Immunohistochemical Expression of CCND1
and p16 Genes in Tissue Microarray
Key words: Basal cell carcinoma (BCC), CCND1, Immunohistochemistry (IHC), p16, skin cancer, Tissue Microarray (TMA)
a Sima Ataollahi Eshkoor, a Patimah Ismail, b Sabariah Abdul Rahman, a Mirsaed Mirinargesi
c Soraya Ataollahi Oshkour
a Department of Biomedical, b Department of Pathology, Faculty ofMedicine and Health Sciences, Universiti Putra Malaysia,
43400UPM, Serdang, Selangor, Malaysia,
c Shafa st. Hasan Makiabadi clinic, Sirjan, Iran.
ABSTRACT
Background and objectives: Immunohistochemistry using Tissue Microarrays (IHC-TMA) is a useful method to identify the alteration of CCND1 and p16 genes. This study determined the sensitivity of this analysis to find the protein over-expression of CCND1 and p16 in Basal Cell Carcinoma (BCC).
Method: Twenty-five spot samples obtained from different patients who were diagnosed with BCC and four spot samples of normal skin tissue. The slides were assessed by IHC-TMA technique.
Results: The study revealed this technique is a feasible and efficient method to diagnose the minute numbers of BCC cells
in the skin tissue. It is a reliable method, which assesses a large number of samples in a research setting. This study illustrated a significant protein expression of CCND1 and p16 genes in TMA samples of 25 patients of BCC compared to normal skin tissue (p<0.05). The findings of this study demonstrated the over-expression of CCND1 and p16 proteins in BCC tissue samples using IHC-TMA method as compared to normal human skin tissue.
Interpretation and Conclusion: Alteration of both CCND1 and p16 genes could lead to the abnormal prolifration activity in the cells and resulting in BCC.
INTRODUCTION
Tissue microarray (TMA) is a method to exhibit tissues from multiple blocks in a single histological section. It allows examination of the expression of several molecular markers such as protein, mRNA, DNA for improving the discovery process and accelerating its efficiency.1-4 A large number
This method permits application of high-dimensional biology techniques in the pathology and translational researches. The TMA improved efficient use of material, personnel, and reagents.3, 4 One of the main advantages of
the TMA is the histological studies such as IHC, fluorescence in situ hybridization, chromogenic in situ hybridization and RNA in situ hybridization with standard protocols.1, 3-4, 6-8 It has been widely used in cancer research
identifying molecular biomarkers with diagnostic and prognostic values.1, 9-12 The TMA and the conventional
whole-section tissue have same validity for histology and IHC approaches.9, 10, 13-18 The TMAs containing two to
four tissue cores provide a degree of concordance ranging from 95% to 97% in immunoreactivity.10, 13, 14, 17, 18 Therefore,
it is a tool for biomarker discovery.18
The BCC is the most common type of skin cancer.19, 20, 21, 22 The incidence of the BCC in the white
populations, who are at higher risk, is between 18% and 40% with higher occurrence in men. Before the age of 20 years the BCC is rarely seen but the incidence of it grows up with increased age. The BCCs are slow growing malignancies but without the treatment can become dangerous. The metastatic rate ranges from 0.0028% to 0.55%.23
The principal cause of BCC is chronic sun exposure over a number of years as the result of chronic sunlight exposure as a child. Mostly the patients with BCC are over 40 years old24 and the greatest incidence is in people older than 55
years.25
BCCs occur most frequently on parts of the body that are exposed to the sun, such as the face, ears, neck, scalp, shoulders, and back. Some people whose occupations require a significant amount of time outdoors or spend extensive leisure time in the sun are at higher risk of taking the BCC of skin.26
CCND1 (Cyclin D1)/(CDK)4-6 complexes initiate the phosphorylation of pRb and cyclin E/CDK2 complex completes the procedure in late G1 phase. Alterations in Cyclin and Cyclin-Dependent Kinase (CDK) expression result in increased cell proliferation and contribute to malignancy.27 CCND1 protein is a member of
cell-cycle-associated nuclear proteins and is encoded by the CCND1 gene. CCND1 gene induces G1 to S-phase transition, promotes cell proliferation and plays a major role in oncogenesis.28
CCND1 gene is disrupted in the cancer cell genome usually by the process of gene amplification or chromosome translocation what may lead to cancer development.29 In
humans over-expression of CCND1 is seen in many tumours such as endometrial,30 thyroid,31 urothelial bladder,32
breast,33 brain gliomas,34 esophageal35 and colorectal
cancers36 and also Squemous Cell Carcinoma (SCC).35
p16 protein plays a key role in cell cycle control at the G1-S transition.37 p16 gene is one of the most altered genes
observed in different human neoplasms.38, 39, 40, 41 It is
believed to encode a negative regulatory protein which prevents cell cycle progression from G1 to S phase by inhibiting the CDK4 or CDK6/cyclin D complex and subsequently Rb protein phosphorylation.38, 42 It reveals the
p16 gene may play a critical role in the pathogenesis of neoplasms.43
Pathologic examination of the BCC suggests important information about the potential mechanisms of disease associated with the genes. Thus far, TMAs have not been used for the systematic studies of the BCC and for biomarker discovery in research study. The point of this study was to assess the feasibility and efficiency of TMAs with BCC tissue using IHC analysis in the finding of the role of CCND1 and p16 genes alterations in the formation of BCC.
MATERIAL AND METHODS
Twenty-five spot samples of formalin-fixed, paraffin embedded AccuMax® TMA slides obtained from twenty-five different patients from Korea (CAT#: A216; LOT#: 122120310121, Location: 73 and 74) who were diagnosed with BCC and four spot samples of normal skin tissue. Each size of single spot is 1.0 mm in diameter. IHC studies were performed on the slides using commercially available monoclonal anti- CCND1 antibody obtained from Research Biolabs (Danvers, USA) and anti-p16 polyclonal antibody as named anti-p16INK4a antibody from Lab vision (Fremont, CA, USA).
Immunohistochemical staining was conducted using DAKO Envision TM system + HRP DAB + Rb / Mo Kit (DAKO Co., Carpinteria, CA, USA) according to the manufacturer’s instructions. Briefly, the slides were
dewaxed by heating on hot plate at 600C and then
deparaffinised. The slides were heated in a microwave oven for 20 min in 10 mM citrate-Na (pH 6.0). After incubation with dual endogenous blocking enzyme for 10 min, sections were incubated with primary antibodies described above for over night at 40C with an antibody dilution of 1: 400 for
were ready to view by light microscope (BX 51, New York, USA).
SCORING SYSTEM
IHC interpretation is qualitative and semi-quantitative study which minimized the many known inconsistencies among laboratories with regard to reagents and methods. This assay may improve intra and inter-laboratories standardization and reproducibility of the study.44
As the strength of reaction was variable we graded the intensity of reaction on a numerical scale from + to +++, reflecting weak, moderate, and strong reactions. We also recorded the extent of reactivity within target cell population on 1 to 4 scales indicating convincingly positive nucleus reaction in 1-25, 26-50, 51- 75, and 76-100% of the cells. The evaluation of IHC staining45, 46, 47 on the slides
was based on signal intensity which was carried out using scoring system. The total scoring for every single spot in the slides counted based on the score for percentage of positive cells and staining intensity.
Statistical Analysis
The data of IHC was stored and analyzed by means of SPSS.12 version software (SPSS Inc, Chicago, IL, USA). The protein expression data of CCND1 and p16 genes were evaluated non-parametrically using Mann-Whitney test. Tests were considered significant when their p value was less than 0.05.
RESULTS
Site of reaction product
Twenty-five paraffin embedded tissue samples obtained from the patients diagnosed with BCC. In analysis tissues were compared with control tissues to enable complete analysis. All BCC tissue samples revealed increasing of CCND1 and p16 protein.
The immunohistochemical analysis expressed the protein expression of CCND1 in the nuclei of tumoral and normal cells while p16 protein expression was visible in the nuclear and cytoplamic area of the cells. All slides were tested at least three times for the presence of both genes.
The protein over-expression of CCND1 (p = 0.024) and p16 (p = 0.008) genes revealed a statistically significant value in the BCC samples. There is a direct correlation between expression of CCND1 and p16 genes. The results demonstrated dependency of their work (r=0.399 and
p=0.032).
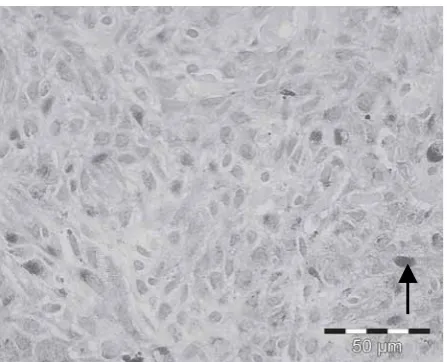
Depending on the gene the staining reaction in IHC is seen in the nucleus, cytoplasm or both. Protein expression of CCND1 and p16 in the BCC is higher than normal skin tissue. CCND1 (Fig1) and p16 (Fig 3) protein are visible in normal skin tissue. Figure 2 shows the protein expression of CCND1 and figure 4 expresses the p16 protein expression in the malignant tissue. The brown staining in the involved cells demonstrated the protein expression of the genes. The number of stained cells in the malignant tissue for both of these genes is more than that noted in the normal skin tissue.
Fig 1: Immunostaining analysis of CCND1 in normal skin tissue illustrates the mild staining intensity (+1) in nuclei of normal epidermal cells (arrow). (Magnification 40X)
cells even though in small numbers. Hence this method will be good for early cancer detection which is the trend in cancer management for optimal outcome.
The knowledge of presence or absence of genes in cancer cells will be one of the most powerful prognostic factors in malignant tissue. The observation of some patients who have positive IHC in face of negative histology and immunohistology, allows prediction of increased risk for further disease progression.
Such finding can certainly be interpreted as supporting the view that new approach is able to identify minute numbers of tumoral cells which have the capacity to proliferate and disseminate. IHC is used to identify protein expression in the inducer cells in the BCC tissue sections. p16 and CCND1 proteins were expressed by all BCC samples which demonstrated the high sensitivity and specificity of this approach. Deregulation of cell cycle G1-restriction point control via abnormalities of Rb-pathway components is a frequent event in the formation of cancer.48
The present study was undertaken to assess expression of the considered genes in BCC of skin and explain their locations in the tumoral and normal skin tissue. The current study results suggested that CCND1 gene changes could lead to alteration of the cell cycle and cell proliferation. CCND1 has been demonstrated to be present at a higher level in BCC rather than normal skin tissue and leads to cell entering cell cycle proliferation resulting development the cancerous in BCC.49, 50
Over-expression of CCND1 protein is important to take a growth advantage18, 19 and plays a critical role in the skin
carcinogenesis.51 It suggested that the decreasing of
expression may lead to cell death.52 The present study also
demonstrated the over-expression of p16 gene in BCC of skin. Changes of p16 gene have been reported in some cancers such as gliomas and mesotheliomas, nasopharyngeal, pancreatic, biliary tract tumors, acute lymphoblastic leukaemias, breast cancer, multiple melanomas,53, 54 colorectal cancer55 and a subset of
dysplastic cells of all precancerous and cancerous skin lesions such as actinic keratoses, SCC in situ, Bowen’s carcinoma, and SCC infected with HPV independent of sun exposure.56
p16 is important gene in proliferating cells in normal and cancer proliferation process. Based on the studies the p16 expression has strong staining presentation in skin cancer tissue unlike expectation of low staining in the other cancers.57, 51, 52 The present study revealed the strong
expression of p16 protein in BCC and confirmed the other
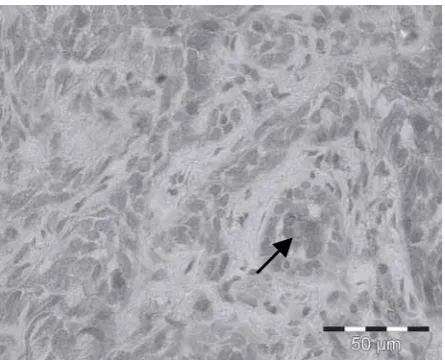
Fig 3: Immunostaining analysis shows nucleus and cytoplasm expression of p16 protein using Tissue Microarray sample of normal skin tissue. The nuclei and cytoplasm of epidermal cells express staining at moderate intensity (+2) (arrow). (Magnification 40X)
Fig 4: Immunohistochemical study for p16 in Tissue Microarray of Basal Cell Carcinoma sample is showing strong staining intensity (+3) in the nuclei and cytoplasm of tumoral cells of skin (arrow). (Magnification 40X)
DISCUSSION
studies of the skin cancer.58, 59, 55
The p16 could be a useful factor to predict the prognosis of the cancer and gene therapy might prevent the increased proliferation resulting of p16 alteration. The results of this present study indicated that TMA-IHC technique is a useful method to approach the p16 gene in the cancerous tissue. The p16 protein expression in all BCC samples revealed the high sensitivity and specificity of TMA-IHC for detection of this protein expression. The in situ detection of p16 gene has thus considerable potential as an assay to detect occult metastatic tumor cells from BCC and other neoplasms.
Our results and those from the others supported the argument of demonstrating enhanced signals for these genes in BCC and identifying the presence of small number of tumoral cells in the cancerous tissue. The results demonstrated that CCND1 and p16 genes are not markers of the BCC but they can predict treatment outcomes of disease.
ACKNOWLEDGMENT
I am extremely grateful to AccuMax® from Korea for giving samples to me and also so thankful from the patients who precipitated in this project.
REFERENCES
1 Kononen J, Bubendorf L, Kallioniemi A, Barlund M, Schraml P, Leighton S, et al. Tissue microarrays for high-throughput molecular profiling of tumor specimens. Nat Med 1998; 4: 844–847.
2 Hoos A, Cordon-Cardo C. Tissue microarray profiling of cancer specimens and cell lines: Opportunities and limitations. Lab Invest 2001; 81: 1331–1338.
3 Bhargava R, Lal P, Chen B. Feasibility of using tissue microarrays for the assessment of HER-2 gene amplification by fluorescence in situ hybridization in breast carcinoma. Diagn Mol Pathol 2004; 13: 213–216.
4 Bhargava R, Oppenheimer O, Gerald W, Jhanwar SC, Chen B. Identification of MYCN gene amplification in neuroblastoma using chromogenic in situ hybridization (CISH): An alternative and practical method. Diagn Mol Pathol 2005; 14: 72–76. 5 Battifora H. The multitumor (sausage) tissue block: Novel
method for immunohistochemical antibody testing. Lab Invest 1986; 55: 244–248.
6 Simon R, Mirlacher M, Sauter G. Tissue microarrays. Methods Mol Med 2005; 131: 257–268.
7 Tzankov A, Went P, Zimpfer A, Dirnhofer S. Tissue microarray technology: Principles, pitfalls and perspectives-lessons learned from hematological malignancies. Exp Gerontol 2005; 40: 737–744.
8 Chang E, Lee A, Lee E, Lee H, Shin O, Oh S, et al. HER-2/neu oncogene amplification by chromogenic in situ hybridization in 130 breast cancers using tissue microarray and clinical follow-up studies. J Korean Med Sci 2004; 19: 390-396.
9 Sallinen SL, Sallinen PK, Haapasalo HK, Helin HJ, Helen PT,
Schraml P, et al. Identification of differentially expressed genes in human gliomas by DNA microarray and tissue chip techniques. Cancer Res 2000; 60: 6617–6622.
10 Rubin MA, Dunn R, Strawderman M, Pienta KJ. Tissue microarray sampling strategy for prostate cancer biomarker analysis. Am J Surg Pathol 2002; 26: 312–319.
11 Lee P, Rosen DG, Zhu C, Silva EG, Liu J. Expression of progesterone receptor is a favorable prognostic marker in ovarian cancer. Gynecol Oncol 2005; 96: 671–677.
12 Fowler JM, Ramirez N, Cohn DE, Kelbick N, Pavelka J, Ben Shachar I, et al. Correlation of cyclooxygenase-2 (COX-2) and aromatase expression in human endometrial cancer: Tissue microarray analysis. Am J Obstet Gynecol 2005; 193: 1262–127. 13 Camp RL, Charette LA, Rimm DL. Validation of tissue microarray technology in breast carcinoma. Lab Invest 2000; 80: 1943–1949.
14 Hoos A, Urist MJ, Stojadinovic A, Mastorides S, Dudas ME, Leung DH, et al. Validation of tissue microarrays for immunohistochemical profiling of cancer specimens using the example of human fibroblastic tumors. Am J Pathol 2001; 158: 1245-1251.
15 Chiesa-Vottero AG, Rybicki LA, Prayson RA. Comparison of proliferation indices in glioblastoma multiforme by whole tissue section vs. tissue microarray. Am J Clin Pathol 2003; 120: 902–908.
16 Jourdan F, Sebbagh N, Comperat E, Mourra N, Flahault A, Olschwang S, et al. Tissue microarray technology: Validation in colorectal carcinoma and analysis of p53, hMLH1, and hMSH2 immunohistochemical expression. Virchows Arch 2003; 443: 115–121.
17 Tzankov A, Zimpfer A, Pehrs AC, Lugli A, Went P, Maurer R, et al. Expression of B-cell markers in classical Hodgkin lymphoma: A tissue microarray analysis of 330 cases. Mod Pathol 2003; 16: 1141–1147.
18 Watanabe A, Cornelison R, Hostetter G. Tissue microarrays: Applications in genomic research. Expert Rev Mol Diagn 2005; 5: 171–181.
19 Levi F, Randimbison L, Te VC, La VECCHIA C. Non-Hodgkin’s lymphomas, chronic lymphocytic leukaemias and skin cancers. Br J Cancer 1996; 74: 1847-1850.
20 Magnus K. The Nordic profile of skin-cancer incidence: a comparative epidemiological study of the three main types of skin cancer. Int J Cancer 1991; 47: 12-19.
21 Preston DS, Stem RS. Nonmelanoma cancers of the skin. N Engl J Med 1992; 327: 1649-1662.
22 Franceschi S, Levi F, Randimbison L, La Vecchia C. Site distribution of different types of skin cancer new aetiological clues. Int J Cancer 1966; 67: 24-28.
23 Wong CSM, Strange RC, Lear JT. Clinical review: Basal cell carcinoma. BMJ 2003; 327: 794-798
24 Mackie R. Epidermal skin tumours. Textbook of Dermatology. 5th edn, Vol 2, Oxford: Blackwell Scientific Publications, 1992; pp1456-1504.
25 The World Health Organization http://www.who.int/uv/faq/ skincancer/en/index1.html.
26 The Skin Cancer Foundation http://www.skincancer.org/basal/ index.php.
27 Bali A, O’Brien PM, Edwards LS, Sutherland RL, Hacker, NF, Henshall SM. Cyclin D1, p53, and p21Waf1/Cip1 Expression Is Predictive of Poor Clinical Outcome in Serous. Clin Cancer Res 2004; 10: 5168–5177.
28 Balcerczak E, Pasz-Walczak G, Kumor P, Panczyk M, Kordek R, Wierzbicki R, et al. Cyclin D1 protein and CCND1 gene expression in colorectal cancer. Eur J Surg Oncol 2005; 31: 721-726.
Mammary Gland Biol Neoplasia 2004; 9: 95–104.
30 Moreno-Bueno G, Rodriguez-Perales S, Sanchez-Estevez C, Marcos R, Hardisson D, Cigudosa JC, et al. Molecular alterations associated with cyclin D1 over expression in endometrial cancer. Int J Cancer 2004; 110: 194–200. 31 Nakashima M, Meirmanov S, Naruke Y, Kondo H, Saenko V,
Rogounovitch T, et al. Cyclin D1 over expression in thyroid tumors from radio-contaminated area and its correlation with Pin1 and aberrant beta-catenin expression. J Pathol 2004; 202: 446–455.
32 Mhawech P, Greloz V, Oppikofer C, Szaly-Quinodoz I, Herrmann F. Expression of cell cycle proteins in T1a and T1b urothelial bladder carcinoma and their value in predicting tumor progression. Cancer 2004; 200: 2367–2375.
33 Stendahl M, Kronblad AA, Ryden L, Emdin S, Bengtsson NO, Landberg G. Cyclin D1 over expression is a negative predictive factor for tamoxifen response in postmenopausal breast cancer patients. Br J Cancer 2004; 90: 1942–1948.
34 Tan PG, Xing Z, Li ZQ. Expression of cyclin D1 in brain gliomas and its significance. Ai Zheng 2004; 23: 63–65.
35 Wu MY, Zhuang Ch X, Yang HX, Liang YR. Expression of Egr-1, c-fos and cyclin D1 in esophageal cancer and its precursors: an immunohistochemical and in situ hybridization study. World J Gastroenterol 2004; 10: 476–480.
36 Kristt D, Turner I, Koren R, Ramadan E, Gal R. Over expression of cyclin D1 mRNA in colorectal carcinomas and relationship to clinicopathological features: an in situ hybridization analysis. Pathol Oncol Res 2000; 6: 65–70.
37 Ghiorzo P, Villaggio B, Sementa AR, Hansson J, Platz A, Nicolo G, et al. Expression and Localization of Mutant p16 Proteins in Melanocytic Lesions From Familial Melanoma Patients. Hum Pathol 2004; 35: 25-33.
38 Kamb A, Gruis NA, Weaver-Feidhaus J, Liu Q, Harshman K, Tavtigian SV, et al. A cell cycle regulator potentially involved in genesis of many tumor types. Science 1994; 264: 436-440. 39 Nobori T, Miura K, Wu DJ, Lois A, Takabayashi K, Carson DA.
Deletions of the cyclin-dependent kinase-4 inhibitor gene in multiple human cancers. Nature 1994; 368: 753-756.
40 Okamoto A, Demetrik DJ, Spillare EA, Hagiwara K, Hussain SP, Bennett WP, et al. mutations and altered expression of p16 INK4 in human cancer. Proc. Natl. Acad. Sci. USA 1994; 91: 11045-11049.
41 Drewa G, Powierska-Czarny J. Genetic basis of malignant melanoma. Postepy Hig Med Dosw 1998; 52: 367-380. 42 Serrano M, Hannon GJ, Beach D. a new regulator motif in cell
cycle control causing specific inhibition of cyclin D/CDK4. Nature 1993; 366: 704-707.
43 Liew CT, Li HM, Lo LW, Leow CK, Chan JYH, Hin LY, et al. high frequency of p16 INK4A gene altereations in hepatocellular carcinoma. Oncogen 1999; 18: 789-795.
44 Sompuram SR, Kodela V, Zhang K, Ramanathan H, Radcliffe G, Falb P, et al. A Novel Quality Control Slide for Quantitative Immunohistochemistry Testing. J Histochem Cytochem 2002; 50: 1425–1433.
45 Argani P, Iacobuzio-Donahue C, Ryu B, Rosty C, Goggins M, Wilentz RE, et al. Mesothelin Is Over-expressed in the Vast
Majority of Ductal Adenocarcinomas of the Pancreas: Identification of a New Pancreatic Cancer Marker by Serial Analysis of Gene Expression (SAGE). Clin Cancer Res 2001; 7: 3862–3868.
46 Franklin RB, Feng P, Milon B, Desouki MM, Singh KK, Kajdacsy-Balla A. et al. hZIP1 zinc uptake transporter down regulation and zinc depletion in prostate cancer. Mol Cancer 2005; 4: 32.
47 Sanno N, Jin L, Qian X, Osamura RY, Scheithauer BW, Kovacs K, et al. Releasing Hormone and Gonadotropin-Releasing Hormone Receptor Messenger Ribonucleic Acids Expression in Nontumorous and Neoplastic Pituitaries. J Clin Endocrinol Metab 1997; 82: 1974–1982.
48 Utikal J, Udart M, Leiter U, Kaskel P, Peter RU, Krahn G. Numerical abnormalities of the Cyclin D1 gene locus on chromosome 11q13 in non-melanoma skin cancer. Cancer Lett 2005; 219: 197-204.
49 Lu Q, Lu F, Yang Z, Wen H, Yan L, Chen S, Liu BA. Study on regulators of the cell cycle in cutaneous squamous cell carcinoma. Hunan Yi Ke Da Xue Xue Bao 1999; 24: 438-440.
50 Kim AL, Athar M, Bickers DR, Gautier J. Stage -specific Alterations of Cyclin Expression During UVB-induced Murine Skin Tumor Development. J Photochem Photobiol 2002; 75: 58–67.
51 Yamamoto H. Enhanced Skin Carcinogenesis in Cyclin D1 conditional Transgenic Mice: Cyclin D1 Alters Keratinocyte Response to Calcium-induced Terminal Differentiation. Cancer Res 2002; 62: 1641–1647.
52 Sauter ER, Nesbit M, Litwin S, Klein-Szanto AJ, Cheffetz S, Herlyn M. Antisense Cyclin D1 Induces Apoptosis and Tumor Shrinkage in Human Squamous Carcinomas. Cancer Res 1999; 59: 4876–4881.
53 Boukamp P. UV induced skin cancer. similarities-variations. J Dtsch Dermatol Ges. 2005; 3: 493-503.
54 Borg A, Sandberg T, Nilsson K, Johannsson O, Klinker M, Masback A, et al. High frequency of multiple melanomas and breast and pancreas carcinomas in CDKN2A mutation-positive melanoma families. J Natl Cancer Inst 2000; 2: 1260-1266. 55 Linardopoulos S, Street AJ, Quelle DE, Linardopoulos S, Street
AJ, Quelle DE, et al. Deletion and altered regulation of p16INK4a and p15INK4b in undifferentiated mouse skin tumors. Cancer Res 1995; 15: 5168-5172.
56 Bianchi AB, Fischer SM, Robles AI, Rinchik EM, Conti CJ. Over expression of cyclin D1 in mouse skin carcinogenesis. Oncogene 1993; 8: 1127-1133.
57 Nindl I, Meyer T, Schmook T, Stockfleth E. Human Papillomavirus and Overexpression of p16INK4a in Nonmelanom Skin Cancer. Dermatol Surg 2004; 30: 409-414.
58 Nakamura S. Enhanced expression of p16 in seborrhoeic keratosis; a lesion of accumulated senescent epidermal cells in G1 arrest. Br J Dermatol 2003; 149: 560–565.