and B HIV-2 RNA Load
Véronique Avettand-Fenoel,a,bFlorence Damond,c,d,eMarie Gueudin,f,gSophie Matheron,c,d,hAdeline Mélard,bGilles Collin,c,d,e Diane Descamps,c,d,eMarie-Laure Chaix,iChristine Rouzioux,a,b Jean-Christophe Plantier,f,gfor the CO5 HIV-2 and the ANRS-AC11 Quantification Working Group
Laboratoire de Virologie, AP-HP, Hôpital Necker Enfants Malades, Paris, Francea
; EA7327, Université Paris-Descartes, Sorbonne Paris Cité, Faculté de Médecine, Paris, Franceb
; INSERM, IAME, UMR 1137, Paris, Francec
; Université Paris Diderot, Sorbonne Paris Cité, Paris, Franced
; AP-HP, Hôpital Bichat-Claude Bernard, Laboratoire de Virologie, Paris, Francee
; Laboratoire de Virologie Associé au Centre National de Référence du VIH, Hôpital Charles Nicolle, CHU de Rouen, Rouen, Francef
; GRAM, Equipe d’Accueil 2656, Faculté de Médecine-Pharmacie, Institut de Recherche et d’Innovation en Biomédecine, Université de Rouen, Rouen, Franceg
; AP-HP, Hôpital Bichat-Claude Bernard, Service de Maladies Infectieuses et Tropicales, Paris, Franceh
; Laboratoire de Virologie, AP-HP, Hôpital Saint-Louis, Paris, Francei
The Agence Nationale de Recherche sur le Sida et les hépatites virales (ANRS) previously developed a widely used method for HIV-1 RNA quantification (Biocentric). Here, we report the development of a new specific and sensitive method for HIV-2 RNA quantification, based on an adaptation of the existing HIV-1 protocol. The new test is based on TaqMan one-step reverse tran-scription-quantitative PCR (qRT-PCR) targeting two conserved consensus regions of HIV-2 (long terminal repeat [LTR] and gag). Analytic performances were determined in three laboratories. Clinical performances were evaluated on 100 plasma samples from HIV-2-infected patients (groups A, B, and H) by comparison with the assay currently used for the ANRS HIV-2 cohort. The specificity was 100%. Sensitivity was 50 copies/ml (cp/ml) and was optimized to 10 cp/ml. The within-run coefficients of varia-tion in the three laboratories varied from 0.54% to 1.61% at 4 log10copies/ml and from 7.24% to 14.32% at 2 log10cp/ml. The between-run coefficients of variation varied from 2.28% to 6.43%. Of the 39 clinical samples below 2 log10in the current assay, the new test improved the detection or quantification of 17 samples, including eight group B samples. For quantifiable samples, similar loads were obtained with the two assays for group A samples. The median difference between the two assays for group B samples wasⴙ0.18 but with greater heterogeneity than for group A. The HIV-2 group H sample had similar results with the two assays. This new assay is highly sensitive and accurately quantifies the most prevalent HIV-2 groups. This test will be useful for monitoring low viral loads in HIV-2-infected patients.
H
IV-2 is characterized by less efficient transmission through the sexual and vertical routes than HIV-1 (1,2) and by a slower natural clinical course (2–4); nevertheless, HIV-2 infection eventually leads to AIDS. HIV-2 infection must be distinguished from HIV-1 infection, as HIV-2 is naturally resistant to non-nucleoside reverse transcriptase inhibitors, T20, and some pro-tease inhibitors, and as patient follow-up differs from that of HIV-1 infection (5,6).Compared to HIV-1, HIV-2 is characterized by lower viral rep-lication (4, 7–10). In the French National HIV-2 Cohort (974 patients in June 2013), 61% of untreated patients had plasma viral loads below 250 copies/ml (cp/ml). Likewise, in a British study, only 8% of patients with CD4 of⬎500 cells/mm3and 62% of patients with CD4 of⬍300 cells/mm3had detectable viral loads (11), implying that 38% of patients had undetectable viral loads in an assay with a quantification limit of 100 copies/ml.
Clinical management of HIV-2 infection is hampered by the lack of validated commercial RNA viral load assays. In-house as-says are therefore widely used (12–18). The ACHIEV2E interna-tional collaboration on HIV-2 infection showed that plasma HIV-2 RNA values vary considerably between laboratories (19,
20). The high genetic diversity of HIV-2, with 9 groups designated A to I, of which only groups A and B are epidemic, also represents an obstacle to accurate viral load quantification (21–25). Previous studies showed that group B viruses are particularly difficult to quantify (13,19,20).
As most cases of HIV-2 infection occur in resource-limited settings, an affordable test is urgently needed, particularly to
iden-tify HIV-1/HIV-2 coinfection. The Agence Nationale de Recher-che sur le Sida et les hépatites virales (ANRS) has previously pro-moted the development of an HIV-1 RNA assay, which is now marketed by Biocentric (Bandol, France) and is widely used in resource-limited settings (26,27). This test is easy to perform and affordable, and it has been proven to be useful for patient moni-toring.
The aim of the present work was to develop a new sensitive method for quantifying HIV-2 RNA, particularly that of epidemic groups A and B. It is based on a one-step real-time duplex PCR method using the same amplification protocol as the Biocentric generic HIV-1 charge virale assay. The new test was compared with the HIV-2 assay currently used for the French HIV-2 cohort and was validated by three laboratories belonging to the ANRS AC11 quantification working group.
Received14 March 2014Returned for modification17 April 2014
Accepted5 June 2014
Published ahead of print11 June 2014
Editor:Y.-W. Tang
Address correspondence to Jean-Christophe Plantier, [email protected].
V.A.-F. and F.D. contributed equally to this article.
Copyright © 2014, American Society for Microbiology. All Rights Reserved.
doi:10.1128/JCM.00724-14
on May 16, 2020 by guest
http://jcm.asm.org/
MATERIALS AND METHODS
The new HIV-2 RNA assay.The new test is based on a one-step duplex TaqMan PCR approach targeting a conserved consensus region in the long terminal repeat (LTR) region and thegagregion. The forward and reverse primers for the LTR region are 5=-TCTTTAAGCAAGCAAGCGT GG-3= and 5=-AGCAGGTAGAGCCTGGGTGTT-3=, respectively (28), with a new internal probe (5= -FAM-CTTGGCCGGYRCTGGGCAGA-BHQ1-3=[FAM, carboxyfluorescein; BHQ1, black hole quencher 1]) to optimize efficiency for HIV-2 group B. The forward and reverse primers for thegagregion are F3 (5=-GCGCGAGAAACTCCGTCTTG-3=) and R1 (5=-TTCGCTGCCCACACAATATGTT-3=), respectively (13), and the in-ternal HIV-2 TaqMangagprobe is S65GAG2 (5=-FAM-TAGGTTACGG CCCGGCGGAAAGA-BHQ1-3=(Eurogentec, Seraing, Belgium) (13).
RNA was extracted from 200l of plasma by using the QIAamp viral RNA minikit (Qiagen, Courtaboeuf, France), as in the Biocentric generic HIV-1 charge virale assay, in labs A and B (Necker Hospital, Paris, and Charles Nicolle Hospital, Rouen) or 1 ml with the total nucleic acid (NA) large-volume MagNA Pure kit (Roche Automated System, Meylan, France) in lab C (Bichat Claude Bernard Hospital, Paris).
The reaction mix consists of a 20-l volume containing the RNA ex-tract (10l), primers (500 nM each), probes (250 nM each), and 1⫻PCR buffer (4⫻one-step mix; Invitrogen, Cergy-Pontoise, France).
The thermocycling conditions are those used for the Biocentric HIV-1 assay (10 min at 50°C and 5 min at 95°C, followed by 50 cycles of 95°C for 15 s and 60°C for 1 min). Amplification and data acquisition were carried out with the TaqMan ABI real-time PCR system (Applied Biosystems, Courtaboeuf, France). The log10number of targets initially present is
proportional to the cycle threshold (CT) and is determined from the stan-dard curve.
A BIOQ HIV-2 RNA group A quantification panel (P0182; Rijswijk, the Netherlands) was used as the external standard. The standard, evaluated at 2.93⫻106cp/ml, was first diluted in RPMI culture medium to a theoretical
concentration of 1,000,000 cp/ml (2,400,000 IU/ml), followed by serial 10-fold dilutions to concentrations ranging from 1,000,000 (5 log10) to 100 cp/ml
(2 log10), and a final dilution to 40 cp/ml (1.6 log10).
Determination of the analytic performance of the new assay. Speci-ficity was determined by testing plasma samples from 49 HIV-negative subjects and 30 HIV-1 group M-positive patients with viral loads ranging from⬎20 to⬍10,000,000 cp/ml. Nine HIV-1 group O coculture super-natants were also tested.
Linearity was assessed using the BIOQ external standard diluted in RPMI to 1,000,000, 100,000, 10,000, 1,000, 100, and 40 cp/ml (each tested in 10 runs at lab A).
Analytical sensitivity was determined by dilution in RPMI of the BIOQ external standard to 100, 50, 40, 20, and 10 cp/ml (10 replicates each).
To determine within-run reproducibility, the BIOQ external standard was tested at concentrations of 10,000 and 100 cp/ml in each of the three laboratories (10 replicates for each dilution).
To determine between-run reproducibility, an HIV-2-positive control was prepared by serial dilution in HIV-negative EDTA human plasma of a coculture supernatant of an HIV-2 group A isolate (GenBank accession numberAY688870). This solution was diluted to obtain aliquots with theoretical concentrations ranging from 10,000 to 100,000 cp/ml in the current assay. These aliquots were each tested once in 7 separate runs with the MagNA Pure automated extraction system (lab C) and in, respec-tively, 18 and 7 separate runs with Qiagen manual extraction at labs A and B.
Statistical analysis.MedCalc software (Ostend, Belgium) was used for data analysis. Bland and Altman curves were used to represent the degree of agreement between the two techniques (29). Thexaxis bore the mean values for each sample obtained with the two techniques, and theyaxis the difference between the values obtained with the two techniques.
Disagreement between the two techniques was defined as a difference of⬎0.5 log10for a given sample.
Clinical samples.One hundred plasma samples from HIV-2-infected patients (n⫽100) included in the French National HIV-2 Cohort (ANRS CO5) were selected according to the viral genotype and the HIV-2 RNA concentration, as determined with our current in-house technique (13). Among these patients, 51% were treated by antiretrovirals. The HIV-2 group was determined for 89 samples, as previously described (22,30). Thirty-eight samples were group A, 50 group B, and 1 group H. Genotyp-ing was not available for the remainGenotyp-ing 11 samples, owGenotyp-ing to the absence of detectable viral RNA and a lack of whole blood or mononuclear cells for viral DNA testing.
The selected samples had the following characteristics:⬍100 (2 log10)
cp/ml (n⫽39; 9 group A and 19 group B, 11 nongenotypable), 100 (2 log10) to 1,000 (3 log10) cp/ml (n⫽16; 5 A and 11 B), 1,000 (3 log10) to
10,000 (4 log10) (n⫽22; 12 A and 10 B), 10,000 (4 log10) to 100,000
(5 log10) (n⫽19; 11 A, 7 B, and 1 H) and⬎100,000 (5 log10) (n⫽4; 1 A and 3B).
RESULTS
Analytic performances of the new assay.As expected, given the wide genomic divergence between HIV-1 and HIV-2, the HIV-2 primers did not hybridize to HIV-1 genes. All HIV-1-positive plasma samples and all HIV-negative samples were negative in the new assay, giving a specificity of 100%.
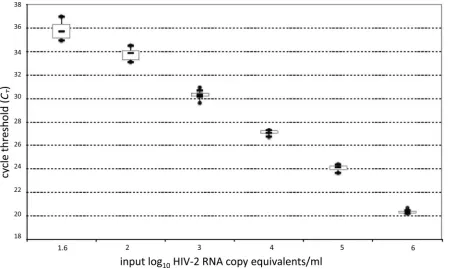
The standard curve showed a strong linear relationship be-tween theCTvalues and log10HIV-2 RNA cp/ml (Fig. 1). The median correlation coefficient was 0.9947 (range, 0.9831 to 0.9997), and the median slope was ⫺3.37 (range, ⫺3.16 to
⫺3.62).
The analytical sensitivity of the assay was 100% at 40 cp/ml (1.6 log10cp/ml) and 90% at 20 cp/ml (1.3 log10cp/ml) after Roche MagNA Pure automated extraction of 1 ml and 100% at 50 cp/ml (1.7 log10cp/ml) after manual extraction of 200l. Optimization of the assay sensitivity after manual extraction was evaluated using 1 ml of plasma. The sample was centrifuged at 17,000 rpm and the pellet was resuspended in 200l of RPMI medium prior to man-ual extraction as previously described, with elution in 60l. This yielded 90% sensitivity at 10 cp/ml (1 log10cp/ml).
Within-run reproducibility was evaluated in the three labs by using the BIOQ external standard with theoretical virus concen-trations of 10,000 and 100 cp/ml (4 and 2 log10cp/ml). For the 4 log10cp/ml value, we obtained a mean of 3.91 log10cp/ml at lab C, 4.1 log10cp/ml at lab A, and 4.2 log10cp/ml at lab B, with within-run coefficients of variation of 1.61%, 0.54%, and 1.10%, respec-tively. At the concentration of 2 log10cp/ml, we obtained mean values of 2.03 log10cp/ml at lab B, 2.07 log10cp/ml at lab A, and 2.17 log10cp/ml at lab C, with within-run coefficients of variation of 10.72%, 14.32%, and 7.24%, respectively.
In between-run assays, the positive control with a theoretical concentration between 10,000 (4 log10) and 100,000 cp/ml (5 log10) was evaluated at 4.61 log10cp/ml in lab C, 4.70 log10cp/ml in lab A, and 4.88 log10cp/ml in lab B, with coefficients of variation of 2.28%, 6.43%, and 3.03%, respectively.
Clinical performances.The clinical performances of the new assay were evaluated in lab C. Clinical samples of 1 ml were ex-tracted with the automated MagNA Pure method, and then the same eluate was used to perform the two assays in parallel with the ABI device for the new assay and the Light Cycler 1.5 device for the current assay. The results obtained with the new assay were categorized into four groups (Table 1), undetectable (⬍40 cp/ml), detectable but not quantifiable (0 to⬍40 cp/ml), quantifiable
on May 16, 2020 by guest
http://jcm.asm.org/
tween 40 and 100 cp/ml, and above the lower limit of quantifica-tion of the current assay (100 cp/ml).
Of the 39 samples below the quantification limit of 100 cp/ml in the current assay, 22 samples (56%) were also undetectable with the new assay (Table 1), while 10 samples (26%; 3 A, 3 B, and 4 nongenotypable) were detected at values between 0 and 40 cp/ml (range, 1 to 36 cp/ml). Three samples (7.7%; 1 B and 2 nongeno-typable) were quantified between 40 and 100 cp/ml (range, 56 to 79 cp/ml), and four samples (10%; all B) were quantified above 100 cp/ml (range, 102 to 970 cp/ml). The latter corresponded to true false-negative samples, taking into account the 100 cp/ml cutoff the current assay. These results showed that the new test improved the detection or quantification of 17/39 samples (43.6%), including eight group B samples (Table 1).
All 61 plasma samples with values above 100 cp/ml in the cur-rent assay were detectable with the new test. One sample at 209
cp/ml (2.32 log10cp/ml) in the current assay gave a value of 46 cp/ml (1.69 log10cp/ml) in the new test (Table 1).
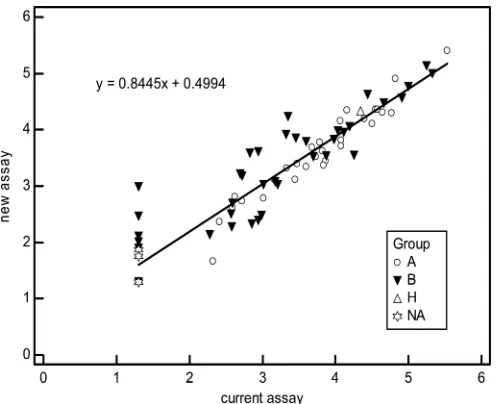
A scatter plot was constructed with the values obtained for the 78 samples detectable or quantifiable with the new assay (Fig. 2). It showed a wider dispersion of values for quantifiable group B sam-ples than for quantifiable group A samsam-ples, as well as better detec-tion or quantificadetec-tion of group B and nongenotypable samples. This was confirmed by scatter equations specific for group A sam-ples (n⫽32;y⫽0.9485x⫹0.0294;r2⫽0.9619) and group B samples (n⫽39;y⫽0.7766x⫹0.8087;r2⫽0.8184) and also by Bland-Altman representations (Fig. 3). Homogeneous quantifica-tion (⫾1.96 standard deviation [SD], range from⫺0.6 to 0.35) and similar values (median difference of⫺0.13) were obtained with the new and current assays for group A samples. The median difference between the two assays for group B samples was⫹0.18, but with greater heterogeneity (⫾1.96 SD, range⫺0.98 to 1.33).
FIG 1Standard curve of the HIV-2 RNA real-time viral load assay. The cycle threshold (CT) is the number of cycles at which fluorescence passes a fixed limit
[image:3.585.70.519.66.335.2](time to positivity). Median values and 25% and 75% interquartile ranges (box plot) of theCTare indicated. The vertical lines show the ranges of theCT.
TABLE 1Clinical performance of the new assay using automated extraction (MagNA Pure plus ABI prism) compared to that of the current assay (MagNA Pure plus Light Cycler method)
VLa(cp/ml) with new
version of HIV-2 assay
No. of samples tested by current version of HIV-2 assay per indicated group at a VL (cp/ml) of:
⬍100 cp/ml (2 log) (n⫽39) ⱖ100 cp/ml (2 log) (n⫽61) Group A
(n⫽9)
Group B (n⫽19)
NAb
(n⫽11)
Group A (n⫽29)
Group B (n⫽31)
Group H (n⫽1)
⬍40 cp/ml (1.7 log) 6 11 5
0 to⬍40 cp/ml 3 3 4
40ⱕVL⬍100 cp/ml 1 2 1
ⱖ100 cp/ml (2 log) 4 28 31 1
a
VL, viral load.
bNA, nongenotypeable samples.
on May 16, 2020 by guest
http://jcm.asm.org/
[image:3.585.44.541.611.707.2]Among the samples that were quantifiable with both assays, 10 samples showed differences above 0.5 log10, 9 of them belonging to group B. Five of these samples were better quantified with the new assay (differences of 0.53, 0.60, 0.68, 0.76, and 0.89 log10/ml) and five with the current assay (differences of 0.51, 0.52, 0.55, 0.66, and 0.70 log10/ml). These differences illustrate the difficulty of correctly assessing HIV-2 group B viral load.
The only HIV-2 group H sample gave very similar results with the two assays (4.33 log10and 4.34 log10).
DISCUSSION
HIV-2 infection differs markedly from HIV-1 infection, notably by its slower natural course, different therapeutic management, and genetic diversity. Specific molecular methods are therefore necessary for diagnosis and patient monitoring. Current assays, mainly consisting of in-house methods or unvalidated deriva-tives of commercial kits, suffer from major limitations in terms of their sensitivity, accuracy, and coverage of HIV-2 genetic diversity (19,20).
The aim of this work was to develop a quantitative assay that takes into account both the low viral load seen in most HIV-2-infected patients and the broad genetic diversity of HIV-2, espe-cially group B (13,19,20). In addition, as most cases of HIV-2 infection occur in West Africa, such a test must be easy to imple-ment in developing countries, as previously achieved with the ge-neric HIV-1 viral load assay marketed by Biocentric.
We chose to optimize the assay currently used to monitor the French HIV-2 cohort based on amplification of the HIV-2gag region, which gave accurate results in the ACHIEV2Estudy (19, 20), but with a lower limit of quantification of 100 cp/ml (13) and not completely adapted to some group B strains. We also used the same operating conditions as those of the Biocentric HIV-1 assay kit, in order to facilitate its use either for HIV-2 alone or jointly for HIV-1 and HIV-2.
The new test exhibits good linearity (40 to 1,000,000 cp/ml)
and within-run reproducibility (⬍15%). Its interlaboratory re-producibility was validated by evaluation at three different sites. Both manual and automated extraction methods were validated for compatibility with local practices in resource-limited coun-tries.
Relative to the current assay, the new test has a significantly better analytical limit of quantification, reaching 50 cp/ml with manual extraction of 200l of plasma and 40 cp/ml with auto-mated extraction of 1 ml. Assuming a probit rate of 90%, the detection limits with 1 ml of plasma would be 10 cp/ml and 20 cp/ml, respectively. This very good analytical sensitivity matches that of recently published in-house methods (12,14,18) and is compatible with virological monitoring of HIV-2 infection, as
⬎60% of untreated patients have viral loads below 250 cp/ml. The new test detected and/or quantified more than one-third of sam-ples that were undetectable with our current assay, which has a quantification limit of 100 cp/ml. This excellent sensitivity should prove useful both for pathophysiological studies and for treat-ment monitoring.
FIG 2Scatter diagram according to the genetic group of the 78 samples de-tectable (0 to⬍40 cp/ml) and quantifiable (ⱖ40 cp/ml) with the new assay (r2⫽0.8886). An arbitrary value of 20 cp/ml (1.3 log) was attributed to
sam-ples undetectable in the current assay, and to those detectable in the new assay (0 to⬍40 cp/ml). NA, nongenotypable samples.
HIV-2 group B (39 samples)
1 2 3 4 5 6 7
-1.5 -1.0 -0.5 0.0 0.5 1.0 1.5 2.0
Mean of new assay and current assay
new assay
-c
u
rr
ent
assa
y
Mean
0.18
-1.96 SD -0.98 +1.96 SD 1.33
HIV-2 group A (32 samples)
1 2 3 4 5 6 7
-1.5 -1.0 -0.5 0.0 0.5 1.0 1.5 2.0
Mean of new assay and current assay
n
e
w
as
s
a
y
-c
urrent
as
s
a
y
Mean -0.13 -1.96 SD -0.60 +1.96 SD 0.35
FIG 3Degree of agreement in log10cp/ml between the new and current assays;
Bland and Altman curves for group A (top) (n⫽32) and group B (bottom) (n⫽39) samples detectable (0 to⬍40 cp/ml) and quantifiable (ⱖ40 cp/ml) with the new assay. An arbitrary value of 10 cp/ml was attributed to samples undetectable with the current assay, and 20 cp/ml to those detectable with the new assay (0 to⬍40 cp/ml).
on May 16, 2020 by guest
http://jcm.asm.org/
[image:4.585.300.543.63.439.2] [image:4.585.40.288.65.267.2]The most difficult issue facing the development of HIV-2 viral load assays is the genetic diversity of this virus (especially group B), with some variants being underquantified or escaping detec-tion with current tests (13,19,20). Three teams recently reported improved sensitivity for HIV-2, but they mainly used superna-tants (14) or a limited number of samples (12,18) or validated detection but not quantification (18), leaving questions as to their clinical performance, especially for group B viruses. We evaluated our new assay on 100 clinical samples, 39% of which were unde-tectable with our current assay, representative of the molecular epidemiology of groups A and B, plus the only one divergent sam-ple of group H. Half the samsam-ples corresponded to group B, and more than one-third of them (n⫽19) were undetectable with our current assay. We chose to develop a duplex method capable of simultaneously amplifying the LTR andgagregions, in order to retain the benefits of each previous test and to improve the detec-tion of group B viruses by reducing the risk of mismatches. Our strategy, based on coupling of primers and probes in two distinct regions of the viral genome, has already been adopted by Roche in version 2.0 of its CAP CTM HIV-1 assay, resulting in better quan-tification of HIV-1 non-B subtypes (31). The new and current HIV-2 assay methods gave similar results for the single group H sample and for the group A samples (although 3 additional group A samples were detectable with the new test), whereas the new test developed by Delarue et al. gave values nearly 0.5 log10lower than their reference test (14). Eight additional group B samples (42%) were detected or quantified with our new test, four samples having values of 102 to 970 cp/ml. This improvement is due to the addi-tion of primers in the LTR region and to changes in the LTR probe (data not shown). However, the wider dispersion of values and the larger number of group B than group A samples with differences exceeding 0.5 log10 relative to the current assay illustrate the greater difficulty of group B quantification. In addition, six non-genotypable samples were better detected or quantified with our new assay.
We designed the new test for use under the same operating conditions as the generic HIV-1 RNA assay currently used with success in many resource-limited countries (26,27), meaning it could be used on the same machine, with the same software pro-gram and even, if necessary, in the same amplification plate, as HIV-1 samples. This will reduce analytical costs by increasing the number of samples per run.
Although ours is an in-house assay, its performance is adequate for patient monitoring in the absence of a validated commercial test. In addition, the use of a standardized kit that includes an external standard will improve interlaboratory reliability, as shown by the 2nd International ACHIEV2Estudy (19,20).
The analytical performance of our new assay is similar to that of other newly developed tests (12,14,18). However, it is difficult to compare our method with the test described by Chang et al., adapted from the Abbott platform (Abbott Molecular, Chicago, IL), as the latter was evaluated on few group B samples and was not compared with other techniques (12). Styer et al. recently com-pared their method with this “Abbott” technique and observed a difference of⫺0.35 log10UI/ml, but they used a limited panel of uncharacterized samples, ruling out any evaluation of in terms of genetic diversity (18). Finally, Delarue et al. (14) and Styer et al. (18) used two-step methods, whereas our assay is performed in a single step.
In conclusion, we have developed and standardized an assay
with better analytical sensitivity than the technique currently used to monitor HIV-2-infected patients in France. Our assay also has improved clinical sensitivity and has been validated on a broad, well-characterized sample panel, unlike other recently published tests (12,14,18). The analytical performance of this new assay, which is easy to perform, makes it suitable for use in resource-limited countries in which multiple HIV-2 variants circulate. In addition, our assay can be used on the same analytical platforms and in the same run as tests for HIV-1, thus improving its cost-efficiency for monitoring patients infected with HIV-1 and/or HIV-2. This possibility of simultaneous analysis will facilitate mo-lecular diagnosis of mother-to-child transmission of HIV-1 and/or HIV-2, and also diagnosis and follow-up of dual HIV-1/ HIV-2 infection in the same sample. Finally, use of this assay for virological monitoring will provide new insights into the natural history of HIV-2 infection at different clinical stages.
ACKNOWLEDGMENTS
This work was supported by the Agence Nationale de Recherche sur le Sida et les hépatites virales (ANRS). We also thank the HIV-2 cohort (ANRS CO5), which is supported by a grant from ANRS.
REFERENCES
1.Andreasson PA, Dias F, Naucler A, Andersson S, Biberfeld G.1993. A prospective study of vertical transmission of HIV-2 in Bissau, Guinea-Bissau. AIDS.7:989 –993.http://dx.doi.org/10.1097/00002030 -199307000-00013.
2.Kanki PJ, Travers KU, MBoup S, Hsieh CC, Marlink RG, Gueye-NDiaye A, Siby T, Thior I, Hernandez-Avila M, Sankale JL, Ndoye I, Essex ME.1994. Slower heterosexual spread of HIV-2 than HIV-1. Lancet
343:943–946.http://dx.doi.org/10.1016/S0140-6736(94)90065-5. 3.Marlink R.1996. Lessons from the second AIDS virus, HIV-2. AIDS.
10:689 – 699.
4.Whittle H, Morris J, Todd J, Corrah T, Sabally S, Bangali J, Ngom PT, Rolfe M, Wilkins A.1994. HIV-2-infected patients survive longer than HIV-1-infected patients. AIDS 8:1617–1620.http://dx.doi.org/10.1097 /00002030-199411000-00015.
5.Desbois D, Roquebert B, Peytavin G, Damond F, Collin G, Benard A, Campa P, Matheron S, Chene G, Brun-Vezinet F, Descamps D.2008.In vitrophenotypic susceptibility of human immunodeficiency virus type 2 clinical isolates to protease inhibitors. Antimicrob. Agents Chemother.
52:1545–1548.http://dx.doi.org/10.1128/AAC.01284-07.
6.Witvrouw M, Pannecouque C, Switzer WM, Folks TM, De Clercq E, Heneine W. 2004. Susceptibility of HIV-2, SIV and SHIV to various anti-HIV-1 compounds: implications for treatment and postexposure prophylaxis. Antivir. Ther.9:57– 65.
7.Marlink R, Kanki P, Thior I, Travers K, Eisen G, Siby T, Traore I, Hsieh CC, Dia MC, Gueye EH, Hellinger J, Gueye-Ndiaye A, Sankale JL, Ndoye I, Mboup S, Essex ME.1994. Reduced rate of disease development after HIV-2 infection as compared to HIV-1. Science265:1587–1590.
http://dx.doi.org/10.1126/science.7915856.
8.Matheron S, Mendoza-Sassi G, Simon F, Olivares R, Coulaud JP, Brun-Vezinet F.1997. HIV-1 and HIV-2 AIDS in African patients living in Paris. AIDS11:934 –936.
9.Nunn AJ, Mulder DW, Kamali A, Ruberantwari A, Kengeya-Kayondo JF, Whitworth J.1997. Mortality associated with HIV-1 infection over five years in a rural Ugandan population: cohort study. BMJ315:767–771.
http://dx.doi.org/10.1136/bmj.315.7111.767.
10. Poulsen AG, Aaby P, Larsen O, Jensen H, Naucler A, Lisse IM, Chris-tiansen CB, Dias F, Melbye M.1997. 9-year HIV-2-associated mortality in an urban community in Bissau, west Africa. Lancet349:911–914.http: //dx.doi.org/10.1016/S0140-6736(96)04402-9.
11. Smith NA, Shaw T, Berry N, Vella C, Okorafor L, Taylor D, Ainsworth J, Choudhury A, Daniels RS, El-Gadi S, Fakoya A, Moyle G, Oxford J, Tedder R, O’Shea S, de Ruiter A, Breuer J.2001. Antiretroviral therapy for HIV-2-infected patients. J. Infect.42:126 –133.http://dx.doi.org/10 .1053/jinf.2001.0792.
12. Chang M, Gottlieb GS, Dragavon JA, Cherne SL, Kenney DL, Hawes
on May 16, 2020 by guest
http://jcm.asm.org/
SE, Smith RA, Kiviat NB, Sow PS, Coombs RW.2012. Validation for clinical use of a novel HIV-2 plasma RNA viral load assay using the Abbott m2000 platform. J. Clin. Virol.55:128 –133.http://dx.doi.org/10.1016/j .jcv.2012.06.024.
13. Damond F, Collin G, Descamps D, Matheron S, Pueyo S, Taieb A, Campa P, Benard A, Chene G, Brun-Vezinet F.2005. Improved sensi-tivity of human immunodeficiency virus type 2 subtype B plasma viral load assay. J. Clin. Microbiol.43:4234 – 4236.http://dx.doi.org/10.1128 /JCM.43.8.4234-4236.2005.
14. Delarue S, Didier E, Damond F, Ponscarme D, Brengle-Pesce K, Re-sche-Rigon M, Vray M, Gueudin M, Simon F.2013. Highly sensitive plasma RNA quantification by real-time PCR in HIV-2 group A and group B infection. J. Clin. Virol. 58:461– 467.http://dx.doi.org/10.1016/j.jcv .2013.08.003.
15. Ferns RB, Garson JA.2006. Development and evaluation of a real-time RT-PCR assay for quantification of cell-free human immunodeficiency virus type 2 using a Brome mosaic virus internal control. J. Virol. Methods
135:102–108.http://dx.doi.org/10.1016/j.jviromet.2006.02.005. 16. Rodes B, Sheldon J, Toro C, Cuevas L, Perez-Pastrana E, Herrera I,
Soriano V.2007. Quantitative detection of plasma human immunodefi-ciency virus type 2 subtype A RNA by the Nuclisens EasyQ Assay (version 1.1). J. Clin. Microbiol.45:88 –92.http://dx.doi.org/10.1128/JCM.01613-06. 17. Ruelle J, Mukadi BK, Schutten M, Goubau P.2004. Quantitative
real-time PCR on Lightcycler for the detection of human immunodeficiency virus type 2 (HIV-2). J. Virol. Methods117:67–74.http://dx.doi.org/10 .1016/j.jviromet.2003.12.006.
18. Styer LM, Miller TT, Parker MM.2013. Validation and clinical use of a sensitive HIV-2 viral load assay that uses a whole virus internal control. J. Clin. Virol.58(Suppl 1):e127– e133.
19. Damond F, Benard A, Balotta C, Boni J, Cotten M, Duque V, Ferns B, Garson J, Gomes P, Goncalves F, Gottlieb G, Kupfer B, Ruelle J, Rodes B, Soriano V, Wainberg M, Taieb A, Matheron S, Chene G, Brun-Vezinet F.2011. An international collaboration to standardize HIV-2 viral load assays: results from the 2009 ACHIEV2Equality control study. J.
Clin. Microbiol.49:3491–3497.http://dx.doi.org/10.1128/JCM.02389-10. 20. Damond F, Benard A, Ruelle J, Alabi A, Kupfer B, Gomes P, Rodes B, Albert J, Boni J, Garson J, Ferns B, Matheron S, Chene G, Brun-Vezinet F.2008. Quality control assessment of human immunodeficiency virus type 2 (HIV-2) viral load quantification assays: results from an interna-tional collaboration on HIV-2 infection in 2006. J. Clin. Microbiol.46:
2088 –2091.http://dx.doi.org/10.1128/JCM.00126-08.
21. Ayouba A, Akoua-Koffi C, Calvignac-Spencer S, Esteban A, Locatelli S, Li H, Li Y, Hahn BH, Delaporte E, Leendertz FH, Peeters M.2013. Evidence for continuing cross-species transmission of SIVsmm to humans: character-ization of a new HIV-2 lineage in rural Cote d’Ivoire. AIDS27:2488 –2491.
http://dx.doi.org/10.1097/01.aids.0000432443.22684.50.
22. Damond F, Worobey M, Campa P, Farfara I, Collin G, Matheron S, Brun-Vezinet F, Robertson DL, Simon F.2004. Identification of a highly divergent HIV-2 and proposal for a change in HIV-2
classifica-tion. AIDS Res. Hum. Retroviruses20:666 – 672.http://dx.doi.org/10 .1089/0889222041217392.
23. Gao F, Yue L, Robertson DL, Hill SC, Hui H, Biggar RJ, Neequaye AE, Whelan TM, Ho DD, Shaw GM. 1994. Genetic diversity of human immunodeficiency virus type 2: evidence for distinct sequence subtypes with differences in virus biology. J. Virol.68:7433–7447.
24. Schulz TF, Whitby D, Hoad JG, Corrah T, Whittle H, Weiss RA.1990. Biological and molecular variability of human immunodeficiency virus type 2 isolates from The Gambia. J. Virol.64:5177–5182.
25. Soriano V, Gomes P, Heneine W, Holguin A, Doruana M, Antunes R, Mansinho K, Switzer WM, Araujo C, Shanmugam V, Lourenco H, Gon-zalez-Lahoz J, Antunes F.2000. Human immunodeficiency virus type 2 (HIV-2) in Portugal: clinical spectrum, circulating subtypes, virus isolation, and plasma viral load. J. Med. Virol.61:111–116.
26. Aghokeng AF, Monleau M, Eymard-Duvernay S, Dagnra A, Kania D, Ngo-Giang-Huong N, Toni TD, Toure-Kane C, Truong LX, Delaporte E, Chaix ML, Peeters M, Ayouba A.2013. Extraordinary heterogeneity of virological outcomes in patients receiving highly antiretroviral therapy and monitored with the World Health Organization public health ap-proach in Sub-Saharan Africa and Southeast Asia. Clin. Infect. Dis.58:99 – 109.http://dx.doi.org/10.1093/cid/cit627.
27. Rouet F, Ekouevi DK, Chaix ML, Burgard M, Inwoley A, Tony TD, Danel C, Anglaret X, Leroy V, Msellati P, Dabis F, Rouzioux C.2005. Transfer and evaluation of an automated, low-cost real-time reverse tran-scription-PCR test for diagnosis and monitoring of human immunodefi-ciency virus type 1 infection in a West African resource-limited setting. J. Clin. Microbiol.43:2709 –2717.http://dx.doi.org/10.1128/JCM.43.6.2709 -2717.2005.
28. Rouet F, Ekouevi DK, Inwoley A, Chaix ML, Burgard M, Bequet L, Viho I, Leroy V, Simon F, Dabis F, Rouzioux C.2004. Field evaluation of a rapid human immunodeficiency virus (HIV) serial serologic testing algorithm for diagnosis and differentiation of HIV type 1 (HIV-1), HIV-2, and dual HIV-1-HIV-2 infections in West African pregnant women. J. Clin. Microbiol.42:4147– 4153.http://dx.doi.org/10.1128/JCM.42.9.4147 -4153.2004.
29. Bland JM, Altman DG.1986. Statistical methods for assessing agreement between two methods of clinical measurement. Lanceti:307–310. 30. Plantier JC, Gueudin M, de Oliveira F, Damond F, Lemee V,
Brun-Vezinet F, Simon F.2004. Rapid discrimination between human immu-nodeficiency virus type 2 groups A and B by real-time PCR. J. Clin. Mi-crobiol. 42:5866 –5870. http://dx.doi.org/10.1128/JCM.42.12.5866-5870 .2004.
31. Damond F, Avettand-Fenoel V, Collin G, Roquebert B, Plantier JC, Ganon A, Sizmann D, Babiel R, Glaubitz J, Chaix ML, Brun-Vezinet F, Descamps D, Rouzioux C.2010. Evaluation of an upgraded version of the Roche Cobas AmpliPrep/Cobas TaqMan HIV-1 test for HIV-1 load quan-tification. J. Clin. Microbiol. 48:1413–1416. http://dx.doi.org/10.1128 /JCM.01409-09.