Development and Evaluation of a CD-ROM Computer Program to Teach
Residents Telephone Management
Mary C. Ottolini, MD, MPH, and Larrie Greenberg, MD
ABSTRACT. Objective. Under managed care,
tele-phone management is crucial to pediatric practice, but an effective method is needed to teach residents telephone skills. Our objective was to design an interactive CD-ROM program to teach residents an organized, consistent approach to telephone complaints and to determine whether use of the program was associated with better subsequent telephone management than reading the same information.
Setting. The general pediatric ambulatory center of a tertiary care children’s hospital.
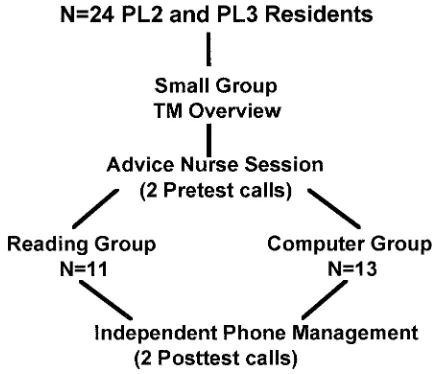
Participants. A total of 24 PL-2 and PL-3 pediatric residents.
Design. A randomized, prospective, controlled com-parison was conducted of resident management of two telephone calls: a 5-year-old with cough and trouble breathing, and a 7-year-old with fever. Thirteen residents were randomized to the computer group and 11 to the reading control group.
Intervention. Scripts, scoring, and feedback for 10 CD-ROM-simulated calls were developed from texts and pediatrician survey using a modified Delphi technique. Volunteers acted out the caller’s role in scenario scripts and were recorded onto a CD-ROM. The computer sim-ulated calls by recognizing questions typed in a free-form free-format and answering with a voice response. Feed-back was provided for omissions in history-taking and errors in assessment, triage, and home management. The computer group worked through the CD-ROM calls while the control group had equal time to read the same information.
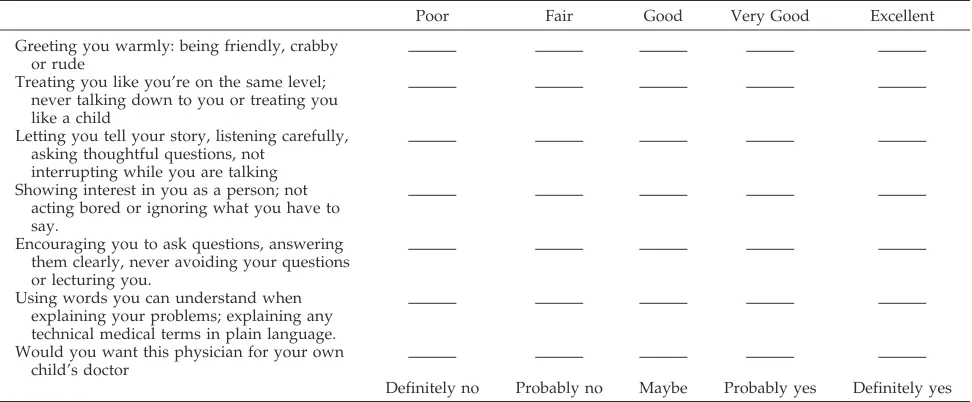
Evaluation Measures. A trained, standardized patient acted as the mother in pretest calls placed at the begin-ning of the month and posttest calls at the end. Calls were recorded and scored in a blinded manner using scoring templates and on interpersonal skills using the Patient Perception Questionnaire.
Results. Pretest scores for the two calls were similar in the computer versus the control group (cough, 70.33%
68.36 vs 68.46%66.73; fever, 75.64%69.82 vs 73.59%6 9.06). Posttest scores were significantly higher in the computer group than in the control group on both calls (cough, 79.08%68.17 vs 69613.3; fever: 83.33%69.96 vs 70.35% 6 9.66). Interpersonal skills also were similar pretest (1963.4 vs 2062.7). There was modest
improve-ment in both groups without a statistically significant difference in posttest scores (24.262.9 vs 22.563.1).
Conclusions. Use of this CD-ROM telephone man-agement program was associated with better postinter-vention telephone management. The program augments faculty instruction by teaching a consistent, general ap-proach to telephone management.Pediatrics1998;101(3). URL: http://www.pediatrics.org/cgi/content/full/101/3/e2;
telephone management, resident education, computer-aided instruction.
ABBREVIATION. PL, postgraduate level.
T
elephone management traditionally has been
an integral component of pediatric practice.
1,2Today, as primary care physicians serve as
gatekeepers for health care services under managed
care, effective telephone management is crucial.
De-spite the significance of telephone encounters in
pe-diatric practice, fewer than half of pepe-diatric
resi-dency programs provide telephone training.
3The
pediatric telephone call is especially challenging
be-cause visual assessment of a child’s appearance and
interaction with the environment are not available to
gauge the severity of illness. Failure to ask
appropri-ate questions to obtain essential information without
visual cues can lead to inappropriate assessment
and management,
4with potentially life-threatening
sequelae.
5Few telephone instructional programs have
re-ported effectiveness in teaching residents telephone
management skills. Working with an expert in
soft-ware design, we developed and evaluated a
CD-ROM interactive telephone management program to
teach residents telephone skills. The CD-ROM allows
the computer to simulate calls and provide pertinent
feedback. Our hypothesis was that guided practice
with feedback using CD-ROM cases would enable
residents to obtain information, assess patients, and
provide advice over the telephone significantly
bet-ter than those who learned by reading similar
mate-rial.
METHODS CD-ROM Development
Scripts for CD-ROM cases representing the 10 most common telephone complaints6 were written to simulate common
tele-phone conversations with parents. The cases are listed in Table 1. To determine the questions that should be asked and feedback that should be provided for the chief complaints depicted in the CD-ROM cases, the historical information essential to forming an appropriate diagnosis and management plan was extracted from
From the Department of General Pediatrics at Children’s National Medical Center and George Washington University School of Medicine, Washing-ton, DC.
This work received the Ray E. Helfer Award for Innovation in Pediatric Medical Education and was presented at the Ambulatory Pediatric Associ-ation Presidential Plenary Session, May 5, 1997, Washington, DC. Received for publication Jul 28, 1997; accepted Nov 7, 1997.
articles, standard pediatrics texts, and telephone advice texts. Questions were then formulated to elicit the essential information, and management options were listed. The lists of questions and management options for each of the 10 scenarios were presented to focus groups consisting of pediatric emergency medicine and general pediatric faculty, pediatric residents, telephone advice nurses, and community pediatricians. Members of the focus groups were asked to score questions as essential, helpful, or unnecessary, and to determine criteria for appropriate triage and home management advice. Responses were analyzed using a Delphi technique.7There was very strong agreement among
mem-bers of the focus groups regarding which questions they rated as essential and which management options they felt were appropri-ate.
In the introductory section of the program, residents were encouraged to use a consistent, organized format for taking a history over the telephone and to learn to use the parent’s descrip-tion of the child to gauge the severity of the complaint. Data-gathering was divided into nine general categories: obtaining identifying information; clarifying the chief complaint with an open-ended question; determining the severity and duration of the chief complaint; ascertaining the child’s overall appearance; previous home therapy; associated symptoms; illness exposure; medical history; and acknowledging the emotional tone of the caller.
Residents began by identifying themselves and obtaining es-sential identifying information about the caller such as parent and child’s names, child’s age, name of primary care provider, tele-phone number, and chief complaint. They were expected to follow up with an open-ended question to learn what was most worri-some about the chief complaint. An open-ended question is em-phasized because Korsch concluded in her classic communication research that failure to address the parent’s main worry resulted in dissatisfaction with the doctor–patient encounter.8 Residents
then asked directly about the severity and duration of the chief complaint, if these were not evident in response to the open-ended question.
Residents often have difficulty assessing how sick the child is over the telephone, because they have been trained to use visual cues such as the child’s environmental interaction almost intu-itively to assess the overall state of health. Therefore, they were directed to ask questions specifically about the child’s overall appearance and activity level. Previous home therapy was as-sessed to judge the level of sophistication of the caller and to gain information about previous medical advice and current manage-ment. Residents were directed to always ask about medical his-tory, including medication use, whereas a brief review of systems or determination of illness exposure was helpful for some com-plaints.
Residents also were instructed to acknowledge the emotional tone of the caller to calm or reassure parents and to establish rapport. To allow residents to respond to angry, frustrated, and frightened callers, volunteers acted out the caller’s role in scripts written for each of the scenarios and were recorded onto a CD-ROM. Residents and staff were asked how they would phrase individual questions so that different ways of phrasing key ques-tions could be programmed, enabling the computer to recognize questions typed in a free-form format and to answer with a voice response.
This program was designed to encourage a consistent, orga-nized approach to the presenting problem. Data-gathering was divided into general categories as described, followed by the assessment and triage, and concluding with call back and home management advice. Feedback was provided for omissions in
history-taking, and errors in assessment, triage, and home man-agement. The entire program can be read from the computer monitor, with the introduction and interactive data-gathering por-tions having a voice component as well.
CD-ROM Evaluation
To test our hypothesis that use of the program would result in better subsequent telephone management than reading the same information, we conducted a randomized, controlled comparison of the pre- and posttest scores of 24 second- and third-year pedi-atric residents during their month-long ambulatory rotation on two telephone scenarios placed by a trained, standardized patient. The study was conducted over a 9-month period from June 1996 until March 1997.
All second- and third-year residents were asked to participate if they did not have vacation or other scheduling conflicts during their ambulatory rotation. No residents refused. Residents con-sented to allow some of their calls to be tape-recorded, but were not told which calls were from the standardized patient.
Both groups of residents attended a small group session cov-ering the expectations and important aspects of telephone man-agement (Fig 1). Next, each resident spent a morning with the telephone advice nurse, first listening to her answer calls and then answering some calls themselves under supervision of the nurse. Practical aspects such as protocol use, documentation, and inter-personal aspects of telephone management were emphasized dur-ing this one-to-one session. The pretest calls were placed by the standardized patient during this session.
Eleven residents then were randomly assigned to the reading control group, and 13 to the computer group. Control residents were given copies of advice protocols and readings covering the same content as in computer cases. Both groups had two 90-minute sessions to complete the cases or the readings. To ensure that there was no contamination between groups, residents in the reading group were told not to share their readings with those in the computer group, and individual access codes necessary to use access the computer program were given only to those in the computer group.
After completing the readings or the cases, the residents spent two half-day sessions independently answering telephone calls from parents of patients followed in the General Pediatric Ambu-latory Center. The two posttest telephone calls were placed at this time. All were free to refer to advice protocols with pre- and posttest calls.
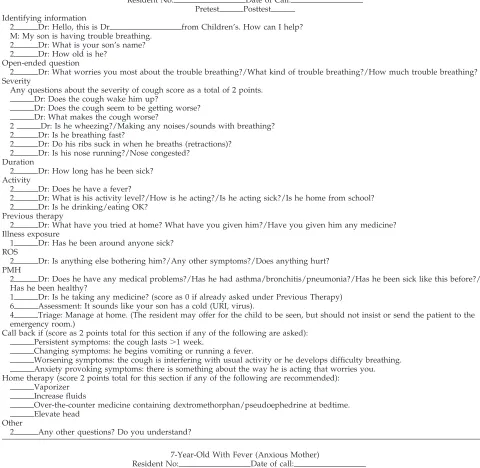
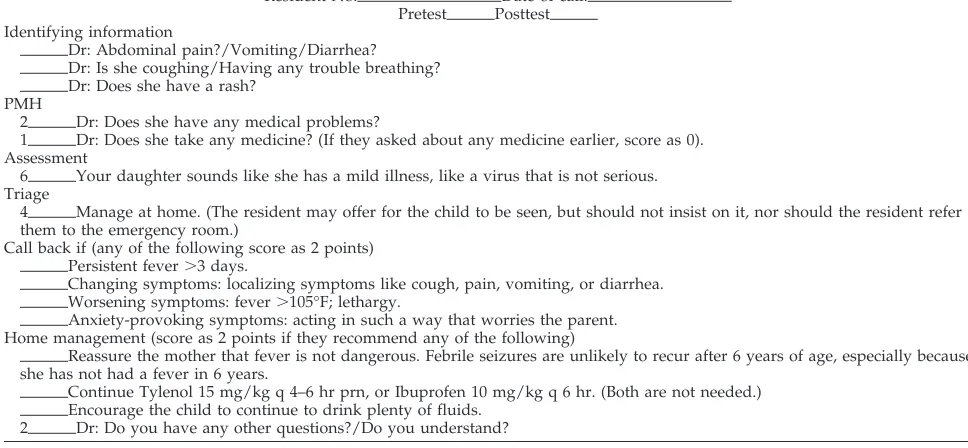
Both groups received the same two pre- and posttest telephone calls: a 5-year-old with cough and trouble breathing and a 7-year-old with fever. Calls were recorded and scored using standard templates (Table 2) and on interpersonal skills using the Patient Perception Questionnaire9(Table 3) by the standardized patient
who was blinded to the group assignment.
The standard scoring templates for the test cases were devel-oped from the consensus of a survey of 100 pediatricians in the Washington, DC area. Sixty percent of those surveyed responded.
TABLE 1. CD-ROM Telephone Scenarios 5-month-old with trouble breathing
Toddler with vomiting and diarrhea
3-week-old infant with persistent crying and a frustrated mother Anxious mother of a child with fever
Angry father of a 3-year-old with ear pain 6-year-old with abdominal pain
Child with a rash
2-year-old with an accidental ingestion Infant with head trauma
Adolescent with a sore throat
TABLE 2. Test Script: Cough in a 5-Year-Old Child
Resident No: Date of Call: Pretest Posttest Identifying information
2 Dr: Hello, this is Dr from Children’s. How can I help? M: My son is having trouble breathing.
2 Dr: What is your son’s name? 2 Dr: How old is he?
Open-ended question
2 Dr: What worries you most about the trouble breathing?/What kind of trouble breathing?/How much trouble breathing? Severity
Any questions about the severity of cough score as a total of 2 points. Dr: Does the cough wake him up?
Dr: Does the cough seem to be getting worse? Dr: What makes the cough worse?
2 Dr: Is he wheezing?/Making any noises/sounds with breathing? 2 Dr: Is he breathing fast?
2 Dr: Do his ribs suck in when he breaths (retractions)? 2 Dr: Is his nose running?/Nose congested?
Duration
2 Dr: How long has he been sick? Activity
2 Dr: Does he have a fever?
2 Dr: What is his activity level?/How is he acting?/Is he acting sick?/Is he home from school? 2 Dr: Is he drinking/eating OK?
Previous therapy
2 Dr: What have you tried at home? What have you given him?/Have you given him any medicine? Illness exposure
1 Dr: Has he been around anyone sick? ROS
2 Dr: Is anything else bothering him?/Any other symptoms?/Does anything hurt? PMH
2 Dr: Does he have any medical problems?/Has he had asthma/bronchitis/pneumonia?/Has he been sick like this before?/ Has he been healthy?
1 Dr: Is he taking any medicine? (score as 0 if already asked under Previous Therapy) 6 Assessment: It sounds like your son has a cold (URI, virus).
4 Triage: Manage at home. (The resident may offer for the child to be seen, but should not insist or send the patient to the emergency room.)
Call back if (score as 2 points total for this section if any of the following are asked): Persistent symptoms: the cough lasts.1 week.
Changing symptoms: he begins vomiting or running a fever.
Worsening symptoms: the cough is interfering with usual activity or he develops difficulty breathing. Anxiety provoking symptoms: there is something about the way he is acting that worries you. Home therapy (score 2 points total for this section if any of the following are recommended):
Vaporizer Increase fluids
Over-the-counter medicine containing dextromethorphan/pseudoephedrine at bedtime. Elevate head
Other
2 Any other questions? Do you understand?
7-Year-Old With Fever (Anxious Mother) Resident No: Date of call:
Pretest Posttest Identifying information
2 Dr: Hello, I’m Dr from CNMC. How can I help? M: My daughter has a fever.
2 Dr: What is your daughter’s name? 2 Dr: How old is she?
Open-ended question
2 Dr: What concerns/worries you most about her right now? Severity
2 Dr: How high is the fever? Duration
2 Dr: How long has she had a fever? Overall appearance
2 Dr: How is she acting now?/Is she acting normal?/What is her activity level?/Did she go to school? 2 Dr: Is she drinking/eating OK?
Previous therapy
2 Dr: What have you done/given her for the fever? Illness exposure
1 Dr: Has she been around anyone sick? ROS
2 Dr: Are there any other symptoms?
Score 1 for any of the following for a maximum score of 2 points Dr: Sore throat?
Pediatricians were presented with a chief complaint and age of the child and asked to rate a series of questions or recommendations as essential, helpful, or unnecessary.
The standardized caller had previous training as a standard-ized patient. She had an additional 10 hours of training for this study, memorizing the scripts, and in role-play sessions with the investigators to ensure that her answers were correct and consis-tent. Interrater reliability was established at .91 by one of the investigators who listened independently to tapes and scored recorded calls blinded to resident group assignment and to the standardized patient assessment.
RESULTS
Statistical analysis was performed using
x
2or the
Mann–Whitney test on Minitab statistical software
(Table 4).
The number of third year residents (PL-3) and the
pretest scores was similar. Posttest scores were
sta-tistically significantly higher in the computer group
than in the reading group on both calls. Some
post-test scores were lower than prepost-test scores in both
groups. All residents reviewed advice protocols with
nurses before pretest calls, and residents in the
read-ing group were provided copies of protocols as part
of their readings. Few residents in the reading group
and no residents in the computer group referred to
protocols when taking the posttest calls.
Interpersonal skills improved modestly in both
groups on the Patient Perception Questionnaire. The
computer group scored higher posttest, but the
dif-ference was not statistically significant.
In an anonymous written evaluation of the
tele-phone training, all of the residents rated the
experi-ence positively. All of the residents in the computer
group rated the program as helpful or very helpful.
A total of 73% of the reading group rated the
pro-gram helpful or very helpful, with the remainder
giving neutral ratings. Residents commented that the
computer program was “fun,” “good cases, pretty
typical,” “nonthreatening learning situation,” “it was
pretty close to being real,” “gave extra time to think,”
“pointed out important questions I should have
asked/advice I should have given,” “easy and fun,”
and “helped me organize my thoughts; very good
learning tool.” The primary criticism was that the
computer did not recognize all ways of phrasing a
question and did not have answers to all questions.
The primary criticism from residents in the reading
group was that they wanted to do the computer
cases.
DISCUSSION
Residents must learn telephone skills because
tele-phone management is an essential part of pediatric
practice. Although institutions such as our own have
implemented telephone advice programs staffed by
nurses using protocols, physicians are ultimately
re-sponsible. Many physicians in smaller communities
still answer the majority of calls, especially
after-hours. Senior residents have the knowledge and skill
necessary to correctly assess and manage most
pa-tients encountered in the clinic or emergency
depart-ment. However, they often fail to gather enough
pertinent information to assess and manage the same
complaints over the telephone. Lack of a consistent,
organized approach to telephone management has
been a problem identified in previous studies.
4,10 –13We emphasized teaching a consistent, general format
that could be applied to a variety of complaints.
Before the development of this computer program,
our residents had little formal training in telephone
management. Fosarelli found that program size and
manpower were predictive of whether pediatric
res-idency programs provided telephone training.
14Large residency programs were less likely to provide
telephone training, and reported instruction was
usually by lecturing. Although lecturing is an
inef-fectual means of teaching an interactive skill, it is the
method most commonly reported because it appears
to be an efficient way to deliver the content.
Increas-TABLE 2. Continued
7-Year-Old With Fever (Anxious Mother) Resident No: Date of call:
Pretest Posttest Identifying information
Dr: Abdominal pain?/Vomiting/Diarrhea? Dr: Is she coughing/Having any trouble breathing? Dr: Does she have a rash?
PMH
2 Dr: Does she have any medical problems?
1 Dr: Does she take any medicine? (If they asked about any medicine earlier, score as 0). Assessment
6 Your daughter sounds like she has a mild illness, like a virus that is not serious. Triage
4 Manage at home. (The resident may offer for the child to be seen, but should not insist on it, nor should the resident refer them to the emergency room.)
Call back if (any of the following score as 2 points) Persistent fever.3 days.
Changing symptoms: localizing symptoms like cough, pain, vomiting, or diarrhea. Worsening symptoms: fever.105°F; lethargy.
Anxiety-provoking symptoms: acting in such a way that worries the parent. Home management (score as 2 points if they recommend any of the following)
Reassure the mother that fever is not dangerous. Febrile seizures are unlikely to recur after 6 years of age, especially because she has not had a fever in 6 years.
Continue Tylenol 15 mg/kg q 4–6 hr prn, or Ibuprofen 10 mg/kg q 6 hr. (Both are not needed.) Encourage the child to continue to drink plenty of fluids.
ing demands on faculty to see more patients and
precept trainees in the clinic have limited the time
available to precept telephone calls.
Although interactive programs have been
devel-oped, there is only modest evidence that they are
more effective at teaching telephone management
than a traditional didactic approach. An innovative
program described by Kosower at UCLA called
T.A.L.K. taught telephone communication skills by
allowing residents to analyze recorded calls in group
and individual feedback sessions.
15Evans used
pa-tient simulators to teach telephone communication
skills to family practice residents.
16Although both
programs were well received by residents, neither
provided an objective evaluation of their
effective-ness at improving skills.
Several researchers did evaluate the effectiveness
of their programs using standardized patients. Curry
and Schwartz studied the effectiveness of a small
group discussion regarding important questions to
be asked for a complaint of vomiting and diarrhea
using five residents in the discussion group and five
in a control group.
17There was no statistical
differ-ence in posttest scores between the groups at either 6
days or 28 weeks. Wood found that role-play
ses-sions in which residents simulated parent callers
helped to improve some aspects of telephone
his-tory-taking in a controlled trial.
10Smith studied the
effect of feedback given to 12 medical students for a
single call on their performance on a subsequent call
using a standard scoring template. He found that
their proficiency improved significantly between the
first and second calls, but there was no control
group.
18We hypothesized that to become proficient at
tele-phone management, skill-modeling using an
orga-nized approach and guided practice was necessary.
19The computer program was modeled on previous
studies using standardized patients as simulated
callers.
20Use of standardized patients both as an
evaluation and a teaching tool has been well
docu-mented.
21,22Standardized patients offer several
ad-vantages to an educational program: 1) the learner
can be evaluated and/or provided feedback in a
controlled situation; 2) use of standardized patients
allows for more objective assessment because criteria
used to judge each learner’s performance can be
tailored and validated against preset standards; 3)
specific simulated encounters can be used that the
learner may not experience by chance during
train-ing or are of such a sensitive nature that it would be
unethical to allow an inexperienced learner to
inter-act with inter-actual patients/parents; 4) standardized
pa-tients can be instructed to provide feedback to the
learner in place of the faculty; 5) students’ and
resi-dents’ history-taking and physical skills can be
eval-uated better because they are assessed directly.
Although use of standardized patients encourages
active learning, it is a costly educational intervention
for a large residency program. Therefore we used the
computer to simulate a series of standardized
pa-tients. Computers have been used successfully to
teach assessment and management skills in other
areas of medical education.
23–26Using a CD-ROM
program, the computer can simulate a telephone call,
with the resident asking questions and receiving
an-swers without visual cues and responding not only
TABLE 3. Patient Perception Questionnaire
Poor Fair Good Very Good Excellent
Greeting you warmly: being friendly, crabby or rude
Treating you like you’re on the same level; never talking down to you or treating you like a child
Letting you tell your story, listening carefully, asking thoughtful questions, not
interrupting while you are talking Showing interest in you as a person; not
acting bored or ignoring what you have to say.
Encouraging you to ask questions, answering them clearly, never avoiding your questions or lecturing you.
Using words you can understand when explaining your problems; explaining any technical medical terms in plain language. Would you want this physician for your own
child’s doctor
Definitely no Probably no Maybe Probably yes Definitely yes
TABLE 4. Results
Reading Group Mean6SD
Computer Group Mean6SD
PValue
Total number 11 13
PL-2 residents 6 6 .68
PL-3 residents 5 7
Cough
Pretest 68.466.73% 70.3368.36% .55 Posttest 69.0613.3% 79.0868.17% .03 Change (Post–Pre) 0.6614% 8.569.9% .15 Fever
Pretest 73.5969.06% 75.6469.82% .45 Posttest 70.3569.66% 83.3369.96% .004 Change (Post–Pre) 24.1613.2% 7.7616.2% .046 Patient perception scale
Pretest 2062.7 1963.4 .77
Posttest 22.563.1 24.262.9 .41
to the content of the complaint, but also to the
emo-tional tone of the voice. The residents can participate
in self-directed guided practice sessions with the
computer to become proficient in the general
ap-proach to telephone management.
Use of this CD-ROM telephone management
pro-gram was associated with significantly higher
post-test scores on telephone calls placed by a
standard-ized patient in a randomstandard-ized, controlled trial. We feel
this program is most helpful in teaching a consistent,
general approach to telephone management,
includ-ing history-takinclud-ing, providinclud-ing an assessment, triage,
call back, and home-management advice. The
CD-ROM program augments, but does not replace,
fac-ulty involvement. Facfac-ulty can help residents to refine
interpersonal skills once residents have gained
knowledge and practice covering general content
areas.
The limitations of this study are the small sample
size and lack of long-term follow-up. To maintain
proficiency at any skill, continued practice and
feed-back are needed over time. We are currently working
to incorporate an integrated telephone management
experience that is not limited to 1 month, but is
ongoing throughout the residency program. In
addi-tion, although the program was very well received,
some residents in both groups scored lower on the
posttest than on the pretest calls. Unanticipated
achievement declines have been reported by
Swan-son and others on performance-based evaluations.
27Residents may have been more highly motivated to
perform well initially, because pretest calls were
taken while reviewing common protocols with the
advice nurse present; however posttest calls were
taken by residents unobserved and unaware of
which calls were recorded. Second- and third-year
residents in our program already were generally
pro-ficient at managing telephone calls, with pretest
scores of 68% to 75% of ideal. More significant gains
may have been seen if first-year residents
partici-pated.
The major costs in developing this program was
for faculty time to develop, record, score, and
pro-vide feedback for the cases, and for the computer
programmer to write the program. Based on the
success of this study, our goal is to share this
pro-gram with other institutions seeking to refine
resi-dent telephone management skills. We also plan to
make use of the computer case-based, interactive
format to develop self-directed learning modules
covering other areas of primary care pediatrics to
help our institution maintain its commitment to
teaching while facing conflicting demands on faculty
time attributable to changes in the health care
envi-ronment.
ACKNOWLEDGMENTS
This work was supported by Bayer Institute for Health Care Communication grants for the development and evaluation of this program.
We thank Ren Lan Loai and Dr Pincetl from the Computer Informatics Department at George Washington University for their help with program design. We also thank the nursing staff and pediatrics faculty at Holy Cross Hospital and Children’s National Medical Center who contributed to the CD-ROM devel-opment and evaluation.
REFERENCES
1. Bergman AB, Dassel SW, Wedgewood RJ. Time-motion study of prac-ticing pediatricians.Pediatrics.1966;38:254 –263
2. Hessel SJ, Haggery RJ. General pediatrics: a study of practice in the mid-1960’s.J Pediatr.1968;73:271–279
3. Wood PR. Pediatric resident training in telephone management: a sur-vey of training programs In the United States. Pediatrics. 1986;77: 822–925
4. Yanovski SZ, Yanovski JA, Malley JD, et al. Telephone triage by primary care physicians.Pediatrics.1992;89:701–706
5. Isaacman DJ, Verdile VP, Kohen FP, et al. Pediatric telephone advice in the emergency department: results of a mock scenario.Pediatrics.1992; 35–39
6. Poole SR, Schmitt BD, Carruth T, Peterson-Smith A, Slusarski M. After-hours telephone coverage: the application of an area-wide telephone triage and advice system for pediatric practices. Pediatrics.1993;92: 670 – 679
7. Milholland AV, Wheeler SG, Heleck JJ. Medical assessment by a Delphi group opinion technique.N Engl J Med.1973;288:1272–1275
8. Korsch BM, Gozzi EK, Francis F. Gaps in doctor-patient communica-tion.Pediatrics.1968;42:855– 871
9. Schnable GK, Hassard TH, Kopelow ML. The assessment of interper-sonal skills using standardized patients.Acad Med.1991;66:534 –536 10. Wood PR, Littlefield JH, Foulds DM. Telephone management curricula
for pediatric interns: a controlled trial.Pediatrics1989;83:925–930 11. Brown SB, Eberle BJ. Use of the telephone by pediatric house staff: a
technique for pediatrics care not taught.J Pediatr.1974;84:117–119 12. Perrin EC, Goodman HC. Telephone management in acute pediatric
illness.N Engl J Med.1978;298:130 –135
13. Greitzer L, Sapleton FB, Wright L, Wedgewood RJ. Telephone assess-ment of illness by practicing pediatricians.Pediatrics.1976;88:880 – 882 14. Fosarelli PD. The emphasis of telephone medicine in pediatric training
programs.Am J Dis Child.1985;138:555–557
15. Kosower E, Inkelis SH, Seidel JS. Telephone T. A. L. K.: a telephone communication program.Pediatr Emerg Care.1991;2:76 –79
16. Evans S, Curtis P. Using patient simulators to teach telephone commu-nication skills.J Med Educ.1983;58:894 – 898
17. Curry TA, Schwartz MW. Telephone assessment of illness: what is being taught and learned?Pediatrics.1978;62:603– 605
18. Smith RS, Fischer PM. Patient management by telephone: a training exercise for medical students.J Fam Pract.1980;10:463– 466
19. Kleflher JH.The Teaching Learning Process. San Antonio, TX: The Uni-versity of Texas Health Science Center at San Antonio; 1989:1–52 20. Dunn EV, Norton PG, Dunn RC. Using simulated patients to teach
family practice residents to manage patients by phone. J Med Educ.
1987;82:524 –526
21. Barrows HS. A review of the uses of standardized patients for teaching and evaluating clinical skills.Acad Med.1993;68:443– 451
22. Anderson MB, Stillman PL, Wang Y. Growing use of standardized patients in teaching and evaluation in medical education.Teach Learn Med.1994;6:15–22
23. Scheidt PC, Lightsey KH, McDaniel D, Labow JC. Evaluation of com-puterized simulations in a pediatric clerkship. Teach Learning Med.
1991;3:108 –111
24. Cohen PA, Dacanay LS. Computer-based instruction and health profes-sions education: a meta-analysis of outcomes.Eval Health Prof.1992;15: 259 –281
25. Lynn HC Jr, Healy JC, Bell JR, et al. Plan Alyzer, an interactive com-puter-assisted program to teach clinical problem solving in diagnosing anemia and coronary artery disease.Acad Med.1992;67:821– 888 26.Enhancing Medical Students Assessing Change in Medical Education. The
Road to Implementation (ACME-TRl Report).Acad Med.1993;68(suppl): S1– 46