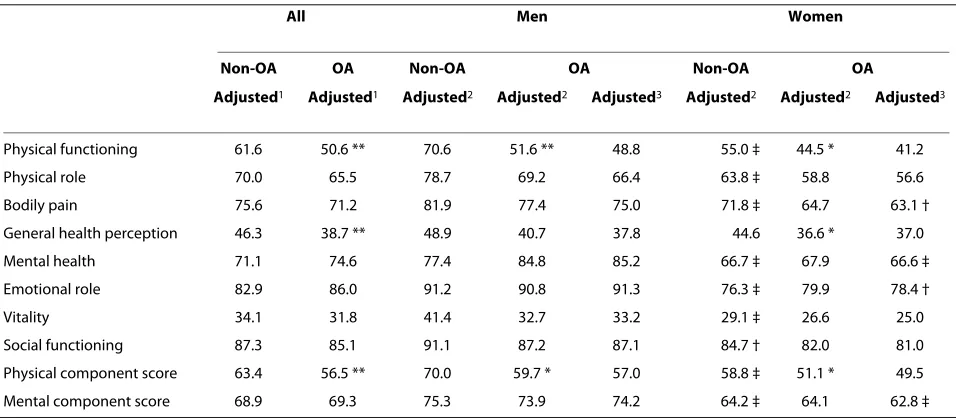
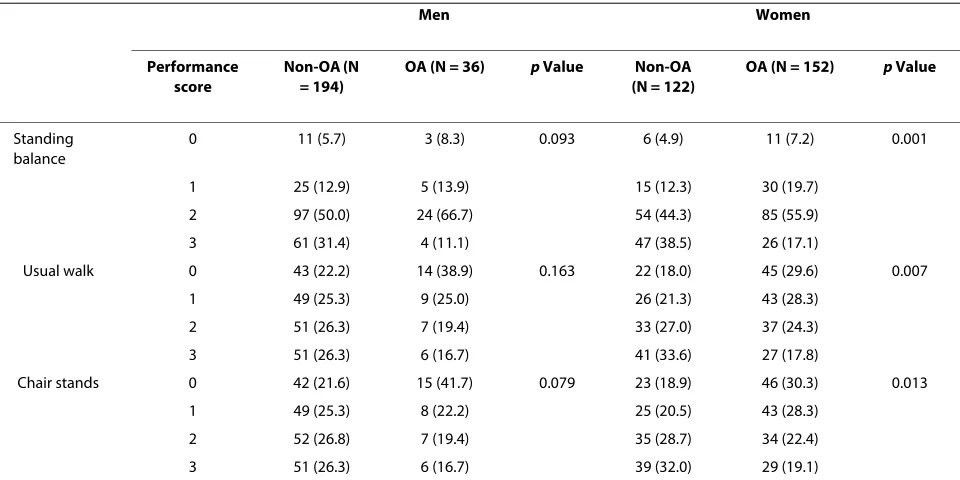
Tibiofemoral osteoarthritis affects quality of life and function in elderly Koreans, with women more adversely affected than men
6
0
0
Full text
Figure
Related documents