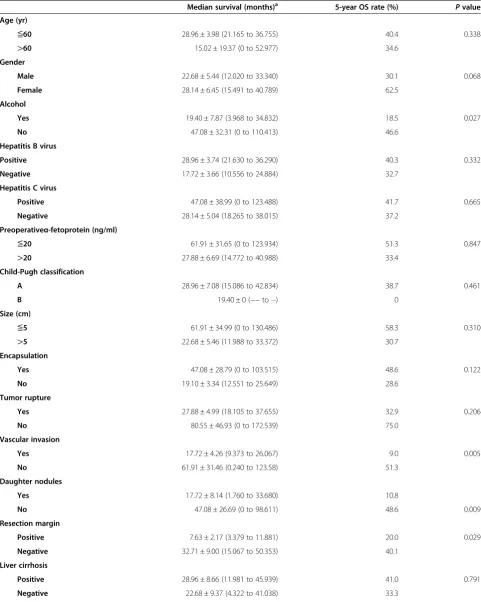
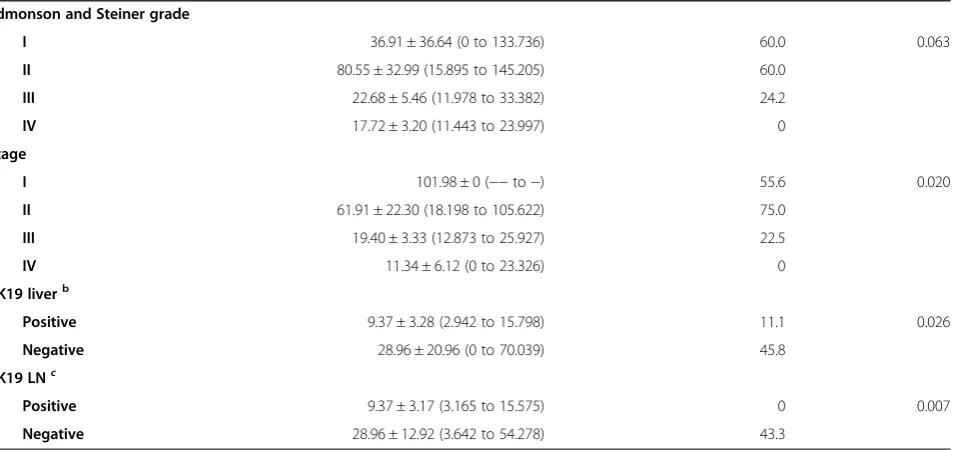
The expression of cytokeratin 19 in lymph nodes was a poor prognostic factor for hepatocellular carcinoma after hepatic resection
11
0
0
Full text
Figure



+4


Related documents