Review
article
Possible
functional
scaffolds
for
periodontal
regeneration
Hidetoshi
Shimauchi
a,*
,
Eiji
Nemoto
a,
Hiroshi
Ishihata
a,
Masatsugu
Shimomura
ba
DivisionofPeriodontologyandEndodontology,GraduateSchoolofDentistry,TohokuUniversity,4-1Seiryo-machi, Aoba-ku,Sendai980-8575,Japan
b
OrganizedPolymerMaterial,InstituteofMultidisciplinaryResearchforAdvancedMaterialsLaboratory(IMRAM), TohokuUniversity,2-1-1Katahira,Aoba-ku,Sendai980-8577,Japan
Received9March2013;receivedinrevisedform29April2013;accepted22May2013
Contents
1. Introduction... 119
2. Currentstrategiesforperiodontalregeneration... 119
3. Periodontaltissueengineering... 120
4. Thedesirablepropertiesofscaffoldsdesignedforperiodontalregeneration... 122
4.1. Mimickingthestemcellnichetoaltertheregulationofstemcells... 122
KEYWORDS
Periodontalregeneration; Scaffold;
Tissueengineering; Cell—scaffoldinteraction
Summary Periodontaldiseasesarethemostprevalentinfectiousdiseaseswiththeirreversible lossoftoothsupportingapparatus.Toreestablishthestablehealthofperiodontaltissuesafter healing,theconceptofregenerativesurgicalprocedureshasbeendevelopedoverthepastthree decades,includingvariousgraftingmaterials,guidedtissueregeneration(GTR),andtheuseof enamelmatrixderivatives(EMD)inaclinicalsetting.Morerecently,tissueengineeringstrategies havealsobeenappliedanddevelopedforperiodontalregeneration:(1)stemcelltherapies;(2) recombinanthumangrowthfactortherapies;(3)combineduseofcellandgrowthfactorswith matrix-based scaffolds. However, the complete and predictable reconstruction of healthy periodontal tissuesstillremains achallenging field.Toovercometherapeuticlimitationsand develop stemcell-basedstrategies,itisnecessarytooptimizecell—scaffoldcombinationsby understanding the cellular events during periodontal wound healing and regeneration. We reviewed: (1)the current statusand strategies for periodontal regeneration; (2)a possible biomaterial design for the scaffold used in periodontal tissue engineering; (3) a possible interactionbetweenscaffoldmaterialsandperiodontaltissuecells.
#2013JapaneseAssociationforDentalScience.PublishedbyElsevierLtd.Allrightsreserved.
* Correspondingauthor.Tel.:+81227178333;fax:+81227178339. E-mailaddress:[email protected](H.Shimauchi).
Availableonlineatwww.sciencedirect.com
j o urn a l hom e pa g e : ww w . e l se v i e r. c om / l oca t e / j ds r
1882-7616/$—seefrontmatter# 2013JapaneseAssociationforDentalScience.PublishedbyElsevierLtd.Allrightsreserved. http://dx.doi.org/10.1016/j.jdsr.2013.05.001
4.2. Cell—scaffoldinterplayandscaffolddesigning... 124
4.3. ApplicationofahoneycombmicroarrayfilmforPDLcellsheetengineering... 124
4.4. Possibleinductionofcementogenesisbymodulationoftheextracellularionicmicroenvironment usingbioactiveceramicscaffolds... 125
4.5. Applicationofnanofabricatedhydroxyapatiteforbonetissueengineering... 127
5. Conclusionsandfutureprospects... 128
Acknowledgements ... 128
References... 128
1.
Introduction
Periodontal diseases are the most common inflammatory diseasescausedbyplaquebiofilmintheoralcavity.During the progression of periodontal diseases, the pathological changeofgingivitis toperiodontitisis characterizedbythe irreversible loss of tooth supporting apparatus, ultimately leadingtothelossofthetooth.Itincludes theprogressive destructionofwholeperiodontaltissue:thegingiva, period-ontalligament(PDL),cementum,andalveolarbone,aswell astheconnectivetissueattachmentbetweentherootsurface andalveolarbone[1].Theconceptofconventional period-ontal treatments is a ‘‘cause-related therapy’’ aimed at removingcausativeagentsfromtheoralcavity,withafocus on eliminating bacterial plaque andcalculus. This therapy commonlyresultsinsuccessfulimprovementsinthe inflam-matoryprocessofperiodontaltissue;however,itonlyinduces theunstablehealthyconditionofdestroyedperiodontal tis-sueincaseofprogressiveperiodontitisevenafterasuccessful result.Therecoveredhealthyconditionofdestroyedtissueis easilybrokenbythereaccumulationofbacteriasurrounding theteeth,leadingtotherecurrenceofperiodontitis.Inthe UnitedStates,arecentnationalsurvey(2009—2010National HealthandNutritionExaminationSurvey;NHANES)revealed thatanestimated47.2%or64.7millionadultsaged30and over suffered from periodontitis, and prevalence rates increasedto70.1%inadults65andolder[2].Theprevalence ratesofperiodontaldiseasesinJapanare alsosimilar, indi-catingthatperiodontaldiseasesareoneofthemostcommon infectiousdiseasesintheworld.Furthermore,recentclinical research hasindicated thecloseandbidirectional relation-shipbetween periodontitis and systemic disorders, suchas diabetes,cardiovasculardisease,andmetabolicsyndromes. Thus, it is important to reestablish the stable health of periodontaltissuesafterhealing,aswellasprevent period-ontaldiseasestomaintainbothsystemicandoralhealth.
Whyisperiodontitisathighriskofrecurrence?Thereare twomajorreasons:easilyoccurringbacterialre-accumulation andtheformationofalongjunctionalepithelium(periodontal repair)aftersurgical/non-surgicalprocedures.Lindheetal.
[3]investigatedthelong-termeffectsofsurgical/non-surgical treatment over a 5-year period, and concluded that the patient’s self-plaque control, but not treatment modality, wasthecriticaldeterminantofagoodprognosisinperiodontal therapy.Bothoftheproceduresinducedhealingwithalong junctional epithelium that was easily broken by recurrent inflammation due to plaque accumulation [4]. To obtain good stability andpredictability after therapy, periodontal regenerationofdestroyedtissue,whichischaracterizedbyde novoformationofcementum,afunctionallyorganizedPDL,
alveolarbone,andgingiva,isdesirable.Clinicalresearchhas extensivelyshownthatregenerationremains the favorable outcomeoverperiodontalrepair[5,6].
Thedesiretoinducethecompleteregenerationof period-ontaltissuehasinspiredtheintroductionoftissue engineer-ingtechnologyintodentalclinics[7,8].Tissueengineeringis definedasamulti-disciplinaryfieldofmedicine,chemistry, physics,engineering,andbiology[9].Thetriadfor conven-tionalcell-basedtissueengineeringinvolvescells,signaling molecules, and scaffold/supporting matrices [10]. In this triad,theroleofthescaffold isthe‘‘niche’’ ofcells, and facilitates the attachment, migration, proliferation, and three-dimensional(3D)spatialorganizationofthecell popu-lation. However, recent progress in material sciences has providedbioactivepropertiestoscaffoldmaterialsfor trans-mittingspecificsignalsto cellsthatwilldecodethese into biochemical signals. Topography, chemistry, and physical properties are considered to be critical parameters for directing cell fate [11]. This review has focused on the following topics: (1) the current status of and strategies for periodontal regeneration; (2) a possible biomaterial designforthescaffoldusedinperiodontaltissueengineering; (3) a possible interaction between scaffold materials and periodontaltissuecells.
2.
Current
strategies
for
periodontal
regeneration
Formorethanthreedecades,periodontalresearchhasbeen attempting to discover clinical treatment regimens that canregenerateperiodontaltissueswithgoodpredictability. Thesetrialssuccessfully developedtwotypesof strategies withthecombineduseofbiomaterialsandgraftsshownin
Table1.
Anumberofanimalandhumantrialsdemonstratedthat thecombineduseofbonegrafts/implantmaterialswithflap surgerysuccessfullystimulatedalveolarboneregeneration. These grafts/materials include: (1) autogenous grafts; (2) allogeneicgraft; (3) xenogeneic grafts, and(4) alloplastic materials[12]. The use of grafts/biomaterials presumably servedas ascaffoldfor boneformationandcontainedthe bone-forming cells and bone-inducting substances that finally resulted in bone formation. The biological perfor-manceofbonegraftscanbedividedintothreeinterrelated, butnotidenticalrationales:osteogenesis(theformationof newbonebystemcelllineagederivedfromgraftmaterial); osteoinduction(bone growthbythe surroundingimmature cells recruited by graft material); and osteoconduction (bonegrowthonthesurfaceofamaterialwithfabrication)
thatcaninduceosteogenesis,andstillservesasthe‘‘golden standard’’ofbonegrafts.
Thesecondstrategyaimedatregeneratinga3Darrayed structureoflostperiodontaltissueincludingrootcementum, alveolarbone,andthePDLwiththeconnectivetissue attach-ment.Thebiologicalrationaleofthisstrategywasbasedon the ‘‘Melcher hypothesis’’ [14], which proposed that the natureoftheattachment inperiodontalhealingdepended ontheoriginofcells(epithelial,gingivalconnective,bone, PDL)repopulatingtheareaadjacenttotherootsurface.The hypothesis was successfully demonstrated in a series of animal experiments, and the principal of Guided Tissue Regeneration(GTR)wasestablished[15,16].Thecell occlu-sivemembraneofGTRfunctionstoisolatetheperiradicular bone and root surface wound area from the rest of the tissues to maintain a space for the repopulation of cells originatingfromthePDL.Forthispurpose,differentbarrier materialshavebeenused,bothnon-resorbableandresorbable (biodegradable).
TheconceptoftheGTRtechniqueonlyawaitsthe repo-pulationofPDLcellsinthewoundhealingareaanddoesnot interfere with the growth/differentiation speed of these cells. Recent biological approaches have attempted to mimic/enhance the cellular events leading to the normal development/woundhealing processofperiodontal tissues
[17].EnamelMatrixDerivative(EMD),theactivecomponent ofEmdogain1
,was the first signalingmolecule that could regenerateperiodontaltissue.Emdogain1
ispreparedfroma piglet’s unerupted teeth and has been clinically used throughouttheworldafterapprovalforthemarketinEurope (1995), the United States (1996), and Japan (1998) [18]. Amelogeninproteinsthatdominate90%ofEMDarecapable ofperiodontalregeneration,but thecontaminated amelo-blastinfunctionedsynergistically[19].Betterunderstanding of the wound healing/regeneration process has driven periodontalresearchtoevaluatetheroleofgrowthfactor, whichisendogenouslysecretedduringthewoundhealing/ regenerationprocess.Itisalsomeritoriousthatadvancesin molecularcloninghavemadeunlimitedquantitiesof recom-binant human proteins available for tissue engineering.
Variousrecombinant growthfactors werestudiedfor their periodontalregenerationabilityinvitroandinvivo.Among them,plateletderivedgrowthfactor(PDGF;GEM21S1
)and bonemorphogenicprotein-2(BMP-2;Infuse1
)havealready becomecommerciallyavailableforclinicaluseintheUnited States[20].Furthermore,fibroblastgrowthfactor(FGF)-2is beinginvestigatedinalargeclinicaltrial(PhaseIII)inJapan, and its clinical efficacy for periodontal regeneration has alreadyreported[21—23].
Ineitherapproach,thereisatherapeuticlimitationdueto themorphologyofalveolarresorptiontoobtainapredictable outcome.Bothstrategiesareonlyapplicabletoangularbony defects,andnothorizontalresorption.Theclassificationof infrabonydefectsthatreferredtothenumberofsurrounding bonywallsalsoexertedasignificantinfluenceonthesuccess andfailureofregeneration[24,25].Toovercomethese lim-itationsandachievecompleteregeneration,theintroduction ofmoderntissueengineeringtechnologiesisanticipatedin thisfield.
3.
Periodontal
tissue
engineering
Periodontal regenerationisoneoftheearliestclinical dis-ciplines that has achieved the therapeutic application of tissueengineering-basedtechnologies.Aswellastheclinical applicationofgrowthfactors (signalingmolecules), precli-nicalstudiesofcelltherapytargetedforperiodontal regen-eration have been carried out using various sources of somatic stem cells (Table 2)[9]. Somatic stem cells were obtainedfrom both dentalandnon-dental tissues: period-ontalligament-derivedstemcells(PDLSC),dentalfollicular cells (FDC), bone marrow stem cells (BMSC), and adipose stem cells (ASC). These stem cells have the capability of periodontal tissue formation as well as bone formation
[26,27]. In addition to adult/somatic stem cells, induced pluripotent stem (iPS) cells were successfully generated fromgingivalfibroblastsbytheintroductionoffourfactors (OcT3/4,Sox2,Klf4,andc-Myc),suggestingthepotentialfor itsclinicalapplicationinregenerativedentistry[28].Itisalso
Table1 Proposedstrategiesclinicallyavailableortestedforperiodontaltissuereconstruction.
1. Targetedforalveolarbonerepair 2. Targetedforperiodontaltissueregeneration (1) Autologousbonegrafts(autografts) (1) Non-resorbablecellocclusivebarriermembranes
Intra-oralgrafts Polytetrafluorethylene(ePTFE)
Extra-oralgrafts (2) Resorbablecellocclusivebarriermembranes (2) Allogenicbonegrafts(allografts) polygolicolacid/polylacticacid
Freeze-driedbonegrafts Collagenmembrane
Demineralizedbonegrafts (3) Growthfactors(bio-regeneration) (3) Xenogenicbonegrafts(xenografts) Enamelmatrixderivative(EMD)
Bovinemineralmatrix Platelet-derivedgrowthfactor(PDGF)
(4) Alloplasticbonegrafts Bonemorphogenicprotein-2(BMP-2)
Hydroxiapatite Fibroblastgrowthfactor-2(FGF-2)
b-Tricalciumphosphate Platelet-richplasma(PRP)
Bioactiveglass (4) Celltherapy
Coral-derivedcalciumcarbonate Autologoussomaticstemcells
(5) Polymerandcollagensponges Allogenicstemcells
Collagen
Hard-tissuereplacementpolymer
importantto providealargeamountofcellsatthesiteof regeneration.Forthispurpose,PDLcellsheettechnologyhas beendevelopedandsuccessfullyregeneratedbothnewbone and cementum connecting with collagen fibers in canine periodontaldefectmodels[29].However,noneofthesecell transplantationmodelsshowedthecompleteregenerationof horizontallylostperiodontaltissues.
Therefore,periodontaltissuestillremainsoneofthemost difficulttissues to achievecompleteregeneration because manyclinicalandbiologicalvariablesmayaffectthe regen-erationprocess.Firstly,thistissueisalwaysincontactwith theoutsideenvironmentoftheoralcavity,andisatriskof infectionduringtheregenerationprocess.Secondly,several typesofmechanicalstressesarealsoloadedontoperiodontal
tissue:oneisfromocclusalforcesandtheotheristhetension stressfromgingivaandmucosalmembranes,whichdisrupts horizontallyresorbedperiodontaltissue.AsshowninFig.1,it maybe difficult to overcome these environmental factors andinducecompleteperiodontalregenerationwithoutthe ‘‘golden’’triadofcell/signalingmolecule/scaffoldfor con-ventionalregenerativemedicine.Itisimportanttomaintain thespaceofhorizontallylosttissuesandprotect regenerat-ingtissuesfrominfectionandmechanicalstresses.
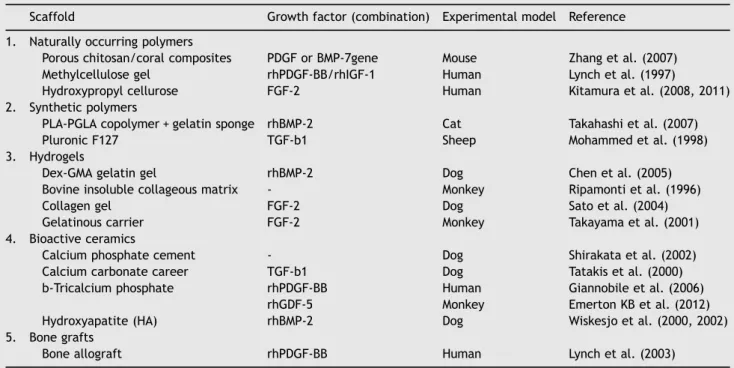
Thelastcomponentofthetissueengineeringtriadisthe scaffold.Table3showsthescaffoldmaterialsusedforgrowth factortherapyaimedatperiodontalregeneration[30]. Poly-meric scaffolds commonly have porous and biodegradable structuresfabricatedfromnatural/syntheticmaterials,and
Table2 Preclinicalapplicationofcelltherapiesforperidontalregeneration.
Celltype Cellorigin Experimentalmodel Reference
Animal Defecttype
BMSC Auto Dog ClassIIIdefects HasegawaNetal.(2006),LiHetal.(2009)
Auto Dog Fenestration YamadaYetal.(2004a)
Auto Dog,Rat Osteotomy YamadaYetal.(2004b,2004c),TobitaMetal.(2008)
ASC Auto Dog Palataldefects DoganAetal.(2003)
PDLcells Auto Rat Fenestration LekicPCetal.(2001)
Auto/Xeno Human Fenestration SeoBMetal.(2005) PDLcellsheet Auto Dog ClassIIdefects AkizukiTetal.(2005)
Auto Dog 1-Walldefects TsumanumaYetal.(2011)
PDLSC Auto Nuderat Ectopic ChangJetal.(2007)
Auto Dog,Rat Fenestration AkizukiTetal.(2005),MajewskiMetal.(2008) Auto Rat Periodontaldefects JinQMetal.(2003)
CM Allo Rat Ectopic ZhaoMetal.(2004)
DFC Allo Rat Ectopic ZhaoMetal.(2004)
ModifiedfromRiosHFetal.,JPeriodontol82:1223—1227,2011[9].
BMSC=Bonemarrowstemcells;ASC=Adiposestromalcells;PDLcells=Periodontalligamentcells;PDLSC=Periodontalligamentstem cells;CM=Cementoblasts;DFC=Dentalfolliclecell;Auto=Autograft;Allo=Allograft;Xeno=Xenograft.
havebeentailoredtofilms,fibers,sheets,gels,andsponges
[31].Inorganicmaterialsalsohavebeenusedforperiodontal regeneration to specifically regenerate alveolar bone defects, including hydroxyapatite (HA) and calcium phos-phates(CaP).CaPmaterialssuchasb-tricalciumphosphate (b-TCP) have excellent properties including: (1) a similar compositiontoboneminerals;(2)theabilityto formbone apatite-like materials or carbonate HA; (3) the ability to stimulatecells,leadingto theformationofbone-CaP; and (4)osteoconductivity[32].HAisthemajormineral compo-nent (approx. 60%) of human hard tissues, and is often clinically applied to fill alveolar bone defects (shown in
Table1).HAcaneliminatedonorsitemorbidity,butcanlead togranularmigrationandincompleteresorption,resultingin long-termdifficulties [33].b-TCPhasbeenshowntobean osteoconductivematerial,allowingforbonegrowthontothe scaffoldadjacenttobonysurfacesinbothanimalandhuman studies[34,35],andhasbeenclinicallyappliedin combina-tionwithPDGF[36].
Even if the material is a polymer or inorganic, it is expected to fill a specific anatomic defect to allow the localizationoftransplantedcells;toserveasscaffoldingfor theformationofnewtissue;toprovideanichemaintaining stem cell viability and proliferation; and to recruit host stemcellsforsubsequenthomingtothesiteofinjury[37]. Thefirstaimofthescaffoldshouldbetocontributetothe maintenance of space for horizontally lost periodontal tissues; however, no material was found to fulfill this requirement and induce complete periodontal regenera-tion.Anotherpointforsuccessfulperiodontalregeneration ishowtoprotecttheregeneratingtissuefrominfectionby oralmicroorganisms.Periodontaltissueistheonly appara-tusinwhichsoftandhardtissueattachmentsareexposed to the outside environment. In skin tissue engineering, the same property is also required; nanofibrous polymer
materialsweredevelopedtoreleaselowmolecularweight antibacterial agents during degradation [38,39]. GTR/ guided bone regeneration (GBR) procedures have been showntofail when membraneswere exposed tothe oral cavityandbecame infected[40].Toavoidcontamination, multiple studies were conducted toincorporate antibac-terial agentssuchas tetracyclinehydroxideand metroni-dazole [41]. However, no suchtrial has beencarried out to develop an anti-infective scaffold specially designed forperiodontalregeneration. Furtherexplorationof scaf-fold-basedinfectioncontrolmethodsmaycontributetothe eliminationofbacteria,resultinginthesuccessful genera-tionofnewtissue.
4.
The
desirable
properties
of
scaffolds
designed
for
periodontal
regeneration
4.1. Mimickingthestemcellnichetoalterthe regulationofstemcells
Thegoaloftissueengineeringanditsapplicationin genera-tivemedicineisthecreationoffunctionaltissuesororgans. Therefore,itisimportantnotonlytogeneratehardandsoft tissuesin periodontal regeneration,but also to mimic the attachment of both tissues. Cell-based tissue engineering requiresbothcellsfromanappropriateorigintocreatethe target organ and a 3-dimensionallydesigned scaffold that promotes cell—cell proximity and enhances self-assembly and tissue functions [42]. The ideal combination of cell andscaffold sourcesvaries in relationto thetargettissue to be created. Furthermore, recent advances in material sciencedevelopednewfeasiblebiomaterialsandfabrication techniques,resultinginthecreationoffunctional/bioactive scaffoldsthatcanactivatecellularfunctions.
Table3 Scaffoldmaterialsappliedwith/withoutsignalingmoleculesforperiodontaltissueregeneration. Scaffold Growthfactor(combination) Experimentalmodel Reference 1. Naturallyoccurringpolymers
Porouschitosan/coralcomposites PDGForBMP-7gene Mouse Zhangetal.(2007)
Methylcellulosegel rhPDGF-BB/rhIGF-1 Human Lynchetal.(1997)
Hydroxypropylcellurose FGF-2 Human Kitamuraetal.(2008,2011)
2. Syntheticpolymers
PLA-PGLAcopolymer+gelatinsponge rhBMP-2 Cat Takahashietal.(2007)
PluronicF127 TGF-b1 Sheep Mohammedetal.(1998)
3. Hydrogels
Dex-GMAgelatingel rhBMP-2 Dog Chenetal.(2005)
Bovineinsolublecollageousmatrix - Monkey Ripamontietal.(1996)
Collagengel FGF-2 Dog Satoetal.(2004)
Gelatinouscarrier FGF-2 Monkey Takayamaetal.(2001)
4. Bioactiveceramics
Calciumphosphatecement - Dog Shirakataetal.(2002)
Calciumcarbonatecareer TGF-b1 Dog Tatakisetal.(2000)
b-Tricalciumphosphate rhPDGF-BB Human Giannobileetal.(2006)
rhGDF-5 Monkey EmertonKBetal.(2012)
Hydroxyapatite(HA) rhBMP-2 Dog Wiskesjoetal.(2000,2002)
5. Bonegrafts
Boneallograft rhPDGF-BB Human Lynchetal.(2003)
Recently,theterm‘‘biomimeticism’’hasbeenintroduced intissueengineeringandreferstothecreativeinitiationof various specificbiological systems gaininginspiration from nature[43—45].Itisalsothecaseforadultstemcelltherapy becausethesecellsresideinspecializednichesthat coordi-nate self-renewal versus differentiation in vivo [46,47]. Thus, themimickingstemcellnicheisconsideredto facil-itateself-renewal(proliferation)anddifferentiationbothex vivoandinvivoaftertransplantation.
Themicroenvironmentornichesurroundingstemcellsis showninFig.2.Cytokine/growthfactorsignalingregulates the proliferation anddifferentiation of stem cells as pre-viously described. Cell—cell and cell—matrix interactions also transmit signals into stemcells, controlling stem cell functions.Cell—cellinteractionsoccurrednotonlybetween stemcells,butalsobetweenstemcellsandsupportingcells that modulate stemcell retentionandregulation. Several cellsurfaceligandsareknownfortheirassociationwithstem cell activation, including cadherins and the Notch ligand
[48,49].
The third pathway is cell—extracellular matrix (ECM) interactions, including matrix composition, stiffness, and topography.TheECMcontainsvariousproteinssuchas fibro-nectinandlaminin,aswellasproteoglycans(GAG), hyaluro-nic acid, and fibers (collagens and elastins) [50]. These components can regulate cellbehavior as well as support cellgrowthbecausestemcellsalsohavecelladhesion mole-cules, including integrins and CD44, initiate intracellular signaling, and associate with the cellular cytoskeleton
[51]. Differences in the composition and crosslink density oftheECMineachorganandtissuehavealsobeenadapted fortheirmechanicalpropertiesofstiffnessandtopography. Cells can sense and respond to various signals, consisting of biochemicalandbiophysical cues provided by theECM. In combination with the mechanical properties of cell membrane, matrix stiffness affects the proliferation and differentiationofstemcells[52—54].Cells areexposedto adiversetopographyincludingfibrousECMandmineralized
bonewitharoughsurface.TheECMpresentsvarious geome-tricallydefinedand3Dphysicalcuesintheorderofamicron andsub-micronscale,knownastopographies[55].Physical cuesinacell’ssurroundingenvironmentareintegratedand convertedtobiochemical,intracellularsignalingresponses, leadingtothemodificationofcellfunctionthroughaprocess ofmechanotransduction[56].
Oxygengradientsinthenichealsoaffectstemcell func-tion.Stemcellnichesareknowntobelocatedinlowoxygen tensionandlowpO2regions,wheretherateofcell
differ-entiationisdecreasedandproliferativepotentialisincreased
[57]. Furthermore, oxidative stress was found to suppress theE-cadherin-mediatedcell—celladhesionof hematopoie-ticstemcells(HSC)toosteoblasts,inducingtheexitofHSC fromtheniche[58].
Additionally, another cue should be added when we considereffective bone regenerationstrategies. Bone is a biocompatible and self-remodeling tissue consisting of an organicphase(mainlycollagentypeI,20%)andaninorganic phase(mainlycarbonatedhydroxyapatite,60%)[32]. Dur-ingbonemetabolism,osteoclastsreleaseCa2+andPO42 (Pi)
derived from the matrix, causing a local increase in ion concentrations in the microenvironment, which plays a roleinosteoblast proliferationanddifferentiation, aswell as on subsequent bone formation. Increased extracellular Ca2+ concentrations are potent chemical signals for cell migration anddirected growth[59,60], as well as homing signalsthatbringtogetherthedifferentcelltypesrequired fortheinitiationof boneremodeling[61].Piis alsoa reg-ulatorof osteoblast proliferation and differentiation [62], andthe highconcentration of Pi inthe microenvironment induced osteoblast apoptosisin vitro[63] and the in vivo
mineralization ofthe bone matrix [64].Moreover, specific Ca2+andPiconcentrationshavebeensuggestedtoinducethe higherproliferation andosteogenic differentiation of MSC
[65].CaPbioceramicsappeartobecandidatesfor scaffold-aimed bone tissue engineering because they can release inorganicionsduringdissolution.
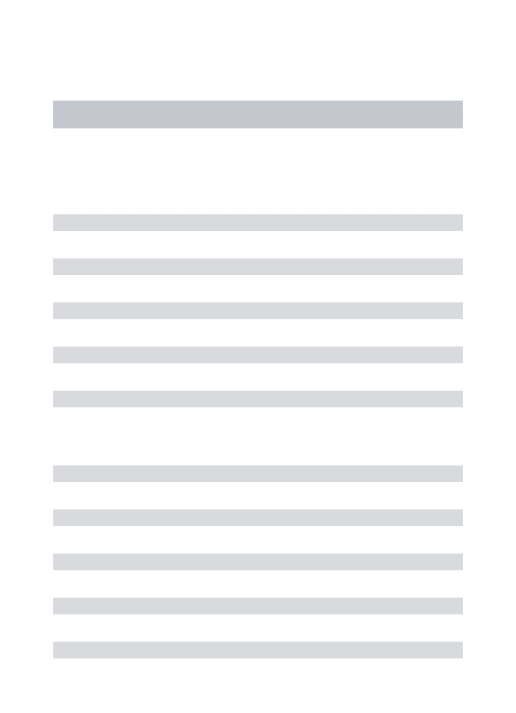
4.2. Cell—scaffoldinterplayandscaffold designing
Asdiscussedabove,manyfactorsareassociatedwith mimick-ingofthecellniche/microenvironmenttoenforce regenera-tion by the application of tissue engineering. Not only scaffoldpropertiesaffectstemcellfunctions;cellscanalso inducethedeformationanddegradationofscaffoldsduring theprocessofregeneration,leadingtothealtered mechan-icalpropertiesofscaffolds(Fig.3).Thus,thecell—scaffold interplayisbidirectionalandinvolvesafeedbackloopofcells andscaffolds. Forces are generatedin the contextof cell adhesiontoECM/scaffolds,andmechanotransductionoccurs totransducethemintointracellularsignalsthatdrive func-tional modulations in cells: proliferation, differentiation, migration,andapoptosis[55].Theactincytoskeletonplays themostprominentroleinthese events [66]. HumanMSC alsoexpressspecifictranscriptionfactorsof mechanotrans-ductionandundergotissue-specificcellfateswitcheswhen cultured on ECMs with mechanical stiffness mirroring the physicalpropertiesofrespectivespecifictissue[67].
To instruct stem cells and modify their fates, scaffold biomaterialshould provide informative microenvironments mimickingaphysiologicalnicheofthetargettissue. Bioma-terialscanhaveasuitabledesigntotransmitspecificsignals tocellsthatcanbedecodedintobiochemicalsignals depend-ingonitscompositionandprocessingmethods.Both biophy-sicalandbiochemicalcueshavebeeninvolvedincell—ECM interactions in nature. Hence, topography, chemistry and physicalpropertiesare involvedandare criticalfor deter-miningcellfate[68].Toaccomplishthedesirableinterplay between cells, biomaterial designingshould include para-meterswithin(a)surface,(b)mechanical,(c)morphological, and(d)electricalproperties(Fig.3).Surfacetopographyand chemicalcompositionwereabletodrivecelladhesion, pro-liferation, migration, and differentiation [55,69,70]. Stem cellscanalso respondtothe mechanicalpropertiesofthe substrate, which were enhanced by the combination of polymersandorganic/inorganicfillers[33,71],and osteoin-ductionwithoutthesupplementationofgrowthfactors has recently been reported [72]. Conductive nanostructures, such as metal nanoparticles and carbon nanostructures,
may modulate the electrical properties of biomaterials, affectingstemcellfunctions[73,74].Scaffold morphology, e.g., pore size and shape, is critical for cell—biomaterial interactions in terms ofmimicking themorphologyof sur-roundingtissue.Highporosityandanadequateporesizein particulararekeyconditionsforincreasingthesurfacearea availablefor cellattachment andgrowth. Inthefollowing sections,theinteractionsbetweenPDLcellsandeach para-meterofthescaffolddesigndiscussedabovewillbecovered indetailusingourfindings.
4.3. Applicationofahoneycombmicroarrayfilm forPDL cellsheetengineering
Cellsheettechnologyisaconceptoftissueengineeringthat providesa massofcellsto thesiteofregenerationbythe transplantation of an in vitro cultured multilayered cell sheet. This technology has already been applied to the regeneration ofmany organsin clinical settings, including corneal surface reconstruction, endoscopic treatment of esophagealulceration,andmyocardialtissuereconstruction
[75].ThecellsheetwassuccessfullypreparedfromPDLcells, andscaffold-freesheet transplantationcould regeneratea complete periodontiumin acanine model[29]. Cellsheet engineeringisalsoapplicableto3D-tissuereconstructionof tissue by applying an appropriate scaffold material to increasethenumberofcelllayers[76].Skinreconstruction isanothermedicalfieldapplicabletocellsheet-basedtissue engineering. The honeycomb biodegradable collagen scaf-foldhasbeenshowntobesuitablefor3Dcellcultures[77]
becausethehoneycombstructurehasmanyadvantages,such asmechanicalstabilityundervariousphysicalconditions,the capabilitytoexchangenutrientsandwasteproductsthrough thehoneycombpores,andtheabilitytoretainitsstructure withoutadeformityorcollapseuntilitsbiodegradation[78]. However,theporesizeofnaturalpolymerssuchascollagenis difficulttocontrol.
The honeycomb pattern was also prepared on various types of polymers by a simple casting method [79—81]. Briefly, thehydrophobic polymersolution was casted on a basalplate,waterdroplets self-assembledon thepolymer solutionwiththeadditionofhumidair,andthehoneycomb
patternwasobservedonthepolymerfilmafterdrying.We couldcontroltheporesizeofthehoneycombstructureand fabricateuniformporesusingthecastingmethod.This cast-ingmethod is applicablefor biodegradable polyester films madefrompoly(lacticacid)andpoly(e-caprolactone)(PCL)
[82],whichisusefulasacellculturesubstrate.
WeculturedPDLcellsonthehoneycomb-patterned poly-merfilms fabricatedby thecastingmethod withdifferent poresizes.PDL cellswereobtainedfrom extractedmolars withahealthyperiodontium,andsubjectedtoexperiments during3—5passages.PDLcellswereculturedonflat(control) andhoneycombPCLfilmswith5-and10-mmporesfor72h. Scanning electronmicroscopy(SEM) imageswereshown in
Fig.4.PDLcellsseemedtobespreadonflatfilms(Fig.4A), althoughtheyfirmlycaughtthepillarstructureofthe hon-eycombonthe5mm-poredfilm(Fig.4B).Interestingly,PDL cellsmigratedthroughtheporesofthehoneycombstructure ofthe10mmfilm(Fig.4C).TheschematicillustrationsofPDL cell behavior cultured on 5 and 10mm-pored honeycomb filmsweregiveninFig.4DandE,respectively.
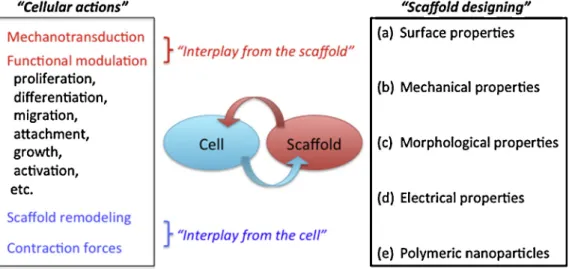
The3DorientationsofPDLcellsinthehoneycombfilms werefurther observedusingconfocallaserscanning micro-scopy after a long-term culture (28 days; Fig. 5).Fig. 5A showsthe3D-constructedimageofPDLcellsculturedonthe 10mm-pored film.PDL cellswere seeninside thefilmand spreadtheirbodieshorizontallyintothecontiguouslylined pores. PDL cells constructed multi-layered cell sheet-like structuresafter28days,andtheshapesofcellsontheupper celllayer,onthesurface,andinsideofthefilmwere sepa-ratelypresentedinFig.5B—D.Theshapesandformsofthe cellsweremarkedlyexchangedbymovingbetweenthe out-sideandinsideofthehoneycombfilms.PDLcellsseemedto bedesperate to movethroughthehoneycomb lumensand showedadendrite-likemorphologyform.Ourresultsclearly indicated that the pore size of artificial substrates has a markedeffectoncellbehavior,andthehoneycombstructure
issuitablefortheconstructionofamulti-layeredcellsheet. Thetopographicaleffectsofthehoneycombfilmalsohavea significantimpactonPDLcelldifferentiation.Wemeasured themRNAexpression levelsof theosteoblastic markersof PDLcellsculturedfor4weeksonthehoneycombfilm[83]. Osteopontin(OPN)andosteocalcin (OCN)expressionlevels werehigherthanthoseonflatfilms,suggesting differentia-tionintoosteoblasticcells.Thisresultwasfurtherconfirmed bytheformationofcalcified noduleson 10mm-pored hon-eycombfilms(datanotshown).
4.4. Possible inductionofcementogenesis bymodulationoftheextracellular ionic microenvironmentusingbioactive ceramic scaffolds
Toaccomplishtherestorationoftheoriginalarchitectureof theperiodontalapparatus,itisimportanttopromote cemen-togenesis rapidly on the root surfaceafter root planning/ conditioningbecausethecementumistheonlyhardtissue thatcaninsertPDLsandassistsinanchoringthetoothtothe surroundingalveolarbone[84].Cementoblastsexpress alka-linephosphatase(ALP),runt-relatedgene2,typeIcollagen, noncollagenousproteins,bonesialoprotein(BSP),andOCNin a similar manner to osteoblasts [84,85]. According to the anatomical location, whichis in proximity to osteoblasts/ alveolarbone,butisseparatedbyaPDL,cementoblastsmay beunderaspecificmicroenvironmentresemblingbonewith higher extracellular Ca2+ and Pi concentrations in part relatedtoosteoclast-mediatedboneresorptionduring alveo-lar bone remodeling. Thus, these cells are physiologically and/or pathologically confronted with alterations in the concentrations of extracellular inorganic ions. Calcium phosphate ceramics are widely used as bone substitutes or scaffolds in dental fields because of their excellent
Figure4 SEMimagesofPDLcellsculturedonhoneycomb(HF)films.Periodontalligament(PDL)cellswereculturedfor72hon(A):a flatPCLfilm,(B):a5mm-poredhoneycombfilm(HF),and(C):a10mm-poredHF.DandEshowtheschematicillustrationofPDLcellson 5mm-and10mm-HF,respectively.
osteoconductivity[86].Theseceramicsareclassifiedas non-resorbableandresorbable,andcanreleaseorexchangeCa2+
andPiionsintotheirsurroundingsafterimplantation[87]as discussed in the previous section. Whether cementoblasts couldsenseextracellularCa2+andPiionicconcentrationsand
alteredcellfunctionssuchascementogenesisandcytokine productionremainedunclear[88].Animmortalizedmurine cementoblastcellline(OCCM-30),establishedbythe isola-tionoftoothroot-surfacecellsfromtransgenicmice contain-ing a SV40 large T-antigen under the control of the OCN promoter[89], was used for the followingstudies. OCCM-30cellswerestimulatedwith10mMCaCl2for24hbecause
basal[Ca2+]was1.8mM.TheexpressionofCOX-2andPGE2
wassignificantlyincreasedinatime-dependentmannerand
subsequently increased Fgf-2 mRNA (Fig. 6). OCCM-30 expressedallEP1,EP2,EP3,andEP4receptorstoPGE2.Only
an EP4 receptor agonist synergistically enhanced CaCl2
-inducedFgf-2geneexpression(datanotshown).Wefinally concluded that the exposure of cementoblasts to CaCl2
activated NF-kB signaling and induced the expression of
Cox-2aswellasEp4,whichledtothesequentialactivation ofPGE2/EP4signalingandincreaseinFgf-2expressionlevels
(Fig.7).COX-2/PGE2/EP4signalingmayfunctionasapositive
regulator for FGF-2 induction in cementoblasts. We pre-viouslyreportedthatincreasedextracellularCa2+increased BMP-2mRNAexpressioninhumanPDLcellsaswellasinthe dentalpulp(DP)cells[90].Furthermore,hDPandPDLcells expressed Na-dependent Pi transporters (Pit-1, Pit-2) and
Figure5 Confocal laser microscopy images of PDL cells cultured for 28 days ona 10mm-pored honeycomb film. (A) Three-dimensionalreconstructedimageofverticalslices,(B—D)PDLcellsonthetopofmultilayeredcells(B),centerofcelllayers(C),and insideofthehoneycombfilm(D),respectively.
Figure6 ElevatedconcentrationsofextracellularCa2+inducedCox-2mRNAexpressionandPGE
2production,andsubsequently up-regulatedtheexpressionofFgf-2mRNA.
sensedextracellularPi,resultingintheup-regulationof BMP-2 mRNA[91].Taken together,periodontal anddental pulp cellscan respondto changes inextracellularinorganicion concentrations,resultinginthesignaltransductionthatleads toproliferation/differentiation.
4.5. Application ofnanofabricated
hydroxyapatiteforbone tissueengineering
Hydroxyapatite(HA)istheprevalentformofCaPfoundinthe bone;therefore,ithasbeenusedasthestablealloplastand scaffold for bone regeneration. However, HA has a lower dissolutionrateatphysiologicalpH(7.2—7.6)thantheother types of CaP such as octacalcium phosphate (OCP) and tricalcium phosphate (TCP), resulting in poor biological responses.Asthisdissolutionbehaviorhasbeenassociated with osteoinductivity, previous studies attempted to engi-neerCaPwithanappropriatelyhighsolubility[87]. Combin-ing the different scaffold fabrication technologies and different biomaterials can provide cells with mechanical, physicochemical, and biological cues at the macro- and micro-scale,aswellasatthenano-scale.Duetosizeeffects andsurfacephenomenaatthenanoscale,nanosizeHA (nano-HA)possesseduniquepropertiesoveritsbulk-phase counter-part. The high surface-to-volume ratio, reactivities, and biomimeticmorphologiesmaymakenano-HAmorefavorable inapplicationsforbonetissueengineering[92,93].We inves-tigatedtheeffectofnano-HAonBMP-2expressioninhuman PDLcells[94].Nano-HAselectivelyincreasedtheexpression ofBMP-2indose-andtime-dependentmanners(Fig.8Aand B)atmRNA andprotein levels,butnotofBMP-4,-7,or-9 (Fig.8C).However,concentrationsofCa2+aswellasPiwere notchangedinculturesupernatants(Fig.9),suggestingthat nano-HAfunctionedasananoparticleratherthanasa pos-siblesource of Ca2+ and/or Piextracellularly, which were
Figure7 IncreasedextracellularCa2+synergistically up-regu-lated FGF-2expression via COX-2/PGE2/EP4 signaling,COX-2: cyclooxygenase-2,EP4:EP4receptor.
Figure8 Nano-HAstimulatedBMP-2expressionatthegenelevelinhumanPDLcells.(A)Cellswerestimulatedwiththeindicated concentrationofnano-HAfor72h.(B)Cellswerestimulatedwith200mg/mlnano-HAfortheindicatedtimeswithamediumchange every3days. (D)Cellswerestimulatedwith200mg/mlnano-HAfor72h. TotalcellularRNAwasextractedandtranscriptswere analyzedbyreal-timePCR.
Figure9 Nano-HAmediatedincreasesinBMP-2werenotcausedbyextracellularCa2+orPi.(A)Cellswerestimulatedwith/without 200mg/mlnano-HA,10mMCaCl2,or3mMPi(asamixtureofNaH2PO4andNa2HPO4,pH7.4)fortheindicatedtimes.TotalcellularRNA wasextractedandtranscriptswereanalyzedbyreal-timePCR.(BandC)Confluentcellswerestimulatedwith/without200mg/ml nano-HAfortheindicatedtimes.TheconcentrationsofCa2+andPiinthesupernatantweremeasured.
showntoalsoenhancetheexpressionofBMP-2inPDLcells. Wefurtherrevealedthatnano-HA-dependentBMP-2 expres-sionwasdependentonp38MAPkinase,butnoton ERK1/2 MAPkinase(datanotshown).Thus,nano-fabricatedHAmay regulatethedifferentiationofhPDLcellsviaa mechanosen-sitivesignalingpathway.Thisnovelmechanismoftheaction ofnano-HAmayofferthepromiseofnewstrategiesforbone andperiodontaltissueengineering.
5.
Conclusions
and
future
prospects
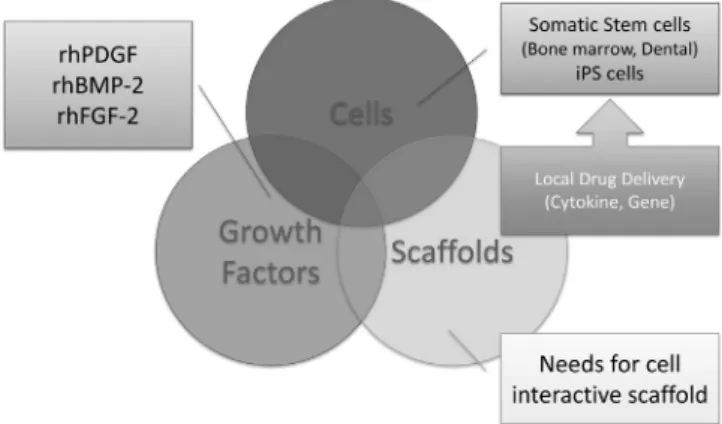
Thisreviewfocusedonthecell—scaffoldinteractionpossibly encountered when tissue-engineering approaches are applied to periodontal regeneration. Recent progresses in periodontal regeneration technology allowed the clinical applicationofcytokinetherapiesindentalclinics.However, asdiscussedintheprevioussections,thesecytokine thera-pies still have therapeutic limitations similar to those of EmdogainandtheGTRtechnique.Toovercome the limita-tions,researchershaveextensivelystudiedtheapplicationof stemcelltherapyinthisfield,includingautologoussomatic stemcellsfromadentaloriginandiPScells.Currentprogress intissueengineering approachesfor periodontal regenera-tion has been summarized in Fig. 10. The biocompatible scaffoldisanotherimportantstrategyintissueengineering technologythathasbeen adoptedforthe creationof new tissue,whetherstemcellsareutilizedornot.Scaffoldsnot onlycancontainstemcellsandmimicthemicroenvironment suitableforthesecells,butalsocanprovidethecontrolled release of growth factors including gene delivery [95]. Furthermore, the scaffold should fill a specific anatomic spaceof the lost periodontal tissue including horizontally resorbedalveolarbone.Thus,a3Dversionofbiomimicryis thekeyforcompleteperiodontalregeneration,althoughthis researchfieldiscurrentlyunderintenseexploration.
Wediscussedthepossibleperiodontalcell—scaffold inter-actionsthatmaybeapowerfultoolfordevelopingthemost suitable scaffold. To date, many cellular and molecular events involved in periodontal tissue repair/regeneration havebeenrevealed.Theseadvancesinunderstandingmay serveas thedrivingforce toward abreakthrough for cell-basedregenerationstrategiesinourresearchfield.Therapid progress in material sciences and micro/nano-fabrication
technology alsopave thewayfor thedevelopmentofnew tissue engineering techniques for ‘‘complete’’ periodontal regeneration.
Conflict
of
interest
None of authors havea conflictof interestrelated to this review.
Acknowledgements
Portions of the author’s research discussed in this review were supported by A Grant-in Aid for Scientific Research (23390745 and 23659910 to H.S.).The authors would like tothankDrs.SousukeKanaya,NagayoshiIwama,andMizuki Suto for their contributions in the research results shown here.
References
[1] PihlstromBI,MichalowiczBS,JohnsonNW.Periodontaldisease. Lancet2005;366:1809—20.
[2] EkePI,DyeBA,WeiL,Thornton-EvansGO,GencoRJ,BeckJ, etal.PrevalenceofperiodontitisinadultsintheUnitedStates: 2009and2010.JDentRes2012;91:914—20.
[3] LindheJ,WestfeltE,NymanS,SocranskySS,HaffajeeAD. Long-termeffectofsurgical/non-surgicaltreatmentofperiodontal disease.JClinPeriodontol1984;11:448—58.
[4] Wikesjo¨ UME,Nilve´usRE,SelvigKA.Significanceofearlyhealing eventsonperiodontalrepair:areview.JPeriodontol1992;63: 158—65.
[5] KoopR,MerhebJ,QuirynenM.Periodontalregenerationwith enamelmatrixderivativeinreconstructiveperiodontal thera-py:asystematicreview.JPeriodontol2012;83:707—20. [6] NeedlemanIG,WorthingtonHV,Giedrys-LeeperTE,TuckerRJ.
Guidedtissueregenerationforperiodontalinfra-bonydefects. CochraneDatabaseSystRev2006;19:CD001724.
[7] RosaV,BonaAD,CavalcantiBN,No¨rJQ.Tissueengineering: fromresearchtodentalclinics.DentMater2012;28:341—8. [8] IzumiY,AokiA,YamadaY,KobayashiH,IwataT,AkizukiT,etal.
Currentandfutureperiodontaltissueengineering.Periodontology 20002011;56:166—87.
[9] RiosHF,LinZ,OhB-N,ParkCH,GiannobileWV.Cell-and gene-basedtherapeuticstrategiesforperiodontalregenerative med-icine.JPeriodontol2011;82:1223—7.
[10] Langer R, VacantiJP. Tissue engineering. Science 1993;260: 920—6.
[11] DellatoreSM,GarciaAS,MillerWM.Mimickingstemcellnicheto increasestemcell expansion.CurrOpinBiotechnol 2008;19: 534—40.
[12] RamseierCA,RasperiniG,BatiaS,GiannobileWM.Advanced reconstructive technologies for periodontal tissue repair. Periodontology20002012;59:185—202.
[13] ReyboldsMA,Aichelmann-reidyME,Branch-MaysGL. Regener-ationofperiodontaltissue:bonereplacementgrafts.DenClin NorthAm2010;54:55—71.
[14] MelcherAH.Ontherepairpotentialofperiodontaltissues.J Periodontol1976;47:255—60.
[15] KarringT,NymanS,GottowJ,LaurellL.developmentofthe biological concept ofguided tissue regeneration-animaland humanstudies.Periodontology20001993;1:26—35.
[16] LindeA,AlberiusP,DahlinC,BjurstamK,SundinY. Osteocor-poration:asofttissueexclusionprincipleusingamembranefor bone healing and bone neogenesis. J Periodontol 1993;64: 1111128.
Figure10 Currentprogressinthedevelopmentofthetriadfor periodontaltissueengineering.
[17] KaoRT,MurakamiS,BeirneOR.Theuseofbiologicmediators and tissue engineering in dentistry. Periodontol 2000 2009; 50:127—53.
[18] GrandinHM,GemperliAC,DardM.Enamelmatrixderivative:a reviewofcellulareffectsinvitroand amodelofmolecular arrangement and functioning. Tissue Eng Part B 2012;18: 181—90.
[19] BrookesSJ,RobinsonC,KirkhamJ,BonassWA.Biochemistryand molecularbiology ofamelogeninproteins ofdentalenamel. ArchOralBiol1995;40:1—14.
[20] PelleggriniG,Seol YJ,GruberR, GiannobileWV.Pre-clinical models for oraland periodontal reconstructive therapies. J DentRes2009;88:1065—76.
[21] Kitamura M, Nakashima K, Kowashi Y, Fujii T, Shimauchi H, SasanoT,etal.Periodontaltissueregenerationusingfibroblast growthfactor-2:randomizedcontrolledphaseIIclinicaltrial. PLoS ONE 2008;3:e2611. http://dx.doi.org/10.1371/journal. pone.0002611.
[22] KitamuraM,AkamatsuM,MachigashiraM,HaraY,SakagamiR, HirofujiT, etal. FGF-2stimulatesperiodontalregeneration: resultsofamulti-centerrandomizedclinicaltrial.JDentRes 2011;90:35—40.
[23] MurakamiS.Periodontaltissueregenerationbysignaling mole-cule(s):whatroledoesbasicfibroblastgrowthfactor(FGF-2) haveinperiodontaltherapy?Periodontology20002011;56:188— 208.
[24] CortelliniP,PiniPratoG,TonettiMS.Periodontalregeneration ofhumaninfrabonydefects.I.Clinicalmeasures.JPeriodontol 1993;64:254—60.
[25] CortelliniP,PiniPratoG,TonettiMS.Periodontalregeneration ofhumaninfrabonydefects,II.Re-entryproceduresandbone measures.JPeriodontol1993;64:261—8.
[26] HynesK,MenicaninD,GronthosS,BartordPM.Clinicalutilityof stemcellsforperiodontalregeneration.Periodontology2000 2012;59:203—27.
[27] EgusaH,SonoyamaW,NishimuraM,AtsutaI,AkiyamaK.Stem cellsindentistry—PartI:stemcellssources.JProthodRes 2012;56:151—65.
[28] EgusaH,OkitaK,KayashimaH,YuG,FukuyasuS,SaekiM,etal. Gingivalfibroblastsasapromisingsourceofinducedpluripotent stemcells.PLoSONE2010;5:e12743.http://dx.doi.org/10.1371/ journal.pone.0012743.
[29] TsumanumaY,IwataT,WashioK,YoshidaT,YamadaA,TakagiR, etal.Comparisonofdifferenttissue-derivedstemcellsheets forperiodontalregenerationinacanine1-walldefectmodel. Biotechnology2011;32:5819—25.
[30] ChenF-M,JinY.Periodontaltissueengineeringand regenera-tion:currentapproachesandexpandingopportunities.Tissue EngPartB2010;16:219—55.
[31] MartinoS,D’AngeloF,ArmentanoI,KennyJM,OrlacchioA.Stem cell—cellbiomaterialinteractionsfor regenerativemedicine. BiotechnolAdv2012;30:338—51.
[32] ChaiYC,CarlierA,BolanderJ,RobertsSJ,GerisL,SchrootenJ, etal.Currentviewsoncalciumphosphateosteogenicityandthe translation intoeffectiveboneregenerationstrategies. Acta Biomater2012;8:3876—87.
[33] Wagoner-JohnsonAJ,HelshelerAJ.Areviewofthemechanical behaviorofCaPandCaP/polymercompositesforapplicationsin bonereplacementandrepair.ActaBiomater2011;7:16—30. [34] LeGerosRZ.Propertiesofosteoconductivebiomaterials:
calci-umphosphates.ClinOrthop2002;395:81—98.
[35] OgoseA,HottaT,KawashimaH,KondoN,GuW,KamuraT,etal. Comparisonofhydroxyapatiteandbetatricalciumphosphateas bonesubstitutesafterexcisionofbonetumors.JBiomedMater ResBApplBiomater2005;72:94—101.
[36] SarmentDP,CookeJW,MillerSE,JinQ,McGuireMK,KaoRT, etal.EffectofrhPDGF-BBonboneturnoverduringperiodontal repair.JClinPeriodontol2006;33:135—40.
[37] DischerDE,MooneyDJ,ZandstraPW.Growthfactors,matrices, andforcescombineandcontrolstemcells.Science2009;324: 1673—7.
[38] ShalumonKT,AnulekhaKH,ChennazhiKP,TamuraH,NairSV, JayakumarR.Fabricationofchitosan/poly(caprolactone) nano-fibrousscaffoldforboneandskintissueengineering.IntJBiol Macromol2011;48:571—6.
[39] JinG,PrabhakaranMP,RamakrishnaS.Stemcelldifferentiation toepidermallineagesonelectrospunnanofibroussubstratesfor skintissueengineering.ActaBiomater2012;7:3113—22. [40] TonettiMS,PratoGP,CortelliniP.Factorsaffectingthehealing
responseofintrabonydefectsfollowingguidedtissue regenera-tionandaccessflapsurgery.JClinPeriodontol1996;23:548—56. [41] BottinoMC,ThomasV,SchmidtG,VohraYK,ChuTM,Kowolik MJ,et al.Recent advances inthedevelopmentofGTR/BBR membraneforperiodontalregeneration—amaterial perspec-tive.DentMater2012;28:703—21.
[42] LevenbergS,LangerR.Advancesintissueengineering.CurrTop DevBiol2004;61:113—34.
[43] SarikayaM.Biomimetics:materialfabricationthroughbiology. ProcNatlAcadSciUSA1999;96:14183—5.
[44] SandezC, ArribartH, GuilleMMG.Biomimeticismand bioin-spiration as tool for the designof innovative material and systems.NatMater2005;4:277—88.
[45] TamerlerC,SarikayaM.Moleculerbiomimetics:utilizing nat-ure’smolecularwaysinpracticalengineering.ActaBiomater 2007;3:289—99.
[46] FuchsE,TumbarT,GuaschG.Socializingwithneighbors:atem cellandtheirniche.Cell2004;116:769—78.
[47] MorrisonSJ,SpradlingAC.Stemcellsandniche:mechanisms that promote stem cell maintenance throughout life. Cell 2008;132:598—611.
[48] Jin Z,KirillyD,Weng C, Kawase E, SongX,Smith S,et al. Differentiation-defectivestemcellsoutcompetenormalstem cellsfornicheoccupancyintheDrosophilaovary.CellStemCell 2008;2:39—49.
[49] HinesM,NielsenL,Cooper-WhiteJ.Thehematopoieticstem cellniche:whatare wetryingtoreplicate?JChemTechnol Biotechnol2008;83:421—43.
[50]MuiznieksLD,KeeleyFW.Molecularassemblyandmechanical properties of the extracellular matrix: a fibrous protein perspective. Biochim Biophys Acta 2012 [pii: S0925-4439(12)00283-289].
[51] KimSH,TurnbullJ,GuimondS.Extracellularmatrixandcell signalling:thedynamiccooperationofintegrin,proteoglycan andgrowthfactorreceptor.JEndocrinol2011;209:139—51. [52] EdalatF, Bae H, Manoucheri S, ChaJM, Khademhosseini A.
Engineeringapproachestowarddeconstructingandcontrolling instemcells.AnnBioemedEng2012;40:1301—15.
[53] HsiongSX,CarampinP,KongHJ,LeeKY,MooneyDJ. Differenti-ationstagealtersmatrixcontrolofstemcells.JBiomedMater ResPartA2008;85A:145—56.
[54] EnglerAj,SenS,SweeneyHL,DischerDE.Matrixelacitydirects stemcelllineagespecification.Cell2006;126:677—89. [55] NikkhahM,EdalatF,ManoucheriS,KhademhosseniA.
Engineer-ingmicroscaletopographiestocontrolthecell—substrate in-terface.Biomaterials2012;33:5230—46.
[56] NavaMM,RaimondiMT,PietrabissaR.Controllingself-renewal anddifferentiationofstemcellsviamechanicalcues.JBiomed Biotechnol 2012;2012:797410. http://dx.doi.org/10.1155/ 2012/797410.
[57] King JA, Miller WM. Bioreactor development for stem cells expansionandcontrolleddifferentiation.CurrOpinChemBiol 2007;11:394—8.
[58] HosokawaK,AraiF,YoshiharaH,NakamuraY,GomeiY,Iwasaki H, et al. Function of oxidative stress in the regulation of hematopoieticstemcell—nicheinteraction.BiochemBiophys ResCommun2007;363:578—83.
[59] LiuHW,LuoYC,HoCL,YangJY,LinCH.PLocomotionguidance byextracellularmatrixisadaptiveandcanberestoredbya transientchangeinCa2+level.PLoSONE2009;4:e7330.http:// dx.doi.org/10.1371/journal.pone.0007330.
[60] AdamsGB,ChabnerKT,AlleyIR,OlsonDP,SzczepiorkowskiZM, PoznanskyMC,etal.Stemcellengraftmentattheendosteal niche is specified by the calcium-sensing receptor. Nature 2006;439:599—603.
[61] BreitwieserGE.Extracellularcalciumasanintegratoroftissue function.IntJBiochemCellBiol2008;40:1467—80.
[62] BeckJrGR.Inorganicphosphatesignalingmoleculein osteo-blastdifferentiation.JCellBiochem2003;90:234—43. [63] LiuYK,LuQZ,PeiR,JiHJ,ZhouGS,ZhaoXL,etal.Theeffectof
extracellularcalciumandinorganicphosphateonthegrowthand osteogenic differentiationof mesenchymal stemcellsinvitro: implication for bone tissue engineering. Biomed Mater 2009; 4:025004.http://dx.doi.org/10.1088/1748-6041/4/2/025004. [64] MurshedM,HarmeyD,Milla´nJL,McKeeMD.Unique
coexpres-sioninosteoblastsofbroadlyexpressedgenesaccountsforthe spatialrestrictionofECMmineralization tobone.GenesDev 2005;19:1093—104.
[65] Chai YC, Roberts SJ, Schrooten J, Luyten FP. Probing the osteoinductiveeffectofcalciumphosphatebyusinganinvitro biomimeticmodel.TissueEngPartA2011;17:1083—97. [66] SchwarzUS,GardelML.Unitedwestand:integratingtheactin
cytoskeletonandcell—matrixadhesionsincellular mechano-transduction.JCellSci2012;125:3051—60.
[67] TitushkinIA,ShinJ,ChoM.Anewperspectiveforstem-cell mechanobiology:biomechanicalcontrolofstem-cellbehavior andfate.CritRevBiomedEng2010;38:393—433.
[68] KumariA,YadavSK,YadavSC.Biodegradablepolymeric nano-particlesbaseddrugdeliverysystems.ColloidsSurfB Biointer-faces2010;75:1—18.
[69] D’AngeloF,ArmentanoI,MattioliS,CrispoltoniL,TiribuziR, Cerulli GG, et al. Micropatterned hydrogenated amorphous carbonguidesmesenchymalstemcellstowardsneuronal dif-ferentiation.EurCellMater2010;20:231—44.
[70] McPheeG,DalbyMJ,RiehleM,YinH.Cancommonadhesion molecules and microtopographyaffect cellular elasticity? A combinedatomicforcemicroscopyandopticalstudy. MedBiol EngComput2010;48:1043—53.
[71] GupteMJ,MaPX.Nanofibrousscaffoldsfordentaland cranio-facialapplication.JDentRes2012;91:227—34.
[72] PoliniA,PisignanoD,ParodiM,QuartoR,ScaglioneS. Osteoin-ductionofhumanmesenchymalstemcellsbybioactive com-posite scaffolds without supplemental osteogenic growth factors.PLoSONE2011;6:e26211.http://dx.doi.org/10.1371/ journal.pone.0026211.
[73] SunS,TitushkinI,ChoM.Regulationofmesenchymalstemcell adhesionandorientationin3Dcollagenscaffoldbyelectrical stimulus.Bioelectrochemistry2006;69:133—41.
[74] NaingMW,Williams DJ.Three-dimensional cultureand bior-eactorsforcellulartherapies.Cytotherapy2011;13:391—9. [75] Elloumi-HannachiI,YamatoM,OkanoT.Cellsheetengineering:
auniquenanotechnologyforscaffold-freetissuereconstruction with clinicalapplications inregenerativemedicine.JIntern Med2010;267:54—70.
[76] YangJ,YamatoM,NishidaK,OhkiT,KanzakiM,SekineH,etal. Celldeliveryinregenerativemedicine:thecellsheet engineer-ingapproach.JControlRelease2006;116:193—203.
[77] George J, Onodera J, Miyata T. Biodegradable honeycomb collagenscaffoldfordermaltissueengineering.JBiomedMater ResA2008;87:1103—11.
[78] Itoh H,Aso Y, FuruseM, Noishiki Y, MiyataT. A honeycomb collagencarrierforcellcultureasatissueengineeringscaffold. ArtifOrgans2001;25:213—7.
[79] Hutmacher DW,SchantzT, ZeinI,NgKW, TeohSH,Tan KC. Mechanicalpropertiesandcellculturalresponseof polycapro-lactonescaffoldsdesignedandfabricatedviafuseddeposition modeling.JBiomedMaterRes2001;55:203—16.
[80] BeattieD,Wong KH,WilliamsC, Poole-WarrenLA, DavisTP, Barner-KowollikC,et al.Honeycomb-structuredporousfilms from polypyrrole-containing block copolymers prepared via RAFTpolymerizationasascaffoldforcellgrowth. Biomacro-molecules2006;7:1072—82.
[81] ZhaoM,LiL,LiX,ZhouC,LiB.Three-dimensional honeycomb-patternedchitosan/poly(L-lacticacid)scaffoldswithimproved
mechanical and cell compatibility. J Biomed Mater Res A 2011;98:434—41.
[82] Fukuhira Y, Kitazono E, Hayashi T, Kaneko H, Tanaka M, ShimomuraM,etal.Biodegradablehoneycomb-patternedfilm composedofpoly(lacticacid)and dioleoylphosphatidylethano-lamine.Biomaterials2006;27:1797—802.
[83] MiranRJ,ZhangYF.Osteoinduction:areviewofoldconcepts withnewstandards.JDentRes2012;91:736—44.
[84] ZeichnerM-D. Regenerationofperiodontaltissues: cemento-genesisrevisited.Periodontology20002006;41:196—217. [85] BronckersALJI,Farach-CarsonMC,VanWaverenE,ButlerWT.
Immunolocalization of osteopontin, osteocalcin, and dentin sialoproteinsduringdentalrootformationandearly cemento-genesis.JBoneMineralRes1994;9:833—41.
[86] El-GhannamA.Bonereconstruction:frombioceramicstotissue engineering.ExpertRevMedDevices2005;2:87—101. [87] SuzukiO.Octacalciumphosphate:osteoconductivityand
crys-talchemistry.ActaBiomater2010;6:3379—87.
[88] Kanaya S, NemotoE,Ebe Y,Sommerman MJ,Shimauchi H. Elevated extracellular calcium increases fibroblast growth factor-2 gene and protein expression levels via a cAMP/ PKA dependent pathway in cementoblasts. Bone 2010;47: 564—72.
[89] D’Errico JA, Berry JE, Ouyang H, Strayhorn CL, Windle JJ, SomermanMJ,etal.Employingatransgenicanimalmodelto obtaincementoblastsinvitro.JPeriodontol2000;71:63—72. [90] TadaH,NemotoE,KanayaS,HamajiN,SatoH,ShimauchiH.
Elevated extracellular calcium increases expressionof bone morphogeneticprotein-2geneviaacalciumchannelandERK pathway in human dental pulp cells. Biochem Biophys Res Commun2010;394:1093—7.
[91] Tada H, Nemoto E,Foster BL, Somerman MJ, Shimauchi H. Phosphateincreasesbonemorphogeneticprotein-2expression throughcAMP-dependentproteinkinaseandERK1/2pathways inhumandentalpulpcells.Bone2011;48:1409—16.
[92] Venugopal J, Prabhakaran MP, Zhang Y, Low S, Choon AT, RamakrishnaS.Biomimetichydroxyapatite-containing compos-itenanofibroussubstratesforbonetissueengineering.Philos TransAMathPhysEngSci2010;368:2065—81.
[93] Zhou H,Lee J.Nanoscale hydroxyapatiteparticles for bone tissueengineering.ActaBiomater2011;7:2769—81.
[94] SutoM,NemotoE,KanayaS,SuzukiR,TsuchiyaM,ShimauchiH. NanohydroxyapatiteincreasesBMP-2expressionviaap38MAP kinasedependentpathwayinperiodontalligamentcells.Arch OralBiol2013[pii:S0003-9969(13)00072-1, doi:10.1016/j.arch-oralbio.2013.02.014].
[95] GargT,SinghO,AroraS,MurthyR.Scaffold:anovelcarrierfor celland drugdelivery.CritRevTher DrugCarrierSyst2012; 29:1—63.