The Effect of FDG-PET on the Stage Distribution of
Non-small Cell Lung Cancer
Daniel Morgensztern, MD,*† Boone Goodgame, MD,* Maria Q. Baggstrom, MD,* Feng Gao, PhD,‡
and Ramaswamy Govindan, MD*
Purpose:To study the impact of18
F-fluorodeoxyglucose positron emission tomography (FDG-PET) on stage distribution and survival for patients with newly diagnosed non-small cell lung cancer (NSCLC).
Methods: We searched the Barnes-Jewish Hospital/Washington University School of Medicine database for patients with non-small cell lung cancer (NSCLC) diagnosed between January 1, 1990 and December 31, 2004. Since the use of FDG-PET increased in our institution in the year 2000, patients were subdivided into those diagnosed before or after January 1, 2000. We compared the stage distribution of NSCLC before and after the year 2000. We also compared the survival for patients diagnosed between 2000 and 2004 staged with or without FDG-PET.
Results:We identified 6118 patients diagnosed with NSCLC, with 3765 (61%) diagnosed before the year 2000 and 2362 (39%) thereafter. The use of FDG-PET was significantly increased after the year 2000 (37% versus 7%,p⬍0.001) and there was a significant increase in the proportion of stage IV patients (30 –37%,p⬍0.001) with an associated decrease in stages I and III. Median overall survival was increased in all patients with stage IV disease diag-nosed after the year 2000 (5.8 months versus 4.5 months). Patients with stage III or IV disease staged with FDG-PET scan also had improved survival compared with those undergoing conventional staging
Conclusion:The increased use of FDG-PET was associated with a stage migration in patients with NSCLC, which may partially account for improvements in survival as compared with historical controls.
Key Words:PET, Outcomes, Non-small cell lung cancer, Staging, Stage distribution, Population.
(J Thorac Oncol.2008;3: 135–139)
L
ung cancer is the second most common malignancy in the United States with an estimated 213,380 new patients diagnosed in 2007, and the leading cause of cancer mortality with 162,460 deaths projected for the same year.1Non-small cell lung cancer (NSCLC) accounts for approximately 86% of the total number of lung cancer cases.2Virtually all patients with known or suspected NSCLC undergo a computed tomography (CT) of the chest and upper abdomen including liver and adrenal glands as the initial anatomic imaging modality of choice, followed by bone scan and brain imaging in selected cases.3Although CT is useful in evaluating the primary tumor size and location, it has limited ability to differentiate between benign and malignant lesions or tumor and atelectasis. It is also not a reliable noninvasive modality for the evaluation of mediastinal ade-nopathy.4 Whole body positron-emission tomography (PET) with18F-fluorodeoxyglucose (FDG) has an established role in the staging of lung cancer patients.
Although FDG-PET is widely considered to be more accurate than CT scan for both locoregional and metastatic disease, there have been no population-based studies evalu-ating its effect on stage distribution among patients with NSCLC. We hypothesized that a more frequent use of PET would increase the relative proportion of stage IV disease at the time of diagnosis because of an increased identification of distant metastatic sites. A secondary objective of the study was to determine if the stage-specific survival of NSCLC had changed because of earlier identification of metastatic dis-ease. We performed a retrospective analysis of patients seen at our institution to evaluate variations in stage frequency and survival between patients diagnosed before and after the widespread availability of this imaging technique.
PATIENTS AND METHODS
We identified all patients with NSCLC diagnosed at our institution between January 1, 1990 and December 31, 2005 using the hospital tumor registry. This registry (Barnes-Jewish Hospital Oncology Data Services) is approved by the American College of Surgeons. Tumor registrars are certified and responsible for collecting the required data elements for *Division of Oncology, Department of Medicine, Washington University
School of Medicine; †Division of Hematology and Oncology, St. Louis Veterans Affairs Medical Center; and ‡Division of Biostatistics, Wash-ington University School of Medicine, St. Louis, Missouri.
Disclosure: The authors declare no conflict of interest.
Address for correspondence: Ramaswamy Govindan, MD, Division of On-cology, Suite 108, 4960 Childrens’ Place, St. Louis, MO 63110. E-mail: [email protected]
Goodgame D, Morgensztern L, Groove R, Govindan R. Non-small cell lung cancer in the new millennium: the effect of FEG-PET on stage distribu-tion. J Clin Oncol 2006;24(20 Suppl):7205. Presented at the ASCO Annual Meeting Proceedings Part I. Atlanta, Georgia. June 2– 6, 2006. Copyright © 2008 by the International Association for the Study of Lung Cancer
all patients with cancer from review of the medical record. All available records, including but not limited to, clinic charts, inpatient charts, radiology reports, and pathology reports are abstracted into the tumor registry database.
All patients diagnosed with NSCLC were included in this study and were staged according to the updated American Joint Committee on Cancer, 6th edition. Pertinent data were obtained from the tumor registry database and included de-mographic information, date of diagnosis, tumor size, histo-logic subtypes, survival, and record of FDG-PET imaging. Because of the widespread availability of FDG-PET imaging in our institution since 2000, patients were grouped by date of diagnosis, either before or after January 1, 2000. This study was approved by the Human Studies Committee at Washing-ton University School of Medicine. Our hypothesis was that the standard use of FDG-PET would lead to an early detection of metastatic disease, causing a shift in the stage distribution.
All statistical comparisons were performed with the two-sided 2test orttest as appropriate. Survival time was defined as time from the date of initial diagnosis to death of any causes, and those alive were censored at the time of last contact. Overall survival was estimated using the Kaplan-Meier product limit method and compared using logrank test. Apvalue under 0.05 was used to indicate significance and all statistical tests were two-sided.
RESULTS
We identified 6118 consecutive patients between Jan-uary 1, 1990 and December 31, 2005 (Table 1). There were 3756 patients diagnosed before January 1, 2000 (cohort 1) and 2362 thereafter (cohort 2). Final stage was assigned according to pathologic findings in 2305 patients and clini-cally in 3813 patients. Approximately 2% of patients had an unknown stage in both groups.
Significant changes in the demographic patterns in-cluded an increased proportion of females (42– 46%, p ⫽ 0.005) and patients younger than 60 (26 –29%,p⫽0.013). A markedly increased proportion of tumors were identified as non-small cell lung cancer not otherwise specified, (14 –25%, p⬍ 0.001) with a concomitant sharp decrease in squamous cell carcinomas (33–23%) in the more recent cohort of patients.
The use of FDG-PET imaging increased in the late 1990s and was obtained in 19% of patients diagnosed in 1999. We observed a steady increase in the use of FDG-PET since the turn of the century from 28% of patients in 2000 to 46% of patients in 2004 (Figure 1). In total, FDG-PET imaging was performed in 273 patients (7%) in cohort 1 and 799 patients (36%) in cohort 2 (p⬍0.001). FDG-PET was used more commonly in early stage disease, where a change of stage could significantly affect the management, than in locally advanced or known metastatic disease (Figure 2).
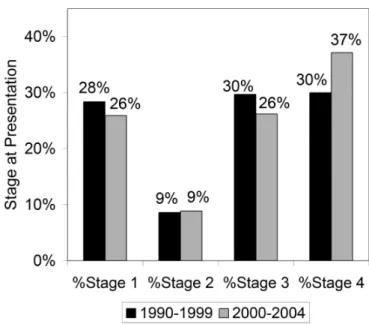
There were significant changes in the distribution of stages I through IV between the two cohorts (p ⬍ 0.001). Patients with stage IV disease at the time of diagnosis increased from 30% in cohort 1 to 37% in cohort 2 (p ⬍ 0.001). This increase in stage IV disease in cohort 2 was
accompanied by a reciprocate decrease in the percentage of patients diagnosed with stage I (29 –25%) and stage III disease (31–27%) (Figure 3).
Because changes in referral patterns to our institution could potentially confound our results (i.e., referrals to med-ical oncology increasing out of proportion to referrals to thoracic surgery), we compared referral rates between de-cades. The proportion of patients diagnosed elsewhere and referred to us for treatment (identified as “referrals”) in-creased after 2000 (26 –38%,p⬍0.001). Although there was a disproportionate increase in the number of referrals for patients with stage IV NSCLC (increased by 12%) compared with all the other stages (increased by 8%), this difference was not statistically significant (p⫽ 0.22). When only pa-tients diagnosed and treated at our institution were analyzed, rates of stage IV disease were still significantly increased after 2000 compared with the previous study period (32– 36%,p⬍0.001).
The overall median survival was 13 months with a 1-year survival of 35%. Although there were no significant changes in overall survival for all stages combined, patients with NSCLC stage IV diagnosed between the years 2000 and TABLE 1. Patient Characteristics by Date of Diagnosis
Variables 1990–1999 2000–2005 p n Percent n Percent Total subjects 3756 61 2362 39 Age at diagnosis 0.005 Median 67 67 Age⬍60 974 26 681 29 Age⬎75 834 22 555 23 Gender 0.005 Male 2164 58 1275 54 Female 1592 42 1087 46 Ethnicity 0.536 White 2870 76 1834 78 Black 848 23 505 21 Stage ⬍0.001 1 1080 29 612 26 2 328 9 209 9 3 1130 30 618 26 4 1142 30 877 37
Clinical staging only 2367 63 1446 61
Unknown 76 2 46 2 Size Median 3.5 3.5 0.995 PET 267 7 865 37 ⬍0.001 Clinical Dx only (no tissue) 169 4 114 5 0.553 Histologic subtype ⬍0.001 Adenocarcinoma 1437 38 912 39 Squamous 1259 34 556 24 Bronchioloalveolar 116 3.1 88 3.7 Other subtypes 274 7.3 107 4.5 NSCLC unspecified 514 13.7 593 25.1
2004 had increased median overall survival (4.5–5.8 months, p ⬍ 0.001) and 1-year survival (21–28%) compared with those diagnosed between 1990 and 1999 (Figure 4). This improvement remained significant after adjusting for age, gender, and histology (p⬍0.0001). There were no difference in survivals between patients with stage IV diagnosed be-tween the years 1990 –1994 and 1995–1999 (p⫽0.114) (data not shown).
Among patients with stage IV disease diagnosed be-tween 2000 and 2004, there was a significant improvement in outcomes for those staged by PET compared with patients without PET, with increased overall median survival (4.5– 8.5
months), 1-year survival (24.8 –38.5%), and 2-year survival rates (9.2–19.9%) (p⬍ 0.0001) (Figure 5A). A similar im-provement was observed in patients with stage III diagnosed in the same period, with increased median overall survival (10.3–22 months), 1-year survival (46 –71%), and 2-year survival (25.9 – 43.8%) (p ⬍ 0.0001) (Figure 5B). The im-provement in survival for stages I and II was small and not statistically significant (data not shown).
DISCUSSION
Data from the National Cancer Data Base including 590,292 patients showed essentially no significant changes in stage distribution between the years 1988 and 1995.5,6During this period, there were no significant advances in imaging modalities for NSCLC staging because, despite improve-ments in CT scan resolution, its accuracy remained essen-tially unchanged.
FDG-PET imaging is a relatively new noninvasive diagnostic technique, which has been used with increased frequency in the diagnosis and staging of lung cancer. Con-ventional anatomic imaging studies frequently lead to under-staging of NSCLC patients and several studies have evaluated the potential benefit from the use of FDG-PET in this setting. A large pooled analysis compared the accuracy of CT imag-ing and FDG-PET imagimag-ing in mediastinal stagimag-ing.7 Among 3438 patients from 18 studies staged with CT scan, sensitivity and specificity of mediastinal lymph node were 57% and 82%, respectively. The addition of FDG-PET improved the sensitivity and specificity to 84% and 89%, respectively. Overall, the prevalence of mediastinal disease increased from 28% in patients staged with CT to 32% in patients staged with PET. Improved accuracy for FDG-PET in mediastinal staging was also observed in a recent meta-analysis of 39 studies, which showed improvements in both median sensitivity (85% FIGURE 1. Rates of FDG-PET imaging at presentation and
rates of stage IV disease for all patients by year of diagnosis.
FIGURE 2. Rates of FDG-PET imaging at presentation, grouped by stage and cohort.
FIGURE 3. Relative distribution of stages of disease at the time of diagnosis, grouped by cohort.
versus 61%) and specificity (90% versus 79%) for this im-aging modality.8
Prospective studies with the use of FDG-PET have shown the detection of unsuspected distant metastases in 11 to 16.5% of patients with newly diagnosed NSCLC, changes in stage in 27 to 62% of patients, and changes in medical management in 25 to 37% of patients.9 –11 As expected, changes in staging were more frequent because of the detec-tion of unsuspected distant lesions.
In one of the largest performed studies,12 FDG-PET was significantly better than CT for the detection of N1 disease (42% versus 13%), mediastinal adenopathy (58% versus 32%), and metastatic disease or second primary ma-lignancy, which were detected in 6.3% of the patients. Over-all, FDG-PET allowed the identification of advanced and unresectable disease (stages IIIA–IV) in 43 of 303 patients (14.2%), thereby avoiding unnecessary thoracotomy. In a recent randomized multicenter trial,13the addition of FDG-PET to standard work-up, improved the selection of
surgi-cally curable patients by decreasing the rate of futile thora-cotomy from 43 to 21%.
Because of the improved accuracy of FDG-PET in the staging of patients with NSCLC, it is likely that the wide-spread use of this imaging technique has caused significant stage migration, although this finding has not been published in any longitudinal, population-based study. The current hos-pital-based cohort study has documented a change in the distribution of stages since the availability of FDG-PET imaging, with an increase in the proportion of stage IV disease and a concomitant decrease in the proportion of stages I and III disease.
We also identified a small but significantly improved survival in patients with stage IV NSCLC treated at our institution since 2000. This improvement may be attributed to the new developments in supportive care and chemotherapy agents, particularly after the proven benefit from second-line therapy14,15 and the introduction of targeted agents such as erlotinib.16 Nevertheless, an alternative explanation is the
FIGURE 4. Overall survival for stage IV NSCLC patients grouped by cohort.
Time to death (years)
Survival Probability 0 1 2 3 4 5 6 0.0 0.2 0.4 0.6 0.8 1.0 A No PET (N=618) PET (N=218) P<0.0001
Time to death (years)
Survival Probability 0 1 2 3 4 5 6 0.0 0.2 0.4 0.6 0.8 1.0 B No PET (N=385) PET (N=207) P<0.0001
FIGURE 5. A, Overall survival for stage IV
pa-tients according to the use of PET.B,Overall
survival for stage III patients according to the use of PET.
“Will Rogers phenomenon,” an apparent paradox obtained when moving an element from one set raises the average values for both the donor and the recipient sets.17With the introduction of new diagnostic procedures, the upstaging of patients with minimal metastatic disease improves the overall prognosis of the donor earlier stages by eliminating those with true metastatic disease. The recipient set, consisting of patients with advanced stage, benefits from the addition of patients with smaller tumor burden, whose prognosis is pre-dictably better than in those with a large volume of disease and easily identified by conventional staging techniques. However, although the prognosis improves within each stage, it does not change for the group as a whole. One would also expect our data to show an improved survival in stages I and III. However, the improvement was small, and not statisti-cally significant. In a recent study, Gauger et al. evaluated the recurrence patterns in patients with clinical stage I NSCLC staged with FDG-PET.18Among the 196 patients, there were 40 (20%) recurrences. The estimated overall survival at 5 years, between 65% and 70%, is modestly improved in comparison with historical controls.19
In a preliminary analysis to evaluate potential stage migration in a larger population, we recently reported the results from a National Cancer Data Base survey in 510,942 NSCLC patients from 1998 to 2003.20 The percentage of stage IV remained relatively constant until the year 2000, when it increased from 35.7 to 38.9%. Subsequent years showed significantly smaller variation and the curve seems to be reaching a plateau, suggesting that an event occurring between the years 2000 and 2001 may be the main factor responsible for the stage migration. This period coincides with the widespread use of PET imaging. Subtle changes in stage may result in increased survival for both early and advanced disease. Caution should be used when comparing results from new studies with historical controls, because improved outcomes may reflect, at least in part, the effects of stage migration.
In summary, we have demonstrated that the introduc-tion of FDG-PET imaging in the staging of NSCLC is associated with a significant change in the stage distribution, with an increased percentage of patients diagnosed with metastatic disease. To our knowledge, this is the first longi-tudinal study addressing this question which has been pub-lished to date.
REFERENCES
1. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2007.CA Cancer J Clin2007;57:43– 66.
2. Govindan R, Page N, Morgensztern D, et al. Changing epidemiology of small-cell lung cancer in the United States over the last 30 years:
analysis of the surveillance, epidemiologic, and end results database.
J Clin Oncol2006;24:4539 – 4544.
3. Pfister DG, Johnson DH, Azzoli CG, et al. American Society of Clinical Oncology treatment of unresectable non-small-cell lung cancer guide-line: update 2003.J Clin Oncol2004;22:330 –353.
4. Knoepp UW, Ravenel JG. CT and PET imaging in non-small cell lung cancer.Crit Rev Oncol Hematol2006;58:15–30.
5. Fry WA, Menck HR, Winchester DP. The National Cancer Data Base report on lung cancer.Cancer1996;77:1947–1955.
6. Fry WA, Phillips JL, Menck HR. Ten-year survey of lung cancer treatment and survival in hospitals in the United States: a national cancer data base report.Cancer1999;86:1867–1876.
7. Toloza EM, Harpole L, McCrory DC. Noninvasive staging of non-small cell lung cancer: a review of the current evidence. Chest 2003;123: 137S–146S.
8. Gould MK, Kuschner WG, Rydzak CE, et al. Test performance of positron emission tomography and computed tomography for mediasti-nal staging in patients with non-small-cell lung cancer: a meta-amediasti-nalysis.
Ann Intern Med2003;139:879 – 892.
9. Bury T, Dowlati A, Paulus P, et al. Whole-body 18FDG positron emission tomography in the staging of non-small cell lung cancer.Eur Respir J1997;10:2529 –2534.
10. Pieterman RM, van Putten JW, Meuzelaar JJ, et al. Preoperative staging of non-small-cell lung cancer with positron-emission tomography.
N Engl J Med2000;343:254 –261.
11. Saunders CA, Dussek JE, O’Doherty MJ, et al. Evaluation of fluorine-18-fluorodeoxyglucose whole body positron emission tomography im-aging in the stim-aging of lung cancer.Ann Thorac Surg1999;67:790 –797. 12. Reed CE, Harpole DH, Posther KE, et al. Results of the American College of Surgeons Oncology Group Z0050 trial: the utility of positron emission tomography in staging potentially operable non-small cell lung cancer.J Thorac Cardiovasc Surg2003;126:1943–1951.
13. van Tinteren H, Hoekstra OS, Smit EF, et al. Effectiveness of positron emission tomography in the preoperative assessment of patients with suspected non-small-cell lung cancer: the PLUS multicentre randomised trial.Lancet2002;359:1388 –1393.
14. Fossella FV, DeVore R, Kerr RN, et al. Randomized phase III trial of docetaxel versus vinorelbine or ifosfamide in patients with advanced non-small-cell lung cancer previously treated with platinum-containing chemotherapy regimens. The TAX 320 Non-Small Cell Lung Cancer Study Group.J Clin Oncol2000;18:2354 –2362.
15. Shepherd FA, Dancey J, Ramlau R, et al. Prospective randomized trial of docetaxel versus best supportive care in patients with non-small-cell lung cancer previously treated with platinum-based chemotherapy.
J Clin Oncol2000;18:2095–2103.
16. Shepherd FA, Rodrigues Pereira J, Ciuleanu T, et al. Erlotinib in previously treated non-small-cell lung cancer.N Engl J Med2005;353: 123–132.
17. Feinstein AR, Sosin DM, Wells CK. The Will Rogers phenomenon. Stage migration and new diagnostic techniques as a source of misleading statistics for survival in cancer.N Engl J Med1985;312: 1604 –1608.
18. Gauger J, Patz EF, Coleman RE, et al. Clinical stage I non-small cell lung cancer including FDG-PET imaging: sites and time to recurrence.
J Thorac Oncol2007;2:499 –505.
19. Mountain CF. Revisions in the international system for staging lung cancer.Chest1997;111:1710 –1717.
20. Morgensztern D, Goodgame B, Chitneni P, et al. Trends in stage distribution for patients with non-small cell lung cancer: a National Cancer Database Survey [Abstract].J Clin Oncol2007;25:7598.