32
Performance analysis and relative assessment of
turmeric, chlorhexidine gluconate and vital oil
mouthwash in anticipation of plaque
development and gingivitis
Dr. Vishal Yadav
1, Dr. Praveen B. Kudva
2, Dr. Monika Rao Goswami
3,
Dr. Geetha K Bhat
4, Dr. Hema P. Kudva
51
PG Student, Dept. of Periodontology and Implantology, Jaipur Dental College, Rajasthan 2
HOD & Prof., Dept. of Periodontology and Implantology, Jaipur Dental College, Rajasthan 3
Professor, Dept. of Periodontology and Implantology, Jaipur Dental College, Rajasthan 4
Reader, Dept. of Periodontology and Implantology, Jaipur Dental College, Rajasthan 5
Reader, Dept. of Anatomy, Jaipur Dental College, Rajasthan
ABSTRACT
Aim: To evaluate and compare clinical parameters such as plaque index and gingival index in all the groups and to evaluate and compare anaerobic bacterial count in various groups.
Objective: To evaluate and compare the efficacy of bisbiguanide mouthwash (Chlorhexidine gluconate), herbal mouthwash and essential oil mouthwash in prevention of gingivitis and plaque formation.
Methodology: A total of 100 randomly selected subjects visiting the Department of Periodontology and Implantology at Jaipur Dental College, were considered for the study. The gingival index (GI) by Loe and Silness was recorded which was followed by TureskyGilmore-Glickman modification of Quigley Hein plaque index (TQHPI) at 0, 14 and 21 days. Individuals who gave an informed consent, subjects in the age group of 25 to 35 years with having fair and poor gingival index scores and a score >1 for plaque index, were included in the study.
Results: Results showed statistically significant reduction in mean plaque index, gingival index and microbial count when the three test groups were compared to the control group. All the three mouthwashes were found to be effective in reducing plaque index, gingival index and microbial count in comparison with control group. However intergroup comparison showed no statistically significant difference in the reduction between the test groups.
Conclusion: From the above observations, it can be concluded that all the mouthwashes can be effectively used following mechanical plaque as adjuncts to control plaque and gingivitis. However chlorhexidine gluconate and herbal and essential oil mouthwash exhibited greater reduction in gingival index, plaque index and microbial scores. Turmeric mouthwashes can be an effective alternative to commercially available mouthwashes.
Clinical significance: From this study, it could be stated that turmeric is definitely a good adjunct to mechanical plaque control. Further studies are required on turmeric based mouthwash to establish it as a low cost plaque control measure.
Keywords: Turmeric mouthwash, Chlorhexidine, Gingival index, Quigley Hein plaque index.
INTRODUCTION
33 adjunct to mechanical plaque control procedures.1 A number of chemical agents have been advocated such as fluorides, bisbiguanides, essential oils, quaternary ammonium compounds, sanguinarine and triclosan, which are either available as a toothpaste/dentifrice or in the form of a mouthwash. Among these, chlorhexidine gluconate (CHX) is regarded as gold standard in dentistry for the prevention of dental plaque. Hence, a need was felt of an alternative medicine that could provide a product already enmeshed within the traditional Indian setup and is also safe and economical. Turmeric, more commonly known as ‘Haldi’, possesses anti-inflammatory, antioxidant and antimicrobial properties, along with its hepatoprotective, immunostimulant, antiseptic, antimutagenic and many more properties. Due to these reasons, it was felt that promotion of turmeric in dental terrain may prove beneficial.
MATERIALS AND METHODS
The study was conducted in Department of Periodontology and Implantology at Jaipur Dental College, India. Nature of study was explained and an informed consent was obtained from all subjects. The subjects were randomly divided into any of the groups by toss of coin method for radomization. Scaling was done using ultrasonic scalers in a single siting. 21 days post scaling the baseline values were recorded. The clinical parameters assessed were plaque index (PI) by Silness and Loe and gingival index (GI) by Loe and Silness at 0 and 30 days in all the groups.
MICROBIOLOGICAL STUDY
34 The gingival index Loe and Silness (1963) was recorded on day 0 and 30 using william graduated periodontal probe.
The plaque samples were transported to reduced transport fluid. Anaerobic bacterial count was done pre treatment and post treatment by incubating samples in 5% CO2 condition using candle jar dessicator at 37 degrees C for 48 hours.
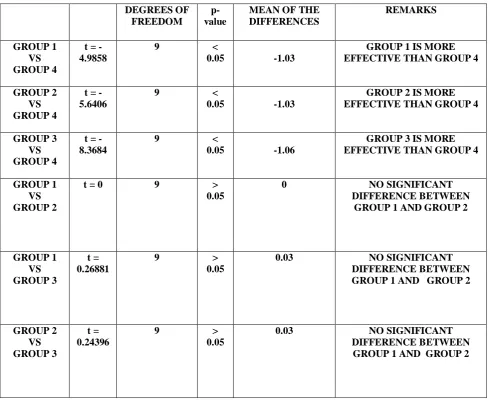
35 Table 1: Comparision of Anaerobic Bacterial Count Between Various Groups Using Paired T-Test
DEGREES OF FREEDOM
p-value
MEAN OF THE DIFFERENCES
REMARKS
GROUP 1 VS GROUP 4
t = -4.9858
9 <
0.05 -1.03
GROUP 1 IS MORE EFFECTIVE THAN GROUP 4
GROUP 2 VS GROUP 4
t = -5.6406
9 <
0.05 -1.03
GROUP 2 IS MORE EFFECTIVE THAN GROUP 4
GROUP 3 VS GROUP 4
t = -8.3684
9 <
0.05 -1.06
GROUP 3 IS MORE EFFECTIVE THAN GROUP 4
GROUP 1 VS GROUP 2
t = 0 9 >
0.05
0 NO SIGNIFICANT
DIFFERENCE BETWEEN GROUP 1 AND GROUP 2
GROUP 1 VS GROUP 3
t = 0.26881
9 >
0.05
0.03 NO SIGNIFICANT
DIFFERENCE BETWEEN GROUP 1 AND GROUP 2
GROUP 2 VS GROUP 3
t = 0.24396
9 >
0.05
0.03 NO SIGNIFICANT
DIFFERENCE BETWEEN GROUP 1 AND GROUP 2
DISCUSSION
In all the above studies in relation to turmeric, antiinflammatory effect was observed but not in relation with gingiva. In our study, anti-inflammatory action of turmeric was evaluated on clinical parameters using the gingival index, which showed significant reduction. On evaluating the literature, the possible mechanism of action of turmeric as an anti-inflammatory agent could be due to its inhibitory action on prostaglandin synthesis and a strong stabilizing action on the lysosomal membranes. Taking into consideration the findings of our study, it is clear that The effectiveness of chlorhexidine on clinical and microbiological parameters is attributed due to anti plaque property of chlorhexidine gluconate.The molecule binds to cell membrane resulting in leakage of intercellular components. It is bacteriocidal in high concentration. The results go in agreement with studies carried out by Francetti et al (2002), Grundemann et al (2002), JL Leys (2002), and GA Vander, CJ Timmerman, MS Mantel (1998) who found improvement in clinical and microbiological parameters. The effectiveness of herbal (turmeric) mouthwash on clinical and microbiological parameters is attributed due to the anti-inflammatory property, which could be due to its inhibitory action on prostaglandin synthesis and strong stabilizing action on the lysosomal membranes.
SUMMARY AND CONCLUSION
36 exhibited greater reduction in gingival index, plaque index and microbial scores. Turmeric mouthwashes can be an effective alternative to commercially available mouthwashes. 3 subjects complained of bitterness with chorlhexidine and 1 subject with essential oil mouth rinse. No discomfort was noted with use of herbal mouthrinse but further long term use needs to be assessed. Turmeric mouthwash was biocompatible and also well accepted by all the subjects without side effects.
REFRENCES
[1]. Mishra M.B., Bhisen A.K., and Mishra S.. 2011, Peripheral Ossifying Fibroma: Report of two unusual cases. J. Oral Maxillo Path 6: 65-68
[2]. Farquha T., MacLellan J., Dyment H., and Anderson R.D., Peripheral Ossifying Fibroma: A Case Report, J. Am. Dent. C., 74: 809-812
[3]. Mathur S., and Manjunath S.M., 2014, Peripheral Ossifying Fibroma: A Review. Int. J. Dent Med. Res., 1: 116-118
[4]. Ramu S., and Rodrigues C., 2012, Reactive Hyperplastic Lesions of the Gingiva: A Retrospective Study of 260 Cases. World Journal of Dentistry 3: 126-130
[5]. Reddy V.G., Reddy J.K., Ramlal G., and Ambati M., 2011, Peripheral ossifying fibroma: Report of two unusual cases. Indian J. Stomatol, 2: 130-133
[6]. Kumar S.K., Ram S., Jorgensen M.G., Shuler C.F., and Sedghizadeh P.P., 2006, Multi-centric peripheral ossifying fibroma. Journal of Oral Sci., 48: 239-243
[7]. Patil D.P., Kanakdande V., Kalele K.P., and Nayyar A.S., 2015, Recurrent peripheral giant cell granuloma: A case report. NJIRM 6: 125-130
[8]. Gardner D.G., 1982, The peripheral odontogenic fibroma: An attempt at clarification. Oral Surg. Oral Med. Oral Pathol., 54: 40-48
[9]. Fine HD. Chemical agents to prevent and regulate plaque development. Perio 2000 1995; 8:87-107. [10]. Lindhe Jan. Textbook of clinical periodontology and implant dentistry (5th ed)748-54.
[11]. Van der Ouder FJG. Anti-plaque agents. Rationale and prospects for prevention of gingivitis and periodontal diseases. J Clin periodon 1991;18:6:447-54.
[12]. Ivan Ross A. Medical Plant of the World Textbook; Human press Inc, Tatowa, New Jersey 1999. [13]. Dunning JM. Principles of Dental Public Health (4th ed). Harvard University Press 1984:322.
[14]. Loe H, Silness J. Periodontal disease in pregnancy: Prevalence and Severity. Acta Odontol Scand 1963;21:533-51.
[15]. Turesky S, Gilmore ND, Glickman I. Reduced plaque formation by the chloromethyl analogue of Victamine C. J Periodontol 1970;41:41-43.
[16]. Leyes Borrajo JL, Garcia Varela L, Lopez Castro G, et al. Efficacy of chlorhexidine mouthrinses with and without alcohol: A clinical study. J Periodontol 2002;73:317-21.
[17]. Grundenman LJMM, Timmerman MF, Ijserman Y, et al. Reduction of stain, plaque and gingivitis by mouthrinsing with chlorhexidine and sodium perborate. Ned Tandheelkd J Periodontol July 2002; 109(7):225-31.
[18]. Francetti L del, Fabbro M, Testroi T, et al. Chlorhexidine spray versus chlorhexidine mouthwash in the control of dental plaque after periodontal surgery. J Clin Periodontology 2000;27: 425-30.
[19]. Bhandari H, Shankwalkar GB. Clinical assessment of action of combination of indigenous drugs on dental plaque, calculus and gingivitis. Dissertation submitted to the University of Bombay 1980.
[20].
[21]. Babu B.K., Kalwa P., and Naag S., 2010 Kumar A.P., Peripheral ossifying fibroma. Ker Dent J; 33: 219-221
[22]. Patil K.P., Kalele K.P., and Kanakdande V.D., 2014, Peripheral giant cell granuloma: Comprehensive review of an ambiguous lesion. J. Int. Clin. Dent. Res. Org.6: 118-125
[23]. Kale L., Khambete N., and Sodhi S., 2014, Sonawane S., Peripheral ossifying fibroma: Series of five cases, J. Ind. Soc. Perio., 18: 527-530
[24]. Mohiuddin K., Priya N.S., Ravindra S., and Murthy S. 2013, Peripheral ossifying fibroma. Journal of Indian Society of Periodontology 17: 507-509
[25]. Reddy G.V., Reddy J., Ramlal G., and Ambati M., 2011, Peripheral ossifying fibroma: Report of two unusual cases. Indian J. Stomatol, 2: 130-133
[26]. Farquhar T., Maclellan J., Dyment H., and Anderson R.D., 2008, Peripheral ossifying fibroma: A case report. J. Can. Dent. Assoc., 7: 809-812
[27]. Shetty D.C., Urs A.B., Ahuja P., Sahu A., Manchanda A., and Sirohi Y., 2011, Mineralized components and their interpretation in the histogenesis of peripheral ossifying fibroma. Indian J. Dent Res., 22: 56-61