THE TEST-RETEST RELIABILITY AND EXERCISE-DRIVEN CHANGES OF UCH-L1 IN HEALTHY, RECREATIONALLY ACTIVE COLLEGE STUDENTS
Grant Hayden Cabell
A thesis submitted to the faculty of the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for graduation with honors in the Department of Exercise and
Sport Science
Chapel Hill 2017
Approved by:
Kevin M. Guskiewicz
Jason P. Mihalik
Erik D. Hanson
©2017
Grant Hayden Cabell ALL RIGHTS RESERVE
ABSTRACT
GRANT HAYDEN CABELL: The Test-Retest Reliability and Exercise-Driven Changes of UCH-L1 in Healthy, Recreationally Active College Students
(Under the direction of Elizabeth F. Teel and Kevin M. Guskiewicz)
Concussions are a common injury in contact sports yet are difficult to diagnose. The current concussion assessment battery is not foolproof, and blood biomarkers are a possible solution to improve sensitivity. To establish clinical utility, a biomarker must remain stable over time and be unaffected by acute exercise. This study investigated the test-retest reliability and acute effect of exercise on UCH-L1 in healthy subjects. Participants (n=30) completed a maximal exercise test during two assessment sessions 10-14 days apart, with blood draws occurring before and after each exercise test. UCH-L1 was highly reliable in males (ICC2,k =0.895), but had poor reliability in females (ICC2,k =0.094). There were no significant changes in UCH-L1 after acute exercise in either sex (t=0.25, p=0.80). UCH-L1 shows potential for utility in males due to its stability, but may have limited utility in females. Further investigation of sex differences in UCH-L1 levels over time is needed.
TABLE OF CONTENTS
CHAPTER 1... 1
Research Questions...3
Research Hypothesis...4
Definition of Terms...4
Operational Definitions...5
Delimitations...5
Limitations... 6
Assumptions...6
Variables...6
CHAPTER II... 8
LITERATURE REVIEW...8
Concussion...9
Prevalence...9
Pathophysiology...11
Symptomology... 11
Concussion Battery Testing...12
Return to Play... 14
Biomarkers... 15
UCH-L1... 17
Summary... 21
CHAPTER III... 22
METHODS... 22
Participants... 22
Instrumentation...22
Screening Instruments...22
Clinical Testing Session Instruments...24
Blood Processing and Analysis Instruments...26
Procedure... 27
Power Analysis... 31
Data Reduction...31
Data Analysis... 32
CHAPTER IV... 34
Results... 34
Participants... 34
Maximal Exercise Test...34
Research Question 1: UCH-L1 Reliability...36
Research Question 2: Effect of Acute Exercise...36
Discussion... 38
Clinical Significance...40
Limitations... 41
Summary... 42
LIST OF TABLES AND FIGURES
Table 1. Stepwise Return to Play Progression...15
Figure 1: EKG Electrode Placement……….24
Table 2: Maximal Exercise Protocol for Healthy Participants...29
Table 3. Maximal Exercise Protocol for Concussed Participants...29
Table 4. Participant Demographics……….. 34
Table 5. Maximal Exercise Test Statistics……….. 35
Table 6. Blood Volume Data………..35
Table 7. Treatment vs. Control Blood Volume Data………..36
Table 8. UCH-L1 Reliability………36
CHAPTER 1
INTRODUCTION
One of the fastest growing fields of interest in sports medicine today pertains to
concussions. From Hollywood movies to millions of dollars in research grants, both the popular culture and medical community have become infatuated with this topic. This fast-growing interest is not unwarranted, as concussions are one of the most prevalent neurological injuries and as many as 3.2 million cases are estimated to occur each year in sports alone.1,2,3
Furthermore, the incidence of annual sport-related concussions (SRC) is probably higher, as some experts estimate the rate of unreported concussions could be as high as 50%.4 Not only is there disconnect on concussion reporting, but experts also have yet to establish a universal definition for concussion. However, many cite that concussions are a pathophysiological
process induced by biomechanical forces that affect the brain.5 Moreover, concussions are often described as functional, rather than structural, injuries, making them difficult to diagnose on neuroimaging technologies due to a lack of observable anatomical damage.5
concussion diagnostic tool, due to the objective nature and lack of practice or learning effects associated with these assessments.
Biomarkers are defined as measureable internal indicators, such as proteins, that reflect changes in organisms while also providing potential information about the mechanism of injury.9 While they have been consistently used in the medical field to diagnose injuries to specific tissues and organs in the body, their use in concussion diagnosis and management has not been widespread, although their potential usefulness remains.10 Premature return to activity, before the brain injury fully heals, represents one of the biggest risks following concussion, as it increases the probability for a life threatening or catastrophic brain injury.11 Using blood
biomarkers in concussion diagnosis and management has the potential to provide a higher degree of certainty in concussion diagnosis, combat barriers to recognition and reporting of concussion (ie. patient disguise of symptoms or underreporting), and provide objective
measures of recovery, decreasing the likelihood of missed diagnosis, premature return to play, and catastrophic injury.
serum levels may theoretically represent neural damage and act as a biomarker of brain
trauma. However, very limited research has been conducted on UCH-L1 in concussed patients, particularly in those with sport-related injury mechanisms. Most of the UCH-L1 data has been taken from large injury databases, which is not standardized to a specific group of people.
While a theoretical model for the inclusion of UCH-L1 as a biomarker of concussion exists, there is still much to be learned in regards to the relationship between UCH-L1 and concussions before it can be used clinically. Though unpublished data from Hayes suggests that the sensitivity and specificity of UCH-L1 is high, other psychometric properties such as reliability of UCH-L1 have yet to be explored.9 As both diagnostic (baseline vs. injury sample) and management (change in biomarker over the course of recovery) biomarker utilization requires serial assessments, establishing the test-retest reliability of UCH-L1 in a healthy sample is a necessary first step. Furthermore, no studies have looked at the relationship of UCH-L1 and acute exercise. As concussions often occur following physical activity in athletic settings, researchers must determine whether exercise affects UCH-L1 levels in healthy participants to understand whether biomarkers levels are altered in the absence of an injury. This is critical to making appropriate diagnostic decisions following a potential concussion.
Research Questions
1. What is the test-retest reliability of UCH-L1 in healthy (non-concussed) recreational athletes over a 10-14 day period?
2. What is the effect of acute exercise on UCH-L1 levels in healthy, recreational athletes? Exploratory Research Questions
1. Do serum levels of UCH-L1 differ in recreational athletes with acute concussion (within 3-10 days of injury) compared to non-injured recreational athletes with head trauma exposure but no concussion and non-injured athletes with no exposure to head trauma and no concussion?
2. What is the effect of acute exercise on UCH-L1 levels in acutely concussed (3-10 days after injury) recreational athletes?
Research Hypothesis
1. UCH–L1 will be highly (ICC>0.75)16 reliable in healthy, recreational athletes. 2. There will be no significant changes in UCH-L1 levels following acute exercise in
healthy, recreational athletes. Exploratory Hypothesis
1. Recreational athletes with sport-related concussion (SRC) will have significantly
2. There will be no significant changes in UCH-L1 levels in acutely concussed recreational athletes following exercise compared to their pre-exercise levels.
Definition of Terms
1. Screening Instrument: Questionnaires, monitors, machines, or any other type of tool or data collecting instrument used in the study to determine whether or not a participant is eligible to enroll into this study.
2. Acute Exercise: A single bout of exercise which raises the heart rate substantially above a basal level resulting in the subject exerting effort above a basal level.
3. Maximal Exercise Test: An exercise test using a cycle ergometer where the exercise intensity is gradually increased over time until the participant reaches their maximum oxygen uptake capacity. This was the mechanism of acute exercise in the study. 4. Blood Draw: Procedure in which participants’ blood is obtained through use of a sterile
needle and collection tube.
Operational Definitions
1. Healthy: Individuals that have not been diagnosed with a concussion and do not have any malaises or other malignancies that would put them at risk to undergo a maximal exercise test.
2. Active: Individuals that exercise on a regular basis; participate in moderate to vigorous physical activity for at least 150 minutes each week during at least 3 separate exercise sessions.
1. Individuals with concussions within the last year were excluded from taking part in the study as a healthy participant to prevent any lingering effects from the injury from altering the healthy, active population due to past injury.
2. Individuals who engaged in recreational drug use during the course of the study were excluded from the analysis because it is unknown how drug use could affect the levels of UCH-L1 in the bloodstream.
3. Individuals who had a history of skull fracture or brain bleed in association with their concussive event were excluded from the study because levels of UCH-L1 in their bloodstream could be affected by their injury.
4. Individuals who were UNC Varsity athletes were excluded from the study because their results as elite athletes would not be representative of a healthy, active population.
Limitations
1. Participants were responsible for reporting their own medical and physical activity history and, thus, some participants may have been included in the study who should have been excluded.
2. Participants with concussions were tested, at the earliest, 3 days post injury due to scheduling limitations, which might have been too long post-injury to detect changes in UCH-L1.
3. Participants self-reported drug use during the study and some participants may have been included who should not have been.
5. Participants were chosen based on interest in the study and may not be representative of the general healthy, active population.
Assumptions
1. Participants fully and accurately reported past medical and physical activity histories. 2. Participants gave maximal effort during all exercise tests.
3. The chosen participants were a good representation of the general, healthy, active population.
4. There was no change to participants’ daily routines during the course of the study.
Variables
1. Dependent
a. Serum levels of UCH-L1 2. Independent
a. Time (session) b. Acute Exercise Bout c. Group
CHAPTER II
LITERATURE REVIEW
Due to the current difficulty in diagnosing concussions, many methods into the recognition and identification of concussive injuries are being explored. Current concussion diagnostic methods, such as physician assessments, neuroimaging, as well as clinical balance and cognitive tests, are subject to several limitations that can prevent accurate identification of the injury.9 The emerging field of blood biomarkers, however, could help alleviate these
difficulties as biomarkers have the potential to increase the sensitivity of the concussion battery. Biomarkers are indicators of internal changes at the molecular level in the body, and thus may be able to detect changes inside the body (injury) that may be unrecognizable by the naked eye or the assessment battery used today.9 Specifically, the biomarker ubiquitin C-terminal
hydrolase L1 (UCH-L1) may be particularly sensitive to detecting changes in the brain after head trauma due to its role in the brain’s biological pathway. UCH-L1 has been found to have high expression levels almost exclusively in neurons, and is associated with the metabolism of misfolded proteins and neurodegenerative disorders.17,18 Unpublished data from Hayes suggests that UCH-L1 is both sensitive and specific in patients with mTBI, and it has also been suggested that UCH-L1 is sensitive to injury in patients with severe TBI.9,19 However, the test-retest
of this study is to determine the effect of exercise on UCH-L1 levels in healthy, recreationally active athletes.
Concussion
While it has been known for decades that head impacts can cause alterations in neurological functioning in athletes, the specifics of what defines a concussion have been refined in recent years. Early definitions described concussions as a state of axonal dysfunction that resulted from acceleration and deceleration forces on the brain leading to “shearing forces or distortion of the vascular and neural elements of the brain.”20 However, the concussion definition has been further developed with advances in research and new discoveries to be more encompassing of the full spectrum of concussive injuries. While a universal definition is yet to be agreed upon, current literature typically defines a concussion as a “complex
pathophysiological process affecting the brain, induced by biomechanical forces.”5 Typically, concussions result in the rapid development of short-term impairment of neurological
functionality, but signs and symptoms may also develop over the course of minutes or hours.5 Furthermore, concussions are described as functional deficiency, rather than a structural one, as the injury usually reflects itself in depressed neurologic functionality rather than structural changes; thus, concussions are quite difficult to diagnose using neuroimaging techniques.5 In addition to somatic, cognitive, and emotional symptoms, behavioral changes and physical symptoms are all clinical markers of concussive injuries. Often, these symptoms resolve
themselves gradually over a period of 7-10 days, but in specific instances these symptoms may last much longer.5 It should be noted that while concussive injuries reflect themselves in
Prevalence
One of the most pressing issues associated with sport-related concussions (SRC) is their high incidence rate. It is estimated that over 300,000 SRC occur annually.2 Furthermore, this number is most likely an underestimate of the actual SRC incidence rates, as some experts believe that the annual incidence rate of SRC could be between 1.6 and 3.8 million.4,21 The high number of estimated concussions that go unidentified is due to a multitude of factors, including medical personnel’s difficulty in recognizing symptoms, the disguise or underreporting of symptoms, or the failure of the individual to seek medical attention for his/her injury.
In recent years, studies have found the incidence rate of diagnosed SRC to be
likely to sustain a concussion than males in sports with equivalent rules (ie. soccer,
basketball).25 This discrepancy in concussion incidence rates among the sexes could be due to playing style differences, biomechanical differences, and even cultural differences.25,26
While the overall number of diagnosed concussions have risen in recent years, it is important to note that many researchers and scholars attribute this increase to factors such as increased awareness, increased medical staff at contact sporting events (especially in high school sporting events), and better training for medical staff around concussion recognition due to the increased attention given to SRC in recent years.21 Regardless of the origin for increasing concussion incident rates, the prevalence of concussions in both collegiate and high school settings has generated more interest in learning about concussion pathophysiology, in hopes that by understanding the neurologic underpinnings of the injury researchers may find more effective ways to treat, or even prevent, concussions.
Pathophysiology
Biologically, a concussion is a series of complex metabolic changes that result in functional neurodeficiencies. Concussions are the end result of an energy crisis caused by impacts to the cranium. When a powerful force is imparted on the skull, shearing and stretching forces are imparted on the neurons of the brain. These forces can rupture the cellular
this increased consumption of ATP, there is also a decrease in cerebral blood flow, which results in less energy stores being delivered to the brain. The combined “hypermetabolism with a decreased energy supply” results in an energy crisis, whereby the brain requires increased levels of ATP but is being supplied with lower than normal levels. In addition to the energy imbalance, oxidative metabolism in the mitochondria is impaired by the influx of extracellular K+, leading to an end result of axonal dysfunction. The metabolic dysfunction described here is thought to cause the symptoms and functional deficiencies seen following concussions.27
Symptomology
Common symptoms of concussive injuries can be stratified into somatic, cognitive, and sensory domains.28 Somatic symptoms tend to include headaches, nausea, and vomiting; cognitive symptoms include attentional deficits and memory problems; and sensory symptoms often found are fatigue, drowsiness, and difficulty sleeping.28 The most frequent of these
Concussion Battery Testing
When a concussion occurs, the resulting energy crisis in the brain often leads to functional deficits rather than structural changes.5 As a result, there is no definitive method yet to identify and diagnose a concussion in athletes. However, studies have recommended that a battery of tests be used to evaluate potential concussions.34,5 Along with a recommended physical examination by a trained clinician, the concussion testing battery includes
deficits and symptoms usually take the longest to reside, as their scores often don’t return to pre-injury levels until 7 to 10 days after injury.42
Scores on these tests post-injury can then be used in comparison with baseline scores for the athlete to determine when it is suitable to return to play. A baseline assessment is administered before the beginning of exposure for the athlete. This assessment is made up of the same battery of concussion tests that will be used to examine the athlete after injury. Every concussion and every athlete is different; thus, by having athletes complete a valid baseline, it is ensured that the deviations measured in score are clinically meaningful.43
Several studies have been conducted to examine the sensitivity and reliability of the current battery of concussion assessments; most notably, Broglio et al. in 2007 and Register-Mihalik et al. in 2013. Broglio et al. examined the sensitivity of the assessment battery and found that the sensitivity to concussive injury of each individual test in the battery was between 43 to 79%.8 However, they also found that when the entire assessment was given in
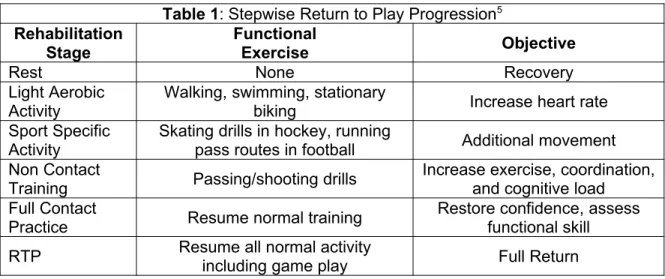
Return to Play
Once a concussion is diagnosed in an athlete, the injury must be monitored carefully to ensure the athlete does not prematurely resume activities, which could put them at risk before their injury is fully healed. If an athlete were to return to play (RTP) too soon, he/she could potentially be at risk for catastrophic injury, such as second impact syndrome. Second impact syndrome occurs when an athlete sustains a second concussive head injury before the first one has completely healed. As a result, the athlete often experiences rapid neurodegeneration and can often experience life-threatening symptoms.4,11 In less severe circumstances, resuming activity before the concussion is fully healed often delays recovery and lengthens the total time lost from injury.44
Table 1: Stepwise Return to Play Progression5
Rehabilitation Stage
Functional
Exercise Objective
Rest None Recovery
Light Aerobic Activity
Walking, swimming, stationary
biking Increase heart rate
Sport Specific Activity
Skating drills in hockey, running
pass routes in football Additional movement Non Contact
Training Passing/shooting drills
Increase exercise, coordination, and cognitive load Full Contact
Practice Resume normal training Restore confidence, assessfunctional skill RTP Resume all normal activityincluding game play Full Return
Once the athlete is asymptomatic at rest, the athlete is instructed to complete
functionality tasks to increase proprioception, range of motion, and flexibility.44 However, care must be taken so that athletes do not over exert themselves, which has been found to increase recovery time and exacerbate concussion symptoms.44 Finally, once the athlete is completely asymptomatic in functional tasks, they can gradually progress (through light aerobic activity to sport specific activities and general training measures) to full participation in their sport once again.5
Biomarkers
identifying interstitial lung abnormalities.9,45,46 By tracking changes through these media, human understanding of the cause, progression, and treatment of disease can be enhanced.46 There are two major types of biomarkers: those for exposure (used in predicting course of illness), and those for disease (used to track progression of disease), which can be detected through any measurable media such as bodily fluids.46,47 Often, though, these biomarkers are measured through extractions of liquid like blood or cerebral spinal fluid (CSF). CSF has been found to yield more accurate levels of many biomarkers produced in the central nervous system;
however, blood is often used because it is easier to draw and less invasive.48 The accuracy and ease of measurement, as well as the potential for high sensitivity and specificity to disease, has made biomarkers useful in relation to internal injuries, specifically head trauma.
Biomarkers Related to Head Trauma
As previously mentioned, concussions can be difficult to detect with neuroimaging devices as structural abnormalities are rare following injury.5 Furthermore, athletes may disguise or choose not to report symptoms, adding additional difficulty to the identification of injury. Additionally, even when diagnosis is correctly made, common evaluation tools may incorrectly assess the severity of injury, as there is no universal scale of measurement for severity of concussion and little prognostic information can be made.49,9 For these reasons, there is hope that blood biomarkers may eventually provide a more concrete method for concussion diagnosis and management. Currently, though, biomarkers are being used to supplement functional and imaging assessments, as a clear marker of concussive injury has proved elusive to find.
(SBDP) 120 and SBDP145 have been found to be elevated in both rats and humans with severe traumatic brain injuries.50,19 The proteins S100B and neuron-specific enolase (NSE) have all also been found to be significantly higher in patients with head trauma than healthy controls. SBDP120 and SBDP145 have only been found to be elevated in patients with severe head trauma, while S100B and NSE have been found to be elevated in patients with moderate TBI.51,52 Due to their mechanisms of injury, NSE and both SBDP biomarkers are hard to study because their levels are not accurate in the blood.51,53 S100B is also difficult to study; while it has been found to be associated with mTBI, it is also present in other tissues as well, which can provide confounding results.54,55 In recent years, however, a novel protein has presented a new opportunity to establish a link between biomarkers and concussive injuries: ubiquitin C-terminal hydrolase L1 (UCH-L1). This biomarker has been found to be both sensitive and specific to moderate and severe head injuries in a hospital setting, but further research is needed to establish a clinical utility for sports medicine.52,56
UCH-L1
Ubiquitin C-terminal hydrolase L-1, or UCH-L1, is one of the most common proteins in the brain and is found almost exclusively in neurons.12 In the brain, UCH-L1 aids in the
trauma and the resulting neuronal damage could cause UCH-L1 to be released out of the neuron and into the extracellular space, passing through the blood-brain barrier and entering the bloodstream.59 However, further research is needed to determine the exact biological pathway that this biomarker acts through.
Due to its novelty, relatively few studies have examined UCH-L1 levels in humans or animal models. However, the existing literature has briefly examined the relationship between UCH-L1 and concussions, both in relation to SRC and concussion occurring outside of sport. In animal models, blood and CSF levels of UCH-L1 were examined prior to and following a
concussion induced through controlled blast overpressure exposure. UCH-L1 was found to accumulate rapidly in the blood 24 hours after blast exposure and then gradually decline after 48 hours until it reached baseline levels 14 days after exposure. UCH-L1 was overexpressed in the bloodstream after neuronal damage, and accumulated rapidly in circulation. Furthermore, expression of UCH-L1 in the CSF was delayed but also increased following blast exposure, and the level of UCH-L1 expression in the CSF varied significantly in individual rats. Svetlov et al. suggested that these results were evidence that the blood-brain barrier is damaged due to blast wave exposure.60 However, these conclusions cannot be generalized to other mechanisms of concussive injuries.
values. Furthermore, it was found that UCH-L1 levels were higher in patients who were injured in assault than in motor vehicle accidents, indicating the mechanisms or severity of injury may potentially influence the expression of UCH-L1 levels. It was also found that UCH-L1 levels tended to peak within 6 hours of admission to the hospital.59
Papa et al. also examined the levels of UCH-L1 in 584 mTBI patients recruited from the emergency room. In this study, patients admitted within four hours of injury were recruited for participation. Both patients with mTBI and controls (patients with traumatic, but not brain-related, injuries) were included. Blood samples were drawn from each participant within four hours of injury, and were continually drawn at 4, 8, 12, 16, 20, 24, 36, 48, 60, 72, 84, 96, 108, 120, 132, 144, 156, 168, and 180 hours following the injury. Using a sandwich ELISA, UCH-L1 levels were found to be significantly higher in the mTBI patients than in the trauma control patients. In the mTBI cohort, UCH-L1 levels were elevated up to 16 hours after injury. Moreover, in mTBI patients with intracranial lesions, the UCH-L1 levels stayed elevated up to 48 hours after injury.52 However, in a pediatric cohort (11-16 years of age, 25 concussed participants, 20 single–extremity orthopedic injury (OI) controls) no statistically significant differences were found in the levels of UCH-L1 between the mTBI group and the OI group.56
Along with diagnosed concussions, a few studies have examined the relationship between UCH-L1 and sub-concussive head impacts. Carr et al. recruited 108 active military personnel to study the relationship of head trauma exposure and UCH-L1 levels. During a two-week period of blast training, participants had their blood drawn daily (on average 2.5 hours after the last blast), which were analyzed using a sandwich ELISA. It was found that 32% of blood samples drawn had UCH-L1 at detectable levels, while 7% contained UCH-L1 at
results show that UCH-L1 is largely unaffected by sub-concussive impacts, or impacts that don’t cause injury. While 39% of the sample showed detectable of quantifiable serum levels of UCH-L1, it is unknown whether these findings have any meaning as no standard cutoff score for UCH-L1 exist in relation to concussion diagnosis. Based upon these results, UCH-L1 could be a valuable biomarker to study as little to no change occurs in relation to clinically insignificant impacts.61
Studies examining the relationship between UCH-L1 and sub-concussive head impacts are not limited to military personnel. Puvenna et al. recruited 15 uninjured varsity collegiate football players and compared their UCH-L1 levels post-game to both positive (concussed) controls and negative (non-concussed) controls recruited from a local hospital. Blood samples were collected before and after games for the players, and within 6 hours of injury in the positive controls. No correlation was found between head trauma exposure and UCH-L1 levels, and UCH-L1 levels failed to accurately identify patients with TBI compared to controls. Like the findings from Carr et al., this study shows that UCH-L1 levels are not elevated due to sub-concussive impacts. However, it raises questions about the sensitivity of the biomarker, as it was unable to accurately differentiate injured and uninjured subjects. This could be due to low power in the study, and further research is needed to verify the results.62
properties of this biomarker, and the information that has been published is variable. One study found the area under the ROC curve measuring 6 hour levels of UCH-L1 in severe TBI vs. controls to be 0.88.58 Another study found the area under the ROC curve for injury time points over seven days to range from 0.30 to 0.67.52 Several authors, though, have labeled the biomarker as sensitive and specific without formal analyses. 61,9 The reliability of biomarker is unknown based upon the current literature, making this the first study to assess the test-retest reliability of UCH-L1.
Additionally, the few studies that have been conducted concerning this biomarker and concussions have presented conflicting results. Research has shown that UCH-L1 levels were not different between injured subjects and uninjured subjects.62 Other studies, though, have shown UCH-L1 has also been found to be associated with injury measures in moderate and severe TBI, but studies with these conclusions have only focused on UCH-L1 levels from hospitalized patients.52,58 Therefore, further research is needed to determine the biomarker’s relationship with concussion and its potential for clinical utility in sports medicine.
Summary
Current identification and diagnostic methods for SRC are not sensitive enough to injury, as it is estimated that thousands of concussions go undetected every year. If concussed
CHAPTER III
METHODS
Participants
This study included 30 healthy, physically active students (14 males; 16 females) and 1 acutely concussed participant (female) selected from the University of North Carolina at Chapel Hill (UNC). Participants were recruited from club and intramural sports, as well as the general student population. Participants were included in the study if they were between the ages of 18-30, engaged in moderate or vigorous physical activity at least 3 days a week (for at least 30 minutes each time), and were in good cardiovascular health. For concussed participants, individuals were recruited at least 72 hours after their injury. Healthy participants were excluded if they engaged in recreational drug use over the course of their participation in the study or had a diagnosed concussion within the past year. Concussed participants were excluded if they had a skull fracture or brain bleed in association with their concussion, which were self-reported on a demographic questionnaire.
Instrumentation
Screening Instruments
Physical Activity Readiness Questionnaire. In order to confirm that participants had
1. Has your doctor ever said that you have a heart condition and that you should only do physical activity recommended by a doctor?
2. Do you feel pain in your chest when you do physical activity?
3. In the past month, have you had chest pain when you were not doing physical activity? 4. Do you lose your balance because of dizziness or do you ever lose consciousness? 5. Do you have a bone or joint problem (for example, back, knee, or hip) that could be made worse by a change in your physical activity?
6. Is your doctor currently prescribing drugs (for example, water pills) for your blood pressure or heart condition?
7. Do you know of any other reason why you should not do physical activity?
The PAR-Q, along with the General Medical History and Electrocardiogram (EKG), were sent to an independent medical monitor prior to enrollment in the study. In general, participants are deemed ready for physical activity if they answered “No” to every question. For this study, participants needed health clearance from the independent medical monitor prior to beginning any data collection sessions. If the medical monitor did not feel participants had sufficient cardiovascular health, they were excluded from participating in this study.
General Medical History Questionnaire. The General Medical History Questionnaire was
used to make sure the participant was healthy enough to complete the exercise testing associated with this study. The questionnaire was comprised of 57 questions that gathered information about the participant’s general health history, family history, mental health history, bone and joint history, and activity history. No study outcomes were obtained from the
questionnaire, as it was used as an inclusion criterion. The General Medical History was reviewed by an independent medical monitor, who had to provide medical clearance for each participant before enrollment into the study.
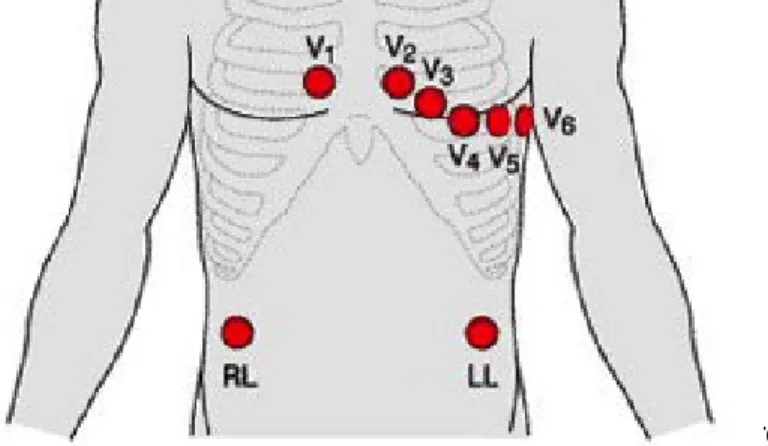
Electrocardiogram (EKG). To ensure participants’ cardiovascular health was sufficient
ensuring the heart could withstand the stress of the maximal exercise test. Five electrodes were placed on the chest of the participant over the heart, while a sixth was placed on the opposite pectoral. Four additional electrodes were placed on the trunk of the participant – two directly below each the clavicle, and two on opposite sides of the abdomen below the rib cage (Figure 1). The participant was asked to sit quietly for 5 minutes, while the EKG was recorded and saved on a computer. No study outcomes were obtained from the EKG; rather, a normal EKG was used as an inclusion criterion.
Clinical Testing Session Instruments
Cycle Ergometer. In this study, a Lode Corival Cycle Ergometer (Lode, Gronigen, The
Netherlands) was used to complete the maximal exercise test. Participants cycled on an electronically braked bike that permitted constant workloads to be maintained without requiring fixed revolutions per minute, allowing for more precise exercise prescriptions during this study. The Corival was used to set the participant’s exercise intensity during the maximal exercise testing. Participant’s VO2peak and resting and maximal heart rate (taken at the termination of the maximal exercise test) will be used as outcomes in this study.
Metabolic Cart. A ParvoMedics TrueOne® 2400 was used throughout the study to
measure gas exchange variables during each maximal exercise test. Participants wore a noseclip and breathed through a mouthpiece attached to a Hans Rudolph 2700-series non-rebreathing valve attached to a Hans Rudolph 2726 head-support during each maximal exercise test. The cart was calibrated according to manufacturer instructions before each clinical testing session. The metabolic cart reported second averages of all data collected. The final 10-second reading of each state of the maximal exercise test protocol was used for analysis.
VO2peak was the only outcome from this study obtained from the metabolic cart; this was used to help determine when the participant had reached maximum exertion.
Incremental Cycle Ergometer Form. The research team completed the Incremental
Cycle Ergometer form during each maximal exercise test to track heart rate and level of
perceived exertion at each stage of testing. Heart rate and total time of maximal exercise test at protocol termination were the study outcomes recorded on this form.
Polar Heart Rate Monitors. Each subject wore a Polar H1 Heart Rate Sensor (Kempele,
Finland) while completing both of the maximal exercise testing sessions. These monitors were strapped to patients around their chest, and could be fitted comfortably under the shirt of the participant. The monitor transmitted data via Bluetooth to a synced watch, including heart rate of the participant throughout the study, which was used as an outcome in this study.
Borg Rate of Perceived Exertion Scale. The Borg Rate of Perceived Exertion (RPE)
Scale measured the participants’ perception of the difficulty of the maximal exercise test. Participants were asked to rate their level of exertion on a scale from 6 (no exertion) to 20 (maximal exertion) 30 seconds before the termination of each stage of the maximal exercise test. The Borg RPE Scale was used along with the VO2peak data, maximal heart rate, and lactate levels to corroborate when the participant had reached their maximum exertion level during the exercise test.
Blood Processing and Analysis Instruments
Centrifuge. After blood collection, a Sorvall ST 8R Centrifuge (Waltham, MA) was used
As a result, the separated serum isolate is left at the top of the tube for use. There were no study outcomes obtained from the centrifuge, as its purpose was to prepare the sample for storage.
Hemoglobin/Hematocrit Analyzer. Prior to spinning the blood samples, Hemoglobin and
hematocrit were measured using a HemoPoint H2 hemoglobin analyzer (Boerne, TX) using whole blood. This analyzer uses the photometric azide methemoglobin method to reliably measure the amount hemoglobin protein in the blood plasma. Hemoglobin amount and hematocrit were derived from this analysis to control for plasma volume shift.
UCH-L1 Analysis. All blood samples were shipped to Banyan Biomarkers, Inc. (San
Diego, CA). The blood was shipped priority overnight, and was completely covered in dry ice for the shipping process. Banyan thawed the serum samples, and then performed a sandwich ELISA. Blood specimens were applied to a 96-well plate that had been pre-coated with an antibody specific to UCH-L1. The plate was then washed to remove any unbound material. Banyan then added a second antibody that was specific to UCH-L1 to aid with detection (creating the “sandwich”) before repeating the wash step. A substrate that reacts with an enzyme attached to the detection antibody was then added to the plate, producing a chemiluminescent signal that could be measured electronically and is proportional to the
Procedure
Participants were introduced to the equipment and procedures during an orientation session to limit any potential learning or familiarization effects. Participants then returned for two, identical clinical testing sessions. Healthy participants enrolled into the study at an arbitrary start date and completed with two clinical testing sessions within 10-14 days of each other. Concussed participants were enrolled into the study within 3-10 days of their injury. Concussed participants completed the first clinical testing sessions as close to three days following injury as possible and the second clinical testing sessions following 24 consecutive hours without
concussive symptoms.
Orientation Session
Prior to testing sessions, participants completed an orientation session to ensure sufficient cardiovascular health to successfully complete the maximal exercise testing, as well as to orient them to the equipment and the timing and intensity of the maximal exercise testing protocol. All participants completed the Physical Activity Readiness Questionnaire (PAR-Q), self-reported a general medical history, and underwent a 10-lead EKG, all of which were read by an independent medical monitor. The independent medical monitor provided medical
clearance for each participant to verify that the participants’ cardiovascular health was sufficient to perform maximum exercise testing without any serious health risks. Any participants not receiving medical clearance (n=4) were excluded from study participation. Participants were then introduced to and fitted for the facemask equipment associated with the metabolic cart and cycle ergometer. Ensuring proper fit to the equipment was necessary to ensure minimal
protocols. Healthy participants were given an abbreviated version of the maximal exercise test to familiarize them with the exercise protocol. Healthy participants were allowed to pedal for five minutes at a comfortable pace with no resistance, and then completed the first two stages of the maximal exercise test. Concussed participants were not given the abbreviated version maximal exercise test due to safety reasons, but were fitted for all equipment. Lastly, the timing, volume, and number of blood draws completed during each testing session was explained to the
participants, who were then given a chance to ask any questions.
Clinical Testing Session 1 and 2
Following the orientation session and medical clearance from the independent medical monitor, participants were scheduled for the first of two, identical clinical testing sessions. Upon arriving for a clinical testing session, participants completed a blood draw in which one 10ml EDTA and one 10ml SST tube were drawn using standard phlebotomy procedures. Following the first blood draw, participants were outfitted with a heart rate monitor (Polar, Kempele, Finland), then asked to sit quietly and rest for five minutes. Participant’s vital signs (heart rate and blood pressure) were taken following this rest period.
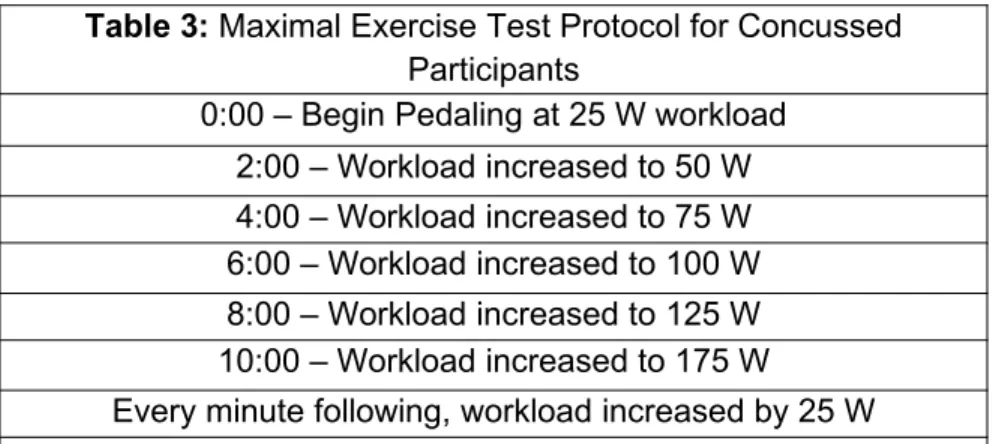
Table 3: Maximal Exercise Test Protocol for Concussed Participants
0:00 – Begin Pedaling at 25 W workload 2:00 – Workload increased to 50 W 4:00 – Workload increased to 75 W 6:00 – Workload increased to 100 W 8:00 – Workload increased to 125 W 10:00 – Workload increased to 175 W
Termination – Volitional fatigue or exacerbation of concussion symptoms
After obtaining vital signs, the participant completed the maximal exercise test. The maximal exercise testing protocol was identical for all participants within each injury classification included in this study. However, the protocol for healthy and concussed participants was different.
The separate healthy and concussed maximal exercise testing protocols are detailed in Tables 2 and 3. Every two minutes, heart rate and rate of perceived exertion (RPE) were collected. To obtain RPE outcomes, participants were asked to point to the Borg Perceived Exertion Scale (6= basal activity to 20= maximal activity) to communicate their level of effort. For healthy participants, the maximal exercise test continued until the patient reached a maximal level of exertion and could not continue (volitional fatigue). For concussed participants, individuals were instructed to end the test immediately if they obtained any new or worsening concussive
symptoms. If no new or worsening symptoms appeared, concussed participants cycled until they reached volitional fatigue. All maximal exercise sessions were evaluated following
completion to ensure the criteria for maximum exertion was met. In order for a maximal exercise test to be considered valid, at least three of the following criteria were met: a) plateau in
maximal volume of oxygen (VO2) values, b) respiratory exchange ratio (RER) ≥ 1.10, c) RPE ≥ 17, d) lactate ≥ 6.0mmol/L, and e) within 90% of age predicted heart rate max. At the termination of the maximal exercise test, all participants were assisted from the cycle ergometer
Table 2: Maximal Exercise Test Protocol for Healthy
Participants0:00 – Begin Pedaling at 50 W workload 2:00 – Workload increased to 100 W 4:00 – Workload increased to 150 W 6:00 – Workload increased to 180 W 8:00 – Workload increased to 210 W 10:00 – Workload increased to 240 W
and taken to a chair for passive recovery. The participant then completed a second, identical blood draw as close to five minutes following the test as possible, to allow time for potential biomarkers of interest to filter into the bloodstream.
Prior to session termination, the participant’s vital signs were reevaluated to ensure that no adverse health events were occurring. Once vital sign values had returned to baseline (pre-exercise) values, participants were allowed to leave the session. A protocol was established for providing medical treatment if participants’ vital signs did not return within a 30-minute window; however, this did not occur for any participants.
Blood Sample Processing
The blood processing associated with each blood draw from the study took place concurrent to the clinical testing sessions. In each blood draw, one 10ml EDTA (plasma) tube and one 10ml SST (serum) tube were collected. For plasma samples, the EDTA tube was spun within 30 minutes of the draw. If the plasma could not be spun within 30 minutes of the draw, the sample was placed on ice until processing could begin. For serum sample, the sample was allowed to sit for 30 minutes to ensure clotting occurred. SST tubes were spun between 30-60 minutes of the draw. For all samples, the centrifuge was set at a level of 3000rpm for 15 minutes at 4ºC. Following the centrifuge process, ~1ml aliquots of both plasma and serum isolates were stored at -80ºC until analysis.
Power Analysis
found UCH-L1 serum levels are on average 0.12ng/ml+/- 0.02ng/ml for healthy (uninjured) controls.63 Using the following parameters (alpha= 0.05, power= 0.80, N= 30, and standard deviation= 0.02), this study is adequately powered to find a change of +/- 0.010ng/L in serum UCH-L1 levels, equal to a 9% change. Other studies looking at the effect of sub-concussive impacts on UCH-L1 found a 26% change in serum UCH-L1 levels following an organized football game.62 Additionally, another study found that UCH-L1 serum levels ranged between 0.015-19.25 ng/ml in a sample of individuals on the traumatic brain injury spectrum, with a mean level of around 2.00 ng/ml for severe TBI and a mean level of 0.60 ng/ml for mild forms of TBI.15 Given these findings, we are confident in our ability to detect any clinically meaningful changes in UCH-LI levels given our study parameters.
Data Reduction
Blood isolate samples obtained from all blood draws (before and after the maximal exercise test in clinical session one and before the maximal exercise test in clinical session two) were run in triplicate. For analysis of UCH-L1 levels, a mean score was created from these three samples. The mean score was calculated between the triplicate samples to average any potential differences in UCH-L1 levels between samples as well as to reduce potential
processing errors.
Data Analysis
levels of UCH-L1 was defined as the change in UCH-L1 directly after the maximal exercise test as compared to UCH-L1 levels prior to exercise.
Research Question 1
The test-retest reliability of UCH-L1 levels in non-injured (no SRC) athletes, both male and female, were calculated using a ICC2, k. An 80% RCI was also calculated and used in conjunction with the ICC value to further investigate the clinical utility of the UCH-L1 levels.
Research Question 2
The influence of acute exercise on UCH-L1 levels in healthy, recreational athletes was measured using a 2 (sex) by 2 (time) mixed-model ANOVA to determine any differences in UCH-L1 levels by sex, acute exercise, or interactions between sex and acute exercise. Exploratory Aim 1 and 2
A descriptive analysis was performed for the concussed participant due to the lack of size of the sample. The test-retest reliability and influence of acute exercise were examined in the one participant tested.
Notes
Hematocrit and hemoglobin values were assessed throughout this study to control for potential effects of plasma value shifts. Due to instrumentation limitations/malfunctions and changes to study protocol, only a subset of the sample completed these measures. In relation to the maximal exercise tests, two subjects of the 30 did not reach maximum exertion as
CHAPTER IV
Results
Participants
A total of thirty subjects participated in this study. Demographic information for these participants are presented in
Table 4. Blood samples were obtained at prior to the maximal exercise test both clinical testing sessions in 27 of 30 participants and these samples were used for the reliability analysis (RQ 1).
Both pre- and post-exercise blood draws were successfully completed for all 30 participants, resulting in their inclusion in the examination on the effect of acute exercise on UCH-L1 (RQ2).
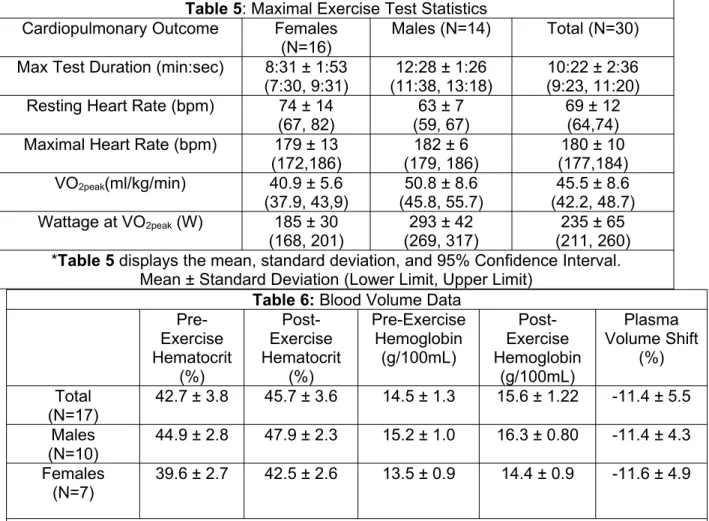
Maximal Exercise Test
Heart rate at the beginning and end of maximal exercise test, maximal exercise test duration, VO2peak, and wattage at maximal exertion were all recorded for each maximal exercise test (Table 5). In general, males had higher VO2peak (t=3.77, p=0.03), higher maximal heart rate (t=0.88, p=0.01), and lower resting heart rates (t=2.72, p=0.05) but there was not a significant difference between male and female max test length (t=6.38, p=0.47) and wattage achieved at max (t=8.27, p=0.37). Hematocrit and hemoglobin levels were measured in plasma from the
Table 4: Participant Demographics Total
(N=30)
Males (N=14)
Females (N=16) Age (years)
21 ± 2.3 21 ± 1.2 21 ± 3.0 Height (cm)
173.8 ± 10.7 182.0 ± 7.9 166.6 ± 6.8 Weight (kg) 70.9 ± 12.0 79.2 ± 9.9 63.8 ± 8.6
Body Mass
pre- and post-exercise samples to account for shifts in plasma volume (Table 6). However, due to limitations in equipment, hematocrit and hemoglobin were not measured for every blood sample taken.
Table 6: Blood Volume Data
Pre-Exercise Hematocrit (%) Post-Exercise Hematocrit (%) Pre-Exercise Hemoglobin (g/100mL) Post-Exercise Hemoglobin (g/100mL) Plasma Volume Shift (%) Total (N=17)
42.7 ± 3.8 45.7 ± 3.6 14.5 ± 1.3 15.6 ± 1.22 -11.4 ± 5.5 Males
(N=10)
44.9 ± 2.8 47.9 ± 2.3 15.2 ± 1.0 16.3 ± 0.80 -11.4 ± 4.3 Females
(N=7)
39.6 ± 2.7 42.5 ± 2.6 13.5 ± 0.9 14.4 ± 0.9 -11.6 ± 4.9
Due to instrumentation limitations, hemoglobin and hematocrit were only obtained in 17 of the 30 subjects used to analyze the effect of acute exercise on UCH-L1.
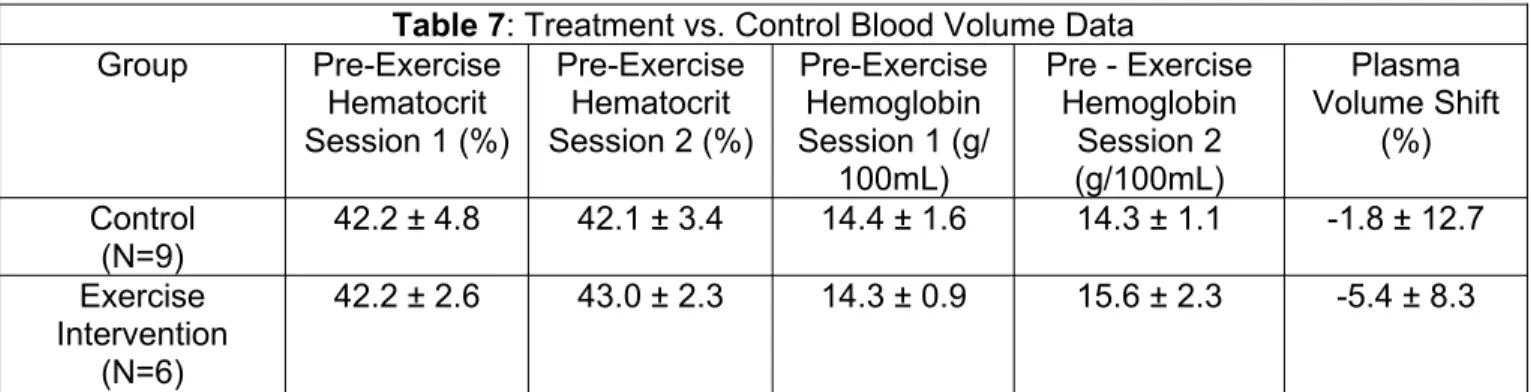
It was also found that there were no differences in shifts in plasma volume between subjects who underwent the exercise intervention and the control subjects who did not (Table 7).
Table 5: Maximal Exercise Test Statistics Cardiopulmonary Outcome Females
(N=16)
Males (N=14) Total (N=30) Max Test Duration (min:sec) 8:31 ± 1:53
(7:30, 9:31)
12:28 ± 1:26 (11:38, 13:18)
10:22 ± 2:36 (9:23, 11:20) Resting Heart Rate (bpm) 74 ± 14
(67, 82)
63 ± 7 (59, 67)
69 ± 12 (64,74) Maximal Heart Rate (bpm) 179 ± 13
(172,186) (179, 186)182 ± 6 (177,184)180 ± 10 VO2peak(ml/kg/min) 40.9 ± 5.6
(37.9, 43,9)
50.8 ± 8.6 (45.8, 55.7)
45.5 ± 8.6 (42.2, 48.7) Wattage at VO2peak (W) 185 ± 30
(168, 201)
293 ± 42 (269, 317)
235 ± 65 (211, 260) *Table 5 displays the mean, standard deviation, and 95% Confidence Interval.
Table 7: Treatment vs. Control Blood Volume Data
Group Pre-Exercise
Hematocrit Session 1 (%)
Pre-Exercise Hematocrit Session 2 (%)
Pre-Exercise Hemoglobin Session 1 (g/
100mL)
Pre - Exercise Hemoglobin Session 2 (g/100mL) Plasma Volume Shift (%) Control (N=9)
42.2 ± 4.8 42.1 ± 3.4 14.4 ± 1.6 14.3 ± 1.1 -1.8 ± 12.7 Exercise
Intervention (N=6)
42.2 ± 2.6 43.0 ± 2.3 14.3 ± 0.9 15.6 ± 2.3 -5.4 ± 8.3
Due to instrumentation limitations and researcher error, blood volume data at both sessions was only obtained on 15 subjects.
Research Question 1: UCH-L1 Reliability
After blood analysis, the reliability of UCH-L1 was examined through an ICC2,k (Table 8). UCH-L1 levels were moderately reliable across the entire cohort (ICC2,k=0.505). However, when split into sex, UCH-L1 levels had excellent reliability in males (ICC2,k=0.895), while poor
reliability was found in females (ICC2,k=0.094). An 80% RCI was also
calculated to determine the variability of the biomarker as well; the mean value of
the biomarker was similar between sexes, but the RCI range was almost 3 times greater in females than it was in males (80% RCIfemales=138.8, 80% RCImales=44.4).
Research Question 2: Effect of Acute Exercise
Table 8: UCH-L1 Reliability
Outcome Males N=14 Females N=13 Total N=27 UCH-L1 (ICC2,k)
0.895 0.094 0.505
Mean Value (pg/ml)
113.4 112.9 113.1
80% RCI (pg/ml)
44.4 138.8 107.0
A 2 (sex) by 2 (time) mixed-model ANOVA was used to examine the effect of acute exercise and sex on healthy, recreational athletes, with the results displayed in Table 9. This analysis was completed for all subjects (N=30, 14 males, 16 females. There were no significant main effects of exercise (F=0.05, p=0.95, df=2) or sex (F=0.14, p=0.713, df=1) on UCH-L1 levels. Additionally, no significant interaction effects were observed (F=3.09, p=0.054). As the sex by time interaction term neared statistical significance, a post-hoc analysis was completed to further investigate these findings. No individual comparisons neared significance, suggesting no clinically or statistically meaningful relationships were found between sex and exercise on UCH-L1 levels.
Table 9: Effect of Acute Exercise on UCH-L1 By Sex
Outcome Males Females P value
Pre-exercise
Post-exercise
Pre-exercise
Post-exercise
Sex Exercise Sex* exercise UCH-L1
N=30
131.4 ± 71.2 (90.2,172.5)
141.5 ± 76.3 (97.5,185.5)
117.9 ± 62.3 (84.7,151.1)
100.8 ± 53.4 (71.3,130.3)
CHAPTER V
Discussion
After examining the reliability and effect of acute exercise on UCH-L1 in healthy, recreationally active college students, we found two important findings. Our most important finding pertained to the reliability of the biomarker. While baseline UCH-L1 values were similar between males and females, they were much less reliable over a two-week period in the females. We found that measures for males showed high reliability over this same period of time. Our second important finding was that UCH-L1 values remained constant in individuals despite acute exercise; pre-and post-exercise levels of UCH-L1 did not change significantly in both males and females. Our findings supported the hypothesis that exercise would not significantly change UCH-L1 levels, but our reliability findings were only partially supported.
The evidence that the biomarker is highly reliable in males supports our original research hypothesis. The majority of UCH-L1 in the human body is found in neurons and neuroendocrine cells; shearing forces associated head trauma imparted upon neurons are thought to dislodge this protein, causing it to increase in the bloodstream.58,59 Thus, increases in UCH-L1 are thought to be associated with head injury.9,56-61,63 However, without trauma, shearing, or some mechanism of dislodging these proteins from the neural tissue, UCH-L1 should stay localized in the neurons and the levels in the bloodstream should remain fairly constant.12,59 No subjects self-reported any blows to the head or potential head trauma over the course of their
Reliability findings for females did not support our original research hypothesis. UCH-L1 was found have poor reliability, with high variability between testing sessions in females.
Considering the similarities in male and female neural anatomy, it was thought that male and females should have similar UCH-L1 responses under resting conditions over time. This
variability matches previous research that has found baseline levels of UCH-L1 to be variable in the population.13 While it is unclear why UCH-L1 variability was much greater in females, we postulated several hypotheses that could explain this phenomenon. Females have fluctuating levels of estrogen and progesterone throughout the menstrual cycle, which may affect UCH-L1 levels. Previous research has shown that these hormones can affect female expression of specific proteins such as C-reactive protein α1acid glycoprotein, which are blood biomarkers for tissue necrosis and inflammation.64 Perhaps the menstrual cycle, through some unknown mechanism, affects UCH-L1 and causes it to fluctuate in females. Another possibility is that UCH-L1 levels could be influenced by outside medications. Previous research has shown that some medications can affect the transport of proteins within the body or on the integrity of the blood-brain barrier.65,66 While we are unaware of any medications that may influence UCH-L1 levels, it is possible that birth control pills or other forms of contraception used to regulate the menstrual cycle could have an effect on the blood-brain barrier or even UCH-L1 itself. This could lead to the variable levels of the biomarker that were found in the study. However, this was not directly assessed in this study and further research is needed to determine why UCH-L1 is not reliable only in female participants.
original research hypothesis. During exercise, the majority of work is done by skeletal muscle, and thus exercise has been found to affect the levels of biomarkers in the body, especially some of those related to head trauma such as S100B.67 However, due to the localization of UCH-L1 primarily in neurons and neuroendocrine tissue, trauma and shearing forces would be needed do dislodge this biomarker to cause it to elevate in the body; this is a mechanism not elicited by stationary cycling. The non-significant increase of UCH-L1 levels in males post-exercise is explained by the shift in plasma volume, which is defined as the amount water lost from the blood plasma during exercise either as sweat or muscle edema as temporary hypertrophy.68,69 Male plasma volume decreased by a similar percentage that UCH-L1 increased in the blood, suggesting that the decrease in fluid volume of the plasma resulted in a similar measured increase in concentration of UCH-L1. UCH-L1 levels in females, however, changed in the opposite direction – there was a slight (though not statistically significant) decrease after
exercise. This could be due to the fact that UCH-L1 seems to be much more variable in females than males (as evidenced by the 80% RCI); however, a more comprehensive understanding of UCH-L1 in females is needed to be certain of why UCH-L1 levels decreased slightly after exercise in females.
Previous research has examined the change in UCH-L1 in rats after exercise and in humans after football games, finding that UCH-L1 changed in both cases
not affected by exercise allows those using the biomarker information in a clinical setting, such as physicians or clinicians, to be more confident that changes in levels of the biomarker are due to injury and not other factors.
Clinical Significance
Baseline levels of UCH-L1 have had yet to be established in the scientific literature. Our findings suggest that these are close to 113 pg/mL. With a baseline level established, there could be potential for clinicians to use the biomarker as a way to track stages of recovery from concussive injury and seeing when UCH-L1 returned to baseline levels after injury. There is also potential for the biomarker to be used in relation to examining the severity of concussive injury; as changes of biomarker levels from baseline after injury could provide important information about the extent of the concussive injury. However, further research would be needed to validate these relationships and usages.
Our finding that UCH-L1 levels do not change due to acute exercise also has clinical significance. People who sustain a SRC will almost always be exercising; the findings from our study suggest that exercise will not affect the levels of L1. Therefore, an increase in UCH-L1 levels that exceed reliable change can most likely be attributed to injury and not a byproduct of physical activity. This could indicate that UCH-L1 is a viable tool in helping to diagnose concussion and tracking recovery. If a sensitive biomarker is established, there is potential for future innovation to create analyses using blood obtained from methods such as finger pricks. This could aid in the evaluation of injury on the sideline or in the locker room during or
immediately following sport.
Limitations
minutes after the end of the maximal exercise test; however, some females were drawn as late as 15 minutes post-exercise due to the inherent difficulty in blood draws associated with female vasculature. This could have possibly led to some of the variation we saw in UCH-L1 levels in females. Participants were also chosen based upon a convenience sample, and thus may not have been representative of the general, healthy, recreationally active college aged population. Finally, participants were asked to self-report any impacts to the head and activity levels during the study. No major head impacts were disclosed by participants, but minor head impacts through recreational activity may not have been reported by participants and could affect UCH-L1 levels.
The findings from this study have illuminated some important questions that can be answered through further research. Specifically, the next steps to make the results of this project more meaningful should focus on two specific areas. First, the sex difference in UCH-L1 should be investigated. Future studies could enroll recreationally active, college aged females and take several samples over the course of a menstrual cycle, and investigate if levels of estrogen or progesterone are related to UCH-L1 levels. Studies could also enroll females who took different types and dosages of birth control, and investigate if different medications or amounts of medication were related to UCH-L1 levels. Second, UCH-L1 levels should be studied in injured (concussed) populations. Studies examining the relationship between concussed individuals and UCH-L1 levels would help determine if this biomarker could eventually be utilized as part of the battery of concussion assessments.
REFERENCES
1. Hirtz D, Thurman DJ, Gwinn-Hardy K, Mohamed M, Chaudhuri AR, Zalutsky R. How common are the “common” neurologic disorders? Neurology. 2007;68(5):326-337. 2. McGuine TA, Hetzel S, McCrea M, Brooks MA. Protective equipment and player
characteristics associated with the incidence of sport-related concussion in high school football players: a multifactorial prospective study. Am J Sports Med. 2014;42(10):2470-2478. doi:10.1177/0363546514541926.
3. Langlois JA, Rutland-Brown W, Wald MM. The epidemiology and impact of traumatic brain injury: a brief overview. J Head Trauma Rehabil. 2006;21(5):375-378.
4. McCrea M, Hammeke T, Olsen G, Leo P, Guskiewicz K. Unreported concussion in high school football players: implications for prevention. Clin J Sport Med. 2004;14(1):13-17. 5. McCrory P, Meeuwisse W, Aubry M, et al. Consensus statement on Concussion in Sport—
The 4th International Conference on Concussion in Sport held in Zurich, November 2012. J Sci Med Sport. 2013;16(3):178-189. doi:10.1016/j.jsams.2013.02.009.
6. Beckwith JG, Greenwald RM, Chu JJ, et al. Timing of Concussion Diagnosis Is Related to Head Impact Exposure Prior to Injury: Med Sci Sports Exerc. 2013;45(4):747-754.
doi:10.1249/MSS.0b013e3182793067.
7. Register-Mihalik JK, Guskiewicz KM, Mihalik JP, Schmidt JD, Kerr ZY, McCrea MA. Reliable Change, Sensitivity, and Specificity of a Multidimensional Concussion
Assessment Battery: Implications for Caution in Clinical Practice. J Head Trauma Rehabil. 2013;28(4):274-283. doi:10.1097/HTR.0b013e3182585d37.
8. Broglio SP, Macciocchi SN, Ferrara MS. SENSITIVITY OF THE CONCUSSION ASSESSMENT BATTERY: Neurosurgery. 2007;60(6):1050???1058.
doi:10.1227/01.NEU.0000255479.90999.C0.
9. Mondello S, Wang KK. Blood-based diagnostics of traumatic brain injuries. Expert Rev Mol Diagn. 2011;11(1):65-78. doi:http://dx.doi.org/10.1586/erm.10.104.
10. Brown AFT, Cullen L, Than M. Future Developments in Chest Pain Diagnosis and Management. Med Clin North Am. 2010;94(2):375-400. doi:10.1016/j.mcna.2010.01.010. 11. Petersen RC, Smith GE, Ivnik RJ, others. Second impact syndrome. NEUROLOGY.
1998;50:677-683.
13. Papa L, Akinyi L, Liu MC, et al. Ubiquitin C-terminal hydrolase is a novel biomarker in humans for severe traumatic brain injury. Crit Care Med. 2010;38(1):138-144. doi:10.1097/ CCM.0b013e3181b788ab.
14. Blyth BJ, Farahvar A, He H, et al. Elevated Serum Ubiquitin Carboxy-Terminal Hydrolase L1 Is Associated with Abnormal Blood–Brain Barrier Function after Traumatic Brain Injury. J Neurotrauma. 2011;28(12):2453-2462. doi:10.1089/neu.2010.1653.
15. Papa L, Lewis LM, Silvestri S, et al. Serum levels of ubiquitin C-terminal hydrolase distinguish mild traumatic brain injury from trauma controls and are elevated in mild and moderate traumatic brain injury patients with intracranial lesions and neurosurgical intervention: J Trauma Inj Infect Crit Care. 2012;72(5):1335-1344.
doi:10.1097/TA.0b013e3182491e3d.
16. Edward S. Bennett, Barry A. Weissman. Clinical Contact Lens Practice. Lippincott Williams & Wilkins; 2005.
17. Wilson PO, Barber PC, Hamid QA, et al. The immunolocalization of protein gene product 9.5 using rabbit polyclonal and mouse monoclonal antibodies. Br J Exp Pathol.
1988;69(1):91-104.
18. Gong B, Leznik E. The role of ubiquitin C-terminal hydrolase L1 in neurodegenerative disorders. Drug News Perspect. 2007;20(6):365-370. doi:10.1358/dnp.2007.20.6.1138160. 19. Brophy GM, Mondello S, Papa L, et al. Biokinetic Analysis of Ubiquitin C-Terminal
Hydrolase-L1 (UCH-L1) in Severe Traumatic Brain Injury Patient Biofluids. J Neurotrauma. 2011;28(6):861-870. doi:10.1089/neu.2010.1564.
20. Johnston KM, McCrory P, Mohtadi NG, Meeuwisse W. Evidence-based review of sport-related concussion: clinical science. Clin J Sport Med. 2001;11(3):150-159.
21. Lincoln AE, Caswell SV, Almquist JL, Dunn RE, Norris JB, Hinton RY. Trends in
Concussion Incidence in High School Sports A Prospective 11-Year Study. Am J Sports Med. 2011;39(5):958-963. doi:10.1177/0363546510392326.
22. Zuckerman SL, Kerr ZY, Yengo-Kahn A, Wasserman E, Covassin T, Solomon GS. Epidemiology of Sports-Related Concussion in NCAA Athletes From 2009-2010 to 2013-2014: Incidence, Recurrence, and Mechanisms. Am J Sports Med. 2015;43(11):2654-2662. doi:10.1177/0363546515599634.
23. Covassin T, Swanik CB, Sachs ML. Sex Differences and the Incidence of Concussions Among Collegiate Athletes. J Athl Train. 2003;38(3):238-244.
25. Barnes BC, Cooper L, Kirkendall DT, McDermott TP, Jordan BD, Garrett WE. Concussion history in elite male and female soccer players. Am J Sports Med. 1998;26(3):433-438. 26. MacFarlane MP, Glenn TC. Neurochemical cascade of concussion. Brain Inj.
2015;29(2):139-153. doi:10.3109/02699052.2014.965208.
27. Hunt T, Asplund C. Concussion Assessment and Management. Clin Sports Med. 2010;29(1):5-17. doi:10.1016/j.csm.2009.09.002.
28. Mansell JL, Tierney RT, Higgins M, McDevitt J, Toone N, Glutting J. Concussive signs and symptoms following head impacts in collegiate athletes. Brain Inj. 2010;24(9):1070-1074. doi:10.3109/02699052.2010.494589.
29. Guskiewicz KM, Ross SE, Marshall SW. Postural Stability and Neuropsychological Deficits After Concussion in Collegiate Athletes. J Athl Train. 2001;36(3):263-273.
30. McCrea M, Guskiewicz KM, Marshall SW, et al. Acute effects and recovery time following concussion in collegiate football players: the NCAA Concussion Study. JAMA.
2003;290(19):2556-2563. doi:10.1001/jama.290.19.2556.
31. Makdissi M, Cantu RC, Johnston KM, McCrory P, Meeuwisse WH. The difficult concussion patient: what is the best approach to investigation and management of persistent (>10 days) postconcussive symptoms? Br J Sports Med. 2013;47(5):308-313.
doi:10.1136/bjsports-2013-092255.
32. Macciocchi SN, Barth JT, Littlefield LM. Outcome after mild head injury. Clin Sports Med. 1998;17(1):27-36.
33. McCrory P, Meeuwisse W, Johnston K, et al. Consensus statement on Concussion in Sport 3rd International Conference on Concussion in Sport held in Zurich, November 2008. Clin J Sport Med Off J Can Acad Sport Med. 2009;19(3):185-200.
doi:10.1097/JSM.0b013e3181a501db.
34. Kontos AP, Sufrinko A, Womble M, Kegel N. Neuropsychological Assessment Following Concussion: an Evidence-Based Review of the Role of Neuropsychological Assessment Pre- and Post-Concussion. Curr Pain Headache Rep. 2016;20(6):38. doi:10.1007/s11916-016-0571-y.
35. McCrea M, Kelly JP, Randolph C, et al. Standardized assessment of concussion (SAC): on-site mental status evaluation of the athlete. J Head Trauma Rehabil. 1998;13(2):27-35. 36. Broglio SP, Ferrara MS, Macciocchi SN, Baumgartner TA, Elliott R. Test-retest reliability of