Trans-Rectal Ultrasonographic Appearance of
Abnormal Combined Utero-Placental Thickness
in Late-Term Gestation and its Incidence During
Routine Survey in a Population of Thoroughbred
Mares (2005–2008)
Jorge L. Colo´ n, DVM
Diagnosis and treatment of placentitis early in the course of the disease process is essential to the success of producing a full-term viable foal. Early diagnosis can be achieved through routine survey of the transrectal combined utero-placental thickness (CUPT) during late-term gestation of Thor-oughbred mares in clinical practice. Author’s address: PO Box 11631, Lexington, KY 40576; e-mail: [email protected]. © 2008 AAEP.
1. Introduction
Early detection of placental failure in the mare has been deemed essential for the successful manage-ment and treatmanage-ment of mares affected with placen-titis.1– 4 Attempts to treat mares after they have started to show external clinical signs of placental failure are often disappointing.2 Clinical observa-tions of vaginal discharge and premature udder de-velopment often imply that the disease process is past the early stage where it may have been more responsive to treatment. Most cases of placentitis in the mare originate from ascending infections through the cervix; the most common bacterial agents areStreptococcus equi subspecies zooepidemi-cus, Escherichia coli, Pseudomonas aeruginosa,
Klebsiella pneumoniae, and nocardioform spe-cies.1,5–7 Increased combined utero-placental thickness (CUPT) and evidence of placental separa-tion with accumulasepara-tion of hyperechoic fluid are
ul-trasonographic signs of placentitis.1,8 –11 Early and frequent trans-rectal ultrasonographic examina-tions of the placenta around the area of the cervical star will increase the clinician’s ability to better detect early signs of placental inflammation before external clinical signs can be seen.2,8,12,13
Several studies have established normal values for trans-rectal measurements of the CUPT in the mare in mid and late gestation.2,14 –16 Renaudin et al.2 and Troedsson et al.12 suggest that their ob-tained measurements combined with a 95% confi-dence interval (CI) may be used as a reference for clinical indication of placentitis and other placental abnormalities. Other studies have also suggested that deviations from these values are associated with placental failure and pending abortion, and suspicion of placentitis by detection of increased CUPT can be confirmed by histopathological exam-ination of fetal membranes post-foaling.12,17
In a retrospective study, Troedsson and Zent9
re-ported a 3.1% rate of placentitis found by abnormal CUPT measurement, and 15.8% of the affected mares aborted despite medical treatment. The af-fected mares that carried to term had a mean ges-tation of 327 ⫾ 2.23 days. Interestingly, the average birth weight of those foals born at term to affected mares was no different from the weight of those born to unaffected mares.
Treatment strategies for the management of pla-centitis have been directed toward combating infec-tion, reducing inflammation, and controlling myometrial activity.1,3,6,18 –21 The
pharmacokinet-ics of trimethoprim-sulfamethoxazole (TMP-SMZ) and pentoxifylline (PTX) in allantoic fluid of preg-nant mares has been studied by University of Flor-ida researchers.22 They have shown good uterine
penetration for both drugs and a potential for down-regulation of pro-inflammatory cytokines by PTX.6
Several studies have reported increased success in the management of mares with placentitis when using a combination of TMP-SMZ, PTX, and altreno-gest (ALT).9,12,18,20,21 The data suggests that
long-term combination treatment may delay the effects of placental failure in mares with placentitis, which can lead to a positive impact on pregnancy outcome. The anti-prostaglandin effect of progestins has been advocated as a means of reducing prostaglandin-induced myometrial activity in the mare. Daels et al.23showed that progestin supplementation helped to prevent prostaglandin-induced abortion during the first trimester. Two reports by Bailey et al.18,20 reported successful reduction of the effects of infec-tion and inflammainfec-tion in initiating pre-term labor
with long-term treatment of placental infections with TMP-SMZ, PTX, and ALT.18,20 The data showed that 83% of the live foals born to mares medically treated after undergoing experimentally induced placentitis had a negative blood culture at birth.
The purpose of this study was to present field-accumulated data regarding the abnormal trans-rectal ultrasonographic combined utero-placental thickness measurement and appearance of early stage cases of placentitis obtained during routine survey of clinically normal Thoroughbred mares in late-term gestation. The goal of the study was to early diagnose potential cases of placentitis and to institute medical treatment in the early stages of disease to reduce or eliminate the incidence of fetal disease or death secondary to placental failure. 2. Materials and Methods
Trans-rectal ultrasonographic measurement of the combined utero-placental thickness was performed by a single examiner on 106 Thoroughbred pregnan-cies at two private farms over three breeding sea-sons between 2005 and 2008. The CUPT was obtained just cranial to the placento-cervical junc-tion in the ventral part of the uterine body just dorsal to the middle branch of the uterine artery as previously described (Fig. 1).2 Measurements were performed at 270, 300, and 330 days gestation as defined by the number of days post-breeding. Ges-tational length was defined as the number of days between foaling date and last breeding date. For the 2005–2006 breeding season, only measurements at 300 and 330 days were obtained. Not all mares Fig. 1. Measurement of the CUPT in a normal mare just cranial to the cervico-placental junction in the ventral part of the uterine body dorsal to the middle branch of the uterine artery (cranial is to the left).
were available for all measurements or for foaling-date data because of horse movement, sale, or other extra-neous circumstances. An analog ultrasound with a 6.0/8.0-mHz linear transducerawas used for the first
year of the study and a 7/3 mHz linear transducerb was used for the remainder of the study. If required, a Caslick’s procedure was performed on all mares after confirmation of ovulation post-breeding.
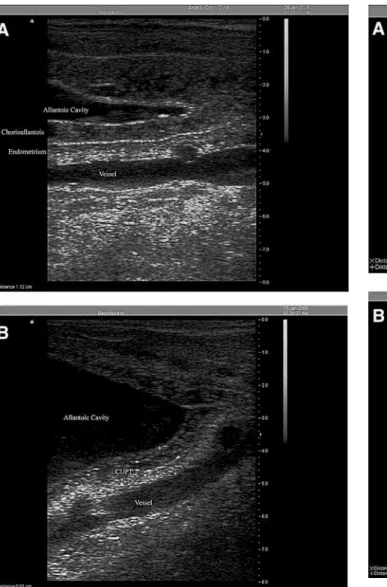
Abnormal CUPT was defined as those measure-ments that deviated from the 95% CI of previously defined normal values.2 It was also defined as those CUPT that had a two-layer ultrasonographic appearance, which indicates a distinguishable de-marcation between the chorioallantois and the uterus (Fig. 2, A and B). Presence of pockets within the layers and/or areas of placental separation were noted (Fig. 3, A and B). Based on treatment data provided by previous research,18,20 all mares with
abnormal CUPT were treated with TMP-SMZc (30
mg/kg, q 12 h, PO), PTXd (8.5 mg/kg, q 24 h, PO),
and ALTe (0.088 mg/kg, q 24 h, PO) until foaling. When an abnormal CUPT was observed, serial ul-trasonographic examinations and measurements were carried out on a weekly to biweekly frequency until foaling.
A necropsy was performed at the University of Kentucky Livestock Disease Diagnostic Center on the fetal membranes of mares who had an abnormal CUPT during routine survey. Neonatal examina-tions were performed, and the examiner obtained neonatal bloodwork profiles for all foals born at the farms in the study. Necropsy of fetal membranes, post-foaling uterine culture, and neonatal blood cul-ture were performed on the six abnormal CUPT cases that foaled in 2008. A local laboratory was used for cultures and bloodwork. Using a personal weight scale, the birth weight of some of the foals and the weight of their corresponding fetal mem-branes were obtained within the first 12 h of life. Fig. 2. Abnormal CUPT in two separate cases (A and B) of
placentitis with distinguishable demarcation between the cho-rioallantois and uterus (cranial is to the left).
Fig. 3. Abnormal CUPT in two separate cases (A and B) of placentitis with pockets of placental separation containing hy-perechoic material (cranial is to the left).
3. Results
One hundred and six pregnancies were examined on 77 different mares during the survey for measure-ment of the CUPT. Included within the group were 11 mares that were evaluated in two breeding sea-sons and 9 that were evaluated on all three seasea-sons of the study. Overall, 16 pregnancies (15% [16/106] of total pregnancies) were found to have at least one abnormal CUPT measurement at some point during the study. The 16 abnormal CUPT pregnancies were carried by 15 mares. One mare was abnormal in two different seasons. Of those 15 mares, 2 were studied over two breeding seasons, and 5 were stud-ied over three breeding seasons.
A total of 225 individual measurements were per-formed during the study. Eighty-five percent of the total measurements (192/225) were considered nor-mal, and 15% (33/225) were considered abnormal (Table 1).
Of the 192 normal measurements, 60 were ob-tained at 270 days gestation with an average CUPT of 0.55⫾0.09 cm, 80 were obtained at 300 days with an average CUPT of 0.71 ⫾ 0.13 cm, and 52 were obtained at 330 days with an average CUPT of 0.85⫾0.17 cm. An average gestation of 344⫾7.3 days was obtained from the records of 81 of these cases (Table 2).
Of the 33 abnormal measurements, 5 were ob-tained at 270 days gestation with an average CUPT of 0.95⫾0.14 cm, 14 were obtained at 300 days with an average CUPT of 1.20 ⫾ 0.14 cm, and 14 were obtained at 330 days with an average CUPT of 1.16⫾0.36 cm. An average gestation of 340⫾6.1 days was obtained from the records of 15 of these cases (Table 3).
Of the 16 cases that were diagnosed with abnor-mal CUPT, 5 had evidence of placental separation with accumulation of hyperechoic fluid. Medical treatment was instituted at the first observation of abnormal CUPT. All five cases found with mal CUPT at 270 days gestation were still abnor-mally increased at 300 days. Nine of twelve cases abnormal at 300 days had a reduced CUPT mea-surement by day 330; of those, six had returned to normal levels but still had an abnormal ultrasono-graphic appearance, and they were, therefore, con-sidered abnormal. The distinguishable line of demarcation between the chorioallantois and uterus was observed on all abnormal CUPT.
Four cases, observed with normal CUPT at 270 days, had abnormal CUPT at 300 days. One case was normal at 270 and 300 days but abnormal at 330 days. One case was normal at 300 days but abnormal at 330 days. Of the 16 cases placed on medical treatment, 4 were started ⬃day 270 and treated for an average of 65 ⫾ 13.5 days, 8 were started⬃day 300 and treated for an average of 39⫾ 5.1 days, and 2 were started⬃day 330 and treated for an average of 16⫾0.7 days (two horses were lost from the study because of sale).
Ninety-six foals, including 15 from abnormal CUPT cases, were born within the study. All preg-nancies in the study were carried to term an average of 344 ⫾ 7 days. Eighteen foals of the normal CUPT cases had an average foal birth weight of 114.2 ⫾ 14.6 lbs (51.9 kg) and an average fetal membranes weight of 15.7⫾ 4.4 lbs. (7.1 kg; Table 2). Five foals of the abnormal CUPT cases had an average foal birth weight of 114⫾11.2 lbs (51.8 kg)
Table 1. Incidence of Normal and Abnormal CUPT Measurements at Different Stages of Late-Term Gestation During Routine Survey in a Population of Thoroughbred Mares
Total Measurements At 270 days At 300 days At 330 days
225 65 94 66
Normal 192 (85%) 60 (92%) 80 (85%) 52 (79%)
Abnormal 33 (15%) 5 (8%) 14 (15%) 14 (21%)
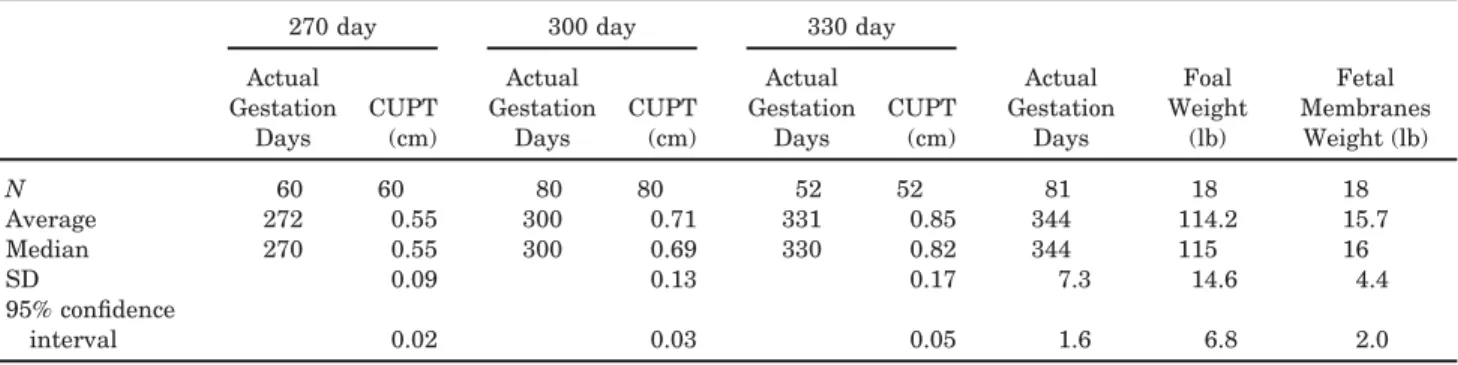
Table 2. Averages of Normal CUPT Measurements and Their Corresponding 95% CI and Standard Deviation (SD) During Different Stages of Late-Term Gestation, Together With Average Gestation Days and Weights of Foals and Fetal Membranes Born to Unaffected Mares
270 day 300 day 330 day
Actual Gestation Days Foal Weight (lb) Fetal Membranes Weight (lb) Actual Gestation Days CUPT (cm) Actual Gestation Days CUPT (cm) Actual Gestation Days CUPT (cm) N 60 60 80 80 52 52 81 18 18 Average 272 0.55 300 0.71 331 0.85 344 114.2 15.7 Median 270 0.55 300 0.69 330 0.82 344 115 16 SD 0.09 0.13 0.17 7.3 14.6 4.4 95% confidence interval 0.02 0.03 0.05 1.6 6.8 2.0
and an average fetal membranes weight of 16.2⫾ 2.9 lbs. (7.4 kg; Table 3).
Necropsies of fetal membranes of 11 of the mares with abnormal CUPT revealed 3 cases where no disease process was identified. Six cases were di-agnosed as placental edema, one case was didi-agnosed as mild multifocal chronic placentitis, and one case was diagnosed as moderate, chronic multifocal sup-purative placentitis. Of the six abnormal cases foaled during 2008, four had a negative post-foaling uterine culture with a negative blood culture on the respective foals. Two cases that were treated since day 270 of gestation had a methycillin-resistant
Staphyloccocus aureus on the uterine culture; the first case had aStaphyloccocus aureuson the foal’s blood culture, and the second case had no growth on the foal’s blood culture. Neither one had any pathogenic bacteria isolated from the culture of the placenta at necropsy.
4. Discussion
Routine survey of trans-rectal CUPT in a population of Thoroughbred mares revealed early ultrasono-graphic signs of placentitis before external clinical signs were evident. Placental edema was noted in all 16 of the affected cases, and 5 of them had evi-dence of pockets of separation between the cho-rioallantois and uterus that contained hyperechoic material. Treatment with TMP-SMZ, PTX, and ALT since the early stages of the disease process seemed to be successful in the maintenance of full-term pregnancy in all abnormal cases despite the presence of placentitis as confirmed by histopathol-ogy of fetal membranes.
PTX treatment was performed q 24 h at the be-ginning of the study period because of the long-term economics of q 12 h treatments. The examiner elected to continue this once a day treatment based on the empirical observations and results obtained. Whether or not the pharmacokinetics of once a day PTX treatment is adequate cannot be corroborated by the present study and would have to be the sub-ject of future experimentation. The successful management of placentitis presented in the study at hand, however, concurs with the referenced reports
that affirm that long-term combination treatment with TMP-SMZ, PTX, and ALT delays the effects of placental failure in mares with placentitis, which leads to a positive impact on pregnancy outcome. All abnormal CUPT cases carried their pregnancies to term and delivered a live foal.
As reported by histopathologic findings, the gross and histologic lesions observed on the fetal mem-branes examined were most likely a result of a chronic process consistent with the history of pla-centitis that had, for the most part, resolved because of prolonged medical treatment. The Staphylocco-cus aureusorganism obtained from the blood culture of one foal was consistent with the microbiologic appearance of what the laboratory considers “skin contaminant,” and although it could not be elimi-nated as a causative organism in the case, it was not recovered from either the uterus or placenta. The methycillin-resistant Staphyloccocus aureus cul-tures obtained from the uterus of two cases were attributed to prolonged antibiotic treatment (63 and 72 days) that led to bacterial resistance. Again, the organism was not recovered from the foal’s blood culture or the placenta in either case. Eighty-three percent (5/6) of the cultured foals born to affected mares in the current study presented a true nega-tive blood culture after being treated in utero; the one positive culture was most likely caused by a contaminant.
Measurements of normal CUPT values in this study were consistent with those previously re-ported by Renaudin et al.2 in 1997. More
impor-tantly, this study presents actual measurement values for abnormal CUPT and associated 95% CI and SD for measurements during different stages of late-term gestation. A distinguishable edematous line of demarcation between the chorioallantois and uterus was consistently observed ultrasonographi-cally on those cases of abnormal CUPT. This dif-fers from the findings of the 1999 case report by Renaudin et al.17where the clinicians were able to distinguish between uterus and chorioallantois in a case of experimentally induced placentitis but not in a naturally occurring case of placentitis defined by abnormal CUPT (0.95 cm at 303 days gestation).
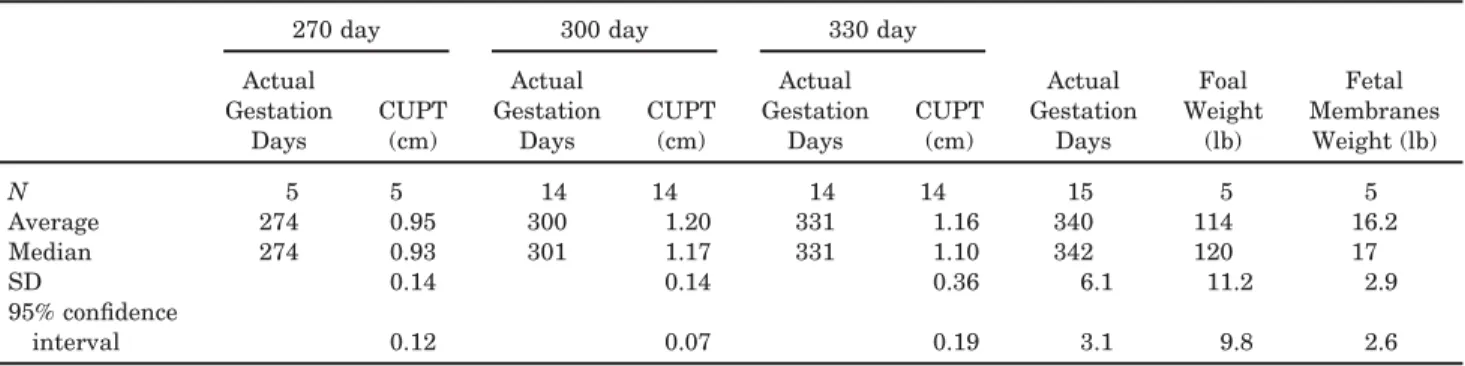
Table 3. Averages of Abnormal CUPT Measurements and Their Corresponding 95% CI and SD During Different Stages of Late-Term Gestation, Together With Average Gestation Days and Weights of Foals and Fetal Membranes Born to Affected Mares
270 day 300 day 330 day
Actual Gestation Days Foal Weight (lb) Fetal Membranes Weight (lb) Actual Gestation Days CUPT (cm) Actual Gestation Days CUPT (cm) Actual Gestation Days CUPT (cm) N 5 5 14 14 14 14 15 5 5 Average 274 0.95 300 1.20 331 1.16 340 114 16.2 Median 274 0.93 301 1.17 331 1.10 342 120 17 SD 0.14 0.14 0.36 6.1 11.2 2.9 95% confidence interval 0.12 0.07 0.19 3.1 9.8 2.6
The greater percentage of abnormal measure-ments observed at 300 days gestation occurred for two reasons: all abnormal cases at 270 days were still abnormal at 300 days despite being on treat-ment, and there were abnormal cases noted at 300 days that were normal at 270 days. Only two cases were originally observed to be abnormal at 330 days gestation after having been normal previously. Those mares that were started on treatment before 300 days gestation showed measured improvement at 330 days; however, the abnormal edematous ul-trasonographic appearance persisted until foaling. Medical treatment reduced the CUPT measurement in 75% (9 of 12) of the cases by day 330, which includes six (50%; 6 of 12) that had returned to normal values by 330 days gestation. The obtained data for the average abnormal CUPT at 330 days was lower than expected (but with a higher SD) because of the positive effects of medical treatment. The two cases that were originally found abnormal at 330 days had measurements of 1.4 cm and 2.2 cm (average⫽1.80⫾0.57 cm); in comparison, the other 12 cases that had previously been started on treat-ment had an average CUPT of 1.05⫾0.19 cm at 330 days. The persistent abnormal ultrasonographic manifestation of placentitis implies that the visual appearance of placental edema is just as important as increased CUPT measurement in the early diag-nosis of placentitis and that treatment should not be terminated when CUPT values return to normal levels in the face of abnormal ultrasonographic CUPT appearance.
The current study presents three main points that deviate from previously reported findings.9,12 First,
this study showed that 15% of cases examined (16/106) had signs of abnormal CUPT (compared with 3.1% reported). This much higher figure points to a higher incidence of disease than that previously observed; this is probably because the whole population of horses was surveyed and not just the ones that might have been deemed at risk. Second, none of the abnormal cases in this study failed to carry a foal to term com-pared with the 15.8% pregnancy loss previously re-ported; presumably, this is because of the implementation of treatment earlier in the disease process. Last, foals from abnormal cases were car-ried longer to an average of 340⫾6.1 days (versus 327 days as reported), which is consistent with full-term gestation of normal mare. The one constant between this study and the reports referenced was that the comparable average birth weight of those foals born to affected mares was no different from the weight of those born to unaffected mares.
The data acquired suggest that survey measure-ments should be started⬃270 days gestation, treat-ment should be initiated when placentitis is first diagnosed, and treatment should be continued until foaling occurs. Economic and logistic factors must be studied before deciding to diagnose and treat a potential placentitis for ⬎20% of the gestation pe-riod (before day 270). This study also suggests that
all mares in a population should be surveyed; the common thought that placentitis mares are at risk for future episodes is not supported by the presented data, because only 1 of 20 mares studied over more than one season was a repeat case of abnormal CUPT.
This study supports the fact that diagnosis and treatment of placentitis early in the course of the disease process is essential to the success of produc-ing a full-term viable foal. The incidence of placen-titis in a field setting seems to be much greater than previously reported. The ultrasonographic appear-ance of chorioallantoic edema, premature separation of fetal membranes, and accumulation of purulent ma-terial between the membranes and uterus can easily and consistently be observed in cases of abnormal CUPT. More importantly, this study proves that early diagnosis and medical management of placenti-tis can be achieved through routine survey during late-term gestation of the trans-rectal CUPT of Thor-oughbred mares in clinical practice.
References and Footnotes
1. Macpherson ML, Troedsson MHT. Diagnosis and treatment of equine placentitis, in Proceedings. 2nd West Coast Equine Reproduction Symposium 2005;75– 86.
2. Renaudin CD, Troedsson MHT, Gillis CL, et al. Ultrasono-graphic evaluation of the equine placenta by transrectal and transabdominal approach in the normal pregnant mare.
The-riogenology1997;47:559 –573.
3. Macpherson ML. Diagnosis and treatment of equine placen-titis. Vet Clin North Am [Equine Pract]2006;22:763–776. 4. Vaala W. New perspectives on the late-term mare and
new-born foal, inProceedings. 53rd Annual American Associa-tion of Equine PractiAssocia-tioners ConvenAssocia-tion 2007;281–292. 5. Giles RC, Donahue JM, Hong CB, et al. Causes of abortion,
stillbirth, and perinatal death in horses: 3,527 cases (1986 – 1991). J Am Vet Med Assoc1993;203:1170 –1175.
6. Macpherson ML. Treatment strategies for mares with pla-centitis. Theriogenology2005;64:528 –534.
7. Calderwood Mays MB, LeBlanc MM, Paccamonti D. Route of fetal infection in a model of ascending placentitis.
Ther-iogenology2002;58:791–792.
8. Kelleman AA, Luznar SL, Lester GD, et al. Evaluation of transrectal ultrasonographic combined thickness of the uterus and placenta (CTUP) in a model of induced ascending placentitis in late gestation in the pony mare. Theriogenol-ogy2002;58:845– 848.
9. Troedsson MHT, Zent WW. Clinical ultrasonographic evalua-tion of the equine placenta as a method to successfully identify and treat mares with placentitis, inProceedings. Workshop on the Equine Placenta 2004;66 – 67.
10. Reef VB, Vaala WE, Worth LT, et al. Transcutaneous ultra-sonographic assessment of fetal well-being during late gesta-tion: a preliminary report on the development of an equine biophysical profile, inProceedings. 42nd Annual American Association of Equine Practitioners Convention 1996;152– 153.
11. Reef VB, Vaala WE, Worth LT, et al. Ultrasonographic as-sessment of fetal well-being during late gestation: develop-ment of an equine biophysical profile. Equine Vet J1996; 28:200 –208.
12. Troedsson MHT, Renaudin CD, Zent WW, et al. Transrectal ultrasonography of the placenta in normal mares and in mares with pending abortion: a field study, inProceedings. 43rd Annual American Association of Equine Practitioners Convention 1997;256 –258.
13. Sheerin PC, Morris S, Kelleman A, et al. Diagnostic effi-ciency of transrectal ultrasonography and plasma progestin
profiles in identifying mares at risk of premature delivery, in
Proceedings. 49th Annual American Association of Equine
Practitioners Convention 2003;22–23.
14. Bucca S, Fogarty U, Collins A, et al. Assessment of feto-placental well-being in the mare from mid-gestation to term: transrectal and transabdominal ultrasonographic features.
Theriogenology2005;64:542–557.
15. Renaudin CD, Troedsson MHT, Gillis CL. Transrectal ultra-sonographic evaluation of the normal equine placenta. Equine
Vet Edu1999;11:75–76.
16. Barnes M, Fite C, Tibary A. Trans-rectal ultrasonographic evaluation of the placenta in Arabian and pony mares in mid-to-late gestation. Theriogenology2005;64:787. 17. Renaudin CD, Troedsson MHT, Schrenzel MD. Transrectal
ultrasonographic diagnosis of ascending placentitis in the mare: a report of two cases. Equine Vet Edu1999;11:69 –74. 18. Bailey CS, Macpherson ML, Graczyk J, et al. Treatment
efficacy of trimethoprim sulfamethoxazole, pentoxifylline, and altrenogest in equine placentitis. Theriogenology2007; 68:516 –517.
19. Blanchard TL, Varner DD, Schumacher J, et al. Manage-ment of the pregnant mare. In: Manual of equine
repro-duction, 2nd ed. St. Louis: Mosby, 2003;93–105.
20. Bailey CS, Macpherson ML, Graczyk J, et al. Treatment efficacy of trimethoprim sulfamethoxazole, pentoxifylline,
and altrenogest in equine placentitis, inProceedings. 53rd Annual American Association of Equine Practitioners Con-vention 2007;339 –340.
21. Macpherson ML. Identification and management of the high risk pregnant mare, inProceeding. 53rd Annual Amer-ican Association of Equine Practitioners Convention 2007; 293–304.
22. Rebello S, Macpherson ML, Murchie T, et al. The detection of placental drug transfer in equine allantoic fluid.
Theriog-enology2005;64:776 –777.
23. Daels PF, Besognet B, Hansen B, et al. Effect of progester-one on prostaglandin F-2 alpha secretion and outcome of pregnancy during cloprostenol-induced abortion in mares.
Am J Vet Res1996;57:1331–1337.
aPie Medical 485 Anser with 6.0/8.0-mHz linear transducer,
Classic Medical, 19900 Mona Rd #105, Tequesta, FL 33469.
bTeraVet 2000 PC Notebook with 7L3 (7/3-mHz) linear
trans-ducer, Classic Medical, 19900 Mona Rd #105, Tequesta, FL 33469.
cSMZ-TMP, Interpharm, Hauppauge, NY 11788.
dPentoxifylline Oral Gel, Hagyard, Davidson & McGee
Phar-macy, Lexington, KY 40511.