Performance Validation of Selective Screening Agars for
Guiding Antimicrobial Prophylaxis in Patients Undergoing
Prostate Biopsy
Sofie C. M. Tops,
aMarlie Bruens,
aSacha van Mook-Vermulst,
aDiane Lamers-Jansen,
aTobias Engel,
aGer van den Brink,
bRob van Duuren,
bHeiman F. L. Wertheim,
aEva Kolwijck
aaDepartment of Medical Microbiology, Radboud University Medical Center, Nijmegen, The Netherlands bMediaproducts BV, Groningen, The Netherlands
ABSTRACT
A rectal culture-guided antimicrobial prophylaxis strategy may prevent
infections after transrectal ultrasound-guided prostate biopsy (TRUSP). The use of
se-lective culture media could assist the choice of appropriate antibiotic prophylaxis.
The objective of our study was to evaluate the performance of four selective media
used for guidance of oral antibiotic prophylaxis in TRUSP. In this prospective
valida-tion study, we used MacConkey media with vancomycin plus one of the following
antibiotics: ciprofloxacin (McC3
⫹
CIP/V), trimethoprim (McC3
⫹
TMP/V), fosfomycin
(McC3
⫹
FOF/V), and amdinocillin-amoxicillin-clavulanic acid (McC3
⫹
MEC/V). First,
clinical strains of Gram-negative bacilli (GNB) (
n
⫽
33) were evaluated for growth on
the selective media. Thereafter, rectal swabs (
n
⫽
97) were randomly collected from
residual material of fresh stool samples and plated on a growth control and the four
selective media. Levels of recovery of GNB on the growth control and selective
me-dia were compared, and the MICs of the antibiotics used in this study were
deter-mined. The sensitivity and specificity of the four selective media amounted,
respec-tively, to 90.0% (55.5 to 99.8%) and 98.7% (93.1 to 100.0%) for McC3
⫹
CIP/V, 95.7%
(85.2 to 99.5%) and 100.0% (91.6 to 100.0%) for McC3
⫹
TMP/V, 95.5% (84.5 to 99.4%)
and 97.8% (88.2 to 99.9%) for McC3
⫹
FOF/V, and 100.0% (76.8 to 100.0%) and 97.6%
(87.4 to 99.9%) for McC3
⫹
MEC/V. In conclusion, the four selective media were
suffi-ciently sensitive and specific for the identification of rectal GNB resistant to
cipro-floxacin, trimethoprim, fosfomycin, or amdinocillin-amoxicillin-clavulanic acid. These
media can have added value in streamlining the optimal culture based antibiotic
prophylaxis in TRUSP in a non-labor-intensive manner.
KEYWORDS
antibiotic prophylaxis, performance, selective culture media,
susceptibility testing of Gram-negative bacilli, validation
T
ransrectal ultrasound-guided prostate biopsy (TRUSP) is a well-established
proce-dure to obtain tissue for the histological diagnosis of prostate cancer. During
TRUSP, a spring-loaded device is used to collect multiple core biopsy specimens,
sampling tissue systematically from both sides of the gland. Due to the transrectal
approach, gut bacteria may be inoculated directly into the prostate, bloodstream, or
urinary tract, which can lead to infectious complications (1–6). The introduction of
empirical antimicrobial prophylaxis with ciprofloxacin (CIP) reduced the risk of
infec-tious complications to 1.6% in cases involving susceptible rectal flora (7). However, with
increasing fluoroquinolone (FQ) resistance of (rectal) Gram-negative bacilli (GNB),
in-fection rates after biopsy have risen to 6% in recent years (5, 8–11).
Culture-guided antimicrobial prophylaxis is a promising strategy to reduce the
amount of TRUSP-related infectious complications (7, 12, 13). In this strategy, a
pre-biopsy rectal swab is obtained to screen for resistant rectal GNB in the rectum in
Received14 March 2018Returned for modification10 April 2018Accepted11 June 2018
Accepted manuscript posted online13 June 2018
CitationTops SCM, Bruens M, van Mook-Vermulst S, Lamers-Jansen D, Engel T, van den Brink G, van Duuren R, Wertheim HFL, Kolwijck E. 2018. Performance validation of selective screening agars for guiding antimicrobial prophylaxis in patients undergoing prostate
biopsy. J Clin Microbiol 56:e00253-18.https://
doi.org/10.1128/JCM.00253-18.
EditorAndrew B. Onderdonk, Brigham and Women's Hospital
Copyright© 2018 American Society for
Microbiology.All Rights Reserved.
Address correspondence to Sofie C. M. Tops, sofi[email protected].
crossm
on May 16, 2020 by guest
http://jcm.asm.org/
patients undergoing TRUSP. Antimicrobial prophylaxis can then be personalized to
each patient based on culture results.
To implement this strategy of culture-guided antimicrobial prophylaxis in daily
clinical practice, an accurate and rapid method to identify patients colonized with
resistant rectal GNB is necessary. Since the rectal flora consists of a large variety of GNB,
susceptibility testing of all cultured GNB is extremely time-consuming and expensive
and not suitable for routine diagnostics. To overcome this difficulty, previous studies
already used a selective agar containing CIP (3, 14–18). Within 48 h, a sterile agar plate
then allows urologists to prescribe CIP without any caution. However, in the case of
growth on the CIP agar (recovery of ciprofloxacin-resistant GNB), these studies
per-formed full susceptibility testing of all individual colonies cultured on nonselective
media to select an alternative antibiotic for prophylaxis (3, 14, 15, 17, 18). Consequently,
this method has a long turnaround time and high cost and introduction in routine
diagnostics is not practical, especially when over 20% of cultures may contain
FQ-resistant GNB, which is the case in The Netherlands (19).
For this reason, we developed four selective agars which contain a standard amount
of antibiotics which (or their derivative) are appropriate oral antimicrobial prophylactic
regimes in TRUSP, namely, CIP (20–25), trimethoprim (TMP) (20, 23, 25), fosfomycin
(FOF) (26–30), and amdinocillin (MEC) combined with amoxicillin-clavulanic acid (AMC)
(31). We hypothesize that these agars will support the choice of antimicrobial
prophy-laxis in TRUSP without need for additional susceptibility testing. The purpose of this
validation study was to test whether these selective media detect resistant GNB and
inhibit growth of susceptible GNB using both bacterial strains and fecal samples.
MATERIALS AND METHODS
Selective media.The following five agars (Mediaproducts BV, Groningen, The Netherlands) were used in this study: (i) MacConkey agar no. 3 plus vancomycin (20 mg/liter) plus ciprofloxacin (0.5 mg/liter) (McC3⫹CIP/V), (ii) MacConkey agar no. 3 plus vancomycin (20 mg/liter) plus trimethoprim (2 mg/liter) (McC3⫹TMP/V), (iii) MacConkey agar no. 3 plus vancomycin (20 mg/liter) plus fosfomycin (4 mg/liter) plus glucose-6-phosphate (25 mg/liter) (McC3⫹FOF/V), (iv) MacConkey agar no. 3 plus vancomycin (20 mg/liter) plus amdinocillin (2 mg/liter) plus amoxicillin-clavulanic acid (8 mg/liter) (McC3⫹MEC/V), and (v) MacConkey agar no. 3 plus vancomycin (20 mg/liter) (McC3⫹V) (growth control).
Agar concentrations for CIP, TMP, and AMC were based on clinical breakpoint concentrations for
Enterobacteriaceaerecommended by EUCAST (http://www.eucast.org/clinical_breakpoints/). For FOF and
MEC, lower agar concentrations than EUCAST breakpoints were used, as these breakpoints are for uncomplicated urinary tract infections only and do not take drug concentrations in the prostate into account. Glucose-6-phosphate was added to the McC3⫹FOF/V agar as this is recommended by EUCAST (http://www.eucast.org/clinical_breakpoints/) for maximal enhancement of fosfomycin activity inin vitro testing (32). MEC was combined with AMC, because this combination was found to synergistically reduce the MIC of MEC over 32-fold in extended-spectrum--lactamase (ESBL)-producingEscherichia coli(33).
Bacterial strains. A collection of 33 clinicalEnterobacteriaceae and Pseudomonas aeruginosa strains were obtained from the microbiology department of the Radboud University Medical Center (Radboudumc) and provided to Mediaproducts BV. Reference MICs of the clinical strains were measured by means of a MIC test strip (MTS; Liofilchem, Italy) on Mueller-Hinton agar (Oxoid, Thermo Fisher, Waltham, MA). The strains had variable MICs around the concentrations of the antibiotics in the respective agar. The following strains were used: 8 strains with CIP MICs ranging from 0.032 mg/liter to 32 mg/liter, 6 strains with TMP MICs ranging from 0.125 to 32 mg/liter, 9 strains with FOF MICs ranging from 0.75 to 8 mg/liter, and 10 strains with MEC MICs ranging from 0.047 to 8 mg/liter and AMC MICs ranging from 2 to 32 mg/liter.
From each strain a suspension of 0.5 McFarland standard was made in 0.85% physiological saline. From this suspension 1:10 and 1:100 dilutions were made in 0.85% physiological saline. The MacConkey agars, including the growth control, were inoculated with these three suspensions (0.5 McFarland standard, 1:10 dilution, and 1:100 dilution) using a standardized inoculation loop of 1l. After incubation (24 and 48 h at 35°C), the inoculated agars were assessed for growth. All strains were evaluated on the growth control MacConkey agar. The four selective agars were tested only using the specific strains selected for their MICs around the concentration(s) of the antimicrobial agent(s) in the respective agar. Fecal specimens.At the Radboudumc, a 604-bed teaching hospital that provides regional micro-biology services, residual material of stool samples submitted for routine parasitological tests by general practitioners was collected.
In total, 95 stool samples were prospectively collected between April and December 2017 for the validation of the McC3⫹CIP/V, McC3⫹TMP/V, McC3⫹FOF/V, and McC3⫹MEC/V media (the MEC/V validation was done separately in November and December 2017). Stool samples were processed within 24 h after collection.
on May 16, 2020 by guest
http://jcm.asm.org/
In our microbiological laboratory, an ESwab (Copan Diagnostics, Murrieta, CA) was put in the fecal residual material and suspended in 1 ml of Copan ESwab medium. Then, after brief vortexing of the ESwab specimen tube, 1 drop of ESwab medium was directly plated on both the McC3⫹V (growth control) and the selective agars using a sterile balloon pipette.
After 24 and 48 h of incubation at 35°C, all inoculated agars were assessed for growth. On each separate agar, each colony with different morphology was captured and analyzed using matrix-assisted laser desorption ionization–time of flight mass spectrometry (MALDI-TOF MS; Bioptyper version 3; Bruker, Bremen, Germany). In the case that an isolate was identified by MALDI-TOF MS as a member of the
Enterobacterbacteriaceae, anAcinetobacterspecies, orPseudomonas aeruginosa, the colony was
subcul-tured on Columbia blood agar and incubated for 24 h at 35°C. After incubation, a MIC test strip (Liofilchem, Italy) on Mueller-Hinton agar (Oxoid, Thermo Fisher, Waltham, MA) was used to determine the MIC according to EUCAST (http://www.eucast.org/clinical_breakpoints/) for each separate colony. For determination of the MIC for fosfomycin, we used Mueller-Hinton agar supplemented with 25 mg/liter of glucose-6-phosphate (Mediaproducts BV) according to EUCAST recommendations (http://www.eucast .org/clinical_breakpoints/).
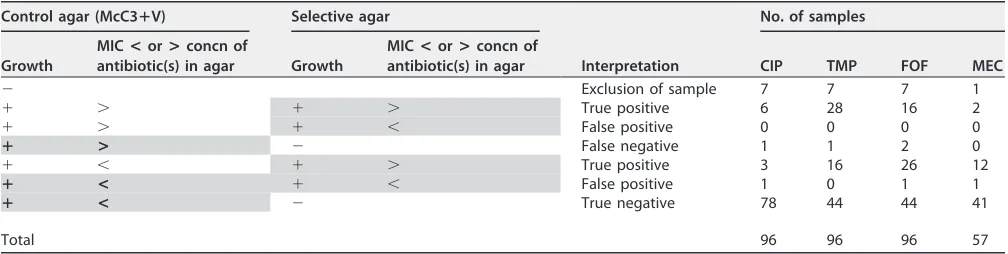
For colonies grown on the control agar (McC3⫹V), the susceptibility to CIP, TMP, FOF, MEC, and AMC was assessed for each morphologically different colony. On the selective agars only the antimicrobial agent present in the agar was tested for each morphologically different colony. After incubation of the agars at 35°C for 24 h, the MIC was read at the point where the zone of inhibition intersected the MIC scale on the strip. In Table 1, the validation process of the selective agars is shown.
Statistical analysis.Descriptive statistics were used as appropriate. For the validation of the media, we calculated the sensitivity, specificity, and accuracy with their 95% confidence interval for the experiments with the fecal samples. The control agar was used as the gold standard for calculation of the sensitivity of the selective media. So, in case of no growth on the selective media, the MIC determination of all morphologically different colonies that grew on the growth control was used to determine if the absence of growth on the selective media was correct. The MIC determination of all morphologically different colonies that grew on the selective media was used as the gold standard for calculation of the specificity.
RESULTS
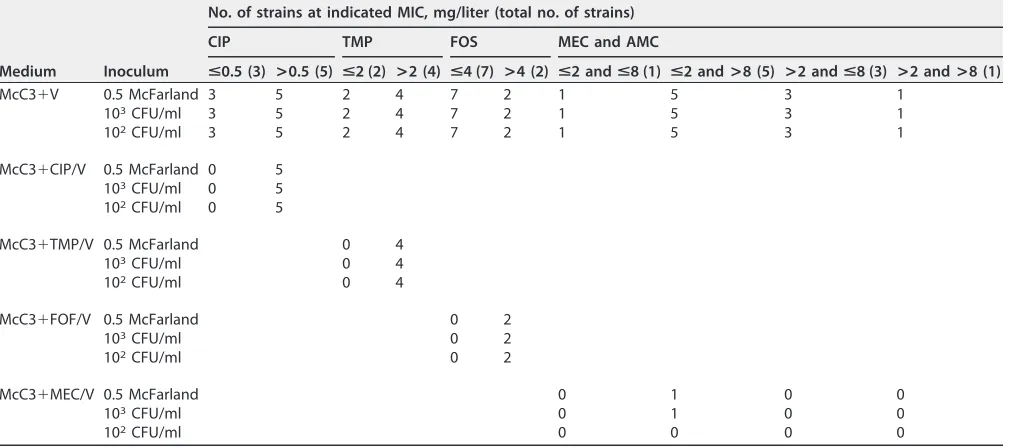
Performance of the selective agars using bacterial strains.
In Table 2, the
numbers of
Enterobacteriaceae
and
Pseudomonas aeruginosa
strains recovered on
the growth control and selective agars are shown. All 33 strains were recovered on
the growth control agar. All GNB with MICs higher than the concentration of the
antibiotic in the selective agar were correctly detected by the selective agars, with
exception of one
Escherichia coli
strain with a MEC MIC of 8 mg/liter and AMC MIC
of 32 mg/liter. This
E. coli
strain unexpectedly showed no growth on the
McC3
⫹
MEC/V agar. In addition, the growth of all GNB with MICs below the
concentration of the antibiotic in the selective agar was inhibited on the selective
agars, with exception of one
E. coli
strain on McC3
⫹
MEC/V at the MIC breakpoint
for MEC (MEC MIC of 2 mg/liter and AMC MIC of 32 mg/liter).
[image:3.585.41.545.82.209.2]Performance of the selective agars using fecal samples.
Ninety-five stool
sam-ples were cultured for
Enterobacteriaceae
,
Acinetobacter
species, or
Pseudomonas
aeruginosa
on the growth control agar (McC3
⫹
V) and the McC3
⫹
CIP/V, McC3
⫹
TMP/V,
and McC3
⫹
FOF/V agars. The performance of the selective agars could not be
deter-mined in 7 stool samples due to a negative growth control, and these samples were
TABLE 1Process of validation of the selective media using fecal samplesaControl agar (McC3ⴙV) Selective agar
Interpretation
No. of samples
Growth
MIC<or>concn of
antibiotic(s) in agar Growth
MIC<or>concn of
antibiotic(s) in agar CIP TMP FOF MEC
⫺ Exclusion of sample 7 7 7 1
⫹ ⬎ ⫹ ⬎ True positive 6 28 16 2
⫹ ⬎ ⫹ ⬍ False positive 0 0 0 0
ⴙ > ⫺ False negative 1 1 2 0
⫹ ⬍ ⫹ ⬎ True positive 3 16 26 12
ⴙ < ⫹ ⬍ False positive 1 0 1 1
ⴙ < ⫺ True negative 78 44 44 41
Total 96 96 96 57
aBold with shading indicates that the control agar was used as the gold standard for calculation of the sensitivity of the selective media. Shading without bold
indicates that the MIC determination of all morphologically different colonies that grew on the concerning selective agar was used as the gold standard for calculation of the specificity.
on May 16, 2020 by guest
http://jcm.asm.org/
excluded from analyses. Fifty-seven stool samples were cultured on the McC3
⫹
V and
McC3
⫹
MEC/V agars. Of these 57 stool samples, 1 sample did not grow on the growth
control agar and was excluded.
Of 88 stool samples, 10 (11.4%) showed growth on the McC3
⫹
CIP/V agar, 44 (50.0%)
on the McC3
⫹
TMP/V agar, and 43 (48.9%) on the McC3
⫹
FOF/V agar. Of 56 stool
samples used for validation of the McC3
⫹
MEC/V agar, 15 (26.8%) showed growth on
the McC3
⫹
MEC/V agar. In Table 3, the performance of the selective agars is shown after
validation in accordance with the protocol in Table 1.
McC3
ⴙ
CIP/V, McC3
ⴙ
TMP/V, and McC3
ⴙ
FOF/V agars.
In total, 141
morphologi-cally different colonies were identified on McC3
⫹
V, originating from the initial 88 fecal
samples used for the validation of the McC3
⫹
CIP/V, McC3
⫹
TMP/V, and McC3
⫹
FOF/V
agars. When comparing the performances of each of the selective agars to the rates of
detection on the control medium, we found that in 52.3% of the fecal samples
additional (resistant) colonies were isolated on the selective agars which we did not
detect on the control MacConkey agar.
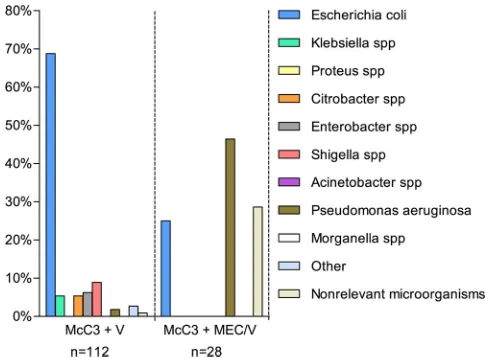
In Fig. 1, the distribution of the cultured microorganisms on the McC3
⫹
V, McC3
⫹
CIP/V,
McC3
⫹
TMP/V, and McC
⫹
FOF/V agars is shown.
McC3
ⴙ
MEC/V agar.
In total, 112 morphologically different colonies were found on
McC3
⫹
V, originating from the 56 fecal samples used for the validation of the McC3
⫹
MEC/V
agar. In Fig. 2, the distribution of the cultured microorganisms on the McC3
⫹
V and
McC3
⫹
MEC/V agars is shown.
DISCUSSION
[image:4.585.42.548.94.318.2]In this validation study, all four screening agars were sufficiently sensitive and
specific for the identification of rectal GNB resistant to CIP, TMP, FOF, and MEC/AMC.
TABLE 2Number ofEnterobacteriaceae(n⫽31) andPseudomonas aeruginosa(n⫽2) strains recovered on various culture media after 48 h of incubationa
Medium Inoculum
No. of strains at indicated MIC, mg/liter (total no. of strains)
CIP TMP FOS MEC and AMC
<0.5 (3) >0.5 (5) <2 (2) >2 (4) <4 (7) >4 (2) <2 and<8 (1) <2 and>8 (5) >2 and<8 (3) >2 and>8 (1)
McC3⫹V 0.5 McFarland 3 5 2 4 7 2 1 5 3 1
103CFU/ml 3 5 2 4 7 2 1 5 3 1
102CFU/ml 3 5 2 4 7 2 1 5 3 1
McC3⫹CIP/V 0.5 McFarland 0 5 103CFU/ml 0 5 102CFU/ml 0 5
McC3⫹TMP/V 0.5 McFarland 0 4
103CFU/ml 0 4
102CFU/ml 0 4
McC3⫹FOF/V 0.5 McFarland 0 2
103CFU/ml 0 2
102CFU/ml 0 2
McC3⫹MEC/V 0.5 McFarland 0 1 0 0
103CFU/ml 0 1 0 0
102CFU/ml 0 0 0 0
aP. aeruginosa(n⫽2) was tested on McC3⫹CIP/V only.
TABLE 3Performance of the selective media using fecal samplesa
Medium % sensitivity % specificity % accuracy
McC3⫹CIP/V 90.0 (55.5–99.8) 98.7 (93.1–100.0) 97.7 (92.0–99.7) McC3⫹TMP/V 95.7 (85.2–99.5) 100.0 (91.6–100.0) 97.7 (92.0–99.7) McC3⫹FOF/V 95.5 (84.5–99.4) 97.8 (88.2–99.9) 96.6 (90.4–99.3) McC3⫹MEC/V 100.0 (76.8–100.0) 97.6 (87.4–99.9) 98.2 (90.5–100.0)
aValues in parentheses are 95% confidence intervals.
on May 16, 2020 by guest
http://jcm.asm.org/
[image:4.585.41.373.675.730.2]Therefore, these media can have added value in guiding the optimal choice of
antibiotic prophylaxis in TRUSP.
Our method of screening for resistant rectal GNB with selective agars is suitable for
use in daily practice, as culture results are available within 48 h and the method is
simple and relatively inexpensive (combined costs of all selective media:
€
5.84 per
patient), as it does not need additional antimicrobial susceptibility testing.
In this study, we showed that an additional advantage of the selective agars was the
increased rate of detection of resistant GNB compared to the control MacConkey
medium. On the standard MacConkey agar, due to the large amount of gut
microor-ganisms that grew, morphologically distinct colonies were difficult to distinguish.
Specifically, we isolated 52.3% additional (resistant) colonies on the selective agars
which we did not detect on the control MacConkey agars. These colonies would have
been missed if the selective agars had not been used, resulting in an incorrect
assumption of antibiotic susceptibility of the rectal flora and possible antimicrobial
prophylaxis failure.
In addition, we found that on the control MacConkey agar even morphologically
identical colonies could have different antimicrobial susceptibilities. So, by using
selective agars, the whole fecal sample administered to the agar can be tested for the
FIG 1Distribution of the cultured microorganisms on the McC3⫹V, McC3⫹CIP/V, McC3⫹TMP/V, and McC3⫹FOF/V agars using fecal samples.FIG 2Distribution of the cultured microorganisms on the McC3⫹V and McC3⫹MEC/V agars using fecal samples.
on May 16, 2020 by guest
http://jcm.asm.org/
[image:5.585.47.400.71.254.2] [image:5.585.83.326.536.715.2]susceptibility of present cultivable bacteria for the specific antibiotic. This is an
advan-tage compared to traditional susceptibility testing, in which only one or a few colonies
are tested and possible heteroresistance might be missed.
The selective agars support the choice of four oral antimicrobial prophylactic
regimes used in TRUSP, namely, CIP, trimethoprim-sulfamethoxazole (SXT), FOF, or
pivmecillinam (PIV) combined with AMC. Trimethoprim was used as marker for SXT
resistance. The McC3
⫹
MEC/V agar contains amdinocillin instead of pivmecillinam, since
pivmecillinam is a prodrug and therefore is not active
in vitro
.
All antibiotics were chosen because of rapid penetration and high concentration in
prostatic tissue (34–37) and potent activity against
Enterobacteriaceae
and
Pseudomo-nas aeruginosa
, which are the most common pathogens causing infections after TRUSP
(5, 11, 21, 22, 31, 38, 39). The antibiotics can be administered orally, and their potential
effectiveness in TRUSP has been shown in previous studies (21–31). Furthermore,
fosfomycin and pivmecillinam are not commonly prescribed in Dutch hospitals, which
diminishes the pressure on antibiotics used in hospitals.
In this study, pivmecillinam was combined with amoxicillin-clavulanic acid, because
this combination was found to synergistically reduce the MIC of amdinocillin over
32-fold in ESBL-producing
Escherichia coli
(33). Moreover, another study (40) showed
that the presence of a single nucleotide polymorphism (SNP) in the promoter of the
TEM-1

-lactamase gene is sufficient to confer resistance to amdinocillin. This resistance
was abolished by the synergistic activity of the combination of amdinocillin and
amoxicillin-clavulanate. To measure synergistic activity, the MIC of the combination of
amdinocillin and amoxicillin-clavulanate can be determined. However, in this study, we
have only determined the MIC of MEC and AMC separately. No synergy testing was
performed. As a result, in our study, resistance to this antimicrobial combination can be
mistakenly assumed if both separate MEC and AMC MICs are higher than their
antibi-otic concentration in the McC3
⫹
MEC/V agar. The synergistic activity between MEC and
AMC might be the reason for the lack of growth of the one
E. coli
strain with a MEC MIC
of 8 mg/liter and AMC MIC of 32 mg/liter on the McC3
⫹
MEC/V agar.
Another limitation of our study is the use of the control agar as the gold standard
for calculation of the sensitivity. As described above, on the control agar,
morpholog-ically distinct colonies were regularly difficult to distinguish; this may have resulted in
an overestimation of the sensitivity.
In addition, the McC3
⫹
MEC/V agar was validated not simultaneously with the other
selective agars but at a later stage with a smaller number of fecal samples. Moreover,
the selective agars were validated with fecal samples from general patients instead of
with fecal samples from our target population (patients undergoing TRUSP). Due to the
relatively low fluoroquinolone resistance rate of the rectal carriage among general
patients (11.4%), there was growth on only 10 (11.4%) of the McC3
⫹
CIP/V agars,
resulting in a wide confidence interval with respect to the sensitivity of this selective
agar. This percentage is probably not representative for our target population, in which
we expect a higher FQ resistance rate. The same applies to the resistance rates of the
other antimicrobial combinations used in this study.
This study was a technical validation of the selective agars. Considering the
encour-aging results of this validation, we are now in the process of using the selective agars
in a prospective, randomized, multicenter trial of approximately 1,600 patients. In this
trial we will assess whether culture-guided antimicrobial prophylaxis in transrectal
prostate biopsy has an influence on infectious complication rates (ClinicalTrials.gov
NCT03228108). The cost-effectiveness of the culture-guided prophylaxis strategy shall
also be estimated in this study. Culture-guided prophylaxis has potential to be an
additional tool to global antibiotic stewardship initiatives in dealing with antibiotic
resistance.
ACKNOWLEDGMENTS
G.V.D.B. and R.V.D. are employed at Mediaproducts BV, which produced the agars for
this validation study. The McC3
⫹
CIP/V agar is already commercially available. The
on May 16, 2020 by guest
http://jcm.asm.org/
McC3
⫹
V, McC3
⫹
TMP/V, McC3
⫹
FOF/V, and McC3
⫹
MEC/V agars are currently available
only for research. The other authors have no conflict of interest to declare.
This study was sponsored by ZonMw, Interreg, and Health-i-Care.
S.C.M.T. had full access to all of the data in the study and takes responsibility for the
integrity of the data and the accuracy of the data analysis. Other contributions are as
follows: study concept and design, G.V.D.B., R.V.D., T.E., E.K., and H.F.L.W.; acquisition,
analysis, or interpretation of data, G.V.D.B., M.B., D.L.-J., S.V.M.-V., and S.C.M.T.; drafting
of the manuscript, S.C.M.T.; critical revision of the manuscript for important intellectual
content, G.V.D.B., T.E., E.K., D.L.-J., S.V.M.-V., and H.F.L.W.; statistical analysis, S.C.M.T.;
technical or material support, G.V.D.B., R.V.D., D.L.-J., and S.V.M.-V.; and study
supervi-sion, E.K.
REFERENCES
1. Liss MA, Taylor SA, Batura D, Steensels D, Chayakulkeeree M, Soenens C, Rao GG, Dash A, Park S, Patel N, Woo J, McDonald M, Nseyo U, Banapour P, Unterberg S, Ahlering TE, Van Poppel H, Sakamoto K, Fierer J, Black PC. 2014. Fluoroquinolone resistant rectal colonization predicts risk of in-fectious complications after transrectal prostate biopsy. J Urol 192: 1673–1678.https://doi.org/10.1016/j.juro.2014.06.005.
2. Loeb S, van den Heuvel S, Zhu X, Bangma CH, Schroder FH, Roobol MJ. 2012. Infectious complications and hospital admissions after prostate biopsy in a European randomized trial. Eur Urol 61:1110 –1114.https:// doi.org/10.1016/j.eururo.2011.12.058.
3. Summers SJ, Patel DP, Hamilton BD, Presson AP, Fisher MA, Lowrance WT, Southwick AW. 2015. An antimicrobial prophylaxis protocol using rectal swab cultures for transrectal prostate biopsy. World J Urol 33: 2001–2007.https://doi.org/10.1007/s00345-015-1571-y.
4. Marino K, Parlee A, Orlando R, Lerner L, Strymish J, Gupta K. 2015. Compar-ative effectiveness of single versus combination antibiotic prophylaxis for infections after transrectal prostate biopsy. Antimicrob Agents Chemother 59:7273–7275.https://doi.org/10.1128/AAC.01457-15.
5. Taylor S, Margolick J, Abughosh Z, Goldenberg SL, Lange D, Bowie WR, Bell R, Roscoe D, Machan L, Black P. 2013. Ciprofloxacin resistance in the faecal carriage of patients undergoing transrectal ultrasound guided prostate biopsy. BJU Int 111:946 –953. https://doi.org/10.1111/j.1464 -410X.2012.11637.x.
6. Zaytoun OM, Vargo EH, Rajan R, Berglund R, Gordon S, Jones JS. 2011. Emergence of fluoroquinolone-resistant Escherichia coli as cause of postprostate biopsy infection: implications for prophylaxis and treat-ment. Urology 77:1035–1041.https://doi.org/10.1016/j.urology.2010.12 .067.
7. Van Besien J, Uvin P, Van den Abeele AM, Merckx L. 2016. Prevalence, risk factors, and clinical relevance of fluoroquinolone-resistant organ-isms in rectal cultures: should we target antibiotic prophylaxis prior to prostate biopsy? Adv Urol 2016:5392107.https://doi.org/10.1155/2016/ 5392107.
8. Vlek ALM, Ruiter AEC, Vijverberg PLM, Kaan JA. 2014. Infectieuze com-plicaties en antibiotische profylaxe bij transrectale echogeleide prosta-atbiopsie. Tijdschr Urol 5:119 –124.https://doi.org/10.1007/s13629-014 -0065-9.
9. Loeb S, Carter HB, Berndt SI, Ricker W, Schaeffer EM. 2011. Complications after prostate biopsy: data from SEER-Medicare. J Urol 186:1830 –1834. https://doi.org/10.1016/j.juro.2011.06.057.
10. Carignan A, Roussy JF, Lapointe V, Valiquette L, Sabbagh R, Pepin J. 2012. Increasing risk of infectious complications after transrectal ultrasound-guided prostate biopsies: time to reassess antimicrobial pro-phylaxis? Eur Urol 62:453– 459.https://doi.org/10.1016/j.eururo.2012.04 .044.
11. Steensels D, Slabbaert K, De Wever L, Vermeersch P, Van Poppel H, Verhae-gen J. 2012. Fluoroquinolone-resistant E. coli in intestinal flora of patients undergoing transrectal ultrasound-guided prostate biopsy—should we re-assess our practices for antibiotic prophylaxis? Clin Microbiol Infect 18: 575–581.https://doi.org/10.1111/j.1469-0691.2011.03638.x.
12. Cussans A, Somani BK, Basarab A, Dudderidge TJ. 2016. The role of targeted prophylactic antimicrobial therapy before transrectal ultrasonography-guided prostate biopsy in reducing infection rates: a systematic review. BJU Int 117:725–731. https://doi.org/10.1111/bju .13402.
13. Lu DD, Raman JD. 2016. Strategies for prevention of ultrasound-guided prostate biopsy infections. Infect Drug Resist 9:161–169.https://doi.org/ 10.2147/IDR.S96163.
14. Dai J, Leone A, Mermel L, Hwang K, Pareek G, Schiff S, Golijanin D, Renzulli JF, II. 2015. Rectal swab culture-directed antimicrobial prophy-laxis for prostate biopsy and risk of postprocedure infection: a cohort study. Urology 85:8 –14.https://doi.org/10.1016/j.urology.2014.09.035. 15. Duplessis CA, Bavaro M, Simons MP, Marguet C, Santomauro M, Auge B,
Collard DA, Fierer J, Lesperance J. 2012. Rectal cultures before transrectal ultrasound-guided prostate biopsy reduce post-prostatic biopsy infec-tion rates. Urology 79:556 –561. https://doi.org/10.1016/j.urology.2011 .09.057.
16. Farrell JJ, Hicks JL, Wallace SE, Seftel AD. 2017. Impact of preoperative screening for rectal colonization with fluoroquinolone-resistant enteric bacteria on the incidence of sepsis following transrectal ultrasound guided prostate biopsy. Res Rep Urol 9:37– 41.
17. Taylor AK, Zembower TR, Nadler RB, Scheetz MH, Cashy JP, Bowen D, Murphy AB, Dielubanza E, Schaeffer AJ. 2012. Targeted antimicrobial prophylaxis using rectal swab cultures in men undergoing transrectal ultrasound guided prostate biopsy is associated with reduced incidence of postoperative infectious complications and cost of care. J Urol 187: 1275–1279.https://doi.org/10.1016/j.juro.2011.11.115.
18. Liss MA, Kim W, Moskowitz D, Szabo RJ. 2015. Comparative effectiveness of targeted vs empirical antibiotic prophylaxis to prevent sepsis from transrectal prostate biopsy: a retrospective analysis. J Urol 194:397– 402. https://doi.org/10.1016/j.juro.2015.03.110.
19. Greeff de SC, Mouton JW. 2017. NethMap 2017: Consumption of anti-microbial agents and antianti-microbial resistance among medically impor-tant bacteria in The Netherlands/MARAN 2017: monitoring of antimicro-bial resistance and antibiotic usage in animals in The Netherlands in 2016. RIVM, Bilthoven, The Netherlands.
20. Zani EL, Clark OA, Rodrigues Netto N, Jr. 2011. Antibiotic prophylaxis for transrectal prostate biopsy. Cochrane Database Syst Rev 2011:CD006576. 21. Kapoor DA, Klimberg IW, Malek GH, Wegenke JD, Cox CE, Patterson AL,
Graham E, Echols RM, Whalen E, Kowalsky SF. 1998. Single-dose oral cipro-floxacin versus placebo for prophylaxis during transrectal prostate biopsy. Urology 52:552–558.https://doi.org/10.1016/S0090-4295(98)00296-9. 22. Aron M, Rajeev TP, Gupta NP. 2000. Antibiotic prophylaxis for transrectal
needle biopsy of the prostate: a randomized controlled study. BJU Int 85:682– 685.https://doi.org/10.1046/j.1464-410x.2000.00576.x. 23. Grabe M, Bartoletti R, Bjerklund-Johansen TE, Çek HM, Pickard RS, Tenke
P, Wagenlehner F, Wullt B. 2013. Guidelines on urological infections. European Association of Urology, Arnhem, The Netherlands.
24. Wolf JS, Jr, Bennett CJ, Dmochowski RR, Hollenbeck BK, Pearle MS, Schaeffer AJ, Urologic Surgery Antimicrobial Prophylaxis Best Practice Policy Panel. 2008. Best practice policy statement on urologic surgery antimicrobial prophylaxis. J Urol 179:1379 –1390. https://doi.org/10 .1016/j.juro.2008.01.068.
25. Nederlandse Vereniging voor Urologie. 2009. Richtlijn. Bacteriële urin-eweginfecties bij adolescenten en volwassenen. Etiologie, diagnostiek, behandeling en profylaxe. Nederlandse Vereniging voor Urologie, Utrecht, The Netherlands.
26. Cai T, Gallelli L, Cocci A, Tiscione D, Verze P, Lanciotti M, Vanacore D, Rizzo M, Gacci M, Saleh O, Malossini G, Liguori G, Trombetta C, Rocco D, Palmieri A, Bartoletti R, Carini M, Wagenlehner FM, Naber K, Mirone V,
on May 16, 2020 by guest
http://jcm.asm.org/
Bjerklund Johansen TE. 2017. Antimicrobial prophylaxis for transrectal ultrasound-guided prostate biopsy: fosfomycin trometamol, an attrac-tive alternaattrac-tive. World J Urol 35:221–228.https://doi.org/10.1007/s00345 -016-1867-6.
27. Fahmy AM, Kotb A, Youssif TA, Abdeldiam H, Algebaly O, Elabbady A. 2016. Fosfomycin antimicrobial prophylaxis for transrectal ultrasound-guided biopsy of the prostate: a prospective randomised study. Arab J Urol 14:228 –233.https://doi.org/10.1016/j.aju.2016.05.003.
28. Sen V, Aydogdu O, Bozkurt IH, Yonguc T, Sen P, Polat S, Degirmenci T, Bolat D. 2015. The use of prophylactic single-dose fosfomycin in patients who undergo transrectal ultrasound-guided prostate biopsy: a prospec-tive, randomized, and controlled clinical study. Can Urol Assoc J 9:E863–E867.https://doi.org/10.5489/cuaj.3068.
29. Ongün S, Aslan G, Avkan-Oguz V. 2012. The effectiveness of single-dose fosfomycin as antimicrobial prophylaxis for patients undergoing tran-srectal ultrasound-guided biopsy of the prostate. Urol Int 89:439 – 444. https://doi.org/10.1159/000342370.
30. Kisa E, Altug MU, Gurbuz OA, Ozdemir H. 2017. Fosfomycin: a good alternative drug for prostate biopsy prophylaxis the results of a prospec-tive, randomized trial with respect to risk factors. Int Braz J Urol 43: 1068 –1074.https://doi.org/10.1590/s1677-5538.ibju.2016.0619. 31. Antsupova V, Norgaard N, Bisbjerg R, Nygaard Jensen J, Boel J, Jarlov JO,
Arpi M. 2014. Antibiotic prophylaxis for transrectal prostate biopsy—a new strategy. J Antimicrob Chemother 69:3372–3378.https://doi.org/10 .1093/jac/dku293.
32. Castaneda-Garcia A, Blazquez J, Rodriguez-Rojas A. 2013. Molecular mech-anisms and clinical impact of acquired and intrinsic fosfomycin resistance. Antibiotics (Basel) 2:217–236.https://doi.org/10.3390/antibiotics2020217. 33. Lampri N, Galani I, Poulakou G, Katsarolis I, Petrikkos G, Giamarellou H,
Souli M. 2012. Mecillinam/clavulanate combination: a possible option for the treatment of community-acquired uncomplicated urinary tract in-fections caused by extended-spectrum beta-lactamase-producing
Esch-erichia coli. J Antimicrob Chemother 67:2424 –2428.https://doi.org/10 .1093/jac/dks215.
34. Charalabopoulos K, Karachalios G, Baltogiannis D, Charalabopoulos A, Giannakopoulos X, Sofikitis N. 2003. Penetration of antimicrobial agents into the prostate. Chemotherapy 49:269 –279.https://doi.org/10.1159/ 000074526.
35. Jeppesen N, Frimodt-Moller C. 1984. Serum concentrations and pene-tration into prostate of mecillinam and ampicillin. Curr Med Res Opin 9:213–218.
36. Rhodes NJ, Gardiner BJ, Neely MN, Grayson ML, Ellis AG, Lawrentschuk N, Frauman AG, Maxwell KM, Zembower TR, Scheetz MH. 2015. Optimal timing of oral fosfomycin administration for pre-prostate biopsy prophylaxis. J Antimicrob Chemother 70:2068 –2073.https://doi.org/10.1093/jac/dkv067. 37. Gardiner BJ, Mahony AA, Ellis AG, Lawrentschuk N, Bolton DM, Zeglinski
PT, Frauman AG, Grayson ML. 2014. Is fosfomycin a potential treatment alternative for multidrug-resistant gram-negative prostatitis? Clin Infect Dis 58:e101– e105.https://doi.org/10.1093/cid/cit704.
38. Campeggi A, Ouzaid I, Xylinas E, Lesprit P, Hoznek A, Vordos D, Abbou CC, Salomon L, de la Taille A. 2014. Acute bacterial prostatitis after transrectal ultrasound-guided prostate biopsy: epidemiological, bacteria and treatment patterns from a 4-year prospective study. Int J Urol 21:152–155.https://doi.org/10.1111/iju.12207.
39. Wagenlehner FM, van Oostrum E, Tenke P, Tandogdu Z, Cek M, Grabe M, Wullt B, Pickard R, Naber KG, Pilatz A, Weidner W, Bjerklund-Johansen TE, GPIU Investigators. 2013. Infective complications after prostate biopsy: out-come of the Global Prevalence study of Infections in Urology (GPIU) 2010 and 2011, a prospective multinational multicentre prostate biopsy study. Eur Urol 63:521–527.https://doi.org/10.1016/j.eururo.2012.06.003. 40. Birgy A, Delecourt M, Geslain G, Desselas E, Caseris M, Magnan M,
Mariani-Kurkdjian P, Bidet P, Bonacorsi S. 2017. A combination of me-cillinam and amoxicillin/clavulanate can restore susceptibility of high-level TEM-1-producing Escherichia coli to mecillinam. J Antimicrob Che-mother 72:1911–1914.https://doi.org/10.1093/jac/dkx087.