Saline Infusion Sonohysterography
Technique, Indications, and Imaging Findings
Debra L. Berridge, MD, Thomas C. Winter, MD
Objective.To review the technique, indications, and common imaging findings regarding saline infusion sonohysterography. Methods. The literature on saline infusion sonohysterography was reviewed. Pertinent images from our institution are presented to illustrate common imaging findings. Results.From the literature review, we summarize the various clinical scenarios in which saline infu-sion sonohysterography is useful and give examples from our clinical practice. Conclusions.Saline infusion sonohysterography is a useful procedure for evaluation of endometrial and subendometrial abnormalities. Key words:endometrium; saline infusion sonohysterography; sonography.
Received July 1, 2003, from the Department of Radiology, Abdominal Imaging, University of Wisconsin Hospitals and Clinics, Madison, Wisconsin USA. Revision requested July 22, 2003. Revised manuscript accepted for publication August 20, 2003.
Address correspondence and reprint requests to Thomas C. Winter, MD, Department of Radiology, University of Wisconsin, E3/311 CSC Box 3252, 600 Highland Ave, Madison, WI 53792 USA.
Abbreviations
HSG, hysterosalpingography; MRI, magnetic resonance imaging; PMB, postmenopausal bleeding; SIS, saline infusion sonohysterography; 3D, 3-dimensional; TVS, transvaginal sonography
aline infusion sonohysterography (SIS) is a tech-nique in which a catheter is placed into the endometrial cavity and sterile saline is instilled to separate the walls of the endometrium. In 1993, a study by Parson and Lense1 in the Journal of Clinical
Ultrasound termed the technique sonohysterography. This technique has been known by many names, includ-ing sonohysterography, hysterosonography, transvaginal sonography (TVS) with fluid contrast augmentation,2
and, finally, SIS.3
This article is a review of the literature on SIS since its introduction and a guide for sonographers and sonolo-gists who are not yet familiar with this technique. We out-line the various settings in which SIS is useful and give a detailed description of the technique itself. In addition, we outline the most common imaging findings on SIS. Technique
Saline infusion sonohysterography is a technique that involves placing a catheter into the uterine cavity through the cervical os to inject sterile saline into the endometrial canal. The saline distends the cavity, pushing the opposed walls of the endometrium apart. The anechoic fluid is then juxtaposed against the echogenic endometrium, giv-ing exquisite detail of the uterine lingiv-ing.
Because there is considerable variation in the thickness of the endometrium in menstruating woman, SIS is best performed as soon as possible after the cessation of menses, during the proliferative phase of the menstrual
S
cycle, no later than day 10.4This is before
ovula-tion because pregnancy is a contraindicaovula-tion to SIS. During days 4 to 6 of the menstrual cycle, the endometrium is at its thinnest. When the endometrium is thinnest, focal lesions such as polyps are best seen. In general, the secretory phase is avoided because of false-positive findings from folds and wrinkles in the lining.1In the
post-menopausal woman with abnormal bleeding, the examination can be performed at any time. If she is receiving hormone replacement therapy, then the study should be coordinated with withdrawal bleeding or the progesterone phase of the hor-mone replacement therapy. Bleeding is not a con-traindication to SIS; however, the presence of blood clots within the endometrial canal can make interpretation more difficult.4
Patient preparation for the examination is mini-mal. We instruct our patients to take ibuprofen orally 1 hour before the examination time. We do not routinely give prophylactic antibiotics. However, patients with active pelvic inflammatory disease are not studied with SIS because of con-cerns about potentially exacerbating the infection. Similarly, although it is rarely an issue, and although there are no hard scientific data to sup-port this stance, we do not perform SIS on patients with an intrauterine device in place. Initially, the patient undergoes routine TVS with full evaluation of the uterus, endometrial stripe, and adnexa. The procedure is explained to the patient, including the small risk of increased bleeding as well as the even smaller risk of infection. Complications are fairly uncommon with SIS. In an article by Bonnamy et al,5the rate was 1% for serious
com-plications (a single case of endometritis). Pelvic pain was also cited as a complication, with a rate of 1%. Consent is obtained after the patient’s ques-tions have been answered.
The equipment needed for the examination includes a sterile speculum with an open side, cervical sounds in the event that the catheter does not pass easily through the cervix, a 20-mL syringe, a tenaculum, clamps, and the hys-terosonography catheter with a 3-mL syringe for the balloon (Figure 1). A tenaculum is included on the SIS tray but is rarely used in our practice. If the tenaculum is used, it is traditionally placed on the anterior lip of the cervix, although it can also be used on the posterior lip. There are sever-al different catheters available for SIS.6We prefer
to use a balloon occlusive catheter to ensure that the endometrial canal is well distended. We
cur-rently use an H/S hysterosalpingography (HSG) catheter (Medi-Tech, Gainesville, FL). The catheter has an outer stiffener to facilitate intro-duction of the flexible catheter into the cervix. The catheter and the balloon must be flushed with sterile saline before insertion to remove as much air as possible. Any air within the catheter will be introduced into the endometrial canal and may obscure abnormalities during scanning (Figure 2).
The patient is placed in the lithotomy position. A brief bimanual examination can aid in locating the cervix. A sterile speculum is placed into the vagina, and the cervix is brought into view. The cervix is then cleansed with povidone-iodine solution. The catheter and stiffener are placed at
Figure 1.Typical tray set for SIS. Equipment needed includes a speculum, various clamps, a tenaculum, cervical dilators, the sonohysterography catheter, a syringe for the occlusive balloon, and a 20-mL syringe for injection of the saline.
Figure 2.Inadvertent injection of a small amount of air. The air appears as a bright echogenic focus in the fundal region of the endometrial cavity (arrow).
the external cervical os, and the catheter is advanced through the stiffener into the endome-trial canal. Cervical stenosis can make passage of the catheter difficult. In a study by Goldstein et al,7 2 of 153 SIS examinations were technically
inadequate. Once into the endometrial canal, the balloon is inflated so that the catheter does not become dislodged. The speculum is carefully removed, and the endovaginal probe is reinserted beside the catheter.
Under direct sonographic visualization, the bal-loon is gently retracted to occlude the internal cervical os. Again, under sonographic guidance, approximately 5 to 30 mL of warm sterile saline is injected. The saline is warmed in a microwave oven for the patient’s comfort and to decrease cramping. We use a 1200-W microwave oven, heating a 500 mL bottle of sterile saline for 55
sec-onds, but each sonologist should always verify this technique to ensure an optimal and safe fluid temperature. Complete sonographic evaluation of the endometrial cavity is performed in both the coronal and sagittal planes. In addition, 3-dimensional (3D) imaging has been advocated to get a better global view of the uterine cavity.8The
balloon is then deflated, and evaluation of the lower uterine segment and endocervical region is performed. Doppler evaluation can be quite helpful for distinguishing blood clots from poly-poid lesions.9 If color flow can be documented
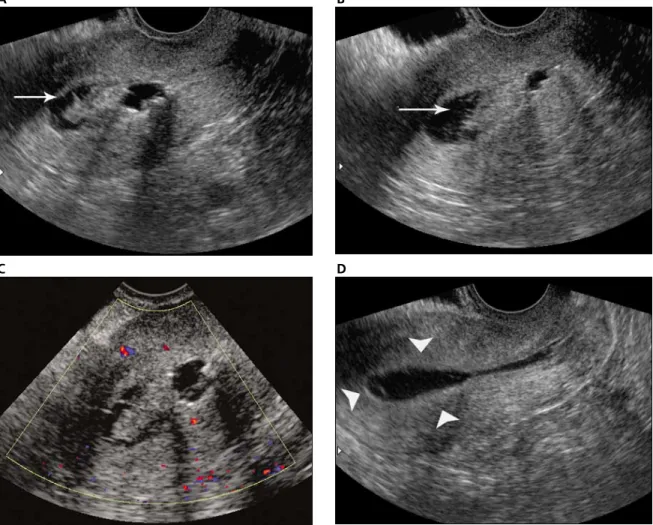
within the lesion, then a blood clot is excluded. In addition, the catheter itself can be manipulated to dislodge the blood clot during the course of the examination (Figure 3). The catheter is then removed. In general, patients tolerate the proce-dure quite well.
Berridge and Winter
Figure 3.Blood clot mimicking a mass. The patient had postmenopausal bleeding. Initial images (Aand B) show an echogenic mass in the endometrial cavity (arrow). Color Doppler imaging (C) shows no color flow within the mass. During the examination, the mass was dislodged with the catheter, and the final image (D) shows a normal thin endometrium (arrowheads).
B A
D C
Indications
Fertility Workup
Uterine anomalies are common in women with infertility and recurrent pregnancy loss. Therefore, it is essential that fertility workups include an eval-uation for structural uterine abnormalities. Saline infusion sonohysterography as an adjunct to TVS can give additional information regarding struc-tural uterine abnormalities.
Congenital Anomalies
Because of the high incidence of congenital uter-ine anomalies among patients with recurrent pregnancy loss, Alborzi et al10performed a study
to evaluate the effectiveness of SIS in differentiat-ing a septate uterus from a bicornuate uterus. In their study, SIS was able to differentiate a septate uterus from a bicornuate uterus in all cases. These authors found that this technique could obviate the need for laparoscopy for diagnosis of these conditions. The importance of the diagno-sis is that patients with a bicornuate uterus must undergo abdominal metroplasty, whereas this procedure has been replaced by hysteroscopic metroplasty in patients with a septate uterus.
Soares et al11evaluated SIS, TVS, and HSG with
regard to uterine malformations. These modali-ties were compared with hysteroscopy. Saline infusion sonohysterography had the highest sen-sitivity and specificity, 77.8% and 100%, respec-tively. Transvaginal sonography and HSG both had a sensitivity of 44%. Hysterosalpingography also had false-positive results, which were not observed with SIS. However, SIS and TVS did not detect 2 of 3 cases of unicornuate uterus.
Masses and Adhesions
Soares et al11compared the diagnostic accuracies
of SIS, TVS, and HSG with hysteroscopy in infer-tile patients. For polypoid lesions and endome-trial hyperplasia, SIS had a sensitivity and specificity of 100%. For polypoid lesions, the sen-sitivity of HSG was 50%, and the specificity was 82.5%. Because endometrial hyperplasia causes diffuse uniform endometrial thickening, HSG did not detect any of these cases.
Saline infusion sonohysterography and HSG had similar results in detecting intrauterine adhesions (Figure 4). Both methods had a sensi-tivity of 75%, and the specificity was 93% and 95%, respectively. In contrast, TVS did not detect any of the cases of intrauterine adhesions.
These authors concluded that SIS is superior to TVS and HSG for polypoid lesions and endome-trial hyperplasia and outperformed both TVS and HSG in the detection of uterine anomalies.
Screening Before In Vitro Fertilization
Patients undergoing in vitro fertilization are gen-erally screened with office hysteroscopy for eval-uation of intrauterine abnormalities. Screening with SIS yields similar diagnostic results but is less invasive, better tolerated, and less costly. In addition, SIS yields more information regarding the size and locations of myomas. At the same setting, the adnexa can be evaluated. Saline infu-sion sonohysterography can also differentiate a septate uterus from a bicornuate uterus. For these reasons, some authors are recommending screening with SIS before in vitro fertilization.12
Recurrent Pregnancy Loss
In patients with recurrent pregnancy loss, there is a high incidence of uterine abnormalities. In a study by Keltz et al,1317 of 34 patients with
recur-rent pregnancy loss (defined as 3 consecutive losses) had an intrauterine abnormality identi-fied on SIS. In their study, SIS had a sensitivity and specificity of 100% for demonstration of these intrauterine abnormalities. In contrast, HSG had a sensitivity of 90% but a specificity of 20%. In addition, HSG had a false-positive rate of 31%. The authors concluded that, because of the excellent sensitivity and specificity afforded by SIS, it could replace HSG as the test of choice for evaluation of intrauterine abnormalities in this setting.
Saline infusion sonohysterography can be a valuable test in the evaluation of female infertili-ty. It gives excellent anatomic detail of the uterus and has been shown to be highly accurate in the diagnosis of polypoid lesions, endometrial hyperplasia, and various uterine anomalies. It offers several advantages over the traditional HSG. It uses no ionizing radiation and no iodi-nated contrast agent. The entire uterus is visual-ized rather than the outline of the endometrial canal. It is well tolerated by the patient and has few complications. In the studies by Keltz et al13
and Soares et al11(in fertility evaluation
popu-lations), there was 1 complication of infection in each study, for a total of 2 infections per 99 patients. The infection in 1 patient resolved with oral antibiotics, whereas that in the other required hospitalization.
Saline infusion sonohysterography can be very helpful in directing subsequent intervention. If a focal lesion is identified on SIS, that lesion can be treated with hysteroscopy. Those patients who do not have a focal lesion can be spared hys-teroscopy in many cases. In addition, those patients found to have a septate uterus rather than a bicornuate uterus can undergo hystero-scopic metroplasty, whereas those patients with a bicornuate uterus must undergo abdominal metroplasty.
Postmenopausal Bleeding
Postmenopausal bleeding (PMB) was defined in a Society of Radiologists in Ultrasound consen-sus statement as “any vaginal bleeding in the postmenopausal woman other than expected cyclic bleeding that occurs with sequential hor-mone replacement therapy.”3 Postmenopausal
bleeding is a common clinical problem. As many as 1 per 10 women older than 55 years have abnormal vaginal bleeding. Postmenopausal bleeding can occur secondary to many condi-tions, including atrophy, endometrial polyps, and endometrial hyperplasia; however, the clini-cal workup is generally performed to exclude endometrial cancer.
Transvaginal sonography is a very sensitive means of evaluating the endometrium. Several studies have evaluated the role of TVS in the eval-uation of the endometrium.14,15Smith-Bindman
et al15 reviewed the literature on endovaginal
sonography and the measurement of endome-trial thickness. The study included 35 previous studies in which prospective endometrial
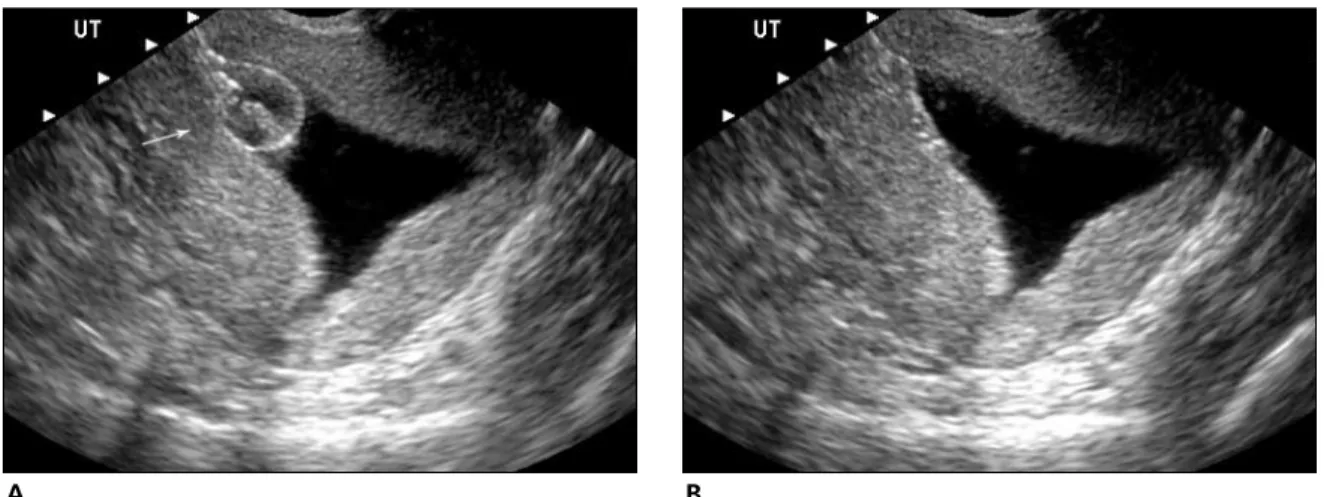
mea-surements were collected before histologic eval-uation. The meta-analysis included 5892 women. Using a double-wall thickness of 5 mm, the sensitivity for detecting endometrial cancer was 96% regardless of whether the woman was receiving hormone replacement therapy. A thin endometrium of 5 mm or less had a high nega-tive predicnega-tive value, and this finding would support the diagnosis of atrophy (Figure 5). If fluid is seen within the endometrial cavity on the initial transvaginal scan, the individual wall thicknesses of the 2 sides of the endometrium are summed, excluding the intervening fluid.
The clinical workup of PMB usually begins with either TVS or endometrial biopsy in the office. Endometrial biopsy in the office is performed as a blind technique and as such has inherent lim-itations, particularly in the evaluation of focal lesions. In a study by Guido et al,1611 of 65
can-cers were missed with blind sampling. In all 11 cases, the abnormalities involved less than 50% of the endometrium. These authors stated that the Pipelle curette is “excellent for detecting endometrial processes when the pathology is global in nature.”16When a focal lesion is
detect-ed, a visually directed biopsy is indicated. When the endometrium is found to be thick-ened, inhomogeneous, or indistinct (poorly visualized) on TVS, further evaluation with SIS can provide additional information. Saline infu-sion sonohysterography can determine whether the abnormality is focal or diffuse and thus can direct the next appropriate step in the patient’s workup. The patient can then proceed to hys-teroscopy or blind endometrial biopsy on the
Berridge and Winter
Figure 4. Intrauterine adhesions in a 33-year-old woman undergoing a fertility workup with a history of 2 dilation and curettage pro-cedures. Saline infusion sonohysterography shows a poorly distensible endometrial cavity with adhesions (arrows). A, Longitudinal image; B, transverse image.
basis of the results of the sonohysterogram.17In
addition, this information can be used to obviate the need for additional biopsy in a patient in whom inadequate tissue was obtained on office endometrial sampling.18,19
Endometrial Polyps
Endometrial polyps are common causes of abnor-mal vaginal bleeding in both premenopausal and postmenopausal women. In postmenopausal women, polyps are found to be the cause of bleed-ing in approximately 30% of cases. Most of these polyps are benign. The incidence of malignancy in polyps ranges from 0.5% to 1.5%.20Polyps are
usu-ally resected for both histologic evaluation and symptomatic relief of bleeding.
On TVS most endometrial polyps are echogenic with respect to the myometrium and are homo-geneous in echo texture (Figure 6).21Cystic
com-ponents can be seen in benign polyps and may indicate hemorrhage, infarction, or inflamma-tion.22 Other causes for cysts include dilated
glands or mucinous metaplasia, particularly in those polyps associated with tamoxifen use. Transvaginal sonography cannot distinguish endometrial hyperplasia from benign polyps because both conditions can cause thickening of the endometrium, are hyperechoic, and can con-tain cystic spaces.22
Saline infusion sonohysterography can distin-guish focal lesions from diffuse endometrial thickening. Polyps are focal lesions, which pro-ject into the lumen of the endometrial cavity (Figure 7). The anechoic saline outlines the
echogenic mass. Polyps are generally uniform in echo texture, and often a stalk can be identified. With color Doppler sonography, a feeding vessel can frequently be shown within the stalk.9,23
There has been interest in identifying charac-teristics that would predict which polyps are benign and which polyps contain foci of atypia. In a recent study, Goldstein et al24 used color
Doppler sonography to evaluate 61 patients with endometrial polyps. Both the resistive index and the pulsatility index were measured in vessels within polyps, and no statistical difference was found between the benign polyps and those taining malignancy. The sample, however, con-tained only 3 malignant polyps.
Perez-Medina et al25 examined a total of 806
patients with endometrial polyps. They mea-sured the resistive index of all polyps that showed color flow. They had a total of 38 atypical polyps in their series, 12 of which contained adenocarci-noma. Using a resistive index of less than 0.50, they identified 35 of the 38 polyps. They also clas-sified 16 polyps as atypical, which at pathologic examination were benign, from a total of 768 benign polyps. These results yielded a sensitivity of 92.1% and a specificity of 97.9%. These were promising initial results; however, because most polyps are resected to relieve symptoms, these findings may be of limited clinical importance.
Again, once a focal abnormality such as a polyp is identified on SIS, visually directed biopsy is suggested for accurate sampling of the abnor-mality. Resection of a polyp or polyps generally resolves the abnormal uterine bleeding.
Figure 5.Normal saline infusion sonohysterogram. The endometrial cavity is well distended, and the endometrial lining is thin, delicate, and uniform in echo texture. Images were obtained before (A) and after (B) balloon deflation. The arrow indicates the SIS balloon.
Leiomyoma
Uterine leiomyomas, or fibroids, are benign tumors of the smooth muscle. They are extreme-ly common, although onextreme-ly a small number are symptomatic.26,27 When they are symptomatic,
the most common symptom is abnormal vaginal bleeding.26 Fibroids are classified by their
loca-tion within the uterus: submucosal, intramural, or subserosal. Submucosal fibroids are the most likely to cause abnormal bleeding. Saline infusion sonohysterography can establish the location of the fibroid with respect to the endometrial lining. Fibroids appear as hypoechoic masses in con-trast to endometrial polyps, which are usually hyperechoic with respect to the myometrium. In addition, the echogenic endometrium can be
seen draping over the fibroid (Figure 8). However, the endometrium may not be seen if the fibroid has eroded through the endometrial lining.28The position of the fibroid within the
endometrial canal cannot reliably be used as a distinguishing factor between polyps and fibroids because fibroids can be contained almost entirely within the endometrial cavity and thus may appear polypoid. The most reliable feature is the echogenicity of the mass. As stated earlier, polyps are echogenic, whereas fibroids typically appear hypoechoic (although their echogenicity can be quite variable) and may pro-duce shadowing as well (Figure 9). Recurrent refractive shadowing is reported to be a particu-larly useful sign for uterine leiomyomas.29
Berridge and Winter
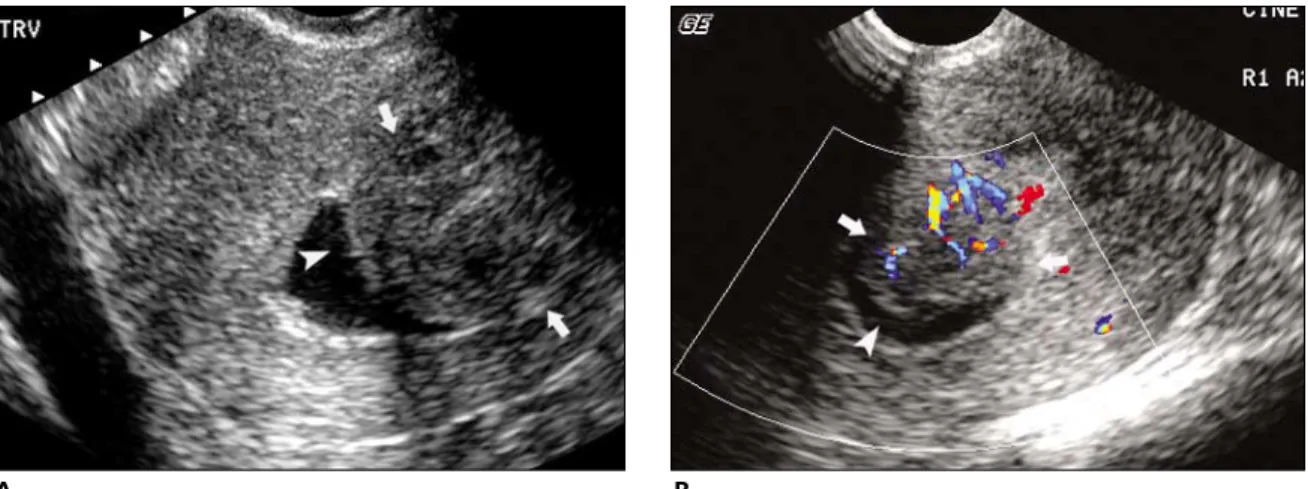
Figure 6. Postmenopausal bleeding in a 55-year-old woman. Saline infusion sonohysterography shows a polypoid mass. The mass (arrow) was resected and was a benign endometrial polyp. A, Gray scale image; B, color Doppler image.
A B
Figure 7. Multiple polyps in a 52-year-old woman with abnormal bleeding. Saline infusion sonohysterography shows multiple poly-poid masses (arrows) outlined by the anechoic saline. A, Longitudinal image; B, transverse image.
The extent to which the fibroid projects into the lumen of the endometrial cavity is of clinical importance. If the fibroid projects into the lumen by more than 50% of its surface, then it can be resected by hysteroscopy, obviating an abdomi-nal surgical procedure (Figure 10).30
Endometrial Hyperplasia
Endometrial hyperplasia is the cause of PMB in approximately 4% to 8% of cases.9,31
Endo-metrial hyperplasia is the result of unopposed estrogen stimulation of the endometrium. Although sonography cannot differentiate among the various types of endometrial hyper-plasia, they are histologically categorized as sim-ple, complex, or atypical. Simple hyperplasia consists of architectural distortion of the glands with alteration of the gland size and irregularity in gland shape with cyst formation.32 Simple
hyperplasia (Figure 11) rarely progresses to endometrial carcinoma. Complex hyperplasia (Figure 12) produces an increase in the size and number of glands with crowding and an irregu-lar shape. If there is no atypia, there is a less than 5% chance of progression to carcinoma. Simple and complex hyperplasia refer to alterations in architecture, whereas atypical hyperplasia refers to cellular atypia. With atypical hyperplasia, there is an approximately 23% chance of pro-gression to endometrial carcinoma.33
Endometrial hyperplasia causes thickening of the endometrial stripe, which can be detected on TVS. Transvaginal sonography usually can-not distinguish whether the thickening is due to a diffuse process or a focal lesion. With SIS, endometrial hyperplasia typically appears as diffuse thickening of the endometrium, al-though it can occasionally appear as a focal area of endometrial thickening.30In a study by
Jorizzo et al34on endometrial hyperplasia, cysts
were seen in 57% of patients, and concomitant endometrial polyps were found in 26% of patients.
As stated previously, TVS and SIS cannot dis-tinguish the different types of hyperplasia. In addition, the thickening of the endometrium that occurs in the secretory and late proliferative phases of the menstrual cycle cannot be distin-guished from the diffuse thickening of endome-trial hyperplasia (Figure 13). In a study by Dubinsky et al35of 28 women with diffuse
thick-ening of the endometrium, all 28 had either a secretory or proliferative endometrium at biopsy.
Figure 8. Saline infusion sonohysterography and MRI of the pelvis show both a submucosal fibroid (arrow) and an endome-trial polyp (arrowhead). A, Gray scale SIS image; B, color Doppler SIS image; C, MRI.
A
B
Hence, this underscores the importance of the timing of SIS in menstruating women; the proce-dure should be performed as early as possible after the cessation of menses, ideally on days 4 to 6 of the menstrual cycle.
Endometrial Carcinoma
Endometrial carcinoma is the fourth most com-mon cancer acom-mong women in the United States. Postmenopausal bleeding is the most common presenting symptom in women with endometrial carcinoma, but only 10% to 20% of women with postmenopausal bleeding will have cancer. Similar to endometrial hyperpla-sia, endometrial carcinoma is caused by unop-posed estrogen. Obesity is considered a major
risk factor, with a 3-fold increased risk if the woman is overweight by 22.7 kg and a 9-fold increase in risk if she is overweight by greater than 22.7 kg.36The risk in overweight women is
secondary to increased estrogen production and bioavailability.37,38 Other risk factors
include nulliparity, early menarche, late menopause, hypertension, diabetes, and poly-cystic ovary syndrome. In the postmenopausal woman, the most important risk factor is age. A woman older than 70 years has a 6- to 10-fold increased risk for development of endometrial cancer when compared with younger women.39
Eighty-five percent of endometrial cancers are adenocarcinomas. They are associated with endometrial hyperplasia and are referred to as
Berridge and Winter
Figure 9. Submucosal fibroid in a 54-year-old woman with postmenopausal bleeding. Saline infusion sonohysterography shows a hypoechoic mass (arrows) with an echogenic endometrium (arrowhead) draped over it. This is the typical appearance of a submucosal fibroid. A, Gray scale image; B, color Doppler image.
A B
Figure 10. Two SIS images (Aand B) show multiple fibroids projecting into the endometrial cavity (arrows). If more than 50% of the fibroid’s surface projects into the endometrial cavity, it can be resected hysteroscopically.
endometrioid. They tend to be well differentiated and have more favorable prognoses. Other types of endometrial carcinomas include papillary serous carcinoma and clear cell carcinoma (Figure 14). These types of carcinoma have less association with the classic risk factors. They tend to behave as poorly differentiated tumors regard-less of their grade and have poorer prognoses.32
Most commonly, endometrial cancer appears as fairly diffuse thickening of the endometrium, which cannot be differentiated from endometri-al hyperplasia.30Endometrial cancer can also be
seen as an inhomogeneous focal mass. A recent article reported that the uterine cavities of women with endometrial cancer were poorly distensible, and this was the most consistent finding in this entity.28Because this is a potential
sign of malignancy, the use of a catheter with an occlusive balloon is important for assessing the distensibility of the uterine cavity.
Tamoxifen
Tamoxifen is used as adjunctive therapy for breast cancer in postmenopausal women. It has been shown to increase disease-free survival time in estrogen receptor–positive tumors, to increase overall survival, and to decrease con-tralateral breast cancers. In addition, the Breast Cancer Prevention Trial showed a 45% reduction in the development of cancer in high-risk patients.40,41 Because of its effectiveness, large
numbers of women are receiving tamoxifen. Tamoxifen is antiestrogenic in the breast but has a weakly estrogenic effect on the endometri-um. Therefore, the incidence of endometrial abnormalities is increased in patients taking tamoxifen. According to the National Surgical Adjuvant Breast and Bowel Project B-14 trial,42
the incidence of endometrial carcinoma was a 1.6 per 1000 annual risk in patients receiving tamoxifen. The relative risk in these women was 2.2 times greater than in control subjects. In addition to an increased incidence of endometri-al cancer, other benign endometriendometri-al abnormendometri-ali- abnormali-ties are also increased in incidence. The incidence of endometrial polyps is estimated at 8% to 36% in women treated with tamoxifen. Tamoxifen-related polyps (Figure 15) are gener-ally larger and differ from non–tamoxifen-related polyps in their histologic characteristics. Endometrial hyperplasia is increased in inci-dence in tamoxifen-treated women as well; the incidence is 1.3% to 20%.43 Because of the Figure 11. Endometrial hyperplasia in a 53-year-old woman with
abnormal vaginal bleeding. Saline infusion sonohysterography shows diffuse endometrial thickening and multiple cystic areas (arrowheads). Pathologic examination showed simple endome-trial hyperplasia. A, Longitudinal image before saline infusion;
B, longitudinal image after saline infusion; C, transverse image after saline infusion.
A
B
increased risk of endometrial abnormalities, SIS and TVS have been advocated as tools for evalu-ating these women.
Fong et al44 evaluated asymptomatic
post-menopausal women being treated with tamox-ifen and found endometrial abnormalities in 40% of their study group. Transvaginal sonogra-phy had a sensitivity of 85% and a specificity of 56% compared with SIS, which had a sensitivity of 90% and a specificity of 79%. Using receiver operating characteristic curves, these authors suggested that a 6-mm endometrial thickness be used as the upper limit of normal in these patients.
Tepper et al45prospectively evaluated
asymp-tomatic women with a history of breast cancer
and tamoxifen therapy who had a thickened endometrium. They defined a thickened endometrium as greater than 8 mm on TVS. The incidence of endometrial abnormalities in the study group was 32%. Saline infusion sonohys-terography enabled accurate diagnoses of uter-ine cavity abnormalities in 95.5% of the patients. The sensitivity for SIS was 100%, with a positive predictive value of 95%.
These studies showed a high incidence of endometrial abnormalities in asymptomatic postmenopausal women being treated with tamoxifen. They also showed that SIS is more sensitive and specific than TVS alone. In these studies, there were no cases of endometrial car-cinoma or atypical endometrial hyperplasia. The
Berridge and Winter
Figure 12. Endometrial hyperplasia in a 54-year-old woman with menorrhagia. Two SIS images (Aand B) show areas of focal thick-ening of the endometrium (arrowheads). Pathologic examination revealed complex endometrial hyperplasia without atypia.
A B
Figure 13.Thickened endometrium in a 43-year-old woman with abnormal bleeding between periods and anemia. Saline infusion sonohysterography shows a thickened endometrium with areas of undulation (arrowheads). Pathologic examination revealed a secre-tory endometrium. A, Before saline infusion; B, after saline infusion.
consensus statement from the Society of Radiologists in Ultrasound3concluded that there
was not enough evidence at that time to recom-mend routine screening in asymptomatic post-menopausal women treated with tamoxifen.
In the postmenopausal woman undergoing tamoxifen therapy who has abnormal uterine bleeding, a full clinical workup should be under-taken (as with any woman with postmenopausal bleeding) (Figure 16). This may include office endometrial biopsy as well as TVS and SIS. The most common imaging finding on TVS is endometrial thickening with cystic spaces. This finding is nonspecific, and endometrial hyper-plasia and endometrial polyps can both cause endometrial thickening. In addition, submucos-al cystic changes can be observed in tamoxifen-treated patients.
A study by Hann et al46evaluated 46
sonohys-terograms in patients who received tamoxifen for a mean of 2.6 years. Saline infusion sonohys-terography revealed endometrial polyps in 62% of patients; 12% had a thickened endometrium, and 8% had subendometrial cysts. Sixty-three percent of sonohysterograms with prior negative endometrial biopsy results had endometrial abnormalities, including 10 polyps. These authors also found that in 14% of cases, the find-ing of a normal endometrium on SIS allowed these patients to avoid further intervention.
Given the increased incidence of endometrial abnormalities in postmenopausal women treat-ed with tamoxifen, SIS is a useful tool for
evalua-tion of these women when vaginal bleeding develops. Not only can a more specific diagnosis be made with SIS over TVS, further intervention can sometimes be obviated on the basis of the increased confidence of negative SIS findings. Future Directions
Currently, most SIS examinations include imag-ing of the distended endometrial canal in the sagittal and coronal planes. These yield 2-dimen-sional representations of the endometrial canal. Some authors are advocating 3D imaging of the uterus with either multiplanar reconstructions or surface-rendering techniques (Figure 17).8,47
Three-dimensional imaging may become stan-dard as the software and hardware become more sophisticated and more laboratories become familiar with this technique. As 3D imaging has become standard practice in computed tomog-raphy and magnetic resonance imaging (MRI), sonography may soon follow.
Because SIS can show focal lesions with such exquisite detail, the next step may be to direct biopsies of endometrial abnormalities with real-time sonographic guidance. Dubinsky et al48
published a study in which biopsy of focal lesions was performed in conjunction with SIS. Under direct sonographic guidance, the endometrial canal was distended with saline, and, in the same setting, sonographically guided biopsy was per-formed. There were technical difficulties with leakage of the saline during the biopsy as well as
Figure 14.Papillary serous carcinoma in a 71-year-old woman with postmenopausal bleeding. Findings from blind endometrial biop-sy performed before the SIS were negative. Two SIS images (Aand B) show a polyp (arrowhead) in the lower endometrial canal. The polyp was subsequently resected. Pathologic examination showed a focus of papillary serous carcinoma of the endometrium arising within the polyp.
limited steerability of the biopsy device. However, with improvements in equipment, this technique may become a valuable adjunct to ensure that sonographically detected abnormalities are ade-quately sampled for biopsy or removed.
Magnetic resonance hysterography has been reported in the literature as a new technique for evaluating uterine abnormalities. Magnetic res-onance imaging gives excellent soft tissue con-trast in the uterus. Rouanet De Lavit et al49
instilled saline into the endometrial canal as performed for SIS. The uterus was then imaged using a fluid-attenuated inversion recovery sequence to null the signal from water. In addi-tion to convenaddi-tional MRI of the pelvis, this tech-nique may provide additional information regarding endometrial abnormalities, which may be particularly useful for evaluation of endometrial carcinoma in which the endolumi-nal component as well as the level of invasion can be established. It remains to be seen indeed whether this technique adds any additional information over SIS or conventional MRI of the female pelvis.
Conclusions
Saline infusion sonohysterography is a simple technique that yields additional information over TVS in evaluation of endometrial and subendometrial conditions. It is well tolerated by patients and has very few complications. Sonographers familiar with endovaginal sono-graphic imaging will find that SIS is not techni-cally difficult to incorporate into their practices.
In the patient with abnormal vaginal bleeding, SIS is able to better delineate the abnormality and to further characterize it. In a study by Bree et al9performed to evaluate the clinical impact of
SIS, they found that SIS added certainty to the diagnosis in 88% of the patients studied. In addi-tion, SIS results changed the patients’ treatment in 80% of cases. Normal SIS findings markedly increased diagnostic confidence by 86%.
In general, SIS has been used as a second-line test for abnormal vaginal bleeding. If the TVS shows a thin homogeneous endometrial stripe, then the probability of endometrial cancer is very unlikely, and often SIS is deferred. However, Laifer-Narin et al50 found that 14% of 114
patients with a normal-appearing endometrium on TVS had abnormalities discovered on SIS. These abnormalities were either endometrial
Berridge and Winter
Figure 15. Polyp in a woman with postmenopausal bleeding and history of treatment with tamoxifen. A, Saline infusion sonohysterography shows a large polyp with multiple cystic areas (arrows). Three-dimensional imaging with multiplanar reconstructions (B) and surface-rendering techniques (C) were performed.
A
B
polyps or leiomyomas. Given that intervention in this setting can provide resolution of symp-toms, SIS yielded additional clinically important information over TVS. Therefore, the authors advocated that SIS be a first-line test in patients with abnormal vaginal bleeding.
In conclusion, SIS is a simple and elegant examination that yields additional information over TVS of the uterus. Because the walls of the endometrium are separated by SIS, they can be evaluated individually. Focal abnormalities are beautifully displayed by this technique. This
information can then be used to direct the inter-vention. Biopsy of diffuse abnormalities can be performed with a blind technique, whereas focal abnormalities are best approached with a visually guided biopsy. Saline infusion sonohys-terography requires minimal patient prepara-tion, has very few complications, and is well tolerated by patients. Given its advantages over other techniques for uterine evaluation, SIS will likely play an even larger role in pelvic imaging in the future.
References
1. Parsons AK, Lense JJ. Sonohysterography for endometrial abnormalities: preliminary results. J Clin Ultrasound 1993; 21:87–95.
2. Syrop CH, Sahakian V. Transvaginal sonographic detection of endometrial polyps with fluid contrast augmentation. Obstet Gynecol 1992; 79:1041– 1043.
3. Goldstein RB, Bree RL, Benson CB, et al. Evaluation of the woman with postmenopausal bleeding: Society of Radiologists in Ultrasound–sponsored consensus conference statement. J Ultrasound Med 2001; 20:1025–1036.
4. American Institute of Ultrasound in Medicine. AIUM standard for the performance of saline infusion sonohysterography. J Ultrasound Med 2003; 22:121–126.
5. Bonnamy L, Marret H, Perrotin F, Body G, Berger C, Lansac J. Sonohysterography: a prospective survey of Figure 16.Mass in a 71-year-old woman with a history of breast cancer treated with tamoxifen for approximately 2 years who had postmenopausal bleeding. Saline infusion sonohysterography shows an inhomogeneous focal mass (arrows). Pathologic examination revealed metastatic breast cancer to the uterus. A, Longitudinal image; B, transverse image.
A B
Figure 17. Three-dimensional image of the endometrial cavity showing 2 polyps. Multiplanar reconstructions show the relationships of the dominant polyp (arrow-heads) in 3 orthogonal planes within the endometrial cavity.
results and complications in 81 patients. Eur J Obstet Gynecol Reprod Biol 2002; 102:42–47.
6. Dessole S, Farina M, Capobianco G, Nardelli GB, Ambrosini G, Meloni GB. Determining the best catheter for sonohysterography. Fertil Steril 2001; 76:605–609.
7. Goldstein SR, Zeltser I, Horan CK, Snyder JR, Schwartz LB. Ultrasonography-based triage for perimenopausal patients with abnormal uterine bleeding. Am J Obstet Gynecol 1997; 177:102–108.
8. Bonilla-Musoles F, Raga F, Osborne NG, Blanes J, Coelho F. Three-dimensional hysterosonography for the study of endometrial tumors: comparison with conventional transvaginal sonography, hysterosalpin-gography, and hysteroscopy. Gynecol Oncol 1997; 65:245–252.
9. Bree RL, Bowerman RA, Bohm-Velez M, et al. US eval-uation of the uterus in patients with postmenopausal bleeding: a positive effect on diagnostic decision mak-ing. Radiology 2000; 216:260–264.
10. Alborzi S, Dehbashi S, Parsanezhad ME. Differential diagnosis of septate and bicornuate uterus by sono-hysterography eliminates the need for laparoscopy. Fertil Steril 2002; 78:176–178.
11. Soares SR, Barbosa dos Reis MM, Camargos AF. Diagnostic accuracy of sonohysterography, transvagi-nal sonography, and hysterosalpingography in patients with uterine cavity diseases. Fertil Steril 2000; 73:406–411.
12. Kim AH, McKay H, Keltz MD, Nelson HP, Adamson GD. Sonohysterographic screening before in vitro fer-tilization. Fertil Steril 1998; 69:841–844.
13. Keltz MD, Olive DL, Kim AH, Arici A. Sonohystero-graphy for screening in recurrent pregnancy loss. Fertil Steril 1997; 67:670–674.
14. Karlsson B, Granberg S, Wikland M, et al. Transvaginal ultrasonography of the endometrium in women with postmenopausal bleeding: a Nordic multicenter study. Am J Obstet Gynecol 1995; 172:1488–1494.
15. Smith-Bindman R, Kerlikowske K, Feldstein VA, et al. Endovaginal ultrasound to exclude endometrial can-cer and other endometrial abnormalities. JAMA 1998; 280:1510–1517.
16. Guido RS, Kanbour-Shakir A, Rulin MC, Christopherson WA. Pipelle endometrial sampling: sensitivity in the detection of endometrial cancer. J Reprod Med 1995; 40:553–555.
17. Jorizzo JR, Riccio GJ, Chen MY, Carr JJ. Sonohysterography: the next step in the evaluation of the abnormal endometrium. Radiographics 1999; 19:S117–S130.
18. Gull B, Carlsson S, Karlsson B, Ylostalo P, Milsom I, Granberg S. Transvaginal ultrasonography of the endometrium in women with postmenopausal bleed-ing: is it always necessary to perform an endometrial biopsy? Am J Obstet Gynecol 2000; 182:509–515. 19. Gull B, Karlsson B, Milsom I, Granberg S. Can
ultra-sound replace dilation and curettage? A longitudinal evaluation of postmenopausal bleeding and transvaginal sonographic measurement of the endometrium as predictors of endometrial cancer. Am J Obstet Gynecol 2003; 188:401–408.
20. Anastasiadis PG, Koutlaki NG, Skaphida PG, Galazios GC, Tsikouras PN, Liberis VA. Endometrial polyps: prevalence, detection, and malignant potential in women with abnormal uterine bleeding. Eur J Gynaecol Oncol 2000; 21:180–183.
21. Lev-Toaff AS. Sonohysterography: evaluation of endometrial and myometrial abnormalities. Semin Roentgenol 1996; 31:288–298.
22. Kupfer MC, Schiller VL, Hansen GC, Tessler FN. Transvaginal sonographic evaluation of endometrial polyps. J Ultrasound Med 1994; 13:535–539. 23. Fleischer AC, Shappell HW. Color Doppler
sonohys-terography of endometrial polyps and submucosal fibroids. J Ultrasound Med 2003; 22:601–604. 24. Goldstein SR, Monteagudo A, Popiolek D, Mayberry
P, Timor-Tritsch I. Evaluation of endometrial polyps. Am J Obstet Gynecol 2002; 186:669–674.
25. Perez-Medina T, Bajo J, Huertas MA, Rubio A. Predicting atypia inside endometrial polyps. J Ultrasound Med 2002; 21:125–128.
26. Hutchins FL Jr. Uterine fibroids: diagnosis and indica-tions for treatment. Obstet Gynecol Clin North Am 1995; 22:659–665.
27. Stewart EA. Uterine fibroids. Lancet 2001; 357:293– 298.
28. Laifer-Narin SL, Ragavendra N, Lu DS, Sayre J, Perrella RR, Grant EG. Transvaginal saline hysterosonography: characteristics distinguishing malignant and various benign conditions. AJR Am J Roentgenol 1999; 172:1513–1520.
29. Caoili EM, Hertzberg BS, Kliewer MA, DeLong D, Bowie JD. Refractory shadowing from pelvic masses
on sonography: a useful diagnostic sign for uterine leiomyomas. AJR Am J Roentgenol 2000; 174:97–101. 30. Davis PC, O’Neill MJ, Yoder IC, Lee SI, Mueller PR. Sonohysterographic findings of endometrial and subendometrial conditions. Radiographics 2002; 22:803–816.
31. O’Connell LP, Fries MH, Zeringue E, Brehm W. Triage of abnormal postmenopausal bleeding: a comparison of endometrial biopsy and transvaginal sonohysterog-raphy versus fractional curettage with hysteroscopy. Am J Obstet Gynecol 1998; 178:956–961.
32. Cotran R, Kumar V, Collins T, (eds). Robbins Pathologic Basis of Disease. 6th ed. Philadelphia, PA: WB Saunders Co; 1999.
33. Kurman RJ, Kaminski PF, Norris HJ. The behavior of endometrial hyperplasia: a long-term study of “untreated” hyperplasia in 170 patients. Cancer 1985; 56:403–412.
34. Jorizzo JR, Chen MY, Martin D, Dyer RB, Weber TM. Spectrum of endometrial hyperplasia and its mimics on saline hysterosonography. AJR Am J Roentgenol 2002; 179:385–389.
35. Dubinsky TJ, Stroehlein K, Abu-Ghazzeh Y, Parvey HR, Maklad N. Prediction of benign and malignant endometrial disease: hysterosonographic-pathologic correlation. Radiology 1999; 210:393–397.
36. Davies JL, Rosenshein NB, Antunes CM, Stolley PD. A review of the risk factors for endometrial carcinoma. Obstet Gynecol Surv 1981; 36:107–116.
37. Gambone JC, Pardridge WM, Lagasse LD, Judd HL. In vivo availability of circulating estradiol in post-menopausal women with and without endometrial cancer. Obstet Gynecol 1982; 59:416–421.
38. Judd HL, Davidson BJ, Frumar AM, Shamonki IM, Lagasse LD, Ballon SC. Serum androgens and estro-gens in postmenopausal women with and without endometrial cancer. Am J Obstet Gynecol 1980; 136:859–871.
39. Feldman S, Shapter A, Welch WR, Berkowitz RS. Two-year follow-up of 263 patients with post/peri-menopausal vaginal bleeding and negative initial biopsy. Gynecol Oncol 1994; 55:56–59.
40. Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 study. J Natl Cancer Inst 1998; 90:1371–1388.
41. Osborne CK. Tamoxifen in the treatment of breast cancer. N Engl J Med 1998; 339:1609–1618. 42. Fisher B, Costantino JP, Redmond CK, Fisher ER,
Wickerham DL, Cronin WM. Endometrial cancer in tamoxifen-treated breast cancer patients: findings from the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-14. J Natl Cancer Inst 1994; 86:527–537.
43. Ascher SM, Imaoka I, Lage JM. Tamoxifen-induced uterine abnormalities: the role of imaging. Radiology 2000; 214:29–38.
44. Fong K, Kung R, Lytwyn A, et al. Endometrial evalua-tion with transvaginal US and hysterosonography in asymptomatic postmenopausal women with breast cancer receiving tamoxifen. Radiology 2001; 220:765–773.
45. Tepper R, Beyth Y, Altaras MM, et al. Value of sono-hysterography in asymptomatic postmenopausal tamoxifen-treated patients. Gynecol Oncol 1997; 64: 386–391.
46. Hann LE, Giess CS, Bach AM, Tao Y, Baum HJ, Barakat RR. Endometrial thickness in tamoxifen-treated patients: correlation with clinical and pathologic find-ings. AJR Am J Roentgenol 1997; 168:657–661. 47. Lev-Toaff AS, Pinheiro LW, Bega G, Kurtz AB,
Goldberg BB. Three-dimensional multiplanar sonohys-terography: comparison with conventional two-dimensional sonohysterography and x-ray hysteros-alpingography. J Ultrasound Med 2001; 20:295–306. 48. Dubinsky TJ, Reed S, Mao C, Waitches GM, Hoffer EK. Hysterosonographically guided endometrial biopsy: technical feasibility. AJR Am J Roentgenol 2000; 174: 1589–1591.
49. Rouanet De Lavit JP, Maubon AJ, Thurmond AS. MR hysterography performed with saline injection and fluid attenuated inversion recovery sequences: initial experi-ence. AJR Am J Roentgenol 2000; 175:774–776. 50. Laifer-Narin S, Ragavendra N, Parmenter EK, Grant
EG. False-normal appearance of the endometrium on conventional transvaginal sonography: compari-son with saline hysterocompari-sonography. AJR Am J Roentgenol 2002; 178:129–133.







![6 (2 Fluorophenyl) 5,6 dihydrobenzimidazolo[1,2 c]quinazoline](data:image/gif;base64,R0lGODlhAQABAIAAAP///wAAACH5BAEAAAAALAAAAAABAAEAAAICRAEAOw==)