Evaluating
the
Accuracy
of Transcribed
Computer-Stored
Immunization
Data
Richard Wilton, MD* and Alfred
J.
Pennisi, MDABSTRACT. Objective. To evaluate the accuracy of
immunization records transcribed into a computer-based
immunization tracking system and to assess factors that
contribute to inaccurate or incomplete immunization
record keeping.
Design. Computer-stored immunization records were
analyzed for 2098 children up to 2 years of age at the time
of their most recent well-child visit to the UCLA
Chil-dren’s Health Center over a 12-month period. For
chil-dren whose immunizations were not up to date, the
com-puter-stored records were analyzed for sources of
inaccuracy by comparison with the handwritten records
from which the computer-stored data were transcribed.
Results. An underimmunization rate of 22.5% (472 of
2098) was observed based on analysis of the
computer-stored records. Comparison of the computer-stored and
handwritten records revealed an overall transcription
er-ror rate of at least 10.2%. In addition, 38.4% of these
apparently underimmunized children had received
unre-corded immunizations from providers outside UCLA.
When transcription errors were corrected and other
avail-able sources of immunization data were taken into
account, the estimated rate of underimmunization
decreased from 22.5% to 10.9%.
Conclusion. Unavoidable inaccuracies can diminish
the utility of the data recorded in an immunization
track-ing system. Some inaccuracies are related to the process
of transcription, but failures to record and communicate
immunization data consistently also contribute to the
inaccuracy of computer-stored immunization records.
Pediatrics 199494:902-906; computer-based immunization
tracking system.
ABBREVIATIONS. UCLA, University of California Los Angeles;
DVT, diphtheria, pertussis, tetanus; TVOP, trivalent oral polio; MMR, measles, mumps, rubella.
A well-publicized goal of the United States Public
Health Service is to ensure that at least 90% of all
children have completed a basic set of
immuniza-tions by their second birthday.’ The data that
docu-ment achievement of that goal necessarily will be
obtained from comprehensive records of childhood
immunizations. The formidable problem of ensuring
the accuracy and completeness of each child’s
immu-nization record will probably be addressed by the
From the Division of General Pediatrics, University of California Los Angeles Department of Pediatrics, Los Angeles, California.
Received for publication Nov 16, 1993; accepted Apr 14, 1994.
Reprint requests to (RW.) UCLA Department of Pediatrics, 12-321 MDCC, Los Angeles, CA 90024-1752.
PEDIATRICS (ISSN 0031 4005). Copyright © 1994 by the American Acad-emy of Pediatrics.
widespread adoption of computer-based
immuniza-lion tracking systems.
Computer systems can be used for a variety of
purposes in clinical practice: for appointment
sched-uling, for accounting or billing, and for recording
clinical information about individual patients in the
form of an electronic medical record. When clinical
records for a number of patients are stored in a
computer database, it becomes possible to evaluate
clinical data for an entire population. A number of
assessments of the immunization status of pediatric
populations have been based on the analysis of
corn-puter-stored immunization data.25
The use of computer-stored clinical data to
deter-mine immunization status implies that the data are
sufficiently accurate and complete to draw reliable
conclusions about the population of patients
repre-sented in the aggregated data. In the process of
eval-uating immunization coverage in the pediatric
out-patient clinics at the University of California Los
Angeles (UCLA), we carried out a limited analysis of
transcription accuracy of a sample of our own
corn-puter-stored immunization records. Of the children
who were underimmunized according to
computer-stored records, 50% had inaccurately transcribed
records in the computer system.6
Based on this preliminary experience, we designed
a more comprehensive retrospective study in which
we analyzed the accuracy of immunization records
for a larger cohort of children who received
continu-ing care in the UCLA Children’s Health Center. The
analysis was designed specifically to describe the
sources of inaccuracy in transcribed,
computer-stored immunization data and to determine the
ex-tent to which inaccurate and incomplete data in
corn-puter-stored immunization records might affect our
ability to identify underimmunized children in our
clinic population.
METHODS
We analyzed the computer-stored clinical records of 8908 en-counters with 4040 patients seen in the outpatient clinics in the UCLA Children’s Health Center in the 12-month period from July 1992 through June 1993. The records covered patients seen in the UCLA housestaff continuity clinic as well as patients seen in the
general pediatric faculty clinics. The clinical records were cross-checked against computer-stored appointment scheduling and registration data (which record all outpatient encounters in the UCLA Children’s Health Center) to ensure that all visits with all patients in these clinics during the study period were included in the analysis.
at Viet Nam:AAP Sponsored on September 1, 2020
www.aappublications.org/news
Data Collection
Data-entry personnel transcribed immunization data after each clinic visit from two locations in the handwritten chart.
Immuni-zations given on the day of the visit were transcribed from a
structured encounter form on which the physician or pediatric nurse practitioner wrote the patient’s medical-management plan.
Transcribers also reviewed each chart’s immunization history form, which lists the dates of all of a child’s immunizations and which is updated after each visit by clinic nursing staff. Transcnb-em were nonmedical personnel who were instructed to transcribe only the date (month, day, and year) and type of each
immumza-tion into the computer system. Incomplete immunization data,
including immunizations without dates, and comments such as
“up to date,” were not transcribed. During the study period, seven different transcribers were responsible for entering immunization data into the computer system.
To improve data-entry speed and accuracy, all immunization
data were transcribed using software that displayed a simple
check-off menu and that allowed data entry using the computer keyboard or mouse. The software also allowed both menu-based and free-text transcription of other significant portions of the outpatient medical record, including problem lists, current medi-cations, and the salient diagnostic content of each clinic encoun-ter.7 The computer-stored records included the date of birth, race, sex, and insurance coverage of each patient, the name of each patient’s primary continuity physician, and dated records of each immunization given during that period.
Routine childhood immunizations were recorded as follows:
DPi’ (diphtheria, pertussis, tetanus), TVOP (trivalent oral polio),
and MMR (measles, mumps, rubella). Combinations of antigens
that were used infrequently, such as dT (diphtheria-tetanus) and IPV (inactivated polio vaccine), were also recorded. For purposes of analysis and for comparison to previous studies of immuniza-tion coverage, records of immunizations against other pathogens, including Haemophilus influenzae type b, influenza, and Pneumococ-cus, were not included in our study. Because the recommendation
for universal immunization against hepatitis B was adopted
dur-ing the study period, the data for these immunizations also were excluded from our analysis.
Data Analysis
We analyzed the immunization records in two phases. First, the computer-stored records were reviewed to identify children whose immunizations were delayed. Then the computer-stored
records were compared with the corresponding handwritten records in the outpatient chart.
Analysis of Computer-Stored Records
We first reconciled all computer-stored immunization records with computer-stored appointment scheduling records, to ensure
that immunization records were reviewed for all children who
had arrived for a clinic visit during the 12-month period studied. We then identified the subset of these children whose age was 732 days (2 years) or less at the time of their most recent clinic visit,
and who had fewer than the recommended number of
age-appro-pnate immunizations according to the computer-stored
immuni-zation records.
To categorize immunization status, we used the schedule of
age-appropriate immunizations that was in effect in the UCLA
Children’s Health Center during the study period. This schedule is
based on the recommendations of the American Academy of
Pediatrics8 and the Center for Disease Control’s Immunization
Practices Advisory Committee.9 The schedule recommended DPi’
immunization at 2, 4, 6, and 15 months; TVOP at 2, 4, and 15 months; and MMR at 12 months. We categorized each child’s immunization status as being up to date if the child had received DPi’, TVOP, and MMR immunizations according to the criteria listed in Table I.These criteria for immunization timeliness were
derived from the routine immunization schedule by adding a
30-day grace period to the age for each scheduled immunization. We determined each child’s primary provider of well-child care by using the appointment scheduling records to count the number
of well-child visits to UCLA Children’s Health Center. A UCLA
clinic was assumed to be the child’s primary provider if the child had had at least as many well-child visits in the clinic as would
have been necessary to administer all recommended
immuniza-TABLE 1.
Age Ranges Used to Determine Timeliness of Im-munizations*Age Numbe r of Immunizations
DVF P/OP MMR
1-91d(0-3mo) 0 0 0
92-151 d (3-5mo) I I 0
152-213 d (5-7mo) 2 2 0
214-395 d (7-13 mo) 3 2 0
396-487 d (13-16 mo) 3 2 1
488-732 d (16-24 mo) 4 3 1
* A child in one of these age ranges was considered up to date if he or she had received at least the corresponding number of each immunization. Abbreviations: DPi’, diphtheria, pertussis, tetanus;
p/op,
trivalent oral polio; MMR, measles, mumps, rubella.tions, according to the criteria in Table 1. We categorized a child’s primary-care provider as “unknown” if the child had not been seen in a UCLA clinic often enough to receive all recommended
immunizations.
Chart Review
For each child identified as being underimmunized based on computer-stored records, we reviewed the handwritten clinic chart for the following information: 1) transcription errors, i.e., if
the computer-stored list of dates and immunizations did not
match those in the handwritten immunization history in the chart; 2) immunization information written in the chart in a way that it could not have been transcribed, e.g., immunizations recorded without dates or recorded only as “up to date”; 3) records of immunizations received from providers other than the UCLA Children’s Health Center; 4) immunization data written in por-tions of the chart that were not transcribed routinely into the computer system, including inpatient discharge summaries, phy-sicians’ orders, and photocopies of medical records from non-UCLA health care providers; and 5) explicit indication that the child’s immunizations were delayed for any reason.
If a transcription error was noted or if additional immunization data were available in part of the chart that was not transcribed routinely, the child’s immunization status was reevaluated using the information written in the chart.
RESULTS
Analysis of Computer-Stored Records
Of the 4040 patients whose immunization records
were analyzed, 2098 were 2 years of age (732 days) or
younger at the time of their most recent well-child
visit. Analysis of the computer-stored immunization
records of these 2098 children revealed 472 (22.5%)
whose immunization status was not up-to-date for
age, according to the criteria in Table I. The
hand-written UCLA Medical Center charts were reviewed
for 458 of the 472 underimmunized patients. (The 14
charts not reviewed were unavailable from the
out-patient medical records department during the
4-week period during which the immunization
records were verified.)
The UCLA clinics were considered to be the
pri-mary provider of well-child care for 1869 (89.0%) of
the 2098 children less than 2 years of age, as
deter-mined by analysis of appointment scheduling
records (Table 2). Children for whom the UCLA
clinics were the primary provider of well-child care
had an underimmunization rate of 16.2% (303 of
1869); children whose primary provider was
un-known (that is, children not seen frequently enough
at UCLA to have received all recommended
immu-nizations) had an underimmunization rate of 70.7%
TABLE 2.
Immunization Status Related to Primary Provider of Well-Child CareContinuity Provider
Immunizations Up to Date
(n = 1626)
Immunizations
Not Up to
Date (n = 472)
Total (n = 2098)
UCLA clinics 1566 303 1869
Unknown* 60 169 229
* Children whose continuity provider is unknown were those who had too few visits to UCLA clinics to have received all recom-mended immunizations.
Chart Review
Of the 458 charts we reviewed for patients who
apparently were underimmunized, 244 were
tran-scribed accurately and completely from the
hand-written record into the computer system. In 214
records, at least one transcription error was noted.
The observed transcription error rate was thus at
least 10.2% (214 of 2098).
Immunizations Received From Non-UCLA Providers
Of the 458 records reviewed, 176 (38.4%) indicated
that the patient had received at least one
immuniza-tion from a provider other than the UCLA faculty or
residents’ continuity clinics.
Nontranscribed Immunization Data
Of the 458 charts reviewed, 72 (15.7%) contained
additional immunization information in locations
that were not transcribed routinely, including
en-counter notes, inpatient discharge summaries, and
photocopies of immunization records from
non-UCLA health care providers. An additional 87 charts
contained immunization data that could not be
tran-scribed: 37 (8.1%) noted that a child’s immunizations
were “up to date” but did not provide explicit dates
that could be recorded in the computer system, and
50 (10.9%) contained an explicit statement that
a patient was underimmunized. In 299 (65.3%) of
the charts, no additional immunization data were
recorded.
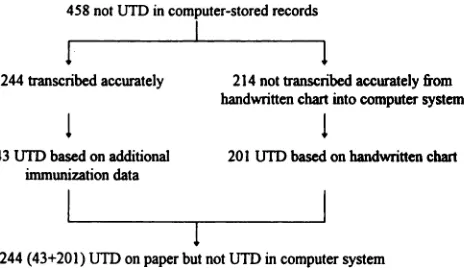
Reevaluation of Immunization Status
Immunization status was reevaluated using the
458 handwritten charts we reviewed, including the
214 charts revealing a transcription error in the
cor-responding computer-stored record and the 58
accu-rately transcribed charts that contained additional
458 not UTD in computer.stored records
‘I
244 transcribed accurately
43 UTD based on additional
immunization data
I
214 not transcribed accurately from
handwiitten chart into computer system
I
201 UTD based on handwritten chart
I
244 (43+201) UTD on paper but not UTD in computer system
Figure. Reevaluation of immunization status based on review of handwritten charts. UTD, up to date.
nontranscribed immunization data (Figure). Of these
458 charts, 244 were reevaluated as being up-to-date
based on data in the handwritten chart. When these
244 patients are recategorized, the perceived
under-immunization rate is 10.9% [(472 - 244)/2098] rather
than 22.5% as originally estimated.
DISCUSSION
In our experience, a computer-based
immuniza-tion tracking system is a practical repository for the
immunization records of individual patients, as well
as a ready resource for the aggregation of
inimuni-zation data for a clinic population. Nevertheless, the
accuracy of the immunization data is influenced by a
number of factors, including not only transcription
errors but also inconsistent or incomplete
immuni-zation record keeping on the part of doctors, nurses,
and parents.
Accuracy of Transcribed Immunization Records
We observed an underimmunization rate of 22.5%
(472 of 2098) in the cohort of children whose records
we analyzed during the 12-month study period. This
rate is comparable to underimmunization rates
ob-served previously in other urban populations.’#{176}
However, any interpretation of this
underimmuniza-tion rate must be qualified by analyzing the validity
of the underlying immunization data.
The observation that at least 10.2% of the
comput-er-stored immunization records were transcribed
in-accurately suggests caution in using the
computer-stored records to determine immunization rates.
Similar transcription error rates have been observed
in at least one other computer-based immunization
tracking system,” as well as in a pediatric
emergen-cy-department record-keeping system.12 In the case
of immunization records, such errors are
predomi-nantly errors of omission, so the true rate of complete
immunization is actually higher than the
computer-stored data indicate. As noted above, our estimated
underimmunization rate fell from 22.5% to 10.9%
when we took such errors into account.
Sources of Transcription Errors
In the present study, immunization data were
transcribed after each clinic visit from two
comple-mentary sources, the encounter form (a record of an
individual visit) and the immunization history form
(a cumulative record in the outpatient chart).
Al-though the present study did not differentiate
be-tween errors in transcribing the encounter forms
ver-sus the immunization history forms, both forms were
transcribed at the same time, so it is unlikely that
there would be a significant difference in the
tran-scription error rate between the two. Regardless of
the origin of the handwritten data, any
immuniza-tion tracking system that requires transcription of
written records wifi be susceptible to transcription-related errors.
This study was not designed to detect the false
entry of immunization data into the computer
sys-tern, that is, the recording of immunizations that
were not in fact given. However, the data-entry
soft-ware was designed so that immunization data could
at Viet Nam:AAP Sponsored on September 1, 2020
www.aappublications.org/news
be entered only by date (month, day, and year) and
by immunization type (selected from a check-off
menu on the computer screen). This software design
does not exclude errors stemming from the incorrect
entry of a date or of an immunization, but it
mini-mizes the possibility of inadvertently entering
im-munization data that are not available on paper. In
fact, of the 214 charts that contained transcription
errors, only two contained transposed immunization
data (e.g., a DPT immunization was recorded instead
of an MMR). All of the remaining errors were
errors of omission, whereby immunizations
writ-ten on paper were transcribed incompletely or not
at all.
Completeness of Computer-Stored Immunization
Records
Several factors influence the completeness of
corn-puter-stored immunization records. For example, we
observed that children with more frequent visits to
UCLA clinics had a much lower rate of
underimmu-nization than children who were seen less frequently
at UCLA (Table 2). However, these data are
con-founded by the fact that non-UCLA immunization
records were not transcribed routinely into the
corn-puter system.
The prevalence of such incomplete immunization
records decreases the utility of the data stored in the
computer system. In particular, it has been suggested
that computer-generated reminder letters to patients
can improve the rate at which parents bring their
children to a clinic to receive needed
immuniza-lions.’3 However, if such reminders are based on
incomplete or inaccurate immunization data, some
of the reminders will be sent to parents whose
chil-dren may actually be up to date. Movement of
pa-tients into and out of a primary-care practice also
may impair the effectiveness of any computer-based
reminder system.14 Because their computer-stored
immunization records are incomplete, children who
receive immunizations from multiple providers may
be mistakenly identified as underimmunized.
Interpreting Computer-Stored Immunization Data
We anticipate that the use of computer-stored
im-munization data will make it possible to estimate
immunization coverage in communities where such
information is difficult to obtain from paper records.
However, it is not easy to determine how well
corn-puter-stored data estimate true immunization rates.
As noted above, there are inherent inaccuracies in the
data resulting from the process of transcription.
Computer-stored immunization records also must be
interpreted cautiously because immunizations
pro-vided outside the scope of the immunization
track-ing system may not be recorded in the system, and
because it is difficult to ensure that immunization
records are transcribed completely from a
handwrit-ten medical chart. These problems complicate any
estimations of community-wide immunization
coy-erage based on computer-stored data.
Representativeness of Data
Because the UCLA Children’s Health Center is
only one of many pediatric health care providers in
the community, it is obvious that UCLA’s recorded
immunization data represent only a sample of the
community’s pediatric population. If we assume that
this sample is random, we compute that the
oh-served 22.5% underimmunization rate has a
stan-dard error of 3.8%. We thus estimate, based on our
sample of the community’s pediatric population, that
the underimmunization rate in the community has a
95% confidence interval from 18.7% to 26.3%.
However, our data almost certainly do not
repre-sent a truly random sample of the pediatric
popula-tion in the community served by UCLA. This is not
because there is an unusually high proportion of
high-risk or subspecialty patients in the UCLA
resi-dent and faculty clinic population.’5 Instead, our
computer-stored data may be unrepresentative
be-cause it is impossible to use the computer-stored
immunization records to determine the true
immu-nization status of children who are not always seen
at UCLA. Children with incomplete immunization
records at UCLA may in fact be fully immUnized
(when immunizations received from other providers
are recorded), underimmi.mized, or entirely
unim-mtinized. Other sources of immunization data, such
as interviews with parents or review of the written
records of immunization providers, must be
accumu-lated to sample the overall immunization coverage in
a community. Such data have been gathered in other
studies in the United States. However, the kinds of
inaccuracies we observed in our transcribed
immu-rnzation data also may exist in other providers’
im-munization data. Because of the scarcity of
cornput-er-stored immunization records in the United States,
published assessments of immunization rates
typi-cally have relied on sampling of handwritten records
in selected populations.’6”7 Although transcription
errors and other factors affecting the accuracy of
sampled immunization data have not been analyzed
systematically, there is no reason that inaccuracies
such as those observed in our computer-stored data
should not also exist in sampled handwritten data.
For example, school records remain an important
source of the data used to estimate immunization
coverage in preschool children,18 yet studies that rely
on school immunization records’#{176}”9 may be
particu-larly susceptible to transcription errors and other
inaccuracies, because school immunization records
are handwritten transcriptions of immunization data
recorded elsewhere.#{176}
Methodologic Considerations
Another barrier to consistent interpretation of
computer-stored immunization data is that there is
no consensus on how to define whether a child’s
immunizations are up to date or delayed.2’ A
num-ber of previous studies of immunization
cover-age’#{176}’17’19have counted a child’s immunizations as
being current if the child receives four DPT, three
plop,
and one MMR by age 2 years. However, thisuseful for evaluating immunization coverage in a
population of children of different ages. For example,
an unimmunized child who is 1 day short of his
second birthday would be considered to be up to
date using the “4:3:1” criterion.
We used a 30-day grace period after the
recom-mended age for each immunization to establish
im-munization coverage for each child at the age they
were last seen in the clinic. Although this method of
evaluating immunization timeliness makes it
practi-cal for assessing the immunization status of a child at
any age, the size of the grace period affects the
perceived immunization status of a significant
number of children. Had we used instead a 60-day
grace period, we would have identified only 408
rather than 472 children as being potentially behind
in immunizations.
Conclusions
There are unavoidable inaccuracies in
computer-stored immunization data. These inaccuracies stem
from several sources. Some result from errors
di-rectly related to the process of transcribing data
from a handwritten record into a computer system.
However, inaccuracies in computer-stored
immu-nization records also may arise from operational
factors unrelated to the mechanical process of
tran-scription.
ACKNOWLEDGMENTS
We thank George Chavez, Simona De La Torre, Ten
Hoff-man, Jennifer Moreda, Mishelle Sharp, Adam Singer, and Scott Welford for their diligent data-entry efforts; Mary Ellen Curry and the outpatient medical records staff in the UCLA Medical Plaza; and Peter Christenson, PhD, for statistical review of the data.
REFERENCES
1. Public Health Service. Healthy People 2000: NationalHealth Promotion and Disease Prevention Objectives. DHHS publication no. (PHS)91-50213. Washington, DC: US Department of Health and Human Services, Public Health Service; 1991
2. Li J,Taylor B. Factors affecting uptake of measles, mumps, and rubella immunization. BMJ. 1993307:168-171
3. Scrivens E. Management information in the National Health Service: the
use of the child-health computer system. Community Medicine. 1984;6:
299-305
4. Alberman E, Watson E,Mitchell P, Day S. The development of perfor-mance and cost indicators for preschool immunization. Arch Dis Child.
1986;61:251-256
5. Hodes Di’, Timms SL, Gill ON. A successful measles campaign as a model for achieving high uptakes of MMR. PublicHealth. 1990;104:27-31
6. Wilton R, Pennisi AJ. Evaluating the accuracy of transcribed dinical data. In: Proceedings of the 17th Annual Symposium on Computer Applica-lions in Medical Care. New Yoric McGraw Hill; 199&279-283
7. Wilton R, McCoy JM. An outpatient clinic information system based on distributed database technology. In: Proceedings of the 13th Annual Sym-posium on Computer Applications in Medical Care. Washington, DC: IEEE Computer Society; 1989:372-376
8. American Academy of Pediatrics. Report of the Committee on Infections Diseases. Elk Grove Village, IL: American Academy ofPediatrics; 1991
9. Centers for Disease ControL Recommendations of the Immunization Practices Advisory Commiftee: general recommendations on immuni-ration. MMWR. 198938:205-228
10. Afford D, Kelly J, Nickey L, Crider R, Arrandondo J,Simpson DM, Kimbler A. Retrospective assessment of vaccination coverage among school-aged children-selected U.S. cities, 1991. MMWR. 1992;41:
103-107
11. Payne 1, Kanvik S, Seward R, Beeman D, et aL Development and
validation of an immunization tracking system in a large health main-tenance organization. Am IPrey Med. 1993996-100
12. Chan IS, Schonfeld N. How much information is lost during process-ing? A case study of pediatric emergency department records. Comput BiOmed Res. 199326:582-591
13. Kemper KJ, Goldberg H. Do computer-generated reminder letters Ira-prove the rate of influenza immunization in an urban pediatric clinic? Am JDis Child. 1993;147:718-719
14. Moran WP, Nelson K, WoffordJL, Velez R. Computer-generated mailed reminders for influenza immunization: a clinical trial. I Gen Intern Med.
1992;7:535-537
15. Wilton R, Pennisi AJ. Insurance coverage and residents’ experience in a pediatric teaching clinic. Am IDis Child. 1993;147:284-289
16. HymelTJ, ShermanJ, Pope SK, Kelleher KJ. Inadequate immunizations: identification using dinic charts. Clin Pediatr. 199332:156-160
17. Bobo JK, Gale JL, Purushoftam BT, Wassilak SGF. Risk factors for delayed immunization in a random sample of 1163 children from Oregon and Washington. Pediatrics. 199391:308-314
18. Orenstein WA. A comprehensive immunization registry. [Transcript of presentation at the 1993 Annual Meeting of the American Academy of Pediatrics.J The SCOT Repert. December 1993;16-18 (Newsletter) 19. Behrens E, Libby J,Borden G, Safranek T. Early ChildhOOd vaccination
in two rural counties-Nebraska, 1991-1992. MMWR. 1992;41:688-691
20. Herold AH, Roetzheim RG, Woodard U, Pamies RJ, Van Durme DJ,
Manning R. Validity of immunization documentation presented to a student health program. IFam Pract. 199336:158-IW
21. Varrasso DA, Redlener LDefining delayed immunizations Eletterl.
Pc-diatr Infect Dis J.1992;11:897
at Viet Nam:AAP Sponsored on September 1, 2020
www.aappublications.org/news
1994;94;902
Pediatrics
Richard Wilton and Alfred J. Pennisi
Evaluating the Accuracy of Transcribed Computer-Stored Immunization Data
Services
Updated Information &
http://pediatrics.aappublications.org/content/94/6/902
including high resolution figures, can be found at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or in its
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
at Viet Nam:AAP Sponsored on September 1, 2020
www.aappublications.org/news
1994;94;902
Pediatrics
Richard Wilton and Alfred J. Pennisi
Evaluating the Accuracy of Transcribed Computer-Stored Immunization Data
http://pediatrics.aappublications.org/content/94/6/902
the World Wide Web at:
The online version of this article, along with updated information and services, is located on
American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 1994 by the
been published continuously since 1948. Pediatrics is owned, published, and trademarked by the
Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it has
at Viet Nam:AAP Sponsored on September 1, 2020
www.aappublications.org/news