Evaluation of the Effects of Clomipramine on Canine Thyroid
Function Tests
Keven P. Gulikers and David L. Panciera
To evaluate the effect of long-term clomipramine administration on the hypothalamic-pituitary-thyroid axis in healthy dogs, 14 healthy adult dogs were enrolled in a prospective study. Clomipramine (3 mg/kg PO q12h) was administered to all dogs beginning on day 0, and continued for 112 days. Serum total thyroxine (T4), free thyroxine (fT4), 3,5,3⬘-triiodothyronine (T3), 3,3⬘,5⬘ -triiodothyronine (reverse T3; rT3), and thyroid-stimulating hormone (TSH) were measured on days 0, 7, 28, 42, 56, and 112. Thyrotropin-releasing hormone (TRH) response tests were performed concurrently. Significant decreases were noted in serum T4, fT4, and rT3concentrations beginning on day 28 through the end of the study period. The lowest mean (⫾SEM) concentrations of T4(26⫾1.2 to 17⫾0.5 nmol/L) and rT3(1.21⫾0.13 to 0.83⫾0.08 nmol/L) occurred at day 112, whereas the lowest mean fT4(29⫾2.4 to 18⫾1.7 pmol/L) was found on day 56 of clomipramine treatment. The effect of treatment over time on serum T3concentration also was significant, but the deviation in T3from baseline was variable. No significant effect of clomipramine treatment was noted on either pre- or post-TRH TSH concentrations. The 35 and 38% decreases in serum T4and fT4concentrations, respectively, during clomipramine administration may lead to a misdiagnosis of hypothyroidism. Although no evidence of hypo-thyroidism was noted in this study population, subclinical hypohypo-thyroidism may have occurred. A longer duration of treatment might further suppress thyroid function, and concurrent illness or other drug administration might exacerbate clomipramine’s effects.
Key words: Dog; Hormone; Thyroxine; Tricyclic antidepressant.
S
everal drugs have been reported to alter thyroid function
tests in dogs, including glucocorticoids, potentiated
sulfonamides, and anticonvulsants.
1–6Many more drugs
have been reported to affect thyroid function in humans and
other species. Among these, tricyclic antidepressants
(TCAs) have been shown to impair thyroid hormone
syn-thesis and thyrotropin secretion in humans and rats.
7–10Clomipramine is a TCA that has been used to treat
var-ious psychiatric disorders in humans for more than 30
years, and recently was approved for treatment of
separa-tion anxiety in dogs. Clomipramine exerts a potent and
rel-atively selective serotonin reuptake-inhibiting effect by
blocking the monoamine reuptake transporter of
serotoner-gic neurons.
11,12Furthermore, the primary metabolite,
des-methylclomipramine, is an inhibitor of norepinephrine
re-uptake.
13–15TCAs have been extensively documented to inhibit
thy-roid hormone biosynthesis by altering thythy-roid follicular cell
iodine uptake
16–18and inhibiting thyroid peroxidase.
17,18In
addition, TCAs interfere with the
hypothalamic-pituitary-thyroid (HPT) axis via the serotonergic and noradrenergic
systems, and therefore could lead to a decrease in thyroid
stimulating hormone (TSH), thyroxine (T4), and 3,5,3
⬘
-tri-iodothyronine (T
3) concentrations.
To the authors’ knowledge, no studies on the effect of
clomipramine on thyroid function have been performed in
the dog. If dogs respond in a manner similar to other
spe-cies, evaluation of thyroid function tests may result in a
misdiagnosis of hypothyroidism if a dog is tested while
receiving clomipramine. An additional concern is that if
From the Department of Small Animal Clinical Sciences, Virginia-Maryland Regional College of Veterinary Medicine, Blacksburg, VA. Reprints requests: David L. Panciera, DVM, MS, Department of Small Animal Clinical Sciences, VA-MD Regional College of Veteri-nary Medicine, Blacksburg, VA 24061-0442; e-mail: [email protected]. Submitted March 22, 2002; Revised June 17, 2002; Accepted August 14, 2002.
Copyright䉷2003 by the American College of Veterinary Internal Medicine
0891-6640/03/1701-0000/$3.00/0
clomipramine decreases plasma thyroid hormones,
iatro-genic hypothyroidism may result. This outcome may be of
particular concern because hypothyroidism is a contributing
factor to a variety of psychologic illnesses in humans, and
the therapeutic benefit of TCAs on affective disorders has
been positively modulated by thyroid supplementation in
both humans
19,20and rats.
9Although the relationship
be-tween hypothyroidism and behavioral disorders in dogs is
tenuous, aggression has been reported.
21,22Administration
of clomipramine, if it induces hypothyroidism, may
exac-erbate behavioral signs or reduce the potential positive
be-havioral response to the drug.
The purpose of the study reported here was to evaluate
the effect of long-term clomipramine administration on the
HPT axis in healthy dogs.
Materials and Methods
Dogs
Fourteen random-source dogs (10 males and 4 neutered females), 16–32 kg in weight, of unknown age were determined to be healthy based on physical examination, CBCs, serum biochemistry, heartworm (Dirofilaria immitis) antigen test, and fecal parasite examination. All subjects were housed in indoor runs with a 12-hour light : dark cycle at 22⬚C and conditioned for 3 weeks before study. Dogs were fed a maintenance dry foodaonce per day. This protocol was approved by the Virginia Tech University animal care committee, and all animals were cared for according to the National Institutes of Health Guide for the Care and Use of Laboratory Animals. Euthyroid status was confirmed by finding a normal serum T4(⬎35 nmol/L) response to TSH administration on day⫺7. The TSH stimulation test23consisted of measurement of serum T4before and 6 hours after administration of bovine TSHbat 0.1 IU/kg IV.
Experimental Protocol
Clomipraminec (3 mg/kg PO q12h) was administered on days 0 through 112. Dogs acted as their own controls. Blood samples were collected for measurement of serum concentrations of T4, free thyrox-ine (fT4), T3, 3,3⬘,5⬘-triiodothyronine (reverse T3; rT3), and TSH on days⫺7, 0, 7, 28, 42, 56, and 112. A thyrotropin-releasing hormone (TRH) stimulation test24was performed on days 0, 7, 28, 42, 56, and 112 by collecting blood samples for measurement of serum TSH
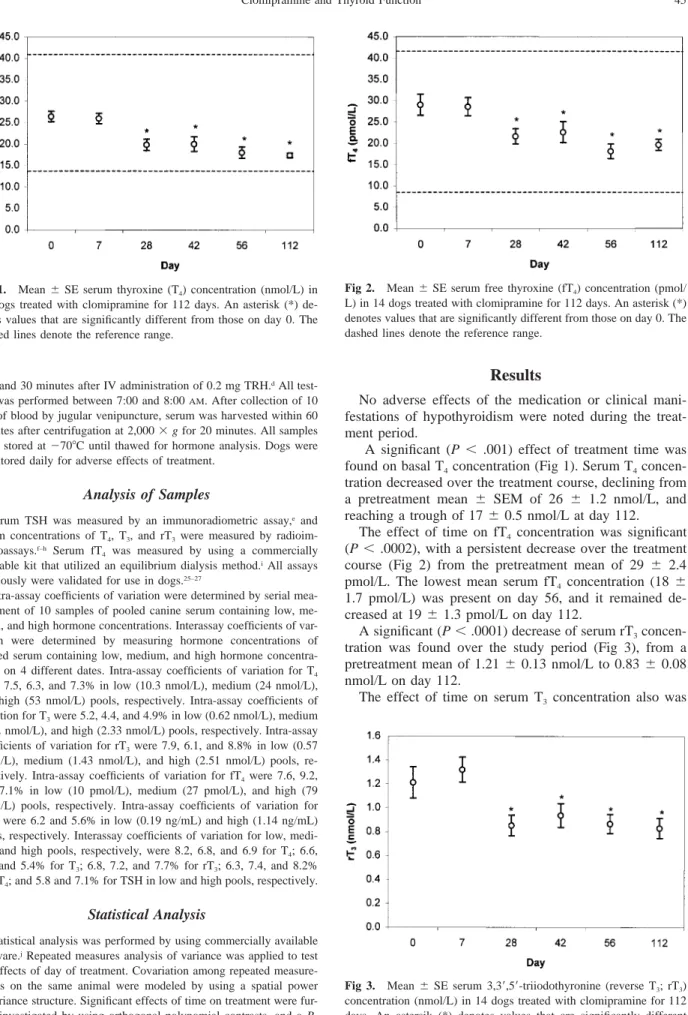
be-Fig 1. Mean⫾SE serum thyroxine (T4) concentration (nmol/L) in 14 dogs treated with clomipramine for 112 days. An asterisk (*) de-notes values that are significantly different from those on day 0. The dashed lines denote the reference range.
Fig 2. Mean⫾SE serum free thyroxine (fT4) concentration (pmol/ L) in 14 dogs treated with clomipramine for 112 days. An asterisk (*) denotes values that are significantly different from those on day 0. The dashed lines denote the reference range.
Fig 3. Mean ⫾SE serum 3,3⬘,5⬘-triiodothyronine (reverse T3; rT3) concentration (nmol/L) in 14 dogs treated with clomipramine for 112 days. An astersik (*) denotes values that are significantly different from those on day 0.
fore and 30 minutes after IV administration of 0.2 mg TRH.dAll test-ing was performed between 7:00 and 8:00AM. After collection of 10 mL of blood by jugular venipuncture, serum was harvested within 60 minutes after centrifugation at 2,000⫻g for 20 minutes. All samples were stored at⫺70⬚C until thawed for hormone analysis. Dogs were monitored daily for adverse effects of treatment.
Analysis of Samples
Serum TSH was measured by an immunoradiometric assay,e and serum concentrations of T4, T3, and rT3were measured by radioim-munoassays.f–h Serum fT
4 was measured by using a commercially available kit that utilized an equilibrium dialysis method.iAll assays previously were validated for use in dogs.25–27
Intra-assay coefficients of variation were determined by serial mea-surement of 10 samples of pooled canine serum containing low, me-dium, and high hormone concentrations. Interassay coefficients of var-iation were determined by measuring hormone concentrations of pooled serum containing low, medium, and high hormone concentra-tions on 4 different dates. Intra-assay coefficients of variation for T4 were 7.5, 6.3, and 7.3% in low (10.3 nmol/L), medium (24 nmol/L), and high (53 nmol/L) pools, respectively. Intra-assay coefficients of variation for T3were 5.2, 4.4, and 4.9% in low (0.62 nmol/L), medium (1.62 nmol/L), and high (2.33 nmol/L) pools, respectively. Intra-assay coefficients of variation for rT3were 7.9, 6.1, and 8.8% in low (0.57 nmol/L), medium (1.43 nmol/L), and high (2.51 nmol/L) pools, re-spectively. Intra-assay coefficients of variation for fT4were 7.6, 9.2, and 7.1% in low (10 pmol/L), medium (27 pmol/L), and high (79 pmol/L) pools, respectively. Intra-assay coefficients of variation for TSH were 6.2 and 5.6% in low (0.19 ng/mL) and high (1.14 ng/mL) pools, respectively. Interassay coefficients of variation for low, medi-um, and high pools, respectively, were 8.2, 6.8, and 6.9 for T4; 6.6, 5.4, and 5.4% for T3; 6.8, 7.2, and 7.7% for rT3; 6.3, 7.4, and 8.2% for fT4; and 5.8 and 7.1% for TSH in low and high pools, respectively.
Statistical Analysis
Statistical analysis was performed by using commercially available software.jRepeated measures analysis of variance was applied to test for effects of day of treatment. Covariation among repeated measure-ments on the same animal were modeled by using a spatial power covariance structure. Significant effects of time on treatment were fur-ther investigated by using orthogonal polynomial contrasts, and a P-value⬍.05 was considered significant.
Results
No adverse effects of the medication or clinical
mani-festations of hypothyroidism were noted during the
treat-ment period.
A significant (P
⬍
.001) effect of treatment time was
found on basal T
4concentration (Fig 1). Serum T
4concen-tration decreased over the treatment course, declining from
a pretreatment mean
⫾
SEM of 26
⫾
1.2 nmol/L, and
reaching a trough of 17
⫾
0.5 nmol/L at day 112.
The effect of time on fT
4concentration was significant
(P
⬍
.0002), with a persistent decrease over the treatment
course (Fig 2) from the pretreatment mean of 29
⫾
2.4
pmol/L. The lowest mean serum fT4
concentration (18
⫾
1.7 pmol/L) was present on day 56, and it remained
de-creased at 19
⫾
1.3 pmol/L on day 112.
A significant (P
⬍
.0001) decrease of serum rT
3concen-tration was found over the study period (Fig 3), from a
pretreatment mean of 1.21
⫾
0.13 nmol/L to 0.83
⫾
0.08
nmol/L on day 112.
Fig 4. Mean⫾SE serum 3,5,3⬘-triiodothyronine (T3) concentration (nmol/L) in 14 dogs treated with clomipramine for 112 days. An as-terisk (*) denotes values that are significantly different from those on day 0. The dashed lines denote the reference range.
Fig 5. Mean ⫾ SE pre– and post–thyrotropin-releasing hormone (TRH) stimulation serum thyroid-stimulating hormone (TSH) concen-trations (ng/mL) in 14 dogs treated with clomipramine for 112 days. No significant differences were noted. The dashed line denotes the upper limit of the reference range.
significant (P
⬍
.0001), but the deviation in T
3from
base-line was variable (Fig 4). No consistent trend in T3
con-centrations could be identified, nor was it possible to fit the
data to either a linear or polynomial trend. Significant
in-creases in serum T
3were noted at days 42 and 112. The T
3concentration increased from a baseline concentration of
1.40
⫾
0.21 nmol/L to 1.83
⫾
0.3 nmol/L on day 112 of
treatment, with the lowest concentration (1.18
⫾
0.09 nmol/
L) occurring on day 56.
No statistically significant effect of time was noted in
either basal or post-TRH TSH concentrations (Fig 5).
Discussion
The significant decreases in serum concentrations of T
4,
fT4, and rT3
during clomipramine administration were rapid
in onset and consistent throughout the duration of
treat-ment. The lack of a placebo-treated control group in the
study detracts from the results because variables other than
the effect of clomipramine treatment could have influenced
hormone concentrations over time. Thyroid hormone
con-centrations are known to fluctuate in individual dogs.
28However, multiple studies over periods of 8 weeks or
lon-ger that used similar husbandry conditions have
document-ed little variation in the mean serum T
4and T
3concentra-tions, although fT4
may be more variable.
26,29,30Similar
study designs have been used in other studies that have
evaluated the effects of drugs on thyroid function,
partic-ularly when the study duration is prolonged.
5,6,31The
pro-longed duration of treatment in the present study was
nec-essary because the effect of TCA on the monoaminergic
systems (serotonin, norepinephrine, and dopamine) via
re-uptake inhibition of neurotransmitters at the synaptic cleft
32may work by modifying receptor site sensitivity rather than
by direct action at the receptor site, thereby taking weeks
to modulate an effect on serotonin concentrations.
33,34This
observation is supported by clinical evidence in humans in
whom beneficial effects attributable to treatment require 4–
6 weeks.
35,36Furthermore, negative feedback of the
mono-aminergic system with resultant upregulation at the level of
the synapse is a prolonged process, and weeks are required
to reach steady state even though high plasma
concentra-tions are achieved.
33,36Power analysis during design of the
study determined that a minimum of 12 dogs was required
to ensure a type II error of 90% or less. To conserve
re-sources because of the length of the study, all dogs acted
as their own controls and were treated with clomipramine.
The results of the present study, which demonstrates that
long-term clomipramine administration decreases T
4, fT
4,
and rT3, are consistent with the suppressive effects of TCAs
on thyroid function found in other species. Although the
effect TCAs have on the thyroid gland and its function
varies among species, several mechanisms probably
ac-count for the clomipramine-induced depression of thyroid
function. Clomipramine binds iodine, thereby preventing T
4synthesis. Clomipramine’s capacity to donate electrons and
impair iodine availability in the thyroid gland has been
shown to be 40 times the minimum amount required to
produce hypothyroidism, and it has a potency
approximate-ly 20% that of methimazole.
17TCAs also inhibit T4
pro-duction via their effect on thyroid peroxidase (TPO),
17,18and in vitro studies have demonstrated that clomipramine
irreversibly inhibits TPO by binding iodide molecules to
the heme portion of the enzyme.
17,37The concentration of
clomipramine required for 50% inhibition of horseradish
peroxidase (as a substitute for TPO) was approximately 14
times the plasma clomipramine concentration obtained in
dogs treated with clomipramine at 2 mg/kg twice daily.
17,38However, plasma concentrations are misleading because
thyroidal concentrations of imipramine and desipramine
(pharmacologically similar TCAs) were 19 and 6 times,
re-spectively, those found in serum in rats treated with these
agents for 4 weeks.
39Therefore, the thyroid gland
concen-tration of clomipramine in dogs in the current study may
have been sufficient to inhibit TPO and result in decreases
in T4
and fT4.
In addition to their effects on thyroid hormone synthesis,
TCAs influence T4
metabolism. In a study of rats treated
with desipramine, a TCA similar to clomipramine, an
in-crease in 5
⬘
-deiodinase activity (responsible for
deiodin-ation of T
4) was noted in the brain. In that study, decreased
serum T
4concentrations and serum T
3concentrations also
were found.
40Although no effect was seen in peripheral
deiodination by the liver or kidneys,
40the effect of TCAs
on canine deiodinases is unknown. Serum concentrations of
thyroid hormones are more dependent on deiodination in
peripheral tissues such as the liver than in the central
ner-vous system (CNS), and the stimulatory effect of TCA on
5
⬘
-deiodinase in the CNS may be of little consequence for
serum thyroid hormone concentrations. The decrease in rT
3found in the present study could be the result of decreased
T
4secretion, and therefore decreased substrate for
conver-sion to rT3.
Considerable variation in T
3concentrations occurred
over the length of the study, and may be due to both
thy-roidal and extrathythy-roidal conversion of T
4to T
3via 5
⬘
-deiodinase enzymes.
41However, changes in deiodination
seem an unlikely explanation for the increased serum T
3.
Enhanced thyroid secretion of T3
in proportion to T4
ap-pears to be dependent on TSH inducing increased type II
5
⬘
-deiodinase activity in the thyroid.
42However, TSH was
not increased in the present study, and is an unlikely
ex-planation for the changes seen. Alterations in alternative
pathways of T
3metabolism, such as sulfation, possibly are
decreased by clomipramine. However, no evidence exists
to support this, and we are unable to explain this result.
Although the 35% decrease in T4
and 38% decrease in
fT
4seen in this study should cause a rise in TSH
tration, no significant change in basal serum TSH
concen-tration or TSH response to TRH adminisconcen-tration was noted.
This poor response likely reflects actual suppression of TSH
by clomipramine, or poor sensitivity, specificity, or both of
the assay method. Alternatively, stimulation of pituitary
type II 5
⬘
-deiodinase activity by clomipramine could result
in increased T3
in thyrotropes and subsequently suppression
of TSH secretion. Although this has not specifically been
studied, type II 5
⬘
-deiodinase activity in the brain of rats is
increased by desipramine administration.
40The smaller
in-crease in serum TSH in response to TRH in the present
study, as compared to other studies,
24,43may have been
af-fected by the source of TRH used, because chemical (not
pharmaceutical) grade TRH was used. However, a
distur-bance in the hypothalamic-pituitary axis still should be
de-tected because of the marked decrease in T
4and fT
4and
their influence on negative feedback regulation of the
pi-tuitary gland. Furthermore, variations in secretion of TRH,
and subsequently TSH, also may be due to clomipramine’s
inhibition of neurotransmitter reuptake at the synaptic
cleft.
32Studies in different species have demonstrated
vari-able effects of serotonin on the HPT axis.
18In rats, serotonin
inhibited TRH secretion, whereas serotonin stimulated TSH
secretion in monkeys.
44Humans administered clomipramine
had a decrease in serum TSH concentrations.
45–47Neuro-chemical regulation of the HPT axis has yet to be
charac-terized in the dog, and any effect of TCAs such as
clomip-ramine on TRH and TSH secretion via monoaminergic
con-trol could not be determined from these data, and was
be-yond the scope of this study.
The clinical importance of the decrease in T4
and fT4
with prolonged administration of clomipramine lies in the
interference with a diagnosis of hypothyroidism, the
poten-tial for hypothyroidism to be induced, and potenpoten-tial effects
on the therapeutic response to clomipramine. The reduction
of serum T4
and fT4
concentrations from baseline values by
35 and 38%, respectively, could lead to a misdiagnosis of
spontaneous hypothyroidism, and, therefore, thyroid
func-tion should be evaluated cautiously in dogs receiving
clo-mipramine.
Although mean concentrations of T
4and fT
4during
clo-mipramine treatment were within the reference range for
most laboratories, examination of our results suggests that
clinical hypothyroidism could develop in some
circum-stances. Dogs with subclinical thyroid dysfunction, those
receiving other drugs that suppress thyroid function, and
those with nonthyroidal illness could be at risk for
devel-oping hypothyroidism during clomipramine administration.
Although clinical evidence of hypothyroidism was not
found in the present study, subclinical hypothyroidism may
have existed. In addition, treatment of longer duration could
result in more pronounced effects on thyroid function, and
the results of this study should be confirmed in a larger,
placebo-controlled population or clinical trial.
Because behavioral changes have been reported in
hy-pothyroid dogs, administration of a TCA such as
clomip-ramine that has the potential to cause hypothyroidism may
exacerbate behavioral signs or reduce the benefit of the
drug. These phenomena have been investigated in humans,
because a decrease in thyroid function has been reported to
be associated with depression, and the supplementation of
thyroxine or T3
as an adjunct to refractory depression has
been shown to be beneficial.
7Although this has not been
demonstrated in the dog, and we do not recommend that
thyroxine supplementation be administered in refractory
cases, it may be prudent to monitor thyroid function tests
in addition to conducting a complete physical examination,
CBC, and serum biochemistry, before and during
clomip-ramine administration, to ensure that hypothyroidism is not
misdiagnosed, or does not subsequently occur.
Footnotes
aHill’s Science Diet Maintenance (Dry), Hill’s Corporation, Topeka, KS bbovine TSH, Sigma Chemical Corporation, St Louis, MO
cClomicalm, Novartis Animal Health, Greensboro, NC
dpGlu-His-Pro-amide trifluoroacetate salt (Synthetic TRH), Sigma Chemical Corporation, St Louis, MO
eCoat-A-Count Canine TSH IRMA, Diagnostic Products Corporation, Los Angeles, CA
fCoat-A-Count Canine T
4, Diagnostic Products Corporation, Los An-geles, CA
gCoat-A-Count Canine T
3, Diagnostic Products Corporation, Los An-geles, CA
hReverse T
3Radioimmunoassay, Biochem Immunosystems Italia SPA, Bologna, Italy
iFree T
4by Equilibrium Dialysis, Nichols Diagnostics, San Luis Obis-po, CA
jSAS, version 6.12, SAS Institute, Cary, NC
Acknowledgments
We wish to thank Dan Ward for support with statistical
analysis; John Strauss, Taryn Brandt, and Stephanie
Mil-burn for assistance with data collection; and Novartis
An-imal Health for donation of the clomipramine. This research
was supported by a grant from the Virginia Veterinary
Medical Association.
References
1. Daminet S, Paradis M, Refsal KR, et al. Short-term influence of prednisone and phenobarbital on thyroid function in euthyroid dogs. Can Vet J 1999;40:411–415.
2. Gaskill CL, Burton SA, Gelens HC, et al. Effects of phenobar-bital treatment on serum thyroxine and thyroid-stimulating hormone concentrations in epileptic dogs. J Am Vet Med Assoc 1999;215:489– 496.
3. Hall IA, Campbell KL, Chambers MD, et al. Effect of trimeth-oprim/sulfamethoxazole on thyroid function in dogs with pyoderma. J Am Vet Med Assoc 1993;202:1959–1962.
4. Kantrowitz LB, Peterson ME, Trepanier LA, et al. Serum total thyroxine, total triiodothyronine, free thyroxine, and thyrotropin con-centrations in epileptic dogs treated with anticonvulsants. J Am Vet Med Assoc 1999;214:1804–1808.
5. Muller PB, Wolfsheimer KJ, Taboada J, et al. Effects of long-term phenobarbital treatment on the thyroid and adrenal axis and ad-renal function tests in dogs. J Vet Intern Med 2000;14:157–164.
6. Torres SM, McKeever PJ, Johnston SD. Effect of oral adminis-tration of prednisolone on thyroid function in dogs. Am J Vet Res 1991;52:416–421.
7. Earle BV. Thyroid hormone and tricyclic antidepressants in re-sistant depressions. Am J Psychiatry 1970;126:1667–1669.
8. Kusalic M, Engelsmann F, Bradwejn J. Thyroid functioning dur-ing treatment for depression. J Psychiatry Neurosci 1993;18:260–263. 9. Martin P, Massol J, Belon JP, et al. Thyroid function and reversal by antidepressant drugs of depressive-like behavior (escape deficits) in rats. Neuropsychobiology 1987;18:21–26.
10. Massol J, Martin P, Chatelain F, et al. Tricyclic antidepressants, thyroid function, and their relationship with the behavioral responses in rats. Biol Psychiatry 1990;28:967–978.
11. Dumas ML, Pons F, Cadilhac J. Histochemical data on the re-uptake blockade of monoamines by chlomipramine [in French; au-thors’ translation]. Ann Histochim 1975;20:283–290.
12. Peters MD, Davis SK, Austin LS. Clomipramine: An antiob-sessional tricyclic antidepressant. Clin Pharm 1990;9:165–178.
13. Hewson CJ, Conlon PD, Luescher UA, et al. The pharmaco-kinetics of clomipramine and desmethylclomipramine in dogs: Param-eter estimates following a single oral dose and 28 consecutive daily oral doses of clomipramine. J Vet Pharmacol Ther 1998;21:214–222. 14. Martensson B, Wagner A, Beck O, et al. Effects of clomipra-mine treatment on cerebrospinal fluid monoaclomipra-mine metabolites and platelet 3H-imipramine binding and serotonin uptake and concentra-tion in major depressive disorder. Acta Psychiatr Scand 1991;83:125– 133.
15. Noguchi T, Shimoda K, Takahashi S. Clinical significance of plasma levels of clomipramine, its hydroxylated and desmethylated metabolites: Prediction of clinical outcome in mood disorders using discriminant analysis of therapeutic drug monitoring data. J Affect Disord 1993;29:267–279.
16. Buxeraud J, Absil AC, Raby C. Secondary antithyroid action of drugs in relation to structure. J Pharm Sci 1984;73:1687–1690.
17. Rousseau A, Comby F, Buxeraud J, et al. Spectroscopic analysis of charge transfer complex formation and peroxidase inhibition with tricyclic antidepressant drugs: Potential anti-thyroid action. Biol Pharm Bull 1996;19:726–728.
18. Sauvage MF, Marquet P, Rousseau A, et al. Relationship be-tween psychotropic drugs and thyroid function: A review. Toxicol Appl Pharmacol 1998;149:127–135.
19. Sokolov ST, Levitt AJ, Joffe RT. Thyroid hormone levels before unsuccessful antidepressant therapy are associated with later response to T3augmentation. Psychiatry Res 1997;69:203–206.
20. Wilson IC, Prange AJ Jr, McClane TK, et al. Thyroid-hormone enhancement of imipramine in nonretarded depressions. N Engl J Med 1970;282:1063–1067.
21. Reinhard D. Aggressive behavior associated with hypothyroid-ism. Canine Pract 1978;5:69.
22. Dodman NH, Mertens PA, Aronson LP. Animal behavior case of the month. Dogs were evaluated because of aggression. J Am Vet Med Assoc 1995;207:1168–1171.
23. Ferguson DC. Update on diagnosis of canine hypothyroidism. Vet Clin North Am Small Anim Pract 1994;24:515–539.
24. Scott-Moncrieff JC, Nelson RW. Change in serum thyroid-stim-ulating hormone concentration in response to administration of thy-rotropin-releasing hormone to healthy dogs, hypothyroid dogs, and euthyroid dogs with concurrent disease. J Am Vet Med Assoc 1998; 213:1435–1438.
25. Scott-Moncrieff JC, Nelson RW, Bruner JM, et al. Comparison of serum concentrations of thyroid-stimulating hormone in healthy dogs, hypothyroid dogs, and euthyroid dogs with concurrent disease. J Am Vet Med Assoc 1998;212:387–391.
26. Panciera DL, Post K. Effect of oral administration of sulfadia-zine and trimethoprim in combination on thyroid function in dogs. Can J Vet Res 1992;56:349–352.
27. Center SA, Mitchell J, Nachreiner RF, et al. Effects of propran-olol on thyroid function in the dog. Am J Vet Res 1984;45:109–111. 28. Miller AB, Nelson RW, Scott-Moncrieff JC, et al. Serial thyroid hormone concentrations in healthy euthyroid dogs, dogs with hypo-thyroidism, and euthyroid dogs with atopic dermatitis. Br Vet J 1992; 148:451–458.
29. Panciera DL, MacEwen EG, Atkins CE, et al. Thyroid function tests in euthyroid dogs treated withL-thyroxine. Am J Vet Res 1990; 51:22–26.
30. Panciera DL, Johnson GS. Plasma von Willebrand factor anti-gen concentration in dogs with hypothyroidism. J Am Vet Med Assoc 1994;205:1550–1553.
31. Gaskill CL, Burton SA, Gelens HC, et al. Changes in serum thyroxine and thyroid-stimulating hormone concentrations in epileptic dogs receiving phenobarbital for one year. J Vet Pharmacol Ther 2000; 23:243–249.
32. Langer G, Resch F, Aschauer H, et al. TSH-response patterns to TRH stimulation may indicate therapeutic mechanisms of antide-pressant and neuroleptic drugs. Neuropsychobiology 1984;11:211– 218.
33. de Montigny C, Agajanian GK. Tricyclic antidepressants: Long term treatment increases responsivity of rat forebrain neurons to se-rotonin. Science 1978;202:1303–1306.
34. Blier P, de Montigny C, Chaput Y. Modifications of the sero-tonin system by antidepressant treatments: Implications for the thera-peutic response in major depression. J Clin Psychopharmacol 1987;7: 24S–35S.
35. McTavish D, Benfield P. Clomipramine. An overview of its pharmacological properties and a review of its therapeutic use in ob-sessive compulsive disorder and panic disorder. Drugs 1990;39:136– 153.
36. Ma˚rtensson E, Axelsson R, Nyberg G. Pharmacokinetic prop-erties of the antidepressant drugs amitriptyline, clomipramine, and imipramine: A clinical study. Curr Ther Res 1984;36:228.
37. Lagorce JF, Thomes JC, Catanzano G, et al. Formation of mo-lecular iodine during oxidation of iodide by the peroxidase/H2O2 sys-tem. Implications for antithyroid therapy. Biochem Pharmacol 1991; 42(Suppl):S89–S92.
38. King JN, Maurer MP, Altmann BO, et al. Pharmacokinetics of clomipramine in dogs following single-dose and repeated-dose oral administration. Am J Vet Res 2000;61:80–85.
39. Rousseau A, Marquet P, Lagorce JF, et al. Thyroid accumulation and adverse effects of imipramine and desipramine in rats after
long-term administration. Pharmacology 1998;57:242–248.
40. Campos-Barros A, Meinhold H, Stula M, et al. The influence of desipramine on thyroid hormone metabolism in rat brain. J Phar-macol Exp Ther 1994;268:1143–1152.
41. Belshaw BE, Barandes M, Becker DV, et al. A model of iodine kinetics in the dog. Endocrinology 1974;95:1078–1093.
42. Wu SY. Thyrotropin-mediated induction of thyroidal iodothy-ronine monodeiodinases in the dog. Endocrinology 1983;112:417– 424.
43. Meij BP, Mol JA, Rijnberk A. Thyroid-stimulating hormone re-sponses after single administration of thyrotropin-releasing hormone
and combined administration of four hypothalamic releasing hormones in beagle dogs. Domest Anim Endocrinol 1996;13:465–468.
44. Morley JE, Brammer GL, Sharp B, et al. Neurotransmitter con-trol of hypothalamic-pituitary-thyroid function in rats. Eur J Pharmacol 1981;70:263–271.
45. Brady KT, Anton RF. The thyroid axis and desipramine treat-ment in depression. Biol Psychiatry 1989;25:703–709.
46. Prange AJ Jr. Psychotropic drugs and the thyroid axis: A review of interactions. Adv Biochem Psychopharmacol 1985;40:103–110.
47. Schlienger JL, Kapfer MT, Singer L, et al. The action of clo-mipramine on thyroid function. Horm Metab Res 1980;12:481–482.