Original Article
Clinical evaluation of hip joint position sense
in patients with hip resurfacing arthroplasty
versus conventional total hip arthroplasty
Cong Wang, Li-Bo Zhu, Hai-Ming Lu, Wei-Lin Sang, Jin-Zhong Ma
Department of Orthopedics, Shanghai First People’s Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 201620, P. R. China
Received April 20, 2016; Accepted July 10, 2016; Epub October 15, 2016; Published October 30, 2016
Abstract: The study aimed to compare the hip joint position sense (JPS) of patients undergoing conventional total hip arthroplasty (THA) or hip resurfacing arthroplasty (HRA). A total of 40 patients who underwent hip arthroplasty (20 THA and 20 HRA) for unilateral coxarthrosis in our department from January 2008 to July 2009 were reviewed. Both groups of patients were matched in age, gender, body-mass index, postoperative rehabilitation and clinical out-comes, and were followed up for > 3 years. The clinical assessments of hip JPS using Active-active method in supine position were performed at preoperatively, postoperative 6, 12, 24 and 36 months. Both groups of patients had similar absolute angle error preoperatively (P = 0.71) and decreased absolute angle error. The THA group had higher mean absolute angle error than that of HRA group at postoperative 6 month and 12 month (both P < 0.01), thereaf-ter, both groups had similar absolute angle error. During the follow up, a tendency towards decreased absolute angle error from 6 month to 36 month was witnessed in both groups. Especially between 6 month and 12 month and between 12 month and 24 month, there were significant differences in absolute angle error (all P < 0.05). After one year, both group of patients had stable absolute angle error (all P > 0.05). Hip JPS after HRA and THA were similar in the long term. In short term, however, HRA was associated with a more improved hip JPS than THA.
Keywords: Arthroplasty, total hip, hip resurfacing, joint position sense
Introduction
In the past, hip replacement is mostly per-formed in elderly sedentary patients, however, in recent years, an increasing number of young and active patients require replacement [1], causing a growing interest for the develop- ment of newer prostheses restoring patient’s anatomy better [2] and physiological loading as well as more durable bearing surfaces [3]. Large diameter metal-on-metal (LDMOM) hip arthroplasty has become an attractive option for the treatment of these younger patients recently [4]. Compared with conventional total hip arthroplasty (THA), the LDMOM hip pros- thesis offers greater range of motion (ROM), more durable bearing surfaces, and lower rate of dislocation [5, 6].
As one of the LDMOM hip arthroplasty, hip resurfacing arthroplasty (HRA) is designed
spe-cifically to meet the high expectations of young
-er and more active patients [7]. Vail et al. reported that both HRA and conventional THA showed improvement in HHS, pain, activity and ROM, and had similar early complication and reoperation rate [8]. However, Pollard et al. found HRA was associated with higher activity, ROM and lower rate of dislocation than THA [9]. The design of large femoral head of HRA makes the prosthetic head must cover more displacement to come out of the cup and dislo-cate [5]. Besides, short-term gait analysis re- search also revealed enhanced postural sta- bility, more symmetric gait pattern, and incre- ased gait speed after HRA [10, 11]. This was supported by the work by Girard et al. who pro-posed that HRA allowed a more anatomical reconstruction of the hip anatomy than conven-tional THA [2].
have been reported. Proprioception, an aware-ness of one’s body and limbs in relation to their surroundings, is determined by the sensation of joint motion (kinesthesia) and joint position sense (JPS) [12]. Joint position sense is the conscious awareness of joint position in space with respect to other parts of the body-the stat-ic aspect of proprioception [13]. As the recov-ery of proprioception is also of great impor-tance for patient’s daily life after hip arthroplas-ty, this study aimed to compare the static aspect of hip proprioception of patients under-going THA or HRA by assessing JPS.
Patients and methods Patients
This study reviewed 40 patients who under-went hip arthroplasty (20 THA and 20 HRA) for unilateral coxarthrosis in our department from January 2008 to July 2009. All the patients were followed up for more than three years. The two groups were matched in age, gender, body-mass index, postoperative rehabilitation and clinical outcomes (Table 1). Any patient who had dislocation or loosening of prosthesis and walking inconvenience was excluded.
For experiments involving human subjects, the study approval was obtained from the institu-tional review board of the ethics committee of
The clinical assessments of hip JPS were per-formed at preoperatively, postoperative 6, 12, 24 and 36 months using Active-active (A-A) method in supine position [14, 15]. This test
evaluated hip flexion in the sagittal plane using
an instrumented spatial linkage (ISL), that is, the ability of patients to reproduce the hip angles actively which were previously
deter-mined actively. Briefly, patients were placed in
a supine position and blindfolded to eliminate visual cues. The test started at neutral position
(0º) and patient actively flexed the hip toward the flexion target position of 45º, which was
indicated by a mechanical obstruction. After holding that position for 5 s, patient focused and remembered the angle, and brought the joint actively back to the neutral starting posi-tion. Then, patient was asked to actively repro-duce the target position without the mechani-cal obstruction and hold at where he/she felt it was the just position. Five repetitions were per-formed for each leg and “absolute angular error” values were obtained from the start and stop angles. The “average absolute angle error”
was finally calculated as the difference between
the patient’s repeat works. Statistical analyses
[image:2.612.88.351.96.163.2]All statistical analyses were performed using SPSS 20.0 (SPSS Inc, Chicago, IL, USA) and P < Table 1. Baseline characteristics and clinical outcomes of
patients undergoing THA and HRA
THA HRA P-value
Mean age, year 48 ± 16.5 46 ± 15.9 0.60
Gender (male/female) 7/13 9/11 0.75
Body mass index 23.6 ± 6.2 21.9 ± 6.1 0.12 Partial weight-bearing walking (d) 3.3 ± 0.57 3.1 ± 0.55 0.27
THA, Total hip arthroplasty; HRA, Hip resurfacing arthroplasty. P < 0.05 was
considered as statistically significant.
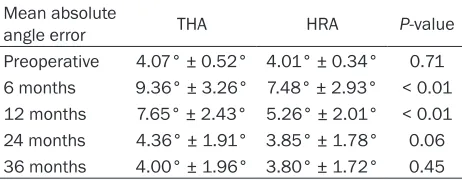
Table 2. Mean absolute angle error of patients under-going THA and HRA
Mean absolute
angle error THA HRA P-value
Preoperative 4.07° ± 0.52° 4.01° ± 0.34° 0.71 6 months 9.36° ± 3.26° 7.48° ± 2.93° < 0.01 12 months 7.65° ± 2.43° 5.26° ± 2.01° < 0.01 24 months 4.36° ± 1.91° 3.85° ± 1.78° 0.06 36 months 4.00° ± 1.96° 3.80° ± 1.72° 0.45
THA, Total hip arthroplasty; HRA, Hip resurfacing arthroplasty. P <
0.05 was considered as statistically significant.
Shanghai First People’s Hospital and the study was performed according to the Declaration of Helsinki. For retrospective study, formal consent is not required.
Each surgery was performed through a posterolateral surgical approach by the same surgical team. In the HRA group, the Durom hip-resurfac-ing system (Zimmer, Warsaw, USA) was implanted according to the instruc-tions provided by the manufacturer. For the THA group, a CLS Spotorno (Zimmer, Warsaw, USA) titanium uncemented femo-ral stem (Zimmer) was used with a 28 mm Metasul femoral head (Zimmer)
articulat-ed with a Metasul bearing insert fittarticulat-ed into
an uncemented acetabular cup (Zimmer, War-saw, USA). All the surgeries and post-operative rehabilitation procedures were standardized.
[image:2.612.91.322.232.322.2]0.05 was considered as statistically significant.
The average absolute angle error between the HRA group and THA group in every follow-up time were compared by multivariate analysis of variance. Comparisons between the respective time points for each group were analyzed with One-way ANOVA.
Results
During the following up, no patient had infec-tion, dislocation or loosening of prosthesis, fra-
ctures around prosthesis, inflammatory pseu -dotumor or walking inconvenience. The JPS test was performed successfully in all the patients. The mean absolute angle error between the HRA group and THA group in every follow-up time are summarized in Table 2. There was no difference in absolute angle error between the two groups preoperatively (P = 0.71). After surgery, both groups of patients had decrea- sed absolute angle error. The THA group had higher mean absolute angle error than that of HRA group at postoperative 6 month and 12 month (both P < 0.01), thereafter, both groups had similar absolute angle error.
During the follow up of 36 months, a tendency towards decreased absolute angle error from 6 month to 36 month was witnessed in both groups. Especially between 6 month and 12 month and between 12 month and 24 month,
there were significant differences in absolute
angle error (all P < 0.05). After one year, both group of patients had stable absolute angle error (all P > 0.05). Patients with typical unilat-eral coxarthrosis were shown in Figures 1, 2.
Discussion
[image:3.612.92.522.72.324.2]Good functional recovery is the ultimate goal of all hip arthroplasty, and as part of the joint function, proprioception following arthroplasty is also of great importance. The performance of the proprioceptive system plays an integral role in maintaining functional joint stability [16], and can be a contributory cause of cartilage lesion [17]. Our study analyzed the static aspect of hip proprioception, as measured by JPS in patients with THA and HRA. The results show- ed that absolute angle error of both groups was decreased within postoperative 12 months and thereafter stable in the following 24 months.
Besides, patients undergoing HRA had lower absolute angle error than that of THA group within 12 months after surgery.
In this study, we chose the supine position to
test the hip flexion in the sagittal plane,
be-cause patients in a supine position would have more supporting and hence focus more on the hip joint. No focus will be necessary to keep balance [15]. The average absolute angle error value was conversely correlated to pro-prioceptive sensibility [18-20]. Larger absolute angle error were witnessed in HRA group than that of THA group in this study at postopera- tive 6 and 12 months but not in the follow- ing months, suggesting that HRA facilitated a greater improvement in JPS than THA in short term. The better biomechanical reconstruction by LDMOM prosthesis system of the HRA might be responsible for the improved JPS, as well
as the faster functional recovery to some extent (not analyzed in this study). However, Larkin et al. reported that total hip resurfacing arthro-plasty did not result in improved proprioception compared with THA [21]. This could be explain-
ed by several reasons: first, the assessment
method was different, as we detected JPS for static proprioception whereas they applied an advanced testing device to objectively quan- tify dynamic postural stability; second, our pa- tients were in supine position whereas their patients were kept in erect position.
Nevertheless, during the long term, HRA and THA didn’t differ in hip JPS as evidenced by the absence of a difference in “error” from 24 to 36 months after surgery. This was supported by previous studies, as reported that, propriocep-tion receptors were located in skin, muscles, and joints [16, 22]. The strength size,
[image:4.612.89.524.73.411.2]ness and joint position, which involved in proprioception, were attributed to the tendon organs of limb and possibly also muscle spin-dles [16, 22, 23]. Therefore, it was presumed that the preservation of the femoral head and neck were not the key for JPS, but the extracap-sular components such as stretch receptors in the adjacent ligament and muscles may mainly
influence hip proprioception.
Several limitations to this study must be addressed. First, the cases of unilateral coxar-throsis patients with THA and HRA were in-
sufficient, and it might affect the statistical
accuracy. Second, JPS in transverse plane and frontal plane were not assessed. Not with standing its limitation, this study did demon-strate that hip JPS after HRA and THA were similar in the long term. In short term, however, HRA was associated with a more improved hip JPS than THA.
Acknowledgements
We would like to acknowledge the editors and reviewers for their valuable comments on this paper. We are also grateful to all the subjects who participated in this study voluntarily.
Disclosure of conflict of interest
None.
Address correspondence to: Dr. Jin-Zhong Ma, De- partment of Orthopedics, Shanghai First People’s Hospital, Shanghai Jiao Tong University School of Medicine, NO. 650, New Songjiang Road, Shang- hai 201620, P. R. China. Tel: +86-021-37798591; Fax: +86-021-37798631; E-mail: majinzhong007@ 126.com
References
[1] Crowninshield RD, Rosenberg AG and Sporer SM. Changing demographics of patients with total joint replacement. Clin Orthop Relat Res 2006; 443: 266-272.
[2] Girard J, Lavigne M, Vendittoli PA and Roy A. Biomechanical reconstruction of the hip a ran-domised study comparing total hip resurfacing and total hip arthroplasty. J Bone Joint Surg Bri Volume 2006; 88: 721-726.
[3] Harris WH and Muratoglu OK. A review of cur-rent cross-linked polyethylenes used in total joint arthroplasty. Clin Orthop Relat Res 2005; 430: 46-52.
[4] Jack CM, Walter WL, Shimmin AJ, Cashman K and de Steiger RN. Large diameter metal on metal articulations. Comparison of total hip ar-throplasty and hip resurfacing arar-throplasty. J Arthroplasty 2013; 28: 650-653.
[5] Mertl P, Boughebri O, Havet E, Triclot P, Lardanchet JF and Gabrion A. Large diameter head metal-on-metal bearings total hip arthro-plasty: preliminary results. Orthop Traumatol Surg Res 2010; 96: 14-20.
[6] Cicek H, Kilicarslan K, Yalcin N, Arslan E, Dogramaci Y and Yildirim H. Primary metal-on-metal total hip arthroplasty with large-diame-ter femoral heads: A clinical trial of 59 hips. Acta Orthop Belg 2010; 76: 758.
[7] Costa ML, Achten J, Parsons NR, Edlin RP, Foguet P, Prakash U and Griffin DR. Total hip arthroplasty versus resurfacing arthroplasty in the treatment of patients with arthritis of the hip joint: single centre, parallel group, asses-sor blinded, randomised controlled trial. BMJ 2012; 344: e2147.
[8] Vail TP, Mina CA, Yergler JD and Pietrobon R. Metal-on-metal hip resurfacing compares fa-vorably with THA at 2 years followup. Clin Orthop Relat Res 2006; 453: 123-131. [9] Pollard T, Baker R, Eastaugh-Waring S and
Bannister G. Treatment of the young active pa-tient with osteoarthritis of the hip a five-to sev -en-year comparison of hybrid total hip arthro-plasty and metal-on-metal resurfacing. J Bone Joint Surg Br 2006; 88: 592-600.
[10] Nantel J, Termoz N, Centomo H, Lavigne M, Vendittoli PA and Prince F. Postural balance during quiet standing in patients with total hip arthroplasty and surface replacement arthro-plasty. Clin Biomech (Bristol, Avon) 2008; 23: 402-407.
[11] Mont MA, Seyler TM, Ragland PS, Starr R, Erhart J and Bhave A. Gait analysis of patients with resurfacing hip arthroplasty compared with hip osteoarthritis and standard total hip arthroplasty. J Arthroplasty 2007; 22: 100-108.
[12] Anderson E and Max E. Barefoot Training and its Effects on Balance, Proprioception, and Stability in Adults 65 and Older. 2012. [13] Jerosch J and Prymka M. Proprioception and
joint stability. Knee Surg Sports Traumatol Arthrosc 1996; 4: 171-179.
[14] Sahin N, Baskent A, Cakmak A, Salli A, Ugurlu H and Berker E. Evaluation of knee propriocep-tion and effects of proprioceppropriocep-tion exercise in patients with benign joint hypermobility syn-drome. Rheumatol Int 2008; 28: 995-1000. [15] Benjaminse A, Sell TC, Abt JP, House AJ and
[16] Moraes MR, Cavalcante ML, Leite JA, Macedo JN, Sampaio ML, Jamacaru VF and Santana MG. The characteristics of the mechanorecep-tors of the hip with arthrosis. J Orthop Surg Res 2011; 6: 58.
[17] Barrett D, Cobb A and Bentley G. Joint proprio-ception in normal, osteoarthritic and replaced knees. J Bone Joint Surg Br 1991; 73: 53-56. [18] Petrella RJ, Lattanzio PJ, Nelson MG. Effect of
age and activity on knee joint proprioception. Am J Phys Med Rehabil 1997; 76: 235-241. [19] Marks R, Quinney H and Wessel J. Proprio-
ceptive sensibility in women with normal and osteoarthritic knee joints. Clin Rheumatol 1993; 12: 170-175.
[20] Lattanizio PJ, Petrella RJ, Sproule JR and Fowler PJ. Effects of fatigue on knee proprio-ception. Clin J Sport Med 1997; 7: 22-27.
[21] Larkin B, Nyazee H, Motley J, Nunley RM, Clohisy JC and Barrack RL. Hip Resurfacing Does Not Improve Proprioception Compared With THA. Clin Orthop Relat Res 2014; 472: 555-561.
[22] Proske U and Gandevia SC. The propriocep- tive senses: their roles in signaling body sha- pe, body position and movement, and muscle force. Physiol Rev 2012; 92: 1651-1697. [23] Isaac S, Barker K, Danial I, Beard D, Dodd C