CAN MINDFULNESS PRACTICE BE THE ANSWER?
Natasha I. Best
A DNP Project submitted to the faculty at the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Doctor of Nursing Practice in the School
of Nursing.
Chapel Hill 2019
ABSTRACT
Natasha I. Best: Targeting Military Healthcare Providers to Self-Identify and Take Action Against Compassion Fatigue: Can Mindfulness Practice Be the Answer?
(Under the direction of Carol Durham)
Background: Like their civilian counter parts, military clinicians are at risk of compassion fatigue. Both anecdotal evidence and data collection have demonstrated that
ACKNOWLEDGEMENTS
I must start off first and foremost by thanking my Heavenly Father, the Lord Our God. Through Him, all things are possible, and He has truly placed a blessing over my life! Of course, I must thank my wonderful and supportive family- My beloved husband, Greg, two children, Khloe and Karlton, my parents, siblings, in-laws and extended family. Without their
understanding, I could not have even began to take the first few steps of this journey; they are my motivation and reasons for always striving to do better and reach for the stars! I would also like to thank my many friends, I know that I do not have to name them all, for they know how they have been ears and eyes for me in completing this journey.
To Dr. Carol Durham, my DNP project chair, I owe a depth of gratitude that I do not know how else to pay back other than, to pay it forward, following her example and graciously, lovingly support my fellow nursing colleagues. She stepped in when I desperately needed mentoring and support through this journey. The same goes for Dr. Cheryl Giscombe and Dr. Julee Waldrop, members of my committee. I am in awe of these three amazing ladies!
PREFACE
Dr. Jean Watson proposed that healthcare providers “are torn between the human caring values and the “calling” that attracted them to the profession, and the technological, high paced, tasked-oriented biomedical practices and institutional demands, heavy patient loads, and
outdated industrial practice patterns” (Watson, 2009, p. 467). This internal battle, that healthcare providers often face, can prove to be personally and professionally detrimental, and can lead to devasting patient outcomes. Healthcare providers have a personal and professional responsibility to themselves and their patients to seek tools to remain resilient while providing quality
TABLE OF CONTENTS
LIST OF TABLES ... ix
LIST OF ABBREVIATIONS ... x
CHAPTER 1: HOW CAN MINDFULNESS ACCOMPLISH THE MISSION ... 1
Background and Significance ... 1
Purpose ... 4
Clinical Question ... 4
CHAPTER 2: REVIEW OF LITERATURE ... 5
Purpose and Methodology for Review of Literature ... 5
Results for Review of Literature ... 6
Studies and Sample Characteristics. ... 6
Mindfulness Effects on Compassion Fatigue. ... 7
Mindfulness Based Interventions Specifically for Healthcare Providers. ... 8
Conclusions for Review of Literature ... 9
CHAPTER 3: THEORETICAL FRAMEWORK AND METHODOLOGY ... 10
Theoretical Framework ... 10
Justification of Theory Utilization ... 12
Participants. ... 13
Procedures. ... 14
Instruments for Data Collection. ... 16
Sample Characteristics ... 19
Pre- and Post- Intervention ProQOL Scores ... 19
Pre- and Post- Intervention MAAS Scores ... 20
Participants’ Reflections ... 21
CHAPTER 5: DISCUSSION ... 23
Limitations ... 24
Participant Selection. ... 24
Intervention Design and Implementation. ... 25
Participants’ Pre-Knowledge and Expectations. ... 27
Recommendations for Practice ... 27
Conclusions ... 31
APPENDIX A: TOOLS TO REVIEW THE LITERATURE... 33
APPENDIX B: PROJECT RECRUITMENT EMAIL/FACEBOOK POST... 35
APPENDIX C: CONSENT FORM ... 37
APPENDIX D: SCREENSHOT OF INSIGHT TIMER MOBILE APPLICATION ... 42
APPENDIX F: SELF-GENERATED CODES FOR SURVEYS ... 45
APPENDIX G: THE PROFESSIONAL QUALITY OF LIFE SCALE (PROQOL) ... 46
APPENDIX H: PERMISSION FOR PROQOL USE ... 47
APPENDIX I: MINDFUL ATTENTION AWARENESS SCALE (MAAS) ... 48
APPENDIX J: PERMISSION FOR MAAS USE ... 50
APPENDIX K: DEMOGRAPHICS QUESTIONNAIRE (IN ELECTROIC LINK)... 53
APPENDIX L: CHECK-IN FACEBOOK POST/EMAIL/MOBILE APP ... 54
LIST OF TABLES
LIST OF ABBREVIATIONS
CINAHL Cumulative Index of Nursing and Allied Health Literature DoD Department of Defense
IHI Institute of Healthcare Improvement MBSR Mindfulness-based Stress Reduction MeSH Medical Subject Headings
PRISMA Preferred Reporting Items for Systematic Reviews and Meta-Analysis ProQOL Professional Quality of Life
CHAPTER 1: HOW CAN MINDFULNESS ACCOMPLISH THE MISSION Background and Significance
The Institute of Healthcare Improvement’s (IHI) Triple Aim initiative to improve health care has three areas of focus: enhancing patient experience, improving population health and reducing the cost of healthcare (Berwick, Nolan, & Whittington, 2008). In 2014, Bodenheimer and Sinsky recommended that the healthcare industry look at adding a fourth aim to focus on improving the work/life balance of healthcare clinicians and staff, proposing that without this additional aim, success in improving population health may never occur. Many view providing healthcare as a selfless, rewarding career that calls on the giving of oneself through empathy and compassion for others, yet, those in the profession can lack empathy and compassion for
themselves (Hevezi, 2016; Varner & Foutch, 2014). This may lead to compassion fatigue among healthcare providers.
Compassion fatigue is described as “a state of exhaustion and dysfunction biologically, psychologically, and socially, because of, prolonged exposure to compassion stress and all it involves” (Figley, 1995, p. 253). It is the combination of two components- burnout and secondary traumatic stress. Burnout is chronic or long-term stress related to one’s occupation that may result in physical and emotional exhaustion. Often replicating symptoms of
post-traumatic stress in individuals, secondary trauma stress is trauma experienced vicariously related to one’s proximity to another’s pain and suffering (Cocker & Joss, 2016; Figley, 1995;
healthcare professionals and is known to lead to detrimental mental health. These negative correlations place providers at risk of leaving their profession altogether (Cocker & Joss, 2016).
Clinicians in the United States, expanding all specialty areas of healthcare within the current 21st century medical model, are particularly vulnerable for developing compassion fatigue as they battle against the constant pressures of a decreasing supply of medical personnel, equipment and funds and the demands of an increasing patient population, who are living longer lives that include complex health and socioeconomic statuses (Bodenheimer & Sinsky, 2014; Friedberg et al., 2017; Nolte et al., 2017). In a RAND 2013/2014 survey, 1,277 clinicians and staff members, representing 42% of 503 federally qualified health centers, indicated a decrease in professional satisfaction over time (Friedberg et al., 2017). Within a time-frame of less than a year, overall job satisfaction went from 84.2% to 74.4%, burnout rates of 23% to 31.5% and intent to leave the practice from 29.3% to 38.2%, all with p values of <0.001 (Friedberg et al., 2017).
Military providers are predominantly vulnerable for developing compassion fatigue. They provide care to a specialized population including armed service members, department of
duty Air Force, family practice providers that responded to their survey, 59% reported medium levels of emotional exhaustion and nearly 66% reported low levels of depersonalization, two symptoms known to lead to burnout, a component of compassion fatigue.
There are currently 62 active duty women’s health nurse practitioners (WHNPs) serving in the US Air Force. These officers provide gynecological and obstetrical care to the female population of armed services members, DoD, retirees and their dependents. They are embedded in stand-alone clinics, family practice/primary care clinics, maternal-child units and emergency rooms throughout the continental United States and overseas locations. For close to two decades, active duty WHNPs, among other military healthcare providers have been observing and treating many horrific injuries, because of war (Weidlich & Ugarriza, 2015). In recent years, they have served along-side their fellow service members during constant combat battle conflicts, to include, Operations Iraqi Freedom and Enduring Freedom. Like their civilian counter parts, military healthcare providers, including active duty WHNPs, are at risk of compassion fatigue. Both anecdotal evidence and data collection have demonstrated that healthcare team members inability to self-identify, manage and recover from compassion fatigue can lead to personal emotional and physical distress which can eventually manifest into negative patient outcomes (Cocker & Joss, 2016; Varner & Foutch, 2014; Weidlich & Ugarriza, 2015).
fatigue and its components of burnout and secondary traumatic stress among healthcare
providers (Cocker & Joss, 2016; Mensah & Anderson, 2015). Dr. Jon Kabat-Zinn developed an 8-week mindfulness-based stress reduction program (MBSR) at the University of Massachusetts Medical Center to help mitigate symptoms of stress in a healthy way (Kabat-Zinn, 1990). This method incorporates mindful meditation and movement to enhance awareness and reduce psychological effects of stress, pain and illness. The method has been well researched and found to be not only scientifically sound, but also clinically useful (Fortney, Luchterband, Zakletskaia, Zgierska, & Rakel, 2013; Goldhagen, Kingsolver, Stinnett, & Rosdahl, 2015).
Purpose
The purpose of this implementation and evaluation project was two-folded. 1: To assess the benefit of the use of the Professional Quality of Life (ProQOL) instrument, to help military healthcare providers self-identify risk of compassion fatigue. 2: To determine if the use of an abbreviated MBSR program involving a mobile application and integrated web-based tools would help decrease symptoms of compassion fatigue and its components (burnout and secondary traumatic stress) among a targeted military provider population of active duty WHNPs.
Clinical Question
CHAPTER 2: REVIEW OF LITERATURE Purpose and Methodology for Review of Literature
In accordance with relevant aspects of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), a review of the literature on the effects of mindfulness-based interventions on compassion fatigue and its components of burnout and secondary
traumatic stress in US military healthcare providers was completed (Moher, Liberarti, Tetzlaff, & Altman, 2009). Due to the limited studies found on US military providers regarding the
problem and intervention strategies, the search was expanded to include US healthcare providers. Pubmed, Embase, PsycInfo, and the Cumulative Index to Nursing and Allied Health Literature (CINAHL) were the four databases included the search. A combination of Medical Subject Heading (MeSH) terms were used to complete the search (see Appendix A). Inclusion criteria for this literature review was limited to English language, peered-reviewed articles, studies primarily completed in the US, studies focused on healthcare providers, to include interns and residents, with a time range between January 2008 and January 2018 (a time frame reflective of IHI’s Triple Aim initiative). Exclusion criteria included research studies without clear outcomes, studies completed primarily outside of the continental US, and studies with a focus solely on mental health providers, social workers, students and family members. The reviewed articles consisted of various study designs that were inclusive of both qualitative and quantitative data.
assessment. Another 22 articles were excluded because they did not fall within the inclusion and exclusion criteria, leaving 18 articles to be included in this literature review.
Results for Review of Literature
Studies and Sample Characteristics. Of the eighteen articles used in this review, six were systematic reviews (Burgess, Beach, & Saha, 2017; Cocker & Joss, 2016; Gilmartin et al., 2017; Lamothe, Rondeau, Malboeuf-Hurtubise, Duval, & Sultan, 2016; Luken & Sammons, 2016; Mensah & Anderson, 2015), three were pilot randomized control trials (Moody et al., 2013; Sood, Sharma, Schroeder, & Gorman, 2014; West et al., 2014), six were single-sample, pre/post studies (Fortney, Luchterband, Zakletskaia, Zgierska, & Rakel, 2013; Goodman & Schorling, 2012; Krasner et al., 2009; Pflugeisen, Drummond, Ebersole, Mundell, & Chen, 2016; Runyan, Savageau, Potts, & Weinreb, 2016; Taylor, Hageman, & Brown, 2016), two were prospective studies (Goldhagen et al., 2015; Kemper & Khirallah, 2015), and one was a cross-sectional survey (Kemper, Mo, & Khayat, 2015). Each study presented, emphasized that all participants were volunteers, with the majority being samples of convenience. All studies’ participants were above 18 years of age, inclusive of various in- and out-patient medical specialties such as pediatrics, family medicine, radiology, acute care, and surgical services. Sample sizes ranged from 7 to 513 participants that were predominately female, apart from three studies involving only physicians that were mostly male (Krasner et al., 2009; Pflugeisen et al., 2016; West et al., 2014). The studies were primarily focused on populations of physicians (including interns and residents), nurse practitioners, nurses and nursing students. In studies where samples were comprised of various healthcare providers, nurses represented a larger portion of the sample (Cocker & Joss, 2016; Gilmartin et al., 2017; Lamothe et al., 2016; Mensah & Anderson, 2015; Moody et al., 2013). Most studies were completed in the US,
such as, Canada, Thailand, Tasmania, Germany and Australia (Cocker & Joss, 2016; Gilmartin et al., 2017; Lamothe et al., 2016; Luken & Sammons, 2016; Moody et al., 2013).
Mindfulness Effects on Compassion Fatigue. Healthcare provider well-being involves being in a state of balance physically, emotionally and mentally in relation to work/life balance (Bodenheimer & Sinsky, 2014; Pospos et al., 2018). Compassion fatigue and its components of burnout and secondary traumatic stress can upset this balance, jeopardizing provider well-being. All studies revealed promising outcomes regarding mindfulness-based interventions on
healthcare provider well-being.
In their systematic review of brief mindfulness practices of 833 healthcare providers, Gilmartin et al. (2017) found 9 of the14 studies reported significant improvements in provider well-being. Specifically, regarding compassion fatigue elements, five studies reported
statistically significant improvements in stress (p <.05 to p <.001), while one study demonstrated improvements in symptoms of burnout post mindfulness-based intervention (p <.05) (Gilmartin et al., 2017). Like the other systematic reviews of mindfulness-based interventions on provider well-being used in this literature review, various instruments were used in studies within this particular review to validate results; they include the Perceived Stress Scale, Maslach Burnout Inventory, Connor-Davidson Resilience Scale, and Mindfulness Attention Awareness Scale (Cocker & Joss, 2016; Gilmartin et al., 2017; Lamothe et al., 2016; Luken & Sammons, 2016; Mensah & Anderson, 2015).
improvement in participants’ mindfulness, self-awareness, compassion, and ability to handle stressful situations. These qualitative findings were analyzed via the participants’ journal entries (Moody et al., 2013). West et al. (2014) reported similar findings in their randomized clinical trial of 74 physician at the Mayo Clinic in Rochester, Minnesota; their findings showed
statistically significant improvement (p= .03) in overall burnout in the intervention group. In the intervention group of their mindfulness-based intervention study, Sood et al. (2014) found statistically significant (p <.005) improvements in perceived stress and mindfulness, post intervention as compared to the control group.
Of the six single-sample, pre/post studies, all indicated statistically significant results (p <.001 to .05) of improvement in symptoms of stress and burnout and increase in mindfulness among healthcare providers (Fortney et al, 2013; Goodman & Schorling, 2012; Krasner et al., 2009; Pflugeisen et al., 2016; Runyan et al, 2016; Taylor et al., 2016). The two prospective studies showed mixed statistical significance in sample baseline and post intervention scales for improvement in burnout, stress and mindfulness, however they identified promising qualitative trends (Goldhagen et al., 2015; Kemper & Khirallah, 2015). The remaining cross-sectional survey demonstrated a positive correlation between the trainable quality of mindfulness and a decrease in burnout symptoms (Kemper et al., 2015).
Mindfulness Based Interventions Specifically for Healthcare Providers. Embedded in the traditional practice of mindfulness are several formal meditation practices (body scan,
course to abbreviated versions of his course to mindfulness-based interventions in conjunction with other provider resiliency training. The systematic reviews represented a wide variety of mindfulness-based practices, often demonstrating feasibility and sustainability among healthcare providers. The practices included healthcare provider specific modifications (such as, emphasis being placed on self-care, and providing quality patient care and satisfaction). There were also brief practice techniques that were accessible conveniently, via on-line modules and mobile devices for the often-busy healthcare provider (Burgess et al, 2017; Cocker & Joss, 2016; Gilmartin et al., 2017; Lamothe et al, 2016; Luken & Sammons, 2016; Mensah & Anderson, 2015).
Conclusions for Review of Literature
A review of the literature suggested that mindfulness-based interventions could have a positive effect on compassion fatigue and its subcomponents of burnout and secondary traumatic stress in healthcare providers. Although no specific study was found on military healthcare providers, the promising results of mindfulness-based interventions in multiple studies on US healthcare providers are readily transferable to military healthcare providers as they face similar challenges. These challenges include limited time and resources, high demand to supply quality healthcare to a growing patient population and battling the ever-changing medical arena.
CHAPTER 3: THEORETICAL FRAMEWORK AND METHODOLOGY Theoretical Framework
Jean Watson’s Human Caring Theory provides a solid framework for addressing compassion fatigue in healthcare providers in the US military (Watson, 2009). The initial premises of American nurse theorist, Jean Watson’s Human Caring Theory, was published in 1979 in her book, Nursing: The Philosophy and Science of Caring (McCance, McKenna, & Boore, 1999). Watson states that the theory is based on “human caring relationships and the deeply human experiences of life itself, not just health-illness phenomena, as traditionally defined within medicine” (Fawcett, 2002, p. 215). Although her theory was developed to guide and describe her nursing experience, it has origins in metaphysics and is a form of humanism (McCance et al., 1999). Over the last four plus decades, many nurses have learned, expanded upon and practiced within Watson’s theoretical framework (Watson, 2009). However, Watson has stated that she saw the “value of [the] Human Caring Theory as a foundational ethic and philosophy for any health professional” (Fawcett, 2002, p. 215).
supportive/protective environment, human needs assistance, and existential-phenomenological-spiritual forces (Cara, 2003). In the late 1980’s, Watson introduced clinical caritas processes, to replace carative factors to give a “greater spiritual dimension” to her theory (Cara, 2003). Caritas comes from the Greek language, meaning “to cherish and to give special loving attention” (Cara, 2003, p. 52). The concept of transpersonal caring is the relationship between the provider and patient, the provider and self, and the provider and colleagues (Lombardo & Eyre, 2011). Lastly, the caring moment or occasion, is the actual event, to include time and location, in which care is given (McCance et al., 1999).
Watson’s Human Caring Theory encompasses care of one’s self to be able to provide the highest level of care through transpersonal relationships between the provider and patient, and the provider and colleagues (Cara, 2003). As mentioned before, Watson’s initial carative factors included “sensitivity to self and others”; she further expanded attention to self in her clinical caritas processes (McCance et al., 1999). Five of her ten clinical caritas processes discuss the importance of being present, showing self-dignity, connecting to one’s deeper self,
acknowledging one’s own spirit and care of self to provide the human care factor to nursing practice (Cara, 2003). Compassion fatigue, which according to the literature is a combination of burnout and secondary traumatic stress, may be the outcome of healthcare providers not taking care of themselves as suggested by Watson’s theory (Cocker & Joss, 2016; Figley, 1995; Nolte et al, 2017).
focus on care of self among healthcare providers have been associated with a decrease in compassion fatigue or components of it (i.e. burnout and secondary traumatic stress) (Duarte & Pinto-Gouviea, 2016; Garland et al., 2015; Gauthier, Meyer, Grefe, & Gold, 2015; Hevezi, 2016; Mensah & Anderson, 2015). Mindfulness is one of these interventions. With the use of
mindfulness, healthcare providers can practice self-care and improve their own relationship with self, which will likely prove to have positive effects not only on self, but on patients and
colleagues’ transpersonal relationships.
Strengths of Watson’s theory as related to decreasing compassion fatigue among providers is that it makes several assumptions about the role of self. It emphasized that caring provides a safe place to overcome challenges and improve one’s own wholeness and connection with one’s own soul and deeper self. According to the theory, caring for one’s self has a positive impact on personal growth, knowledge, control, healing processes and practice, which in turn helps others (Cara, 2003).
Limitations of the Human Caring Theory is that it does rely on the provider to make a conscious connection with his or her own thoughts and feelings and be able to translate from a viewpoint of self to others. The provider must recognize, honestly, own thoughts of humanity, definition of individuals with consideration of real or perceived bias and prejudice and outward display of caring for self and others. If the provider is unable or unwilling to delve deep into self, then care of others can come off superficial and ingenuine, reducing the provider and patient relationship to the sterile curer and the sick status of medicine.
Justification of Theory Utilization
vision of any action, theory is often leaned upon to provide a guide of explanation (Pipe, 2008). Watson’s Human Caring Theory does just that for the identification of compassion fatigue among healthcare providers and the importance of combating it for the betterment of both provider and patient. Watson’s theory goes in depth about the importance of the concept of caring being a foundation of nursing practice and being complimentary to the curing aspects of modern medicine. The theory calls on intrapersonal, interpersonal and transpersonal relationships to express caring; relying on acts of caring of self and others (Cara, 2003). Through caring for one’s self with the practice of mindfulness, healthcare providers can reduce their risk of the symptoms of compassion fatigue and mitigate impact on patients.
Project Methodology
Participants. To focus on the Human Caring Theory’s concept of having a healthy relationship with self to be able to provide better care to others, a convenience sample of military providers, active duty WHNPs in the US Air Force, was recruited (n = 62) to participate in an abbreviated MBSR intervention. Non-active duty WHNPs (to include, civilian, reserve and contract employees) were not invited to participate. Recruitment was conducted through an electronic announcement posted via a private FaceBook group page and personal email sent to active duty WHNPs in the US Air Force (see Appendix B). Project recruits had to have reliable internet access and connectivity, as well as mobile application download capabilities throughout the duration of the project. Consent was obtained (see Appendix C). To incentivize completion of the project, all participants who completed the intervention phase were entered in a drawing for a $200 gift card. The project was reviewed and approved by the University of North
Procedures. The intervention was a 4-week MBSR program that used a mobile
application called Insight Timer, based on an abbreviated version of the 8-week MBSR program developed by Dr. Jon Kabat-Zinn (Pospos et al., 2018) (see Appendix D). In 2017, Pospos et al. reviewed web-based tools and mobile applications used to help mitigate burnout and found that the Insight Timer had several positive features for this mindfulness-based intervention. These features include that the application is free, it offers tracking of practice sessions, reminders to practice, a built-in timer, and a user interactive network (Pospos et al., 2018).
To better orient the participants to the project and to provide background information on compassion fatigue and mindfulness, informational modules were given in block segments: Module 1: Overview of the project; Module 2: Instructions on how to complete pre and post surveys; Module 3: Download and use of the mobile application; Module 4: Logging of
sessions/journaling; Module 5: Background and history of MBSR; Modules 6-9: Introduction to four formal mindfulness practices (body scan, mindful movement, walking meditation and sitting meditation); and Module 10: Overview of compassion fatigue and its subcomponents of burnout and secondary traumatic stress. These informational modules were pre-recorded by the author and available online to be accessed at the participants’ convenience throughout the intervention phase (see Appendix E).
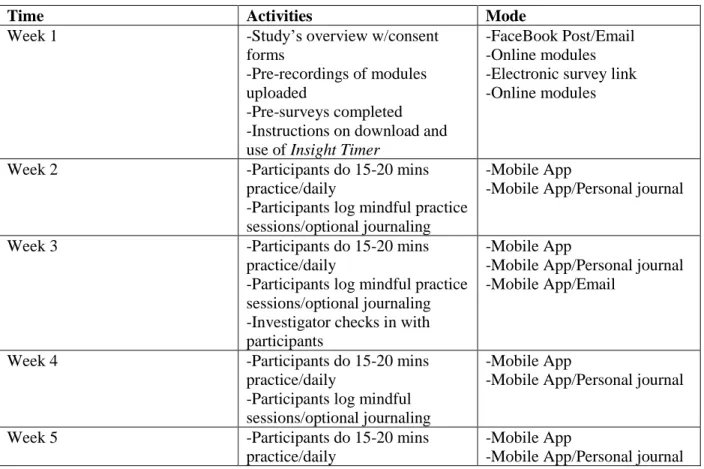
Throughout this phase of the project, participants were encouraged to journal their experiences. Paying purposeful attention and journaling provided yet another outlet to focus on self as the Human Caring Theory emphasized. The author supplied the participants with her contact information and made herself readily available if any questions or concerns aroused. The author used her experience obtained through a traditional in-person, 8-week MBSR course at the University of North Carolina-Chapel Hill in December 2017 and used the resources to manage questions. There were two formal check-ins conducted by the author to assess participants’ journey through the intervention; this was done through the FaceBook group page, personal email and the mobile application group message page at midpoint and post intervention (see Table 1).
Table 1. Project Timeline
Time Activities Mode
Week 1 -Study’s overview w/consent forms
-Pre-recordings of modules uploaded
-Pre-surveys completed -Instructions on download and use of Insight Timer
-FaceBook Post/Email -Online modules -Electronic survey link -Online modules
Week 2 -Participants do 15-20 mins practice/daily
-Participants log mindful practice sessions/optional journaling
-Mobile App
-Mobile App/Personal journal
Week 3 -Participants do 15-20 mins practice/daily
-Participants log mindful practice sessions/optional journaling -Investigator checks in with participants
-Mobile App
-Mobile App/Personal journal -Mobile App/Email
Week 4 -Participants do 15-20 mins practice/daily
-Participants log mindful sessions/optional journaling
-Mobile App
-Mobile App/Personal journal
Week 5 -Participants do 15-20 mins practice/daily
-Mobile App
Time Activities Mode
-Participants log mindful sessions/optional journaling
Week 6 -Post-surveys completed
-Investigator’s final check in with participants
-Thank you email sent to participants
-Rough data findings shared with participants
-Selecting participant for incentive drawing
-Electronic survey link -Mobile App/FaceBook Post/Email
-FaceBook Post/Email -FaceBook Post/Email -FaceBook Post/Email
Instruments for Data Collection. Data was collected pre and post intervention through an electronic link. In order to protect the participant’s anonymity yet be able to match responses, Damrosch’s (1986) self-generated codes strategy was used (see Appendix F) (Damrosch, 1986; Garvey Wilson, Hoge, McGurk, Thomas, & Castro, 2010). The first instrument was the
Professional Quality of Life (ProQOL) tool (see Appendix G). Permission to use this tool was granted and can be found in Appendix H. The second instrument was the Mindful Attention Awareness Scale (MAAS) (see Appendix I). Permission was also granted for the use of this tool (see Appendix J).
compassion satisfaction, a protective measure against compassion fatigue, burnout and secondary traumatic stress, both risk factors and subcomponents for compassion fatigue (Cocker & Joss, 2016; Figley, 1995). Although both subscales of burnout and secondary traumatic stress demonstrate the negative affect of compassion fatigue, likely reflecting the individual’s feeling of distress, secondary traumatic stress addresses fear, while burnout does not. The two subscales share an intra-scale variance of 34% (r= .58; co-α= 34%; n=1187). The ProQOL is scored in three steps; first, some items are reversed, then the items are summed by subscale, and finally, the raw scores are converted to t‐scores; higher scores represent higher levels of each
subcomponent of compassion fatigue (Stamm, 2010).
CHAPTER 4: RESULTS Data Analysis
The purpose of this implementation and evaluation project was twofold. One of the goals of the project was to assess the use of the ProQOL to help military healthcare providers self-identify risk of compassion fatigue. Another goal of the project was to determine if the use of an abbreviated MBSR program involving a mobile application and integrated web-based tools would help decrease symptoms of compassion fatigue and its components among a targeted military provider population of active duty WHNPs.
Sample Characteristics
Although 62 active duty WHNPs were recruited for the project, six active duty WHNPs enrolled. Two of the recruited participants did not complete pre-intervention surveys, log practice sessions in the mobile application or complete post-intervention surveys. Four participants completed the project. All four participants were female, at least 35 years old, married or in a relationship and had children. Of these four participants, one had a Master of Science in nursing and the other three had a Doctor of Nursing Practice degree. Each participant held the role of WHNP for at least five years, were in the military for a time range of 12 to 22 years, held various leadership positions and reported that they worked at least 45 hours per week. All four participants self-identified as religious or spiritual. Half of the participants (n= 2)
reported that they had no experience with mindfulness, yoga or meditation. The sample had one representative each from the following race/ethnicity: white/Caucasian, black/African-American, Asian/Pacific Islander and Hispanic.
Pre- and Post- Intervention ProQOL Scores
Scores mean different things for each subscale of the ProQOL. Regarding burnout and secondary traumatic stress scales, higher scores correlate with higher burnout and stress levels. The compassion satisfaction scale scores represent how well protected a participant is against compassion fatigue, the higher the score, the more resilience against compassion fatigue.
Pre-intervention, 75% (n= 3) of the participants had average burnout scores on the ProQOL, while 25% (n= 1) of the participants had a low burnout score on the scale.
Post-intervention, 75% (n= 3) of the participants had low burnout scores; one
participant’s score remained average, but raw scores trended towards lower burnout (raw score of 30 pre-intervention to raw score of 25 post-intervention). Post-intervention, 75% (n= 3) of the participants’ secondary traumatic stress scores were low; while one participant’s secondary traumatic stress score was average, that participant’s raw scores trended towards lower secondary traumatic stress (raw score of 35 pre-intervention to raw score of 25
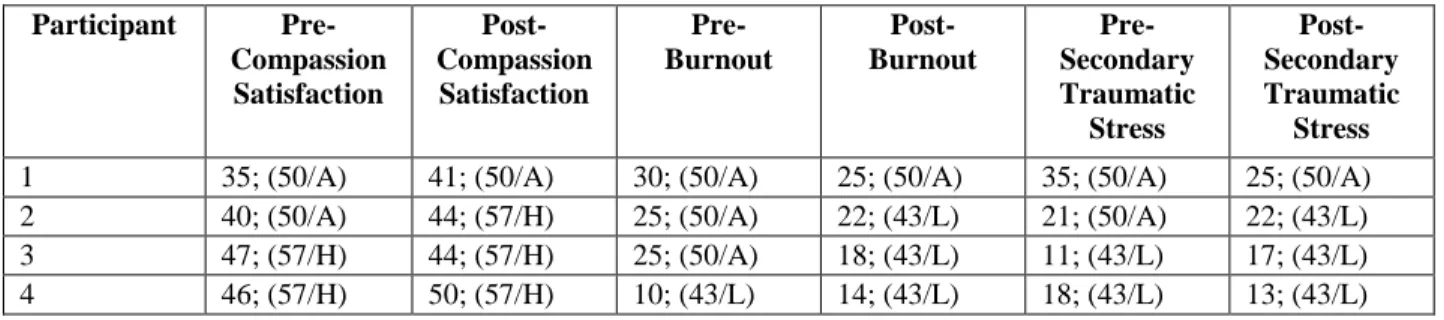
post-intervention). Lastly, 75% (n= 3) of the participants scored high for compassion satisfaction, with one participant remaining average for the measure, but trending towards higher in the measure with her raw scores, post intervention (raw score of 35 pre-intervention to raw score of 41 post-intervention) (see Table 2).
Table 2. Participants’ Pre- and Post- ProQOL Scores Across Three Subscales
Participant Pre-Compassion Satisfaction Post- Compassion Satisfaction Pre- Burnout Post- Burnout Pre- Secondary Traumatic Stress Post- Secondary Traumatic Stress
1 35; (50/A) 41; (50/A) 30; (50/A) 25; (50/A) 35; (50/A) 25; (50/A) 2 40; (50/A) 44; (57/H) 25; (50/A) 22; (43/L) 21; (50/A) 22; (43/L) 3 47; (57/H) 44; (57/H) 25; (50/A) 18; (43/L) 11; (43/L) 17; (43/L) 4 46; (57/H) 50; (57/H) 10; (43/L) 14; (43/L) 18; (43/L) 13; (43/L) Key: The first number in each row is the participant’s raw score, followed by their converted scores. A = average, L = low, H = High.
Pre- and Post- Intervention MAAS Scores
Participants were encouraged to engage in a mindfulness practice of choice, found under the MBSR heading in Insight Timer, for 15 to 20 minutes a day for four weeks. The logged time in the mobile application for the participants’ practice sessions ranged from 10.8 minutes to 122 minutes per day. All four participants increased their mindfulness per the MAAS post
post-intervention goal of this project. Participant pre- and post-post-intervention MAAS results can be seen on Table 3.
Table 3. Participants' Pre- and Post- MAAS Scores
Participant Pre-Intervention Post-Intervention
1 2.8 3.86
2 3.46 3.53
3 3.46 3.73
4 3.46 4.6
Participants’ Reflections
At the mid-point and end of the project, participants were asked several questions to assess the intervention’s effect on their work/life balance. These questions were also asked to assess the feasibility of using the mobile application to practice MBSR. These specific questions were: 1. How has the journey been for you at this point? 2. Are there any challenges that you’ve come across in completing the daily exercises? 3. Have you noticed any changes in your
work/life routines? 4. Any changes in how you are providing patient care?
During the mid-point check-in session, participants indicated that they were enjoying the designated “carved-out” time for practicing mindfulness, although they were finding it
challenging as to when, specifically, were they going to take the time to practice. At this point, they did not necessarily see changes in their work/life routines or how they were providing patient care but, they did report that they were starting discussions with their coworkers on tools to become more resilient at work.
CHAPTER 5: DISCUSSION
There were two aims of this project. The first was to assess the use of the ProQOL to see if it could help a targeted group of military healthcare providers self-identify risk of compassion fatigue. The second aim was to determine if the use of an abbreviated MBSR program involving a mobile application and integrated web-based tools would help decrease symptoms of
compassion fatigue among these targeted military provider population of active duty WHNPs. Initially, six active WHNPs agreed to participate in the project, using the mobile application, Insight Timer, to practice mindfulness activities daily for four weeks. However, only four of the
six active duty WHNPs who enrolled completed the project.
fatigue (Burgess et al., 2017; Cocker & Joss, 2016; Gilmartin et al., 2017; Lamothe et al., 2016; Luken & Sammons, 2016; Mensah & Anderson, 2015).
Previous studies on mindfulness-based interventions specifically for healthcare providers, demonstrated that the more successful interventions were brief and easily assessible (Gilmartin et al., 2017). This project utilized a mobile application called the Insight Timer to meet these
successful attributes. In 2018, Pospos et al, discussed key features of the app to include: free download capability, in app session tracking, in app reminders, a built-in timer, and a user interactive network; they indicated that the mobile application was useful and doable.
Participants in this project reported that they found the application easy to use and enjoyed the variety of activities that it had to offer.
Participants were encouraged to practice MBSR activities for 15 to 20 minutes a day. The participants’ practice sessions varied, ranging from 10.8 minutes to 122 minutes per day.
Overall, the participants reported feeling less stressed, more focused, more mindful of their surrounds, attitudes and feelings and started discussing resiliency with their coworkers and patients. At the end of the intervention, participants did not find that the care that they provided to their patients was directly impacted by their use of mindfulness. Interestingly, one participant reported she began sharing the intervention with her patients, which may have an impact on her practice and the patients’ outcomes.
Limitations
Limitations of this project include participant selection, intervention design and implementation, and participants’ pre-knowledge and expectations.
project, but only four of those participants completed the project in its entirety, representing only 6% of the targeted population. Approximately six months prior to the start of the project, an exploratory assessment of the local problem was initiated by a FaceBook post question on a WHNP page. The question was: What are your thoughts on compassion fatigue and how it relates specifically to your professional and personal roles? Several WHNPs indicated that compassion fatigue was a problem with negative effects on their professional and personal lives. They expressed concerns with dealing with emotionally taxing patients’ diagnoses, such as miscarriages and infertility, and finding time after work to decompression from the stressors of their professional roles. All the respondents of this exploratory assessment were civilian, non-active duty WHNPs. When this project was in the planning stages, the focus was on a
convenience sample of active duty WHNPs, as they appeared to be easily assessible without going through the bureaucracies of official military channels to assess subjects. In retrospect, a more robust sample could have been recruited from a larger, more diverse population through social media and personal email accounts. Future studies would benefit from a larger sample size. It could also be informative to extend the sample to providers of various medical
specialties, such as, family practice, surgical and emergency services, since they share stressors of continual patient management, high risk procedures and life-saving measures. Future studies could also benefit from randomization with a control and experimental group to further assess the intervention’s validity and reliability.
Intervention Design and Implementation. Based on the of the literature on the effects of mindfulness-based interventions on compassion fatigue and its components of burnout and secondary traumatic stress in US military healthcare providers, this project involved the
web-based tools to help decrease symptoms of compassion fatigue among a targeted military provider population of active duty WHNPs. Although previous studies showed positive
correlations with brief, easily assessible mindfulness-based activities and a decrease in healthcare provider compassion fatigue symptoms, some studies suggested that the traditional, in-person, 8-week MBSR program, may provide the added benefit of group collaboration and support among participants (Gilmartin et al., 2017; Mensah & Anderson, 2015; Taylor et al., 2016). The
participants in this study were not geographically located in the same place and only had the opportunity to have contact with one another via the mobile application and online channels. Although participants posted comments through these channels, they did not appear to make direct contact with one another. There is no way of knowing if their outcomes may have been different with the traditional, in-person, 8-week MBSR program. Future studies may want to compare traditional in-person program and an asynchronous modified abbreviated program as designed for this project.
This project was two folded. It looked at assessing a problem and the feasibility of an intervention to help decrease negative effects of the problem. Both goals were lumped together in a total of six weeks. Perhaps, future studies may be designed in two phases: problem
Participants’ Pre-Knowledge and Expectations. According to Dr. Kabat-Zinn and
other researchers, mindfulness can be a challenging phenomenon for some to understand
(Mensah & Anderson, 2015). Therefore, to better acquaint participants with mindfulness, as well as compassion fatigue, informational modules were pre-recorded by the author and available online to be accessed at the participants’ convenience throughout the intervention phase of this project. Due to these informational sessions, participants’ prior knowledge on what the literature presented regarding the benefits of mindfulness may have consciously or subconsciously
affected their outcome measure scores. Additionally, all collected information on the participants were self-reported, therefore outcome results may have reflected what the participants assumed that they should be, instead of what they really were. Future studies may want to focus on the observation of pre-intervention scales without giving the participants prior knowledge of the benefits of mindfulness to see any changes in post-intervention scales. Also, future studies may want to use a more objective way in gathering information on the participants that extend beyond self-report.
Recommendations for Practice
Some of these barriers may include leadership support/buy-in, time constraints/workload, and lack of understanding or acceptance of the concept of mindfulness.
Leadership and management support in any organization is vital to the assurance of product goals, quality and improvement. This could not be truer in the healthcare, when the end-product is healthy human life. Leaders in the healthcare industry may find themselves
succumbing to the pressures of a decreasing supply of medical personnel, equipment and funds and the demands of an increasing patient population, who are living longer lives that include complex health and socioeconomic statuses. Healthcare managers may not prioritize the individual needs of clinicians in the grand scheme of these mounting pressures of production. They may need to be educated about the negative outcomes that compassion fatigue could have on not only staff, but inevitably patients (Cocker & Joss, 2016; Figley, 1995; Nolte, Downing, Temane, & Hastings-Tolsma, 2017). Prior to implementing mindfulness as an intervention to combat against compassion fatigue in a provider population, the management/leadership team of the targeted population can be made aware of the evidence. Mindfulness can be a tool that leaders could support to help keep medical personnel actively engaged and satisfied with employment, keeping them in the business of providing healthcare to patients.
With the seemingly endless demands on the US healthcare industry and shortage of clinicians, providers may find themselves stressed, unable to find a healthy work/life balance, much less time to dedicate to their own self-care. This can be especially true during busy eight and twelve-hour work days. Mensah & Anderson (2015) conducted a systematic review of the literature and found that time constraints and workload presented barriers to mindfulness practice among healthcare providers. Participants of this project reported that setting aside time to
flowed comfortably with the rhythm of their days. Mindfulness-based stress reduction (MBSR) usually entails approximately eight weeks of 2.5 to 3 hours classes once a week, daily practice outside of class and one full day of a mindfulness retreat (Duchemin et al., 2015). Studies that incorporated modified versions of MBSR in Mensah & Anderson’s (2015) review were well received and still showed positive impacts of staff stress levels; modifications included total length of program and time spent in classes. In this project, participants were encouraged to practice mindfulness-based activities for 15 to 20 minutes a day. Although the time the
participants engaged in the activities ranged from 10.8 to 122 minutes per day, they all increased their mindfulness post-intervention. Implementation of a MBSR intervention for busy healthcare providers could include class sessions that meet for shorter than 1 hour at a time, offer
communication through online and telephone modems and have mobile device application content for personalized practice. Prior to implementation, the intervention facilitator could survey that targeted population and strategize on the most conducive schedule for the participants.
Though subtle changes can seem like paradigm shifts to some, education can be the key to greater understanding and lead to smoother transition. Healthcare providers, generally, like to be presented with evidence prior to embracing change. Prior to implementing mindfulness as a defense against compassion fatigue, healthcare providers should be presented with background information on the “fourth aim” of the Institute of Healthcare Improvement’s (IHI) initiative to improve healthcare and how the literature shows evidence on the positive correlation of
Anderson, 2015). For this project, pre-recorded modules were posted online for the participants to access at their convenience. They were intended to give the participants background
information regarding compassion fatigue and elements of mindfulness-based practice. Based on the participants’ post-intervention scale scores, the modules may have been beneficial in
supplying the participants with insight regarding problem and intervention. However, it may have been more beneficial to post the modules prior to sample recruitment, so that the targeted audience may have been more informed and potentially more willing to enrolled in the project. Both participants and their leadership team should be made aware of what the intervention will cost them up front as well, as Mensah & Anderson (2015) pointed out in their article that another barrier to MBSR implementation was lack of funding for an expensive program (typically
ranging from $250 to $500 per person in total cost). A proposed intervention could be void of financial cost per participant because it could be done virtually over the internet and through a free mobile device application download, as was done in the design of this project.
application that does not require online connection (data plan or WiFi usage) which was a barrier for mindfulness practice for participants of this project.
Conclusions
The Institute of Healthcare Improvement’s initiative to improve population health while enhancing patient experience and reducing the cost of healthcare, cannot be achieved without the recently added forth aim of this initiative- improving the work/life balance of healthcare
clinicians and staff. Clinicians and staff are charged with the great responsibility of providing quality healthcare to the masses, therefore, they are the healthcare industry’s most important commodity, supplying human resources. Since the forth aim was added, the US healthcare industry has seemingly paid lip-service to the goals of providers’ resiliency and self-care. However, with the ever-increasing demands of a growing patient population, who are living longer lives that include complex health and socioeconomic statues, providers’ needs are often placed on the back burner. Consequently, this strain may lead to provider personal emotional and physical distress, eventually manifesting into negative patient outcomes. Jean Watson’s Human Caring Theory outlines the importance of caring relationships among healthcare team members, their patients and themselves to be able to meet the challenges of providing superior healthcare. Human relationships require the key elements of caring, communication and resiliency. This project attempted to highlight these elements within a sample of active duty WHNPs.
APPENDIX A: TOOLS TO REVIEW THE LITERATURE
This appendix includes PICOT(S) question, key words for searching and the PRISMA graph. PICOT(S) Question: In active military healthcare providers, can mindfulness mitigate the negative symptoms of compassion fatigue?
Key Words: military search
("compassion fatigue" OR burnout OR "burn out") AND (military OR army OR navy OR marine* OR "air force" OR veteran OR veterans OR soldier* OR "coast guard" OR "active duty" OR officer*) AND mindful*
Provider- not military
("compassion fatigue" OR burnout OR "burn out") AND mindful* AND (provider* OR practitioner* OR doctor* OR physician*)
Databases: Pubmed, Embase, PsycInfo, CINAHL
Inclusion and Exclusion Criteria: English language, United States focused, time-period of 2008 to present (representative of IHI’s triple initiative), research studies not just stories in journals; not focused on patients, family members or students (may include residents/interns)
PubMed
1 Military OR army OR navy
OR marine* OR “air force” OR veteran OR veterans OR soldier* OR “coast guard” OR “active duty” OR officer*
469876
2 mindful* 6700
3 Compassion fatigue OR
burnout OR “burn out”
12945
4 Provider*OR practitioner*
OR doctor* OR physician*
644382
5 1+2+3 9
6 4+2+3 91
CINAHL
1 Military OR army OR navy
OR marine* OR “air force” OR veteran OR veterans OR soldier* OR “coast guard” OR “active duty” OR officer*
42814
2 mindful* 3085
3 Compassion fatigue OR
burnout OR “burn out”
4532
5 1+2+3 2
6 4+2+3 41
Embase
1 Military OR army OR navy
OR marine* OR “air force” OR veteran OR veterans OR soldier* OR “coast guard” OR “active duty” OR officer*
380168
2 mindful* 8630
3 Compassion fatigue OR
burnout OR “burn out”
9557
4 Provider*OR practitioner*
OR doctor* OR physician*
521983
5 1+2+3 12
6 4+2+3 175
PsychInfo
1 Military OR army OR navy
OR marine* OR “air force” OR veteran OR veterans OR soldier* OR “coast guard” OR “active duty” OR officer*
45272
2 mindful* 10686
3 Compassion fatigue OR
burnout OR “burn out”
6741
4 Provider*OR practitioner*
OR doctor* OR physician*
53994
5 1+2+3 12
PRISMA 2009 Flow Diagram
Scr ee ni ng Inc lu de d El igi bi lity Iden tific ation Records identified through PubMed (100), CINAHL (43), Embrase (187), PsychInfo (96)
database searching (n = 426)
Additional records identified through other sources
(n = 0)
Records after duplicates removed (n =175) Records screened (n =175) Records excluded (n =135) Full-text articles assessed for eligibility
(n =40)
Full-text articles excluded, with reasons
as stated above in inclusion/exclusion
criteria (n = 22)
APPENDIX B: PROJECT RECRUITMENT EMAIL/FACEBOOK POST Dear esteemed colleagues,
I’m Major Natasha Best, an AD USAF WHNP, currently attending the University of North Carolina-Chapel Hill on a full-time AFIT scholarship to earn my DNP. To provide high quality healthcare to TriCare beneficiaries, we must also be able to properly take care of ourselves.
As an AD WHNP, you are invited to participate in my DNP project focused on using mindfulness-based stress reduction (MBSR) to combat the negative symptoms of compassion fatigue. This project is based on an abbreviated version of the well-researched 8-week MBSR program developed by Dr. Jon Kabat-Zinn.
Participants will be asked to practice any exercise of choice, found under the MBSR heading in Insight Timer (a mobile application), for 15 to 20 minutes a day for four weeks. Additionally, participants will be encouraged to pay purposeful attention to their emotional, mental and physical responses both at work and at home. Participants will be asked to
anonymously complete two surveys prior to initiation and upon completion of the intervention through an electronic survey link. Two formal check-ins by email and the mobile application group message page will be led by me to assess participants’ journey through the intervention at midpoint and post intervention.
Participation in this project will be exclusively open to AD WHNPs, completely voluntary and will only require a small amount of your valuable time. Participants completing the project will be entered in a drawing to win a $200 gift card. I will provide pre-recorded informational modules, available online to be accessed at the participants’ convenience throughout the intervention phase, to help expand your understanding of the project and build your self-care tool-box.
If you are interested in adding another tool to your self-care tool box, please sign up now at this link: https://unc.az1.qualtrics.com/jfe/form/SV_aXleb5Q3Fwvsg6N . If you have any questions or concerns, please feel free to email me at [email protected],
[email protected] or [email protected]. The project will start in two weeks. I look forward to engaging in this life changing experience with you!
Thanks in advance,
Maj Natasha Best, WHNP-BC
APPENDIX C: CONSENT FORM University of North Carolina at Chapel Hill
Consent to Participate in an Evaluation Project Adult Participants
Consent Form Version Date: __May 8, 2018__ IRB Study #: ________
Title of Study: Targeting Military Healthcare Providers to Self-Identify and Take Action Against Compassion Fatigue: Can Mindfulness Practice Be the Answer?
Principal Investigator: Natasha Best
Principal Investigator Department: School of Nursing Principal Investigator Phone number: 706-339-6384
Principal Investigator Email Address: [email protected] Faculty Advisor: Dr. Carol Durham
Faculty Advisor Contact Information: (919) 966-1753
_________________________________________________________________ What are some general things you should know about evaluation projects?
You are being asked to take part in an evidenced-based project. To join the project is voluntary. You may refuse to join, or you may withdraw your consent to be in the project, for any reason, without penalty.
Evidence-based projects are designed to test existing knowledge. This information may help people in the future. You may not receive any direct benefit from being in the project. There also may be risks to being in evidence-based projects.
Details about this project are discussed below. It is important that you understand this information so that you can make an informed choice about being in this project.
You will be given a copy of this consent form. You should ask the principal investigator (PI) named above, or staff members who may assist them, any questions you have about this project at any time.
What is the purpose of this evaluation project?
The purpose of this project is to focus on using mindfulness-based stress reduction (MBSR) to combat the negative symptoms of compassion fatigue. This project is based on an abbreviated version of the well-researched 8-week MBSR program developed by Dr. Jon Kabat-Zinn. By engaging you in this project, we hope to positively encourage you to build your toolkit of self-care to protect yourself as well as others from the negative symptoms of compassion fatigue. Ideally, you may also pass on this knowledge and skills to future colleagues and patients through informal discussions and formal education.
As a background, clinicians in the United States, expanding all specialty areas, are vulnerable of developing compassion fatigue as they battle against the constant pressures of a decreasing supply of medical personnel, equipment and funds and the demands of an increasing patient population, who are living longer lives that include complex health and socioeconomic statuses. Like their civilian counter parts, military healthcare providers are at risk of compassion fatigue. Both anecdotal evidence and data collection have demonstrated that healthcare team members inability to self-identify, manage and recover from compassion fatigue can lead to personal emotional and physical distress which can eventually manifest into negative patient outcomes. Studies have shown a relationship between mindfulness interventions and reduction of
compassion fatigue and its components of secondary traumatic stress and burnout among healthcare providers.
You are being asked to be in the project because you are an active duty military provider. As such, you are a health care professional who may be affected by the negative symptoms of compassion fatigue.
How many people will take part in this evaluation project? There will be approximately 10-20 people in this project. How long will your part in this project last?
The total time estimate for your active involvement in this project ranges from 6 ½ hours to over 8 hours (over the course of 6 weeks). Going through the informational module, downloading the mobile app and taking the pre-survey, will be approximately 1 hour on the first week. You should expect to spend 15-20 minutes a day on the individual MBSR exercises (during weeks 2-5; an average of around 5 hours total). You should spend around 15 minutes on the post-survey (at the end of week 6). The optional check-in questionnaires during weeks 3 and 6 should take no more than 10 minutes each time. The optional Facebook time may be as little or as much as you choose to spend. You may expect it to average 1 hour total if posting a few comments every week during weeks 1-6. The project will end mid-semester, Fall 2018.
After project completion, there is no planned follow-up, although you are encouraged to continue talking to each other about compassion fatigue and mindfulness.
What will happen if you take part in the project?
You will be part of a project focused on using MBSR to combat the negative symptoms of compassion fatigue over a time period of 4 weeks. For the sake of convenience, participation in the project requires only electronic interactions. The project is designed to focus and support your self-care by 1) discussing self-identification of compassion fatigue; 2) raising your awareness of how its negative symptoms can affect you and your patients; and 3) providing mindfulness tools to combat compassion fatigue symptoms in the future. You will be asked to:
- Review short informational modules
- Download the Insight Timer mobile app (week 1)
- Complete daily 15 to 20 minutes MBSR exercises via the mobile app (week 2-5) - Optionally join a Facebook site
- Complete two optional questionnaires (week 3; week 6) What are the possible benefits from being in this project?
Evidence-based projects are designed to benefit society by testing existing knowledge. The benefits to you from being in this project may be improved knowledge of personal coping techniques or self-care using MBSR. In a general sense, it is to be hoped that you will be able to adapt content beyond your own self-care to provide information to future patients.
What are the possible risks or discomforts involved from being in this project?
We except that most of you will find this project to be a positive experience. However, a small possibility exists that during the course of this project, you may identify and express distress. In this unlikely event, the PI will refer you to your primary care manager (PCM). If, in the course of this project, any possible breach of confidentiality occurs, you, the School of Nursing, and the research project’s faculty advisor will be immediately notified.
A small, highly unlikely, possibility exists that the Facebook site may be misused by
participants’ posting derogatory or unprofessional remarks. We consider this behavior highly unlikely, but the PI will read site content on a daily basis and take down any inappropriate posts.
There may be uncommon or previously unknown risks. You should report any problems to the investigator.
What if we learn about new findings or information during the project?
You will be given any new information gained during the course of the project that might affect your willingness to continue your participation.
How will information about you be protected?
This consent form, with your name and email, will be collected and stored separately from survey results in a secure, locked location when not in use. Only the PI and faculty advisor will have access to individually identifiable data. You will be provided with a copy of Damrosch’s (1986) anonymity code to be used on all survey results. The anonymous code will also be used in data storage and analysis.
The Insight Timer app and Facebook site will not be anonymous. You should be reminded that although researchers will do their best to retain your confidentiality, anything you post online will not be anonymous. Qualitative data will be summarized thematically and anonymously in analysis.
All data will be stored on the hard drive of a password-protected computer.
project could be reviewed by representatives of the University, research sponsors, or
government agencies (for example, the FDA) for purposes such as quality control or safety. You must agree not to reveal anything you learn from group discussions or other activities. What will happen if you are injured by this project?
All research involves a chance that something bad might happen to you. This may include the risk of personal injury. In spite of all safety measures, you might develop a reaction or injury from being in this project. If such problems occur, the researchers will help you get medical care, but any costs for the medical care will be billed to you and/or your insurance company. The University of North Carolina at Chapel Hill has not set aside funds to pay you for any such reactions or injuries, or for the related medical care. You do not give up any of your legal rights by signing this form.
What if you want to stop before your part in the project is complete?
You can withdraw from this project at any time, without penalty. The investigators also have the right to stop your participation at any time. This could be because you no longer meet inclusion criteria, have failed to follow instructions, or because the entire project has been stopped.
If you decide to withdraw, you will no longer be able to complete the intervention. Please notify the PI in writing of your decision to withdraw.
Will you receive anything for being in this project?
As an incentive, at the end of the project, a drawing based on chance will be held in which each participant who completes the entire project, including pre and post surveys, will have an equal chance at winning a $200 gift card. However, there is no guarantee that you will receive any benefits or incentives for participating.
Will it cost you anything to be in this project? It will not cost you anything to be in this project. What if you are a UNC student?
You may choose not to be in the project or to stop being in the project before it is over at any time. This will not affect your class standing or grades at UNC-Chapel Hill. You will not be offered or receive any special consideration if you take part in this project.
What if you have questions about this project?
You have the right to ask, and have answered, any questions you may have about this project. If you have questions about the study (including payments), complaints, concerns, or if a research-related injury occurs, you should contact the researchers listed on the first page of this form. What if you have questions about your rights as a project participant?
Review Board at 919-966-3113 or by email to [email protected]. Participant’s Agreement:
I have read the information provided above. I have asked all the questions I have at this time. I voluntarily agree to participate in this project.
I DO □ DO NOT □
____________________________________________________
Email of Project Participant (for electronic communication and surveys)
____________________________________________________ Signature of Project Participant
___________________ Date
APPENDIX E: LIST OF MODULES AND SAMPLE NARRATION Module 1: The overview of the project
Module 2: Instructions on how to complete pre and post surveys Module 3: Downloading and use of the mobile application Module 4: Logging of sessions/journaling
Module 5: The background and history of MBSR Module 6: Body Scan
Module 7: Mindful movement Module 8: Walking meditation Module 9: Sitting meditation
Module 10: An overview of compassion fatigue and its subcomponents of burnout and STS
*Lead Investigators’ voice over PowerPoint presentation; source: (Greater Good in Action: Science-Based Practices for a Meaningful Life website, 2018) *
Body scan:
The body scan provides a rare opportunity for us to experience our body as it is, without judging or trying to change it. It may allow us to notice and release a source of tension we weren’t aware of before, such as a hunched back or clenched jaw muscles. Or it may draw our attention to a source of pain and discomfort. Our feelings of resistance and anger toward pain often only serve to increase that pain, and to increase the distress associated with it; according to research, by simply noticing the pain we’re experiencing, without trying to change it, we may actually feel some relief.
The body scan is designed to counteract these negative feelings toward our bodies. This practice may also increase our general attunement to our physical needs and sensations, which can in turn help us take better care of our bodies and make healthier decisions about eating, sleep, and exercise.
This exercise asks you to systematically focus your attention on different parts of your body, from your feet to the muscles in your face. It is designed to help you develop a mindful awareness of your bodily sensations, and to relieve tension wherever it is found. Research suggests that this mindfulness practice can help reduce stress, improve well-being, and decrease aches and pains.
The body scan can be performed while lying down, sitting, or in other postures. These following steps are a guided meditation designed to be done while sitting.
Begin by bringing your attention into your body. You can close your eyes if that’s
any sensation in your arms. Let your shoulders be soft. Notice your neck and throat. Let them be soft. Relax. Soften your jaw. Let your face and facial muscles be soft. Then notice your whole-body present. Take one more breath. Be aware of your whole whole-body as best you can. Take a breath. And then when you’re ready, you can open your eyes.
APPENDIX F: SELF-GENERATED CODES FOR SURVEYS This appendix is based off Damrosch’s 1986 study on anonymity. Online link: https://unc.az1.qualtrics.com/jfe/form/SV_1FX110JVsexKatD
Please carefully read and fill in the following information to establish your own personal code to help maintain your anonymity throughout this project:
1. Please enter the FIRST letter of your mother’s maiden name: _____ 2. Please enter the FIRST letter of your father’s first name: _____ 3. How MANY children do you have? _____
4. How MANY OLDER siblings do you have? _____ 5. How MANY YOUNGER siblings do you have? _____
6. What MONTH (IN NUMBER) were you born? (01-Jan/02-Feb/03-Mar/04-Apr/05-May/06-Jun/07-Jul/08-Aug/09-Sep/10-Oct/11-Nov/12-Dec) ____
APPENDIX G: THE PROFESSIONAL QUALITY OF LIFE SCALE (PROQOL)
APPENDIX I: MINDFUL ATTENTION AWARENESS SCALE (MAAS)