.
Similarly, a young man aged 18 years (W17) said that he did physical exercise to avoid fatigue: ‘Well, it’s important for me to keep-fit because of my.. general life. Because, I have quite bad fatigue issues, I have to kind of keep my sta-mina up. Or else I get very, very tired, very, very quickly. So keeping fit does a lot in terms of making my life easier to live. . . I notice if I stop maintaining my fitness for a few weeks, pushing (self-propelling the wheelchair) becomes more difficult and I become more tired and things like that, so. . .. to start with, the reducing fatigue and the increase in
stamina were kind of happy side effects because I was going and I still go to basketball for the social aspect of it. It’s just now become the–because I’ve noticed the increase in stamina and that kind of thing that is an additional motiva-tor, but I don’t think that it would ever be the primary motivator’. This young man recognized how the improved fitness resulting from physical exercise improved his energy and stamina and experienced those benefits as combatting his condition, which is logical because it is the present that has an impact on his daily life and not the risk of later sec-ondary diseases, such as cardiovascular disease or diabetes.
Perceived behaviour control
Children were commonly placed in inappropriate classes or received an inappropriate level of assistance at school physi-cal education (PE) lessons. Participation in school-time PE lessons varied significantly between children, especially those in main-stream schools who participated less than children in Special schools. Many children were
Table 4 Child participant inclusion and exclusion criteria.
Inclusion criteria Exclusion criteria
Children aged between 6 and 18 years with a mobility impairment and issued with a wheelchair, were eligible to participate along with family members. Children who were not wheelchair users; had significant challenging behaviours who may have posed a potential risk to themselves, others or the researcher during aspects of data collection such asphysiological monitoring and testing of equipment; or had significant mental health issues, or their disability may hinder participation (such as not being able to communicate).
Attitudes
Motivators to undertake keep-fit activities Attitude towards exercise and keep-fit Expected outcomes of keep-fit activities Experienced outcomes of keep-fit activities
Subjective norms
Normative beliefs about exercise and keep-fit Influence of others on keep-fit participation
Perceived behavioural control
Perceived ease/difficulty of keep-fit activities Barriers to keep-fit participation
Facilitators to keep-fit participation
Keep-fit behaviour
intention
Actual keep-fit behaviours
discriminated against by being excluded from PE lessons at mainstream school. Children reported many different exam-ples of alternative activities, such as: Researcher: ‘What do you do when the children in your class go to PE lessons?’. . . ‘Well, I have to judge their skills’. Girl aged 12 (W13). In contrast, Special schools appeared to provide more oppor-tunities: For example, the mother of a boy aged 9 (W16) explained about the bike club that her son attended: ‘It’s a school based one and he’s just got a specially adapted trike from a charity for himself’.
Some older children intended to maintain a stable physi-cal condition but created perceived barriers. For example, a boy aged 14 (W10) had an attitude that it was going to be difficult to sustain a sufficient level of physical exercise to prevent his condition deteriorating: ‘but trouble is I don’t think I get enough exercise, I want to do more exercise, but then when it comes to it I’m thinking, well, I’m thinking it’s going to be a lot of work, but, I do want to keep-fit, because obviously if I don’t keep-fit,. . . my condition is going to get a lot worse’. He was unclear as to what could help him to overcome this attitude and he was not probed about what could help him overcome his own behavioural control (such as making the exercise fun rather than a lot of work). Nonetheless, he shows that he contextualises keeping fit as important for his medical condition.
Along with cost, accessibility, locality and lack of child-care, barriers to participation commonly included lack of parental time. A mother of a girl aged 8 (W30) explained: ‘I honestly cannot see that I’ll get a chance [to take her to an activity]. . .. And and to be honest I haven’t got the energy. . ... Because I work and then I’ve got (name of girl) so. . .. it’s really difficult with a disabled child’.
Grandparents frequently stepped in to provide additional support: ‘Grandparents, they help me a lot’ (Boy aged 14 W10), whose grandparents took him swimming on a weekly basis and looked after him when his parents were at work. Despite the time constraints expressed by many par-ents, some were very resourceful and facilitative at home. For example, a mother of 8-year-old girl (W24) said: ‘We do a bit of yoga every morning’.
Due to limited time and having to attend several health-related appointments, some parents were forced to priori-tise attendance at therapy sessions (maintaining function) over keeping fit activities (staying healthy). For example, one father said that his son (aged 14) now attended two sessions of private physiotherapy per week on a Saturday. Father (W10): ‘He used to go to (name of a club) which was for disabled kids and he’d go–and I think he did horse riding on that and he did the trampoline and basketball and stuff like that–he did everything. But that is on a
Saturday morning, which is when he has physio now, so we had to stop just for a few years’. Similarly, some chil-dren had physiotherapy instead of attending PE lessons at school.
Children also frequently needed additional sport-specific wheelchairs that were not available through the local wheel-chair service and parents were not always aware when they were available in local sports groups/providers. The father of a girl aged 11 (W02), for example, said that his daughter had shown an interest in wheelchair racing, but she did not have a suitable wheelchair and he was not aware that many clubs provided wheelchairs: ‘I took part in the (Name of city) Great Run, a couple of years ago and she’s seen the wheelchairs going–they go off first and she wanted to fol-low-them–she tried to go through the barrier to follow them around. And it’s like, well I would take her down there (to the local athletics track), but if I take her down there I need to sort out a wheelchair, because that chair isn’t suitable to go around the track’. . .’But even saying that, I priced up a proper racing wheelchair, like they have in the Paralympics and I priced up one of them. . .which isn’t too, too bad a price. Just getting the money to pay for it’. . ...’The NHS would only supply one chair’.
Subjective norms and conceptualizations of physical exercise and keep-fit compared with therapy
None of the children or their parents could remember the last time that the children were weighed or had their height measured in any context. Until we told them the results of their child’s physiology tests, they had no clear idea as to their child’s height, weight, body mass index or fitness sta-tus, other than how their children looked or felt when han-dled. In contrast, they recognized that the physiotherapist, who many regularly attended, measured their therapy out-comes to assess progress and re-set therapy goals.
Child and young people’s perspectives
also commonly stated that they wanted to maintain func-tional mobility to achieve future goals through exercising.
Children commonly talked about their physiotherapy exercises as physical exercises and other sports related activities in the same sentence. For example, a 9-year-old girl (W22) said: ‘Because I like staying healthy and with the clubs it helps me exercise and also I do physio(therapy) at school sometimes’.
Further illustrations of this narrow conceptualization of outcomes of physical exercise and their overlap and depen-dence on therapy outcomes include a boy aged 11 (W11) who said that exercise was very important to him to improve strength and function: ‘. . ..because exercise is really, really important to me, because, I need, I need it to strengthen my bones and just to get better at walking and actually moving about’. A young woman aged 18 (W23) said that participating in exercise stopped her from becom-ing stiff: ‘Keep-fit means, sort of like, when you’ve got someone in a wheelchair, if you don’t do, like, keep-fit, you end up getting stiff, so, it’s important to me’.
Unless prompted, children did not usually make the immediate association between physical exercise and health benefits such as a healthy heart, lungs and healthy weight. Following direct prompting a girl, aged 6 (W09) answered as follows: Researcher: ‘What do you do to keep healthy?’ Girl: ‘I eat apples, grapes, oranges, not bananas but raisins’. Researcher ‘Do you do exercise to keep healthy as well? Do you move your body around?’. Girl: ‘Yes, for my cerebral palsy, I do’. In doing so, the researcher re-orientated her to think about the association between moving her body around and keeping healthy, but her answer was still orien-tated to her medical treatment and therapy.
When asked to talk with further prompting about the specific effect of named physical exercises that they partici-pated in on their bodies, children could mostly make the association between physical exercise and the physiological response. Most children made the link to feeling good (a key motivator for exercising) and the sensations associated with exercise such as feeling hot and sweaty and experienc-ing an increased heart rate. With promptexperienc-ing, most children recognized that these sensations contributed to them feeling good after exercise. For example, a girl aged 9 (W22) said that exercise was good to get the heart pumping: ‘It just makes it pump more blood out and you need blood in your body because that’s really important’.
There was some evidence of disconfirming cases when children responded unprompted by the researcher. A few children seemed to begin to superficially differentiate between therapy and physical exercise but without explain-ing the different expected outcomes.
Individual influences
Specific individual influences included a young man aged 18 (W17) who said that exercise referral staff were influ-ential: ‘I thought I would join the gym so I thought I could have a more kind of personalized programme, obvi-ously because the people that normally work in the gym, aren’t used to working with people with my kind of impairments, whereas the people who run the exercise referral scheme are’.
Parent perspectives
In contrast, most parents could distinguish the differences between keep-fit and therapy. The grandmother of a 6 year old girl (W09) explained: ‘when she does these [therapy] exercises at home. . .it’s not for keeping generally fit–it’s for specific things–specific ways of moving and keeping balance in the core and strengthening in her core and all this. She doesn’t really like having to do these things [therapy] every day, but they are very necessary and you’ve got to do some-thing when you are older, I mean I would like her to do something which involves a bit of competitiveness which is enjoyable and specific to keeping fit, rather than keeping able, you know, but they are two different things but they are linked aren’t they?’.
There were some disconfirming cases such as a parent with an 8 year old child (W30) who had severely limited mobility who appeared to conceptualize physiotherapy as keep-fit exercise when asked about keeping fit: ‘. . .she’s regularly in a standing frame. She goes to hydrotherapy every other term, once a week’. Likewise, the father of W11 (11-year-old boy) said that his son took part in physical exercise to re-build all the strength and balance after a major operation:’. . ..he had the (named) surgery and then, it’s basically well he was ten, a ten year olds body on a new born baby’s legs because all his spasticity had gone so we’re just trying to re-build all the strength and balance and what not’.
Parental influences
Wheelchair services were not noted as a means of access-ing advice about keepaccess-ing fit.
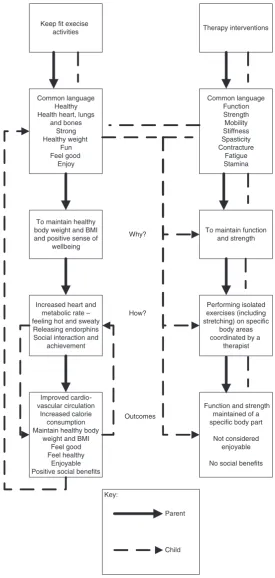
Theory development
By mapping the subjective norms and conceptualizations of children and young people compared with parents we could create an analytical model showing some distinct differ-ences and misconceptions (Figure 3).
Discussion
We report the first evidence as to how children who use wheelchairs and their parents conceptualized physical exer-cise, keeping fit and the impact of keep-fit activities on chil-dren’s bodies. The children conceptualized their health and fitness differently to typically developing children who are more acutely aware of their weight (Thomas et al. 2014). Unlike their parents, children across the age range broadly confused the purpose and outcomes of physical exercise with therapy and incorrectly understood the effects of phys-ical exercise on body function and strength, preventing stiff-ness, increasing stamina and reducing fatigue. The language associated with therapy is likely to have been engrained from a young age when they were first exposed to thera-pists and therapy interventions. We believe that more appropriate and more consistent language and terminology needs to be used during interactions with these children and their families so that keep-fit activities and benefits are bet-ter described, differentiated and understood.
Although confused about the anticipated outcomes of physical exercise, children experienced wide-ranging posi-tive impacts and social and health benefits from regularly participating in physical exercise. A recent systematic review likewise showed that children conceptualized their wheelchair should provide more than just mobility and should include a range of lifestyle benefits and opportunities for participation in physical and social activities (Brayet al. 2014). Even some outcomes perceived as a negative impact, such as being tired after exercise in the short term, could be considered positive, as it indicates an exercise intensity that was likely physiologically beneficial.
Nonetheless, these important new findings need to be con-textualised in the specific context of an atypical group of 24 wheelchair using children, 21 of which actively engaged in physical exercise and bucked the international trend for being very overweight with highly elevated body fat. The results of physiological assessments showed that the children had good levels of cardiovascular fitness and healthy metabolic profiles. Despite high levels of physical exercise, their body fat levels were still higher than desirable. Improved levels of
cardiovascular fitness and metabolic profiles were also reported in our systematic review of physical exercise inter-ventions (O’Brienet al.2016).
We think it possible that the subjective norms of these highly active and atypical disabled children are likely to have a multi-directional interaction that contextualised their (mis)understanding and conceptualization of keeping fit and physical exercise. Their misconceptions about expected out-comes of physical exercise (which were more aligned with therapy outcomes) inadvertently contributed to motivating them to do more physical exercise and conversely physical exercise participation influenced their subsequent conceptu-alizations of the benefits of keeping fit.
Although there were exceptions, parents of the atypically fit children were generally also engaged in physical exercise and understood the benefits of keeping fit. Parents did not appear to conceptualize their children as particularly ‘frag-ile’ or any less in need of maintaining general health and fitness compared with typically developing counterparts. They did not seem to be overly ‘protective’ (a common cop-ing style of parents of disabled children, see Antle et al. 2008, Guite et al. 2011) and despite the extra effort required and recognition of the numerous barriers, they managed to transport their children to physical exercise activities. Some parents also supported simple keep-fit exer-cises at home on a regular basis. Exercise had become a pleasant habit and a routine in children’s lives and they liked the feeling of well-being in the same way as typically developing children.
Despite the importance of weighing and measuring chil-dren in universal child health screening programmes none of the 24 children or their parents could remember when they were last weighed or knew what they weighed until we told them (Department of Health 2010). Children attended both mainstream and special schools and although it may be assumed that special schools would be more likely to have accessible weighing scales and height sticks, the children who attended special schools and their parents could not recall their children being weighed and measured. Children who attended special schools did, however, generally have greater access to physical exercise and sporting activities.
done using body composition measurement with bioelectri-cal impedance analysis–a simple test to measure body fat. Body composition measurement should be made available
for these children rather than requesting accessible scales and height sticks. Nurses will need additional training to do this routinely.
Key:
To maintain function and strength Common language
Function Strength Mobility Stiffness Spasticity Contracture
Fatigue Stamina
To maintain healthy body weight and BMI and positive sense of
wellbeing Common language
Healthy Health heart, lungs
and bones Strong Healthy weight
Fun Feel good
Enjoy
Why?
Performing isolated exercises (including stretching) on specific
body areas coordinated by a
therapist Increased heart and
metabolic rate – feeling hot and sweaty
Releasing endorphins Social interaction and
achievement
Function and strength maintained of a specific body part
Not considered enjoyable
No social benefits Improved
cardio-vascular circulation Increased calorie
consumption Maintain healthy body
weight and BMI Feel good Feel healthy
Enjoyable Positive social benefits
How?
Outcomes
Therapy interventions Keep fit execise
activities
Parent
Child
Although there has been investment to develop disability sports for children, there are fewer keep-fit activities avail-able for children who use wheelchairs to use on a daily basis without the need for expensive special equipment or participating in a team or group activity (English Federation for Disability Sport no, date).
Strengths and limitations
One of the strength is the longitudinal engagement in data collection and gaining different child and adult perspectives on the same phenomena of interest.
Asking children and their families to self-select to partici-pate in a study about their fitness had the effect of attract-ing those already participatattract-ing in physical exercise and those who did not were very unlikely to respond. Around 60% of the sample had Cerebral Palsy, which mirrors other studies but does not represent the demographic of the total population of children who use wheelchairs. This evidence constitutes useful feasibility information to inform the design and recruitment strategies for future studies.
Conclusion
The general health and fitness of disabled children, espe-cially those with mobility impairments, is not sufficiently acknowledged in policy or proactively monitored and addressed in practice. Proactive and physically active par-ents can go some way to compensate for the lack of health promotion support and advice and to overcome the consid-erable barriers, to enable their disabled children to engage in and benefit from physical exercise.
Introduction of body composition measurement is required into school health screening for children who need wheel-chairs. PE lessons and teacher training need further improve-ment so more children engage in exercise. Misconceptions and misunderstandings of children about the differences between and benefits of therapy and physical exercise are likely to hinder their ability to better self-manage their health and weight as they grow up. Professionals (including nurses) need to improve the clarity of their communications to cor-rect children’s misunderstandings about the respective bene-fits of therapy and physical exercise. Further research is needed in this critically under researched area.
Acknowledgements
We gratefully acknowledge the following study advisors for their time and supporting the research: Marcus Politis and Mark Richards, Disability Sports Wales; Katherine Wyke,
Contact a Family Wales; Amanda Hopkin, Whizz Kidz and Michael Hayes, Wheelchair user representative. We thank Ruth Owen, CEO Whizz Kidz and Carol McCudden North Wales Wheelchair Service.
We acknowledge Rhiannon Whitaker for contributing to a discussion on the findings and to Jacob Meaton for sup-porting the research team at the Family Day.
Funding
The National Institute for Social Care and Health Research Wales (now Health and Care Research Wales) funded the study. Grant Reference Number RFS-12-08. The views expressed are those of the researchers and not the funder.
Conflicts of interest
No conflict of interest was declared by the authors in rela-tion to the study itself. Note that Jane Noyes is a JAN editor but, in line with usual practice, this paper was sub-jected to double blind peer review and was edited by another editor.
Author Contributions
All authors have agreed on the final version and meet at least one of the following criteria [recommended by the ICMJE (http://www.icmje.org/recommendations/)]:
•
substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data;•
drafting the article or revising it critically for important intellectual content.Supporting Information
Additional Supporting Information may be found in the online version of this article at the publisher’s web-site.
Data S1: Application of the Theory of Planned Behaviour (Azjen, 1991)
References
Ajzen I. (1991) The theory of planned behavior. Organizational Behavior and Human Decision Processes50, 179–211.
American Academy of Pediatrics, Committee on Nutrition. (2003) Policy statement on prevention of pediatric overweight and obesity.Pediatrics112, 424.
families of adolescents with physical disabilities. Child: Care, Health and Development34(2), 185–193.
Atlasti. (2011)Scientific Software, Version 6. Retrieved from http:// atlasti.com on 11 March 2016.
Booth A. (2006) Clear and present questions: formulating questions for evidence based practice.Library Hi Tech24(3), 355–368. Bray N, Noyes J, Edwards RT & Harris N. (2014) Wheelchair
interventions, services and provision for disabled children: a mixed-method systematic review and conceptual framework.BMC Health Services Research14:309. doi: 10.1186/1472-6963-14-309 Carroll C., Booth A. & Cooper K. (2011) A worked example of’
best fit’ framework synthesis: a systematic review of views concerning the taking of some potential chemopreventive agents.
BMC Medical Research Methodology11(1), 1–9.
ChiMat Child and Maternal Health Observatory. (2011) Disability and obesity: the prevalence of obesity in disabled children. Retrieved from http://www.chimat.org.uk/resource/item.aspx? RID=115188 on 11 March 2016.
Department of Health (2010) Healthy Weight, Healthy Lives: National Child Measurement Programme. Retrieved from http:// webarchive.nationalarchives.gov.uk/20130107105354/http:// www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/docume nts/digitalasset/dh_115055.pdf on 11 March 2016.
Department of Health (2011) Healthy Lives, Helahty People: A call to action on obesity in England. Retrieved from https:// www.gov.uk/government/uploads/system/uploads/attachment_da ta/file/213720/dh_130487.pdf on 11 February 2016.
English Federation for Disability Sport (no date) £10.2 Million Legacy Investment to Deliver More Sport for Disabled People. Retrieved from https://www.sportengland.org/news-and-features/ news/2012/december/3/102-million-legacy-investment-to-deliver-more-sport-for-disabled-people/ on 11 March 2016.
Guite J.W., McCue R.L., Sherker J.L., Sherry D.D. & Rose J.B. (2011) Relationships Among Pain, Protective Parental Responses and Disability for Adolesecnets with Chronic Musculoskeletal Pain: the Mediating Role of Pain Catastrophizing. Clinical Journal of Pain27(9), 775–781.
National Institute for Health and Clinical Excellence (NICE. (2009) Promoting physical activity, active play and sport for
pre-school and school-age children in family, pre-school, school and community settings. Retrieved from http://www.nice.org. uk/nicemedia/live/11773/42883/42883.pdf on 1 December 2012. O’Brien T.D., Noyes J., Spencer L.H., Kubis H.P., Hastings R.P., Edwards R.T., Bray N. & Whitaker R. (2014) ‘Keep-fit’ interventions to improve health and fitness of children and young people who use wheelchairs: mixed-method systematic review protocol.Journal of Advanced Nursing70(12), 2942–2951. O’Brien T.D., Noyes J., Spencer L.H., Kubis H.P., Edwards R.T.,
Bray N. & Whitaker R. (2015) Well-being, health and fitness of children who use wheelchairs: feasibility study protocol to develop child-centred ‘keep-fit’ exercise interventions.Journal of Advanced Nursing71(2), 430–440. doi:10.1111/jan.12482. O’Brien TD, Noyes J, Spencer L, Kubis H.-P., Hastings R. &
Whitaker R. (2016) A Systematic Review of ‘Keep fit’ exercise interventions to improve health, fitness and wellbeing of children and young people who use wheelchairs. BMJ Open Sport & Exercise Medicine 2, e000109. doi:10.1136/bmjsem-2016-000109.
Public Health England (2014) Obesity and Disability: Children and Young People. Retrieved from http://www.efds.co.uk/assets/0000/ 9592/OO280.pdf on 11 March 2016.
Scianni A., Butler J.M., Ada L. & Teixeira-Salmela L.F. (2009) Muscle strengthening is not effective in children and adolescents with cerebral palsy: a systematic review. Australian Journal of Physiotherapy55, 81–87.
Scott R. (2010)The Health Benefits of Play and Physical Activity for Disabled Children and Young People: Kids Briefing Paper. KIDS NDD, London.
Spencer L., Ritchie J. & O’Connor W. (2003) Carrying out qualitative analysis. In Qualitative Research Practice: A Guide for Social Science Students and Researchers. SAGE, London, pp. 219–262.
Thomas S.L., Olds T., Pettigrew S., Randle M. & Lewis S. (2014) ‘Don’t eat that you’ll get fat’ Exploring how parents and children conceptualise and frame messages about the causes and consequences of obesity.Social Science & Medicine119, 114–122. WHO (2015). Overweight and Obesity Factsheet. http://www.who.
int/mediacentre/factsheets/fs311/en/ on 15 March 2016.
TheJournal of Advanced Nursing (JAN)is an international, peer-reviewed, scientific journal.JANcontributes to the advancement of evidence-based nursing, midwifery and health care by disseminating high quality research and scholarship of contemporary relevance and with potential to advance knowledge for practice, education, management or policy.JANpublishes research reviews, original research reports and methodological and theoretical papers.
For further information, please visitJANon the Wiley Online Library website: www.wileyonlinelibrary.com/journal/jan
Reasons to publish your work inJAN:
• High-impact forum:the world’s most cited nursing journal, with an Impact Factor of 1·917–ranked 8/114 in the 2015 ISI
Jour-nal Citation Reports©(Nursing (Social Science)).
• Most read nursing journal in the world:over 3 million articles downloaded online per year and accessible in over 10,000 libraries
worldwide (including over 3,500 in developing countries with free or low cost access).
• Fast and easy online submission:online submission at http://mc.manuscriptcentral.com/jan.
• Positive publishing experience:rapid double-blind peer review with constructive feedback.
•Rapid online publication in five weeks:average time from final manuscript arriving in production to online publication.
• Online Open:the option to pay to make your article freely and openly accessible to non-subscribers upon publication on Wiley