Nephrol Dial Transplant (2013) 0: 1–6 doi: 10.1093/ndt/gft412
Original Article
The prognostic value of time needed on dialysis in patients
with delayed graft function
Caitlyn Marek
1,2,
Benjamin Thomson
3,
Ahmed Shoker
2,
Patrick P. Luke
3and Michael A.J. Moser
1,21Department of Surgery, University of Saskatchewan, Saskatoon,
SK, Canada,
2Saskatchewan Renal Transplant Program, St. Paul’s Hospital,
Saskatoon, SK, Canada and
3Multi-Organ Transplant Program, London Health Sciences Centre,
Schulich School of Medicine, Western University, London, ON, Canada
Correspondence and offprint requests to: Michael A.J. Moser; E-mail: [email protected]
Keywords: delayed graft function, dialysis, kidney transplantation, prognosis, time needed on dialysis
A B S T R AC T
Introduction. We hypothesize that in patients with delayed graft function (DGF), the need for a longer time needed on dialysis (TND) post-kidney transplant is associated with poorer long-term function and an increase in complications. Methods.This was a retrospective chart review involving col-laboration between Western University (WU) Renal Trans-plant Program of London, Ontario and the Saskatchewan renal transplant program (SRTP). A total of 774 patients (567 WU and 207 SRTP) received kidney transplants between 2004 and 2011, of which 83 patients with deceased donor trans-plants (59 WU and 24 SRTP) developed DGF, defined as the need for dialysis in thefirst week posttransplant.
Results.Patients with DGF were divided into three groups de-pending on TND [group 1: <7 days (n= 52), group 2: 7–14 days (n= 13) and group 3 (n= 18): >14 days]. The creatinine clearance (CrCl) at 30 days (42.5, 33.8, 20.0 cc/min; P < 0.001) and 1 year (56.7, 49.2, 37.3 cc/min, P = 0.031) were signifi -cantly different between the three groups. Multivariate regression analysis identified length of TND posttransplant (β=−0.5, P < 0.001) and donation after cardiac death (DCD) donor (β= 19.5, P < 0.001) as the most significant predictors of CrCl at 1 year in these patients with DGF. DCD kidneys with DGF had a higher CrCl at 1 year and fewer readmissions in thefirst year compared with non-DCD kidneys with DGF. Discussion.Our study suggests that increased TND is associ-ated with worse CrCl at 1 year. The data also support the
hypothesis of a different mechanism for DGF in DCD and non-DCD kidneys.
INTRODUCTIO N
In the early posttransplant period, some kidneys recover quickly from delayed graft function (DGF), while others can take weeks before resuming function [1]. Overall, the long-term outcomes are less favorable for grafts that have initial DGF [2, 3]. Yet, little has been written about the long-term prognosis of those kidneys that take longer to‘wake up’after transplant, particularly in the era of donation after cardiac death (DCD) kidney transplants.
A review of the literature shows that only a few studies have examined time needed on dialysis (TND) as a factor in long-term graft function. An early study used a unique definition of DGF that was independent of the need for dialysis (time to attain an estimated glomerularfiltration rate (eGFR) of≥10 mL/min) [4]. In their study, kidneys requiring >6 days to cross this threshold of eGFR were shown to have a poorer long-term graft survival. In 2009, a small study suggested that serum creatinine at 1 year was adversely affected by a longer DGF duration [5]. A more recent study showed that the need for only a single dialysis treatment after transplant was not associ-ated with the worse outcomes seen in patients requiring a longer duration of dialysis [6]. Our study differed from these previous studies in that it included patients receiving kidneys
from DCD donors and more expanded criteria (ECD) donors than the early study, in keeping with the demographics of the donor population in most North American and European pro-grams today.
We hypothesize that a longer length of TND portends a poorer prognosis for long-term renal function in terms of creatinine clearance (CrCl) at 1 year. Also, recent publications [7, 8] have documented a better prognosis for DCD kidneys with DGF than for non-DCD kidneys with DGF, and we wished to examine the effect of a longer TND on function in these DCD kidneys.
M AT E R I A L S A N D M E T H O D S
This was a retrospective chart review involving collaboration between the Western University (WU) and the Saskatchewan renal transplant program (SRTP). Information about each re-cipient and their donor as well as investigations in the preo-perative and postopreo-perative course of these 83 patients with DGF was collected retrospectively. Patients were divided into three groups depending on TND [group 1: <7 days (n= 52), group 2: 7–14 days (n= 13) and group 3 (n= 18): >14 days], but analysis was also carried out using TND as a linear vari-able. Our main outcome of interest was the CrCl at 1 year, and secondary outcomes were adverse events.
CrCl was estimated using the Cockcroft–Gault equation. Complications examined included wound infection or leakage, reoperation, ICU admission, readmission or graft loss within less than a year. Wound infection was defined as the need for the incision to be reopened partially or completely and packed. Significant wound leakage was defined as a need for consul-tation to a specialized wound care team or the placement of a bag appliance. Reoperations for the purpose of our study in-cluded only those reoperations that required reopening the kidney transplant incision. Neither program performed routine protocol biopsies, but instead performed biopsies based on clinical indication; rejection episodes in this study were biopsy proven.
Univariate analysis of factors involved in CrCl at 1 year was carried out and factors with P < 0.20 were included in the multivariate analysis as per the classic method of Kleinbaum
et al. [15].
The multivariate analysis was repeated to include variables that are generally considered classic confounders, including donor age [16], early acute rejection [17] and DCD donor, in addition to TND. Cold ischemic time (CIT), one of the tra-ditional confounders, was not included because the range of CIT was very narrow and the difference between the donor kidneys with the longest and shortest CIT’s would not be ex-pected to make a significant difference to renal function [18], and in order to keep the number of variables to an acceptable number. Medications used postoperatively were not included in the model because all but one patient received induction (61 thymoglobulin, 21 basiliximab, 1 patient refused); no differences were found between the two types of induction with respect to CrCl at 1 year. Finally, all but three of the patients received tacrolimus-based immunosuppression,
precluding any meaningful analysis of the effect of immuno-suppressive drugs as a confounder. Biopsy-proven early acute rejection was included as a possible confounder in one of the regression models because of a trend towards less early acute rejection in the DCD group and because of this well-documen-ted factor in the outcome of kidney transplants. Due to con-cerns over colinearity between donor age and donor Cr (r=−0.206, P = 0.05), these two could not be included in any model at the same time, but were analyzed individually in sep-arate multivariate models. TND was analyzed in multivariate regression modelsfirst as a continuous variable, then as a cat-egorical variable.
Data were analyzed using SPSS 20.0 (IBM Corporation, Armonk, NY), including multivariate linear regression, theχ2 -test, ANOVA, and Student’st-test with Bonferroni correction for multiple comparisons. Ethics approval was obtained from the Ethics Review Board at both institutions.
R E S U LTS
Between January 2004 and December 2011, there were 567 kidney transplants at WU Renal Transplant Program of London, Ontario and 227 at SRTP, for a total of 774 trans-plants. For the purposes of our study, multi-visceral, repeat and en bloc kidney transplants were excluded. A total of 83 patients receiving deceased donor kidney transplants devel-oped DGF, which is defined as the need for dialysis in thefirst week posttransplant. There were 59 cases of DGF at WU and 24 cases of DGF at SRTP during this time period. The two sites had similar practices and, aside from the fact that the WU site has had a DCD program since 2006 and the SRTP does not have a DCD program, the two sites showed no signifi -cant differences in terms of donor or recipient age, dialysis modality, use of machine cold perfusion, CIT rate of DGF, rate of early acute rejection and length of stay.
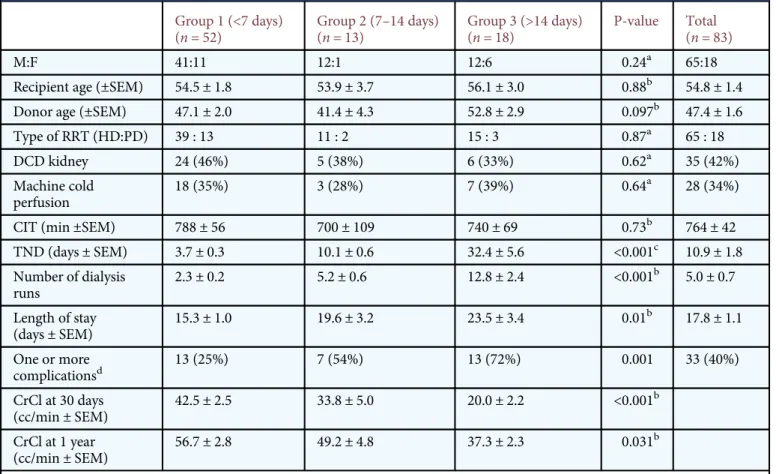
Patient demographics are shown in Table1. The 83 patients with DGF were divided into three groups based on the number of days postoperatively that dialysis was needed, whether <7 days (group 1, n= 52), between 7 and 14 days (group 2, n= 13) and >2 weeks (group 3,n= 18). The three groups were similar in terms of recipient demographics, dialy-sis modality, proportion of DCD transplants and CIT. The CrCl at 30 days and at 1 year showed differences between the three groups, with poorer function seen in patients having longer TND. A greater proportion of patients with one or more complications were seen in the groups of patients requir-ing longer time on dialysis.
Univariate analysis of potential predictors of CrCl at 1 year is shown in Table2. A multivariate regression model of CrCl at 1 year was constructed including the variables with P-value < 0.20 on univariate analysis (donor age, DCD kidneys and TND). TND and DCD donor emerged as highly signifi -cant predictive factors of CrCl at 1 year (each with P < 0.001, Table3). A longer TND predicted a lower CrCl and a patient receiving a DCD donor kidney would be expected to have a higher CrCl at 1 year.
ORIGINAL
The multivariate analysis was repeated using variables that are generally considered to be classic confounders. The result of the model including donor age, early acute rejection, DCD
donor and TND was the same, with TND and DCD donor being highly significant predictors of CrCl at 1 year (each P < 0.001). Donor age and donor creatinine, which showed sig-nificant colinearity, were entered separately in multivariate models and again the results were the same. Likewise, when TND was entered as a categorical value in the models men-tioned above, the results were unchanged.
Comparison between patients with DGF who received a kidney from a DCD donor versus a non-DCD donor was carried out (Table4). The two groups were similar in terms of demographics except for machine cold perfusion use
Table 2. Univariate analysis of factors
predictive of CrCl at 1 year
Factor P-value
Donor age 0.02
Donor Cr 0.68
DCD kidney 0.001
Use of machine cold perfusion 0.29
CIT 0.73
Thymoglobulin use 0.53
Hemodialysis 0.96
TND 0.001
Acute rejection episode infirst 30 days 0.28
Table 3. Multivariate regression model of
CrCl at 1 year
Factor P-value Β 95% CI
TND <0.001 −0.5 −0.76,−0.24
DCD donor <0.001 19.5 11.4, 27.6 Donor age 0.54
Table 1. Demographics and outcomes for the three groups of patients, divided according to TND
Group 1 (<7 days) (n= 52) Group 2 (7–14 days) (n= 13) Group 3 (>14 days) (n= 18) P-value Total (n= 83) M:F 41:11 12:1 12:6 0.24a 65:18Recipient age (±SEM) 54.5 ± 1.8 53.9 ± 3.7 56.1 ± 3.0 0.88b 54.8 ± 1.4
Donor age (±SEM) 47.1 ± 2.0 41.4 ± 4.3 52.8 ± 2.9 0.097b 47.4 ± 1.6
Type of RRT (HD:PD) 39 : 13 11 : 2 15 : 3 0.87a 65 : 18
DCD kidney 24 (46%) 5 (38%) 6 (33%) 0.62a 35 (42%)
Machine cold perfusion
18 (35%) 3 (28%) 7 (39%) 0.64a 28 (34%)
CIT (min ±SEM) 788 ± 56 700 ± 109 740 ± 69 0.73b 764 ± 42
TND (days ± SEM) 3.7 ± 0.3 10.1 ± 0.6 32.4 ± 5.6 <0.001c 10.9 ± 1.8 Number of dialysis runs 2.3 ± 0.2 5.2 ± 0.6 12.8 ± 2.4 <0.001b 5.0 ± 0.7 Length of stay (days ± SEM) 15.3 ± 1.0 19.6 ± 3.2 23.5 ± 3.4 0.01b 17.8 ± 1.1 One or more complicationsd 13 (25%) 7 (54%) 13 (72%) 0.001 33 (40%) CrCl at 30 days (cc/min ± SEM) 42.5 ± 2.5 33.8 ± 5.0 20.0 ± 2.2 <0.001b CrCl at 1 year (cc/min ± SEM) 56.7 ± 2.8 49.2 ± 4.8 37.3 ± 2.3 0.031b
RRT, renal replacement therapy.
aCalculated using theχ2-test.
bCalculated using ANOVA.
cCalculated using ANOVA, Kaplan Meier, and Krushkal–Wallis. The result was the same for all three tests.
dComposite of wound leak, wound infection, ICU admission, reoperation, graft loss under 1 year and death <1 year posttransplant.
ORIGINAL
(P = 0.05). While the CrCl was very similar for the two groups at 30 days, a marked difference was seen at 1 year, with the DCD, DGF group having a higher CrCl (63.7 versus 45.7 cc/ min, P < 0.001). A comparison of the adverse events sustained by patients in the two groups (Table4) showed a difference in terms of readmissions in thefirst 6 months (50 versus 11%, non-DCD versus DCD). There was a trend towards more early acute rejection, graft loss and complications in the non-DCD DGF patients.
D I S C U S S I O N
In our study of patients with DGF, the length of TND before the resolution of DGF was shown to be a factor predictive of CrCl at 1 year. Also, patients with DGF whose kidney trans-plants came from DCD donors had better CrCl at 1 year com-pared with patients with DGF whose kidneys did not come from DCD donors.
Although DCD kidneys have a high incidence of DGF, it is becoming clear that DCD kidneys with DGF have similar crea-tinine at 1 year compared with standard criteria donors or DCD donor transplants that did not experience DGF [9,10]. Markedly lower readmission rates were seen for recipients of DCD kidneys and (although not statistically significant), we
saw trends towards less TND, lower early acute rejection, lower complication rates and lower readmission rates for the DCD group, similar to that in previous reports and arguing in favor of different mechanisms for DGF in the two groups.
One possibility is that DCD donors are more carefully se-lected, but our data in Table4shows the DCD and non-DCD kidneys to have similar demographics. It has been hypoth-esized that there exist different mechanisms for the injury that leads to DGF whether a kidney is from a DCD donor or a donation after brain death (DBD) donor. In the case of DBD, inflammatory mediators and cytokines released due to the mechanism of death may increase inflammation and tissue injury [11]. Early diminished allograft reserve may then explain the long-term diminished GFR. On the other hand, the ischemic injury that occurs to DCD kidneys may be less likely to provoke immune attack and early acute rejection and more likely to be reversible.
The reason for the association of prolonged TND with worse long-term function could be that more dialysis is somehow detrimental to long-term renal function, either because of transient hypotension that occurs with hemodialy-sis or to inflammatory reactions to dialysis membranes or dia-lysate [12,13]. In our study, there was no difference in CrCl at 1 year between patients dialyzed postoperatively with perito-neal dialysis or with hemodialysis (56.0 ± 6.3 cc/min versus
Table 4. Comparison of patients with DGF who received a DCD kidney transplant or a non-DCD
kidney transplant
Non-DCD (n= 48) DCD (n= 35) P-value
Recipient age (±SEM) 53.8 ± 2.0 56.0 ± 1.9 0.45a
Donor age (±SEM) 47.7 ± 2.2 47.1 ± 2.2 0.86a
ECD 18 (38%) 9 (26%) 0.26b
Machine cold perfusion 12 (25%) 16 (46%) 0.05b
CIT (min) 660 ± 41 547 ± 39 0.08a
TND (days ± SEM) 12.5 ± 2.4 8.8 ± 2.5 0.15a
Number of dialysis runs 5.1 ± 0.8 4.8 ± 1.2 0.95a
Length of Stay (days ± SEM) 18.4 ± 1.8 16.8 ± 1.2 0.48a
CrCl at 30 days (cc/min ± SEM) 38.0 ± 2.6 34.7 ± 3.4 0.43a
CrCl at 1 year (cc/min ± SEM) 45.7 ± 2.4 63.7 ± 4.0 <0.001a
Dialysis dependence at 30 days 8 (17%) 1 (3%) 0.10b
Rejection infirst 30 days 9 (19%) 2 (6%) 0.06b
Readmission infirst 6 months 24 (50%) 4 (11%) 0.001b
Graft Loss before 1 year 4 (8%) 0 0.22b
Death before 1 year 2 (4%) 1 (3%) 0.78b
One or more complicationsc 23 (48%) 10 (29%) 0.08b
DCD, donation after cardiac death; CIT, cold ischemic time.
aCalculated using Student’st-test.
bCalculated using theχ2-test.
cComposite of wound leak, wound infection, ICU admission, reoperation, graft loss under 1 year and death <1 year posttransplant.
ORIGINAL
53.1 ± 2.5 cc/min, P = 0.27). An earlier study found that a single dialysis run in the early postoperative period resulted in no detrimental effect to long-term kidney function [6].
Instead, it seems more likely that the association between prolonged TND and decreased long-term function is due to the fact that kidneys with worse baseline function also have less functional reserve or perhaps fewer glomeruli [14] and hence require more support in terms of dialysis. The fact that increased donor age is associated with worse function at 1 year is in keeping with this possibility [7].
Our study is limited by the somewhat subjective nature of the definition of DGF. If and when to initiate dialysis as well as when to stop doing dialysis on these patients is somewhat of a subjective judgment call of the treating transplant physician, but is thought to be similar between the two sites. Thus, the number of days needed on dialysis (TND) is a rough measure at best, yet there is no denying that a patient who ‘needed’ dialysis for the first 14 days postoperatively needed signifi -cantly more support than a patient who needed 5 days, for example. When the kidney‘wakes up’out of DGF, however, it generally does so quite convincingly and it is likely that two transplant physicians might differ only by one dialysis treat-ment, if there was a difference at all.
We used well-documented variables to construct our regression models, in order to control for known factors, yet any regression study is limited by the fact that a number of variables are likely unknown. CIT, one of the usual known factors, for example, did not emerge as a significant predictor likely because the average CIT’s was quite reasonable and the range of CIT’s was quite narrow. Early acute rejection, a classic confounder, did not emerge as a statistically significant con-founder, and this may be related to the fact that neither center does protocol biopsies nor is there a protocol dictating how many days of lack of return of function warrants a biopsy. Only 30 out of 83 (36%) of the patients in our study had a transplant biopsy, with 12 done in the first week, 10 in the second week, and 8 after a period of >2 weeks from the time of the transplant. The incidence of early acute rejection may have been underestimated in our study as a result. A trend towards more early acute rejection in the non-DCD transplants in our study and literature showing significant differences between non-DCD and DCD transplants in terms of early acute rejec-tion [13] further emphasizes the need for inclusion of early acute rejection in a multivariate analysis model.
The proportion of patients experiencing one or more com-plications seems to increase with increased TND. Whether this is a cause or an effect of the increased TND cannot be dis-cerned in this study, but it is nonetheless an interesting
finding. In both centers, DGF is an indication to hold off the use of calcineurin inhibitors and to use thymoglobulin in the initial postoperative period. The use of thymoglobulin has been associated with leaky capillaries, hypotension, respiratory embarrassment and an increased risk of ICU admission, all of which may contribute to prolonging DGF. One of our earlier studies found that a large number of patients requiring ICU admission after transplant had received thymoglobulin [8]. The dosing and duration of thymoglobulin administration are protocol based and, according to our data, there is no
difference in dose received whether someone had DGF for 5 or 21 days.
The length of time it takes for a kidney to recover from DGF can provide useful prognostic information about long-term function, and it seems that the need for prolonged dialy-sis is more likely an effect than a cause of a reduced function kidney. DGF that lasts >2 weeks results in a markedly poorer function at 1 year. As the length of time on dialysis seems to be an effect rather than a cause of decreased function, early weaning from dialysis prior to definite return of renal function would not be expected to lead to an improvement in renal function. The differences between patients with DGF from DCD and non-DCD kidneys suggest a different mechanism of injury between the two types of organs and perhaps looking at interventions aimed at reducing the inflammatory response that occurs at the time of procurement of non-DCD kidneys should be pursued.
AC K N OW L E D G E M E N T S
The authors thank Michael Bloch (WU), Corinne Weernink (WU), Sandra Lockhart (SRTP) and Verna Bloom (SRTP) for help in data collection and Dr Rhonda Bryce and Dr Punam Pahwa for their help with the statistics. C.M. supported by the University of Saskatchewan College of Medicine Dean’s Research Program and the Department of Surgery Research Chair Funding.
A U T H O R’S CON TRIB UT ION
C.M. participated in study design, data collection, data analysis and writing of the paper. B.T. participated in study design, data collection, data analysis and writing of the paper. A.S. participated in study design and writing of the paper. P.P.L. participated in study design, data analysis and writing of the paper. M.A.J.M. participated in study design, data collection, data analysis and writing of the paper.
R E F E R E N C E S
1. Yarlagadda SG, Klein CL, Jani A. Long term renal outcomes after
DGF. Adv Chr K Dis 2008; 15: 248–256
2. Perico N, Cattaneo D, Sayegh Met al. Delayed graft function in
kidney transplantation. Lancet 2004; 364: 1814–1827
3. Ojo AO, Wolfe RA, Held P et al. Delayed graft function: risk
factors and implications for renal allograft survival. Transplan-tation 1997; 63: 968
4. Giral-Classe M, Hourmant M, Cantarovich Det al. Delayed graft
function of more than six days strongly decreases long-term
sur-vival of transplanted kidneys. Kidney Int 1998; 54: 972–978
5. Dominguez J, Lira F, Rebodello Ret al. Duration of delayed graft
function is an important predictor of 1-year serum Creatinine.
Transpl Proc 2009; 41: 131–132
6. Jayaram D, Kommareddi M, Sung RSet al. Delayed graft function
requiring more than one-time dialysis treatment is associated
ORIGINAL
with inferior clinical outcomes. Clin Transplant 2012; 26:
E536–E543
7. Weinstein JR, Anderson S. The aging kidney: physiological
changes. Adv Chronic Kidney Dis 2010; 17: 302–307
8. Moser M, Sharpe M, Weernink Cet al. Five-year experience with
donation after cardiac death kidney transplantation in a Cana-dian transplant program: factors affecting outcomes. Cdn Urol
Assoc J 2012; 6: 448–452
9. Singh RP, Farney AC, Rogers Jet al. Kidney transplantation from
donation after cardiac death donors: lack of impact of delayed graft function on post-transplant outcomes. Clin Transplant
2011; 25: 255–264
10. Nagaraja P, Roberts GW, Stephens Met al. Influence of delayed
graft function and acute rejection on outcomes after kidney trans-plantation from donors after cardiac death. Transtrans-plantation
2012; 94: 1218–1223
11. Stroo I, Stokman G, Teske GJet al. Chemokine expression in
renal ischemia/reperfusion is most profound during the
repara-tive phase. Int Immunol 2010; 22: 433–442
12. Bitla AR, Reddy PE, Manohar SM,et al. Effect of a single
hemo-dialysis session on inflammatory markers. Hemodial Int 2010;
14: 411–417
13. Jofre R, Rodriguez-Benitez P, Lopez-Gomez JMet al. Infl
amma-tory syndrome in patients on hemodialysis. JASN 2006; 17:
S274–S280
14. Nyengaard JR, Bendtsen TF. Glomerular number and size in relation to age, kidney, and body surface in normal man. Anat
Rec 1992; 232: 194–201
15. Kleinbaum DG, Kupper LL, Muller KEet al. Applied Regression
Analysis and Other Multivariable Methods, 3rd edn. Belmont,
CA: Wadsworth, 1998, pp. 186–199
16. Saidi RF, Elias N, Kawai Tet al. Outcome of kidney
transplan-tation using expanded criteria donors and donation after cardiac death kidneys: realities and costs. Am J Transplant 2007; 7:
2769–2774
17. McLaren AJ, Jassem W, Gray DWet al. Delayed graft function:
risk factors and the relative effects of early function and acute re-jection on long-term survival in cadaveric renal transplantation.
Clin Transpl 1999; 13: 266–272
18. Layler LK, Srinivas TR, Schold JD. Influence of CIT-induced
DGF on kidney transplant outcomes. Am J Transplant 2011; 11:
2657–2664
Received for publication: 29.4.2013; Accepted in revised form: 27.8.2013
ORIGINAL