Urological Oncology
INSURANCE STATUS AND OUTCOMES AFTER RADICAL PROSTATECTOMY GALLINA
et al.
Health-insurance status is a determinant of the stage at
presentation and of cancer control in European men
treated with radical prostatectomy for clinically localized
prostate cancer
Andrea Gallina*‡, Pierre I. Karakiewicz*, Felix K.-H. Chun*†, Alberto Briganti*‡,
Markus Graefen¶, Francesco Montorsi‡, Jochen Walz†, Claudio Jeldres*,
Andreas Erbersdobler§, Andrea Salonia‡, Nazareno Suardi‡, Federico Dehò‡,
Thorsten Schlomm†, Vincenzo Scattoni‡, Alexander Haese†, Hans Heinzer†,
Luc Valiquette*, Patrizio Rigatti‡ and Hartwig Huland†¶
*Cancer Prognostics and Health Outcomes Unit, University of Montreal, Montreal, Quebec, Canada, †Department of
Urology, ¶Martini Clinic – Prostate Cancer Center, and §Institute of Pathology, University of Hamburg, Hamburg,
Germany, and ‡Department of Urology, Vita-Salute University, Milan, Italy
Accepted for publication 7 December 2006 A.G and P.I.K contributed equally to the manuscript
variables according to insurance status (private vs public). Means and proportions tests were complemented with logistic regression or Kaplan–Meier analyses. RESULTS
Serum prostate-specific antigen level
(P< 0.001), clinical stage (P< 0.001),
pathological Gleason sum (P= 0.02), positive
surgical margin rate (18.4% vs 25.4%,
P< 0.001), extracapsular extension rate
(17.7% vs 20.0%, P= 0.047) and seminal
vesicle invasion rate (9.6% vs 11.6%, P= 0.04)
were more favourable in privately insured patients. Conversely, the rate of lymph-node involvement was higher in those with private than public insurance (4.4% vs 3.3%,
P= 0.045). In univariate analyses addressing
pathological variables, private insurance
was invariably protective (all P< 0.05). The
Kaplan–Meier analyses showed that privately insured patients had a lower rate of BCR after
RP (log-rank P= 0.017).
CONCLUSION
Despite uninhibited access to healthcare, insurance status represents a rate-limiting variable, which affects stage at presentation and the outcome of cancer control.
KEYWORDS
insurance status, prostate cancer, outcome prediction
OBJECTIVE
To determine whether health-insurance status might result in more localized stage at presentation, more favourable stage at surgery and in a lower rate of biochemical recurrence (BCR), in patients diagnosed with prostate cancer and treated with radical prostatectomy (RP), as despite uninhibited access to healthcare, private and public health insurance are available in most European countries.
PATIENTS AND METHODS
In all, 4442 consecutive men had RP in two large European centres, of whom 2372 had public and 2070 had private health insurance. The groups were compared for several
INTRODUCTION
Many European countries enjoy publicly funded and general access to healthcare [1]. However, patients have the choice of purchasing additional ‘private’ coverage, which might provide several advantages. These include the opportunity of choosing among different healthcare providers, to have access to more senior consultants, and to ‘jump the queue’ if there are long waiting times. We postulated that these advantages might result in better outcomes. This question
was raised by several investigators who addressed the effect of health-insurance status on medical care use in American and Australian patients [2–6]. However, these analyses are of limited applicability in European countries, as there are substantial healthcare differences that distinguish these continents. To the best of our best knowledge, no study has addressed the influence of insurance status on clinical and pathological outcomes in European patients treated with radical prostatectomy (RP) for clinically localized prostate cancer.
We hypothesized that insurance status might affect clinical and pathological variables, and the rate of biochemical recurrence (BCR) after RP. To test this hypothesis, we analysed 4442 men diagnosed with prostate cancer and treated in two large European referral centres.
PATIENTS AND METHODS
Between October 1992 and July 2005, 5033 consecutive patients diagnosed with clinically localized prostate cancer had RP in two large
I N S U R A N C E S T A T U S A N D O U T C O M E S A F T E R R A D I C A L P R O S T A T E C T O M Y
European referral centres (Vita-Salute University, Milan, Italy; and University of Hamburg, Hamburg, Germany). The private and public systems in both countries are very similar and can be considered identical for analytical purposes. Patients with data unavailable before (433) or after RP (158), e.g. for initial PSA level, clinical stage or biopsy Gleason score, organ-confined disease, extracapsular extension (ECE), seminal vesicle invasion (SVI), lymph node invasion (LNI), positive surgical margins (PSM), or pathological Gleason score, were excluded from the study. Thus the analyses targeted 4442 evaluable patients. Comparisons were based on insurance status, i.e. public (2372) vs private (2070), according to billing information. Finally, BCR analyses were restricted to 2655 patients with available BCR status (1442 public and 1213 private). The clinical stage was assigned by the attending urologist as either T1c, T2 or T3 [7]. The PSA level before RP (Abbott Axym PSA assay, Abbott Park, IL, USA) was measured before a DRE and TRUS. All biopsies were
taken under TRUS guidance and were graded according to the Gleason system. All RP specimens were processed according to the Stanford protocol [8] and were graded according to the Gleason system [9] by genitourinary pathologists. Pathological stages were assigned according to the Partin stages [10]. A PSM was defined as cancer cells in contact with the inked specimen surface. No patient received neoadjuvant androgen therapy. For all patients, PSA levels were measured every 3 months in the first year, followed by biannual measurements in the second and annual measurements in the third and subsequent years after RP. BCR was
defined as a PSA level of >0.1 ng/mL and
increasing after an initial undetectable PSA. Patients with no evidence of BCR were censored at the last PSA follow-up.
The chi-square and independent sample t-test
were used respectively for comparing proportions and means. Variables assessed before RP were PSA level, clinical stage, biopsy Gleason sum and insurance status. Univariate logistic regression models were used to assess
the magnitude of the effect of insurance status on pathological stages, i.e. ECE, SVI, LNI and PSM. Conversely, Cox regression models were used to assess the magnitude of the effect of insurance status on the rate of BCR. The rates of BCR were graphically represented with Kaplan–Meier curves; all tests were two-sided with a significance level set at 0.05.
RESULTS
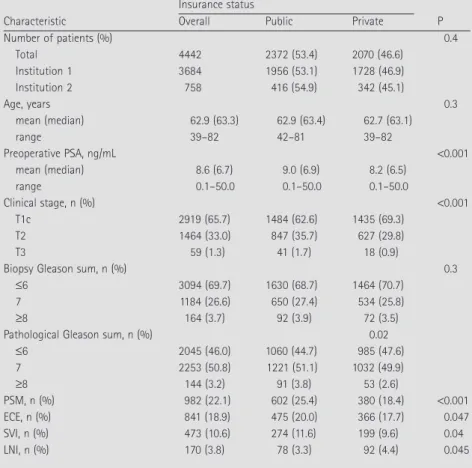
The patients’ characteristics are shown in Table 1; of all patients, 2372 had public and 2070 private insurance. The PSA level before
RP (P< 0.001) and clinical stage (P< 0.001)
were more favourable in privately insured patients, as were the pathological Gleason
sum (P= 0.02), ECE (P= 0.047), SVI (P= 0.04)
and PSM (P< 0.001), but the biopsy Gleason
sum did not differ (P= 0.3). Moreover, the
rate of LNI was higher in privately insured
patients (4.4% vs 3.3%, P= 0.045).
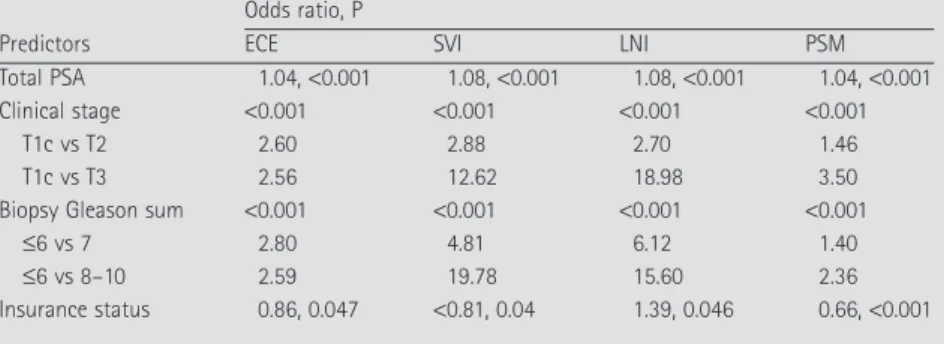
Table 2 shows the univariate models assessing the ability to predict ECE, SVI, LNI and PSM; in all regression analyses, insurance status was invariably a statistically significant predictor
(all P≤ 0.05). Private insurance had a
‘protective effect’ against ECE, SVI and PSM
(all odds ratios ≤0.86). However, private
insurance was associated with a 1.4-fold increase in the risk of LNI.
Table 3 shows the Cox regression models addressing BCR after RP. Insurance status was a statistically significant predictor of BCR
(P= 0.02) and publicly insured patients had a
higher risk of BCR after RP (odds ratio 1.2). Table 4 shows the actuarial BCR-free survival according to insurance status; the overall
mean (SD, range) follow-up was 30.7 (26.5,
0.13–129.7) months. Privately insured patients had a higher actuarial BCR-free survival at 2, 3, 4 and 5 years after RP. Figure 1 shows the overall BCR-free survival rates (a) and those according to insurance status (b). DISCUSSION
The advantages of private healthcare might favourably affect the outcome of patients with private health insurance. Based on these considerations, we hypothesized that private insurance might be associated with more favourable clinical and pathological stages, and with lower BCR rates in men treated with RP. The analyses showed that at diagnosis privately insured patients had TABLE 1 Descriptive characteristics of 4442 patients included in the analyses
Characteristic
Insurance status
P
Overall Public Private
Number of patients (%) 0.4 Total 4442 2372 (53.4) 2070 (46.6) Institution 1 3684 1956 (53.1) 1728 (46.9) Institution 2 758 416 (54.9) 342 (45.1) Age, years 0.3 mean (median) 62.9 (63.3) 62.9 (63.4) 62.7 (63.1) range 39–82 42–81 39–82 Preoperative PSA, ng/mL <0.001 mean (median) 8.6 (6.7) 9.0 (6.9) 8.2 (6.5) range 0.1–50.0 0.1–50.0 0.1–50.0 Clinical stage, n (%) <0.001 T1c 2919 (65.7) 1484 (62.6) 1435 (69.3) T2 1464 (33.0) 847 (35.7) 627 (29.8) T3 59 (1.3) 41 (1.7) 18 (0.9)
Biopsy Gleason sum, n (%) 0.3
≤6 3094 (69.7) 1630 (68.7) 1464 (70.7)
7 1184 (26.6) 650 (27.4) 534 (25.8)
≥8 164 (3.7) 92 (3.9) 72 (3.5)
Pathological Gleason sum, n (%) 0.02
≤6 2045 (46.0) 1060 (44.7) 985 (47.6) 7 2253 (50.8) 1221 (51.1) 1032 (49.9) ≥8 144 (3.2) 91 (3.8) 53 (2.6) PSM, n (%) 982 (22.1) 602 (25.4) 380 (18.4) <0.001 ECE, n (%) 841 (18.9) 475 (20.0) 366 (17.7) 0.047 SVI, n (%) 473 (10.6) 274 (11.6) 199 (9.6) 0.04 LNI, n (%) 170 (3.8) 78 (3.3) 92 (4.4) 0.045
G A L L I N A E T A L .
more favourable clinical characteristics than their publicly insured counterparts (Table 1), as shown by a lower PSA level (8.2 vs
9.0 ng/mL, P≤ 0.001), and lower clinical
stage (T1c in 69.3% vs 62.6%, P< 0.001).
These more favourable clinical characteristics, as expected, translated into more favourable
pathological Gleason sum (P= 0.02), a lower
rate of ECE (17.7% vs 20.0%, P= 0.047), SVI
(9.6% vs 11.6%, P= 0.04) and PSM (18.4% vs
25.4%, P< 0.001).
These findings suggest that private insurance status is associated with more favourable cancer characteristics at both the diagnosis and at RP. However, despite overall better stages in privately insured patients, the rate of LNI was counter-intuitively higher in the privately insured group (3.3% vs 4.4%,
P= 0.045). This finding might be explained
by the extent of pelvic lymphadenectomy, whereby there is possibly a more meticulous and more extensive dissection. We previously showed that, unlike other pathological stages, the rate of LNI could be strongly affected by the extent of dissection [11–13]. Therefore, more attention to detail and greater extent of pelvic lymphadenectomy appear to represent a valid explanation for the observed effect of insurance status on LNI.
Moreover, PSM rates are linked to surgical volume and surgical skill. Private insurance status might provide more experienced surgeons, which translates into a lower rate of PSM [14,15]. Conversely, ECE and SVI are strongly associated with the tumour volume and they cannot be influenced by surgical skill or expertise [16]. Thus, they only reflect cancer characteristics, and therefore these unfavourable outcomes are more frequent in the publicly insured patients.
The analyses of BCR rates confirmed the results reported for clinical and pathological stages, where private insurance was related to more favourable disease characteristics. The rate of BCR was 1.2 times higher in publicly
insured patients (odds ratio 0.81, P= 0.018),
as shown in Fig. 1B.
We chose not to include multivariate analyses, as these might obscure the effect of insurance status on the targeted outcomes. Adjusting for clinical stage, PSA level and biopsy Gleason sum, and pathological stage and PSM, corresponds to voluntarily removing the underlying effect of insurance status, which rests on the observed differences in clinical
variables at presentation. Thus, multivariate analyses are not applicable to hypothesis testing. Insurance status represents a proxy of household annual income, socio-economic status, education, social status and health-conscious behaviour. These variables were identified as potential reasons for the discrepancy in several North American and
Australian studies [6,17,18]. Roetzheim et al.
[18] showed that, in the USA, more advanced cancers, including prostate cancer, were diagnosed in the uninsured and in patients on
Medicaid. Moreover, Ford et al. [17] found that
lack of health insurance coverage represents a TABLE 2 The univariate LRMs for each outcome
Predictors
Odds ratio, P
ECE SVI LNI PSM
Total PSA 1.04, <0.001 1.08, <0.001 1.08, <0.001 1.04, <0.001
Clinical stage <0.001 <0.001 <0.001 <0.001
T1c vs T2 2.60 2.88 2.70 1.46
T1c vs T3 2.56 12.62 18.98 3.50
Biopsy Gleason sum <0.001 <0.001 <0.001 <0.001
≤6 vs 7 2.80 4.81 6.12 1.40
≤6 vs 8–10 2.59 19.78 15.60 2.36
Insurance status 0.86, 0.047 <0.81, 0.04 1.39, 0.046 0.66, <0.001
TABLE 3 Univariate Cox regression models assessing BCR after RP
Predictors Rate ratio P
Total PSA 1.05 <0.001
Clinical stage <0.001
T1c vs T2 2.01
T1c vs T3 5.43
Biopsy Gleason sum <0.001
≤6 vs 7 3.14
≤6 vs 8–10 7.76
Insurance status 0.86 0.02
TABLE 4
Actuarial BCR-free survival percentage according to insurance status
Years after RP Overall Private Public P
N 2655 1213 1442 1 84 85 83 0.2 2 78 80 77 0.06 3 74 77 72 0.003 4 70 74 67 <0.001 5 65 69 62 0.002
FIG. 1. The overall BCR-free survival rates (A) and those according to insurance status (B).
B 100 90 80 70 60 50 40 30 20 10 0 0 20 40 60 80 100 120 140 Time, months
Percentage of patients free from BCR
A 100 90 80 70 60 50 40 30 20 10 0 0 20 40 60 80 100 120 140 Time, months
Percentage of patients free from BCR
Private
Public Log rank p = 0.017
I N S U R A N C E S T A T U S A N D O U T C O M E S A F T E R R A D I C A L P R O S T A T E C T O M Y
barrier to prostate cancer screening and
treatment in American patients. Hall et al. [6]
analysed >14 000 Australian men diagnosed
with prostate cancer and showed that the 3-year survival was lower in those with no private health insurance. Therefore, the present findings are consistent with previous reports, where insurance status was a determinant of various outcomes of cancer control. Notably, none of these studies relied on multivariate analyses to detect the effect of health insurance status. This further validates our univariate approach to data analysis.
Taken together, the present results showed that privately insured patients treated with RP for localized prostate cancer present with more favourable clinical and pathological characteristics. These in turn translate into lower BCR rates and better outcomes. There are several limitations to the present study. Unfortunately, we could not directly compare our results to North-American or Australian findings where the effect of insurance status was considered. The inability to make valid comparisons stems from fundamental differences between the North-American and the European health-economic and care systems. Our findings might not be applicable to small institutions, where the choice between private and public insurance might not translate into important differences in the care provided or in the delay before RP. Furthermore, all the present patients included in the analyses represent a referral population, and thus the findings do not apply to a screened population. However, previous studies indicate that screening participation rates are higher in populations with a high socio-economic status [19–21]. Delays related to urological referral, biopsy, diagnosis and definitive treatment might have affected our findings. Unfortunately, we have no data to comment on the effect of delays between initial suspicion of prostate cancer and urological referral. Similarly, we cannot comment on the effect of any delay between the initial urological assessment and histological proof of prostate cancer. However, the delay between diagnosis and RP had no effect on the rate of BCR, and therefore it is unlikely that publicly insured patients had worse outcomes due to longer waiting times [22]. Finally, our results are not applicable to other healthcare systems, where insurance status could be significantly different from that in Italy or Germany.
In conclusion, privately insured patients had more favourable clinical and pathological tumour characteristics, which translated in better pathological and cancer control outcomes.
ACKNOWLEDGEMENTS
Pierre I. Karakiewicz is partially supported by the Fonds de la Recherche en Santé du Québec, the CHUM Foundation, the Department of Surgery and Les Urologues Associés du CHUM.
CONFLICT OF INTEREST
None declared.
REFERENCES
1 Buchmueller TC, Couffinhal A, Grignon M, Perronnin M. Access to physician services: does supplemental insurance
matter? evidence from France. Health
Econ 2004; 13: 669–87
2 Tarman GJ, Kane CJ, Moul JW et al. Impact of socioeconomic status and race on clinical parameters of patients undergoing radical prostatectomy in an
equal access health care system. Urology
2000; 56: 1016–20
3 Greene KL, Cowan JE, Cooperberg MR, Meng MV, DuChane J, Carroll
PR;Cancer of the Prostate Strategic
Urologic Research Endeavor (CaPSURE) Investigators. Who is the average patient
presenting with prostate cancer? Urology
2005; 66 (Suppl.): 76–82
4 Optenberg SA, Thompson IM, Friedrichs P, Wojcik B, Stein CR, Kramer B. Race, treatment, and long-term survival from prostate cancer in an equal-access
medical care delivery system. JAMA 1995;
274: 1599–605
5 Mullins CD, Snyder SE, Wang J, Cooke JL, Baquet C. Economic disparities in treatment costs among ambulatory Medicaid cancer patients. J Natl Med Assoc 2004; 96: 1565– 74
6 Hall SE, Holman CD, Wisniewski ZS, Semmens J. Prostate cancer: socio-economic, geographical and private-health insurance effects on care and
survival. BJU Int 2005; 95: 51–8
7 Greene F, Page D, Fleming I et al. eds,
American Joint Committee on Cancer. AJCC Cancer Staging Manual, 6th edn. New York, NY: Springer, 2002 8 McNeal JE, Villers AA, Redwine EA,
Freiha FS, Stamey TA. Histologic differentiation, cancer volume, and pelvic lymph node metastasis in adenocarcinoma of the prostate. Cancer
1990; 66: 1225–33
9 Gleason DF and the Veterans Administration Cooperative Urological Research Group. Urologic Pathology. Philadelphia: Lea & Febiger, 1977 10 Partin AW, Kattan MW, Subong EN
et al. Combination of prostate-specific
antigen, clinical stage, and Gleason score to predict pathological stage of localized prostate cancer. A multi-institutional
update. JAMA 1997; 277: 1445–51
11 Briganti A, Chun FK, Salonia A et al. Validation of a nomogram predicting the probability of lymph node invasion based on the extent of pelvic lymphadenectomy in patients with clinically localized
prostate cancer. BJU Int 2006; 98: 788–93
12 Briganti A, Chun FK, Salonia A et al. A nomogram for staging of exclusive nonobturator lymph node metastases in men with localized prostate cancer. Eur Urol 2007; 51: 112–20
13 Briganti A, Chun FK, Salonia A et al. Validation of a nomogram predicting the probability of lymph node invasion among patients undergoing radical prostatectomy and an extended pelvic
lymphadenectomy. Eur Urol 2006; 49:
1019–27
14 Eastham JA, Kattan MW, Riedel E et al. Variations among individual surgeons in the rate of positive surgical margins in radical prostatectomy specimens. J Urol
2003; 170: 2292–5
15 Hernandez DJ, Epstein JI, Trock BJ, Tsuzuki T, Carter HB, Walsh PC. Radical retropubic prostatectomy. How often do experienced surgeons have positive surgical margins when there is extraprostatic extension in the region of the neurovascular bundle? J Urol 2005;
173: 446–9
16 Nelson BA, Shappell SB, Chang SS et al. Tumour volume is an independent predictor of prostate-specific antigen recurrence in patients undergoing radical prostatectomy for clinically localized
prostate cancer. BJU Int 2006; 97: 1169–
72
17 Ford ME, Vernon SW, Havstad SL, Thomas SA, Davis SD. Factors
G A L L I N A E T A L .
influencing behavioral intention regarding prostate cancer screening among older African-American men. J Natl Med Assoc 2006; 98: 505–14 18 Roetzheim RG, Pal N, Tennant C et al.
Effects of health insurance and race on early detection of cancer. J Natl Cancer Inst 1999; 91: 1409–15
19 Duffy CM, Clark MA, Allsworth JE.
Health maintenance and screening in breast cancer survivors in the United
States. Cancer Detect Prev 2006; 30: 52–7
20 Parker PA, Cohen L, Bhadkamkar VA
et al. Demographic and past screening
behaviors of men attending a free community screening program for prostate cancer. Health Promot Pract
2006; 7: 213–20
21 Swan J, Breen N, Coates RJ, Rimer BK, Lee NC. Progress in cancer screening practices in the United States: results from the 2000 National Health Interview
Survey. Cancer 2003; 97: 1528–40
22 Graefen M, Walz J, Chun KH, Schlomm T, Haese A, Huland H. Reasonable delay of surgical treatment in men with localized prostate cancer – impact on
prognosis? Eur Urol 2005; 47: 756–60
Correspondence: Pierre I. Karakiewicz, Cancer
Prognostics and Health Outcomes Unit, University of Montreal Health Center (CHUM), 1058, rue St-Denis, Montréal, Québec, Canada, H2X3J4.
e-mail: [email protected]
Abbreviations: RP, radical prostatectomy;
BCR, biochemical recurrence; ECE,
extracapsular extension; SVI, seminal vesicle
invasion; LNI, lymph node invasion; PSM,