Aleksandra Iljin, Julia Kruk-Jeromin
Aplasia Cutis Congenita
Agenezja skóry owłosionej głowy
Department of Plastic, Reconstructive and Aesthetic Surgery, Medical University of Lodz, Poland
Abstract
Background. Aplasia cutis congenita (ACC) is a congenital malformation mostly of the scalp. Although the etiol-ogy of ACC is unknown, external and genetic factors are considered. Apart from preservative management, surgery is a recommended for aesthetic and life-saving indications.
Objectives. Twenty-seven cases of ACC were analyzed with regard to pathology and therapy.
Material and Methods. The study group consisted of 27 patients with ACC aged 2–17 years treated at the Department of Plastic, Reconstructive and Aesthetic Surgery, Medical University of Lodz, in 1981–2007. Morphology of the lesions, coexistence of other congenital malformations, and the etiopathogenesis of the ACC were analyzed. Different techniques of local plasty were used in the reconstruction after resection.
Results. In this group the involvement of etiopathogenetic factors was not confirmed. One patient had other con-genital malformations. The aesthetic effects of the surgery were very good. The histopathological pictures of the resected lesions corresponded with the scars.
Conclusions.Aplasia cutis congenita rarely coexists with defects of deeper layers of the skull covering and other distant congenital anomalies. It is seldom possible to establish the etiopathogenesis of ACC. ACC in the form of a scar of the scalp can be managed surgically for aesthetic indications. The choice of reconstruction technique depends on the size and localization of the lesion (Adv Clin Exp Med 2010, 19, 1, 121–125).
Key words: aplasia cutis congenita of the scalp.
Streszczenie
Wprowadzenie. Wrodzony ubytek skóry (ACC) jest wadą rozwojową dotyczącą najczęściej skóry owłosionej głowy. Etiologia ACC nie jest wyjaśniona, podejrzewa się czynniki zewnętrzne i dziedziczne. Oprócz leczenia zachowawczego, zaleca się interwencję chirurgiczną ze wskazań estetycznych lub życiowych.
Cel pracy. Analiza 27 przypadków wrodzonego ubytku skóry owłosionej głowy pod względem patomorfolo-gii i terapii.
Materiał i metody. W pracy przedstawiono 27 pacjentów z ACC głowy w wieku 2–17 lat leczonych w Klinice Chirurgii Plastycznej, Rekonstrukcyjnej i Estetycznej UM w Łodzi w latach 1981–2007. W badanej grupie chorych analizie pod-dano: cechy morfologiczne zmian, a także współistnienie innych wad rozwojowych oraz etiopatogenetyczne uwarun-kowanie ACC. Do rekonstrukcji tkanek po wycięciu zmiany wykorzystano różne techniki plastyki miejscowej. Wyniki. W badanej grupie chorych nie udało się potwierdzić udziału czynników etiopatogenetycznych. Tylko u jed-nej pacjentki obserwowano także inne anomalie wrodzone. Estetyczne wyniki leczenia chirurgicznego były bardzo dobre. Histopatologiczna ocena wyciętych zmian skórnych odpowiadała bliźnie.
Wnioski. Wrodzony ubytek skóry owłosionej głowy rzadko współistnieje z ubytkiem głębokich warstw pokrywy czaszki oraz innymi odległymi zaburzeniami rozwojowymi. Izolowany ACC rzadko daje możliwość określenia podłoża etiopatogenetycznego. ACC w postaci blizny skóry owłosionej głowy może być leczony chirurgicznie ze wskazań estetycznych. Wybór metody rekonstrukcyjnej skóry owłosionej głowy zależy od wielkości i umiejscowie-nia ubytku (Adv Clin Exp Med 2010, 19, 1, 121–125).
Słowa kluczowe: wrodzony ubytek skóry owłosionej głowy.
Adv Clin Exp Med 2010, 19, 1, 121–125 ISSN 1230-025X
ORIgINAL PAPERS
© Copyright by Wroclaw Medical University
Aplasia cutis congenita (ACC) is a congenital malformation of the scalp occurring in 1 in every 10,000 of births [1]. In the majority of cases (75%)
presence of ACC on the trunk or limbs, usually with a symmetrical distribution, is found in 25% of the patients. In 10% of cases, lesions are pres-ent at all three sites [1]. The classifications of ACC confirm the nosological heterogeneity of the mal-formation, from an isolated defect to lesion com-bined with other congenital disorders. ACC may also accompany some genetic syndromes [3–5].
Despite the knowledge of the morphology of the defect since its first description by Cordon, Friedel, and Campbell, none of the hypotheses unequivocally explains its pathogenesis [1–3]. The influence of exogenous (biological, pharma-cological, and mechanical) together with endog-enous (genetic, teratogens) is considered. The involvement of a hereditary factor characterized by autosomal dominant transmission has been confirmed in some cases of ACC [1, 6]. The his-topathological picture of the lesion corresponds with the cicatrix [2].
The treatment of ACC depends mostly on the progression of the defect. Therapeutic manage-ment in patients with lesions limited to the skin includes preventive treatment (controlled healing of the ulceration) and surgery using different tech-niques of local plasty (for aesthetic indications). In defects of bones and dura mater, skin grafts, local scalp flaps, composite grafts, and free flaps are used [3, 7–12]. Early surgical management in these cases allows avoiding complications such as meningitis or hemorrhage from the sagittal sinus and maintaining proper thermoregulation and liq-uid balance in children [1–3, 5, 13–15].
Material and Methods
Twenty-seven patients with ACC (14 females and 13 males) aged 2–17 years were treated at the Department of Plastic, Reconstructive and Aesthetic Surgery of the Medical University of Lodz between 1981 and 2007. Lesions with diam-eters between 4–25 cm2 were found only within
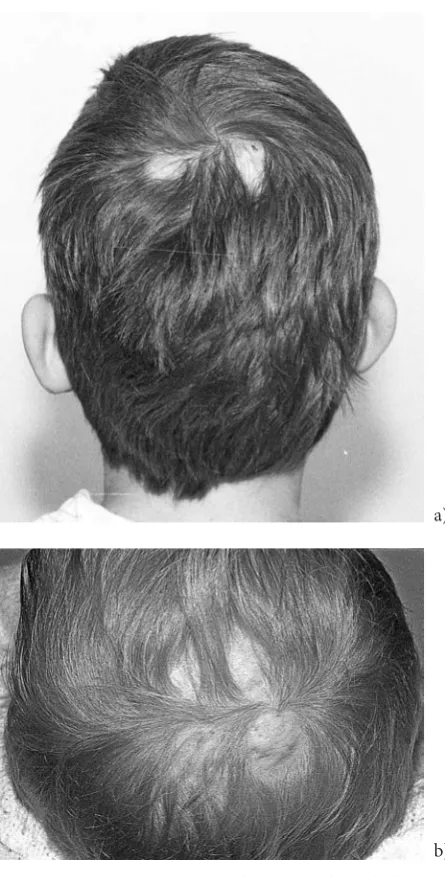
the scalp. The defects were observed on the ver-tex of the skull in 19 subjects, in the temporal area in 2, and in the parietal area in 6. In 25 patients the defects were isolated; 15 cases were round and 10 were oval. Multiple defects/variform scars or 4 round islet-likelesions occurred in only 2 sub-jects (Figs 1a, b).
In 7 children, surgery followed preservative management of the ulceration in the neonatal peri-od. Nineteen patients were subjected to one-stage and 8 to two-stage resection of the lesion. Wound edges of the resultant defects were sutured or closed using rotation, or advancement, or two and three-flap techniques as well. One girl was
afflict-ed with pilar anomaly of the entire head (hair-less patch within the scalp), triangular hair growth in the midline of the forehead, tumor of the forehead, hypertelorism, epicanthic folds, short and wide upper lip frenulum, diastema, narrow and high palate with bony ridge in the midline, congenital heart disease, and anomaly of the auricle. In this case the frontal tumor (lipoma) was resected.
Results
In all patients a history of exposure to patho-genic agents during fetal development and the presence of genetic determinants were excluded. genetic examination did not reveal any
chromo-Fig. 1. Multiple ACC types on the vertex of the skull: double (a), quadruple (b)
Ryc. 1. Mnogie postacie wrodzonego ubytku skóry owłosionej szczytu głowy: podwójny (a), poczwórny (b)
a)
somal aberrations in this group. ACC located at different sites than the scalp was not observed. Accompanying malformations of the face, oral cavity, and heart were confirmed in one female. In all the cases the surgeries were performed for aesthetical indications (Figs 2a, b). The early post-operative course was normal in all the patients. Distant aesthetic results of the surgical treatment were regarded as very good.
Histopathological assessment of the resected lesions showed characteristics of the cicatrix: thin-ning of the epidermis, proliferation of the fibrous tissue in the skin, increase in the number of the collagen fibers in the subcutaneous layer, and the presence of single hair follicles in 15 specimens or lack of follicles in the rest of the cases.
Discussion
Congenital isolated defects of superficial lay-ers or full-thickness scalp are the most common cases of ACC. All the patients of the present study belonged to this group. Lesions of this type are usu-ally separate and located on the vertex of the head or in the median line of the head. The shape of the ulceration or the scar is mostly round or oval [1–3]. The lesions have sizes ranging from a few cm2 to
one third of the scalp surface [9]. The present observations confirm these data. Defects extend-ing to deeper structures such as bones, menextend-inges, or even brain are a separate topic [9, 15]. Those are referred to neurosurgery and thus are not cap-tured in these data. Some defects of the hairy skin of the limbs, trunk, face, or neck were described in the literature in patients included in groups 5, 6, 7, and 9 according to the I. Frieden classification [4, 16]. The authors did not observe such cases.
ACC may coexist with other congenital mal-formations or malformation syndromes such as cleft palate, umbilical hernia, defects of the heart, eyes, alimentary tract (pyloric stenosis), and ner-vous system (distematomyelia), skin diseases (epidermolysis bullosum, cutis marmoratta), dys-raphia, and chromosomal syndromes (e.g. Down’s syndrome, 4p) [1–3, 5, 7, 9–12]. Local defect of the skin and bones may be a symptom of Adams-Oliver syndrome, in which it accompanies defects of distal limb segments or trisomy 13. In a pediat-ric cohort, 13.4% of children with this syndrome had heart disease [17]. There are descriptions of ACC coexisting with cheilognathopalatoschisis, persisting arterial duct, and defects of the fingers and central nervous system [3, 18, 19]. Those with syndromic associations and other defects may not consider plastic surgery correction, which explains why most of the patients in the present series had
no other associated findings. In this study group, only one girl had congenital anomalies of the face, oral cavity, and heart.
The etiopathogenesis of ACC is still unclear. Environmental and genetic factors have been con-sidered. Many authors believe that ACC results from interruption of skin continuity during central nervous system development in the fetus under the influence of different intrauterine conditions (amniotic adhesions, hypertension, vascular anom-alies, embolism, ischemia) and also external trauma, pharmacological agents (methimazole, benzodiaze-pines), or viral infections [1–3, 5, 9, 11, 12, 20, 21].
Sometimes genetic determination of ACC can be clinically confirmed. In patients with lesions
Fig. 2. ACC of the apex of the skull (a), after aesthetic procedure (b)
Ryc. 2. Wrodzony ubytek skóry owłosionej szczytu głowy (a), po operacji estetycznej (b)
a)
distributed multifocally and symmetrically, hereditary origins of the malformation have not been established [1, 6]. Fullana reported a case of ACC in 12 people from a five-generation family [22]. Pousti described ACC in one of male twins with Adams-Oliver syndrome and with a heart defect. The twins’ mother had ACC of the scalp and a mitral valve defect and some members of the twins’ family had a congenital heart defect [23]. None of the patients of the present study were exposed to teratogens in the fetal period. A genetic background for the ACC was also excluded.
Histopathological examination of the resected lesion revealed the presence of cicatrix, which con-firmed present observations [1–3].
Ulceration of only skin, found shortly after birth, requires preservative treatment [1, 2, 5, 16]. Deep defects extending to the brain must be treat-ed surgically (covering with skin grafts or flaps) as early as possible to avoid bleeding and infection [3, 8, 10, 11, 14, 15].
Autogenic grafts should be used to recon-struct all layers of the defect. In case of very large defects, composite grafts of autologous fibroblasts and keratinocytes or allo-autografts (alloderm) are performed [2, 9]. In small lesions, authors sug-gest the use of temporary grafts combined with other methods of wound closure, for example the „shoelace technique“ [3]. Scars of the scalp are indications for aesthetic surgery. Depending on the lesion size and location, different methods of local plasty are used. In the patients of the pres-ent study, plasty was performed using one or more skin flaps from the nearest vicinity. Apart from local plasty techniques, ACC scalp defects can also be reconstructed with the use of expanders [2, 7, 20, 24, 25].
Patient age is of no significance. In this clinic, patients were from 2 to 17 years old were oper-ated. Results of the surgery performed for aesthetic indications are usually good, which was confirmed by the present authors’ observations.
References
Casanova D, Amar E, Bardot J, Magalon G:
[1] Aplasia Cutis Congenita. Eur J Pediatr Surg 2001, 11, 280–284.
Simman R, Priebe CJ, Simon M:
[2] Reconstruction of Aplasia Cutis Congenita of the Trunk in a Newborn Infant
Using Acellular Allogenic Dermal graft and Cultured Epithelial Autografts. Ann Plast Surg 2000, 44(4), 451–454. Vanamo K, Härmä M:
[3] The Shoelace Method in Congenital Aplasia of the Scalp and Skull. EurJ Pediatr Surg 2005, 15, 425–427.
Frieden IJ:
[4] Aplasia cutis congenital: a clinical review and proposal for classification. J Am Acad Dermatol 1986, 14(4), 646–660.
Canter HI, Vargel I, Nasir S, Kayikcioglu A:
[5] Use of a Water-Vapour Permeable Polyurethane Film (Omiderm)
in the Non-Surgical Treatment of Aplasia Cutis Congenita. Scand J Plast Reconstr Surg Hand Surg 2004, 38, 232–235.
Vijayashankar MR:
[6] Aplasia cutis congenita: a case report. Dermatol Online J 2005, 11(3), 28. Kruk-Jeromin J, Janik J, Rykała J:
[7] Aplasia Cutis Congenita of the Scalp. Dermatol Surg 1998, 24, 549–553.
Yang JY, Yang WG:
[8] Large scalp and skull defect in aplasia cutis congenita. Br J Plast Surg 2000, 53(7), 619–622. Donati V, Arena S, Capilli G, Carrera G, Ciralli F, Liberatore A:
[9] Reparation of the Severe Case of Aplasia cutis
congenita with Engineered Skin. Biol Neonate 2001, 80, 4, 273–276. Ploplys EA, Muzaffar AR, Gruss JS, Ellenbogen RG:
[10] Early Composite Cranioplasty in Infants With Severe Aplasia
Cutis Congenita: A Report of Two Cases. Cleft Palate – CraniofacJ 2005, 42, 4, 442–447. Shivakumar SK, Dwarakanath S, Swaroop G, Venkataramana NK:
[11] Aplasia cutis congenita of the scalp:
Therapeutic modalities. Neurology India 2006, 54, 3, 312–313. Izci Y, Gönül M, Secer HI, Gönül E:
[12] Aplasia cutis congenita: a rare cutaneous sign of split cord malformations.
Int J Dermatol 2007, 46, 1031–1035. Kim CS, Tatum SA, Rodziewicz G:
[13] Scalp aplasia cutis congenita presenting with saggital sinus hemorrhage. Arch Otolaryngol Head Neck Surg 2001, 127(1), 71–74.
Beekmans SJ, Haumann TJ, Vandertop WP, Mulder JW:
[14] Aplasia cutis congenita in 4 infants. Ned Tijdschr
geneeskd2002, 146(39), 1842–1845. Bajpai M, Pal K:
[15] Aplasia cutis cerebri with partial acrania – total reconstruction in a severe case and review of the literature. J Pediatr Surg 2003, 38(2), e4.
Santos de Oliveira R, Barros Jucá CE, Lopes Lins-Neto A, Aparecida do Carmo Rego, M, Farina J, Machado HR: [16]
Aplasia cutis congenita of the scalp: is there a better treatment strategy? Childs Nerv Syst 2006, 22(9), 1072–1079. Zapata HH, Sletten LJ, Pierpont ME:
[17] Congenital cardiac malformations in Adams-Oliver syndrome. Clin genet
1995, 47, 80–84.
Beekmans SJ, Wiebe MJ:
[18] Surgical treatment of aplasia cutis in the Adams-Oliver syndrome. J Craniofac Surg 2001, 12(6), 569–572.
Rajabian MH, Aghaei S:
[19] Adams-Oliver syndrome and isolated aplasia cutis congenita in two siblings. Dermatol Online J, 2006, 12(6), 17.
Martinez-Lage JF, Almagro MJ, López Hernández F, Poza M:
[20] Aplasia cutis congenita of the scalp. Childs Nerv
Moros Peña M, Labay, Matias M, Valle Sánchez F, Valero Adán T, Martin-Calama Valero J, Muñoz Albillos [21]
M: Aplasia cutis congenita in a newborn: etiopathogenic review and diagnostic approach. An Esp Pediatr 2000, 52(5), 453–456.
Fullana F:
[22] Aplasia cutis congenita of the scalp in five successive generations of the family. Plast Reconstr Surg 1995, 95, 214–215.
Pousti T:
[23] Adams Oliver Syndrome: genetics and associated anomalies of cutis aplasia. Plast Reconstr Surg 1997, 100, 1491–1496.
Gibstein LA, Abramson DL, Bartlett RA, Orgill DP, Upton J, Mulliken JB:
[24] Tissue expansion in children: a
ret-rospective study of complications. Ann Plast Surg 1997, 38(4), 358–364.
Komuro Y, Yanai A, Seno H, Ichida M, Inoue M, Miyajima M, Arai H, Sato K:
[25] Surgical treatment of aplasia
cutis congenita of the scalp associated with bilateral coronal synostosis. J Craniofac Surg 2002, 13(4), 513–519.
Address for correspondence:
Aleksandra Iljin
Department of Plastic, Reconstructive and Aesthetic Surgery Medical University of Lodz
Lutomierska 129 m. 70 91-037 Łódź
Poland
Tel.: +48 42 651 70 62 E-mail: [email protected]
Conflict of interest: None declared