ARTICLE
Governing Peripherally Inserted Central Venous
Catheters by Combining Continuous Performance
Improvement and Computerized Physician
Order Entry
Darren S. Migita, MDa,b, Liz Postetter, RN, BSNa, Susan Heath, RN, MN, NEA-BCa, Patrick Hagan, MHSAa, Mark Del Beccaro, MDa,b
aSeattle Children’s, Seattle, Washington;bDepartment of Pediatrics, University of Washington School of Medicine, Seattle, Washington
The authors have indicated they have no financial relationships relevant to this article to disclose.
What’s Known on This Subject
PICC usage has increased dramatically since the 1980s. However, the complication rate for such catheters is significant. The reduction of CABSIs through the reduction of cath-eter days is one approach to improving this patient safety metric.
What This Study Adds
Hospitals seeking to reduce PICC volumes or streamline PICC placement could benefit from the processes and techniques described here. Creating specific PICC-placement criteria combined with a method of governing such criteria helps promote sustained results. The use of CPI techniques provides the foundation for consensus building and ensures that solutions are created by local “experts.”
ABSTRACT
OBJECTIVE.Seattle Children’s in Seattle, Washington sought to establish governance over peripherally inserted central catheters. Preventing overuse and creating an efficient placement process were of paramount importance.
METHODOLOGY.We describe a process by which the marriage of continuous perfor-mance-improvement projects and computerized physician order entry has led to a reproducible reduction in peripherally inserted central catheter volumes and an increase in overall provider satisfaction with the ordering process. This was accom-plished by increasing daily awareness of central venous catheters, establishing peripherally inserted central catheter-specific insertion criteria, establishing a governing vascular-access service, and creation of a peripherally inserted central catheter-specific computerized order set.
RESULTS.After implementation of these measures, peripherally inserted central cathe-ter insertion volumes decreased by 33.4%; these results have been sustained over a period of 19 months. From August 2006 to October 2006, 48% of peripherally inserted central catheters were placed on the same calendar day of order entry, 37% within 24 hours of order entry, and 15% within 48 to 72 hours. Overall, provider satisfaction with the ordering process improved according to a Likert scale. Scores increased from 2.68 of 5 to 3.55 of 5 over a 9-month period. This result was statistically significant at the 95th percentile level according to the t-test method.
CONCLUSIONS.We conclude that properly constructed computerized order sets can be effective in altering physician ordering practices through standardization.Pediatrics 2009;123:1155–1161
S
INCE THEIR INTRODUCTION in the 1980s, peripherally inserted central catheter(PICC) usage has increased dramatically. After uncuffed central venous catheters (CVCs), PICCs are the second most common type of CVC. The purported potential advantages of PICCs as compared with traditional CVCs (Hickman, Broviacs, un-cuffed CVCs) include but are not limited to a minute risk of pneumothorax, lowered cost, reduced risk of hematoma formation after placement, ability to be used in an outpatient setting for adult and pediatric populations, and the ability to be placed at the patient’s bedside without general anesthesia or deep sedation.1
More recent data, however, indicate that PICCs are not without significant complications. Up to 50% of PICCs require radiologically guided insertion techniques requiring anesthesia,20.7% experience fracture,37% become
occluded,1 and 58% migrate ⱖ20 mm.4 Between 30% and 46% of all PICCs are removed because of a
complication before the completion of therapy.1,5–7 Other complications include deep venous thrombosis,
www.pediatrics.org/cgi/doi/10.1542/ peds.2007-3670
doi:10.1542/peds.2007-3670
Key Words
peripherally inserted central venous catheter, computerized physician order entry, continuous performance improvement, rapid process-improvement workshop
Abbreviations
PICC—peripherally inserted central catheter
CVC— central venous catheter CABSI— catheter-associated bloodstream infection
BSI— bloodstream infection PIV—peripheral intravenous line CPI— continuous performance improvement
CPOE— computerized physician order entry
VAS—vascular-access service SC—Seattle Children’s IR—interventional radiology RN—registered nurse
RPIW—rapid process-improvement workshop
MD— doctor of medicine TPN—total parenteral nutrition
Accepted for publication Aug 19, 2008 Address correspondence to Darren S. Migita, MD, 4800 Sand Point Way NE, Mail Stop T-1201, Seattle, WA 98105. E-mail: darren. [email protected]
extravasation and catheter-associated bloodstream in-fections (CABSIs).8–13 PICC infection rates are ⬃4 to
5.3/1000 line-days depending on the study. Given that nearly 80 000 CVC-associated bloodstream infec-tions (BSIs) occur in ICUs each year in the United States,8that the reported mortality from a CABSI may
be as high as 12% to 25%,8and that central line sepsis
is far more likely than peripheral intravenous line (PIV) sepsis (2% vs 0.04%),9PICCs can no longer be
considered a benign procedural intervention.
We describe a process by which a combination of continuous performance-improvement (CPI) mea-sures and computerized physician order entry (CPOE) led to the creation of a new PICC line order set. This order set combined with the creation of a specific vascular-access service (VAS) resulted in increased provider satisfaction with the ordering process, de-creased PICC use, and reproducibility of desired changes.
Seattle Children’s (SC) is a 250-bed teaching hospital located in Seattle, Washington. At SC, we were faced with 3 major issues surrounding PICC lines: infection, overuse, and confusion regarding the PICC ordering pro-cess.
Reducing CABSIs is an important patient safety benchmark. Approximately 42% of all central line infections at SC occurred in PICC lines. Between 2003 and 2006, an average of 71 PICCs were placed per month. Ordering providers were not required to indi-cate the reason for PICC placement, and institutional criteria for placement did not exist. PICCs were or-dered via CPOE and placed either by interventional
radiology (IR) or a registered nurse (RN)-staffed “IV team.” The ordering provider was responsible for de-termining the mode of insertion (IR versus bedside), contacting the proceduralist, coordinating PICC place-ment with other procedures requiring anesthesia, and coordinating care directly with the patient’s primary nurse. Significant dissatisfaction with the PICC order-ing process resulted.
METHODS
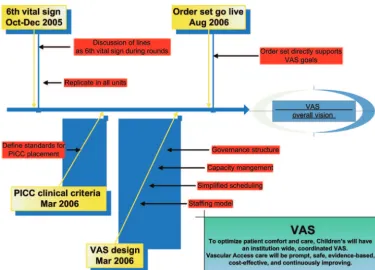
We sought to create a system of governance over PICCs by creating a centralized VAS. The VAS was designed to be an institution-wide, coordinated, gov-ernance structure aimed directly at streamlining and standardizing all aspects of PICC lines from insertion to removal. Interventions were accomplished in stages within the SC CPI framework. A series of 3 rapid process-improvement workshops (RPIWs) were com-pleted over a 9-month period (Fig 1). Participants in RPIWs included a multidisciplinary group of staff from various areas of the hospital including doctors of med-icine (MDs), RNs, housestaff, and nurse practitioners. Workshops occurred over 3 to 5 days with participants being relieved from all other duties. The hallmark of RPIWs is that solutions are “bottom up,” that is, local experts are responsible for building the specific solu-tions. In addition, the team is given the authority to institute change with the support of senior manage-ment.
FIGURE 1
Workshop 1: The “Sixth Vital Sign”: 6 Questions to Ask Each Day if Your Patient has a CVC
The goal of this workshop was to ensure that central lines are included as part of the daily discussion during morning patient rounds. We recognized that the success of this and all future projects depended on increasing staff awareness of lines. Housestaff were prompted to cover the following questions daily on rounds:
1. Can the line be removed?
2. Can we change intravenous medications to oral?
3. Can the patient be fed enterally?
4. Can we decrease blood draws?
5. Can we bundle tubing changes with blood draws?
6. What does the site or dressing look like today?
This process was further supported in the ICUs by reproducing these questions on daily progress notes. In addition, medical unit RNs are required to give a synop-sis on their patients’ central lines on intake forms as well as on daily progress notes.
Workshop 2: PICC Clinical Criteria: Creation of Insertion Standards for PICCs
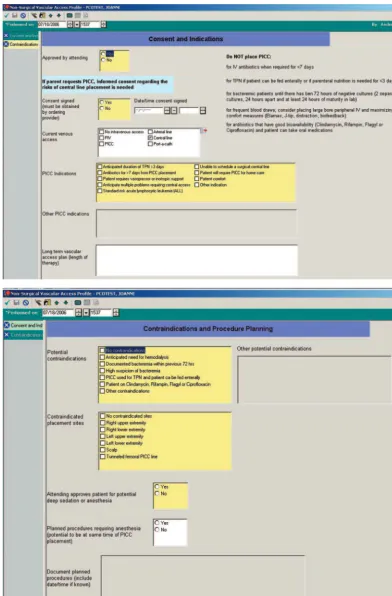
The PICC clinical criteria workshop team established a set of general and specific criteria for PICC lines (Fig 2). Before this workshop, no specific standards guiding PICC usage existed at SC.
The general criteria remind practitioners that PIVs should be used whenever possible and reinforce the most common indications for PICCs. These include the need for home intravenous infusions and patients with multiple medical issues requiring central venous access. Specific PICC criteria were subdivided into 4 sections: total parenteral nutrition (TPN), antibiotics, chemother-apy, and critical care. Because PICCs are often placed for antibiotics or TPN, the team sought to specifically stan-dardize PICC usage in these situations. The team deter-mined that PICCs would be used in patients requiring ⬎7 days of antibiotics or⬎3 days of TPN. Patients who did not meet these criteria would instead be candidates for PIVs. It should be noted that placing PICCs for pa-tients requiring frequent blood draws was purposely omitted from the criteria. This was consciously done FIGURE 2
because of the increased risk of CABSIs in patients with CVCs.
Contraindications to PICC lines were also established by the workgroup. These contraindications were guided by both the best available literature evidence and local expert opinion. PICCs would not be placed for TPN if the patient could be fed enterally or in those whose antibiotics could be administered orally. Potential hemodialysis patients should not receive PICCs because of the risk of thrombosing vessels, which may later be required for placement of a permanent hemodialysis line. Patients with active or recent bacteremia ought not to receive PICCs because of the potential risk of coloniz-ing the newly placed line.
Workshop 3: Creation of the VAS
The third workshop was the VAS design event in which the specifics of the VAS were created. The workshop’s goals were to create a staffing model, simplify scheduling for PICCs, and create a structure that reliably governed the insertion of PICC lines.
The VAS is staffed by a group of 7 RNs representing 5.8 full-time employee equivalents. The VAS RNs are available for all hours of the day except between 2AM
and 6AM. Medication infusions and blood draws through
PICCs are performed by the patient’s bedside RN. Their primary responsibilities of the VAS with regard to PICCs include the following:
1. individual assessment of each patient to determine their specific PICC needs;
2. placement of the PICC line on the unit (medical, surgical, hematology/oncology);
3. arrangement of IR placement if necessary;
4. ensuring appropriate sedation for the patient and co-ordination with an anesthesiologist if deep sedation or anesthesia is required;
5. coordination of the process with the patient’s primary nurse;
6. offering alternatives (eg, PIVs) to the practitioner if the PICC request does not meet criteria;
7. coordination of PICC placement with other proce-dures requiring anesthesia; and
8. providing consultation if the PICC is malfunctioning, requires repair, or requires removal.
Before the creation of the VAS team, individual practi-tioners were responsible for coordination of the above-mentioned tasks. Given that SC is a busy teaching hospital, completion of these tasks in a timely manner is often difficult. Moreover, trainees (resident physicians) are at times unfamiliar with specific hospital procedures, which, in turn, creates additional delays, errors, and dissatisfac-tion. Centralizing and standardizing those processes within the VAS was a requirement for improvement.
After consent is obtained by the ordering physician, the VAS places all bedside PICCs by using the modified Seldinger technique. In addition, all VAS staff have been trained to use sonographic guidance for initial venous
cannulation. If necessary, a single dose of a benzodiaz-epine is used for conscious sedation. Conscious sedation is ordered by the MD, and the patient is monitored and recovered by the bedside RN. Final PICC tip position is verified by obtaining an anterioposterior chest film that visualizes the radio-opaque tip within the region of the superior vena cava. This radiograph is reviewed by both the VAS RN and the ordering physician after placement. The VAS RN adjusts the PICC tip position to a central location before any infusion being started through the line. The line is not used until there is a physician order to do so. If necessary, additional verification of the PICC tip within the intravascular space can be accomplished by drawing blood directly from the PICC. At SC we do not use PICCs that are not central because of the in-creased complication rates of such “midline” catheters.11
If bedside placement is anticipated to be technically difficult (eg, chronic medical patient with poor periph-eral access, inability to visualize periphperiph-eral vasculature), if the patient requires deep sedation, or if bedside place-ment fails after 2 attempts, the VAS refers the case to the interventional radiologist for PICC placement under flu-oroscopic guidance. Deep sedation/anesthesia is admin-istered by a pediatric anesthesiologist in the IR suite. Central catheter tip position is definitively verified under fluoroscopy and documented in the MD procedure note. For the period between October 2005 and June 2007, 60.9% of PICCs were placed at the bedside by the VAS, and 39.1% were placed by IR. When bedside placement was attempted by the VAS, the success rate was 85.6% for the period September 2007 to July 2008.
Project: Creation of the PICC Order Set
The final project was to design an order set that sup-ported the work of the first 3 workshops (Fig 3). The “PICC-placement order set” is the sole method by which the MD provides the minimal necessary information that the VAS requires to place the PICC. Within the order set resides the data the VAS requires to verify that place-ment meets criteria, verify that there are no contraindi-cations to placement, avoid placement in certain ex-tremities, and coordinate PICC placement with other procedures that require anesthesia. In addition, the or-der set verifies that consent for the procedure has been obtained. The order set cannot be electronically signed unless all required fields are completed. In essence, the order set is a piece of standard work that ensures that the PICC-ordering process is accomplished by a reliable method.
If the PICC request does not meet criteria or if contra-indications are present, the VAS RN offers other access alternatives to the ordering provider. The VAS RNs have the authority to deny inappropriate PICC insertions. Cases that need higher-level arbitration are few and arise most often when there is a potential contraindication to PICC placement in a patient who has no other venous access options. Cases of this nature are directed either to the medical director of line management or the RN director of VAS, one of whom is available at all times.
fields indicating the reasons for discontinuation of the catheter (ie, completion of therapy, suspected infec-tion, thrombosis, leakage, or other malfunction).
To ensure timeliness of placement, the VAS is notified of the new order in 2 ways. First, completion of the order set triggers an alphanumeric page to the on-call VAS RN; FIGURE 3
second, completion of the order set also becomes an active issue on the VAS electronic in-box. All fields within both order sets are downloadable. This allows retrospective analysis of PICC volumes, reasons for placement, duration of placement, and reasons for dis-continuation. Such data sets were not previously avail-able at SC.
RESULTS AND DISCUSSION
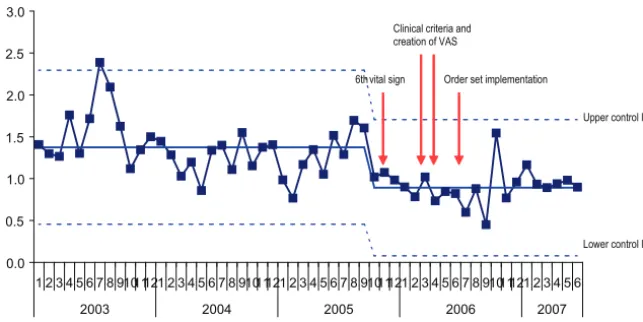
The above-mentioned workshops were completed in a serial fashion (see Fig 1). The sixth vital sign project was initiated in October 2005 and standardized across the entire hospital by December 2005; clinical criteria and the VAS infrastructure were established in March 2006; and the PICC order set was implemented in August 2006. There has been a significant reduction in the num-ber of PICC lines placed. From January 2003 to Septem-ber 2005 the rate of PICC placement was 1.37 lines per 100 patient-days (mean: 71 PICCs placed per month; upper control limit(UCL): 116 PICCs placed per month; lower control limit (LCL): 25 PICCs placed per month). From October 2005 to June 2007 the rate of PICC place-ment was 0.913 lines per 100 patient-days (mean: 50 PICCs placed per month; UCL: 89 PICCs placed per month; LCL: 10 PICCs placed per month) (see Fig 4). This represents a reduction of 33.36%. Volume data were obtained by retrospective analysis of SC charge codes for PICC insertions.
Individual chart reviews were conducted for the time frame December 2004 to March 2005 (n ⫽ 120). The purpose of these reviews was to verify documentation justifying PICC placement. On the basis of these chart reviews, 13.3% of PICCs during this time period would not have met criteria that were later established in March 2006. Therefore, the actual decrease in the vol-ume of PICC insertions was higher than predicted from the implementation of criteria alone. There seems to be a synergistic effect between the creation of defined strin-gent criteria and an increased daily awareness of CVCs. Increasing provider awareness of the potential dangers of CVCs promotes increased use of PIVs rather than PICCs. Creation of a VAS with the authority to stop unnecessary placements and the ability to offer other
venous access alternatives additionally reduces PICC volumes.
Increased provider satisfaction with the PICC order-ing process was also a targeted metric. Preimplemen-tation surveys were collected in March 2006, and postimplementation surveys were collected in December 2006. Data were collected via online survey techniques (Survey Monkey). All results are expressed on a Likert scale of 1 to 5 (1⫽very dissatisfied, 5⫽very satisfied). Respondents in both preimplementation and postimple-mentation surveys were given 7 days to respond, and the response rate for each survey was 15.5% (n⫽93) and 11.7% (n⫽ 70), respectively. Resident physicians and staff RNs from all inpatient medical and surgical units were surveyed. Significant improvements were seen for the question, “Overall, how satisfied are you with the current process of scheduling PICC line placement?”: from 2.68 (March 2006) to 3.55 (December 2006). This result was statistically significant at the 95th percentile level according to thet-test method.
The VAS has been able to insert PICCs in a timely fashion. From August 2006 to October 2006, 48% of PICCs were placed on the same calendar day of order entry, 37% within 24 hours of order entry, and 15% within 48 to 72 hours. Of note, all patients without intravenous access at the time of PICC order entry had their PICCs placed on the same calendar day. Although postimplementation surveys did not specifically ask about satisfaction with timeliness of placement, we pos-tulate that providers were satisfied with these time-frames given the response to the question, “Overall, how satisfied are you with the current process of scheduling PICC line placement?”
CONCLUSIONS AND FUTURE IMPLICATIONS
We have described a process by which the marriage of CPI methodology and CPOE has led to a reproducible reduction in PICC volumes and an increase in overall provider satisfaction with the ordering process. The sus-tainability of these efforts is as much because of the consensus-building nature of RPIWs as it is the forced function that the order set represents. The RPIW pro-vides the forum that allows local experts to debate in
0.0 0.5 1.0 1.5 2.0 2.5 3.0
1 2 3 4 5 6 7 8 91011121 2 3 4 5 6 7 8 91011121 2 3 4 5 6 7 8 91011121 2 3 4 5 6 7 8 91011121 2 3 4 5 6
2003 2004 2005 2006 2007
6th vital sign Clinical criteria and creation of VAS
Order set implementation
Upper control limit
Lower control limit FIGURE 4
detail the issue at hand. Achieving initial consensus makes creation of a durable solution more likely. The PICC order set allows providers to order a PICC by a single standardized method. Only relevant information is passed via the order set, and all relevant information must be transmitted through the use of required fields. Without CPOE, the communication between the order-ing provider and the VAS remains subject to omissions, errors, and delays.
At SC, there are a series of BSI-reduction initiatives in place, including the use of insertion and maintenance bundles, reduction of line openings, and antibiotic-im-pregnated catheters in addition to the efforts to reduce usage of these lines. Although we cannot assume a ca-sual relationship, there has been a steady reduction of BSIs coincident with the reduction of PICC line place-ments and these other initiatives. The BSI rate for the hospital has fallen from a rate of 6.4/1000 central line-days (September 2005) to 2.4/1000 central line-line-days (October 2007). Abovementioned rates are derived from all CVCs placed at SC. All CABSIs at SC are identified per the most recent Centers for Disease Control criteria.
In addition to the order set’s ability to standardize placement criteria, the order set has significant value as a teaching tool. At any busy academic medical center, training resident physicians is a particular challenge. Balancing a heavy workload, honoring work-hour re-strictions, and providing educational didactics is often difficult and sometimes not possible. The order set allows for precisely relevant real-time education as to the indi-cations and contraindiindi-cations of PICCs. In this way, a “required field” is recapitulated as an important teaching moment. Required fields also have the added benefit of maintaining patient safety by alerting the ordering phy-sician and the VAS team to any existing or potential contraindications to PICC placement.
Future uses of such “teaching order sets” abound. The techniques (both CPI and CPOE) we have described could be adopted for the management of specific pedi-atric disease states (eg, fever without focus, urinary tract infection, dehydration). There may also be relevant ap-plications for diagnostic imaging or other blood test or-dering. For example, a properly constructed order set could help guide the clinician to that imaging study with the highest pretest probability. Navigation through a particular disease process, whether by trainees or vet-eran clinicians, is often left to the “art of medicine.”
Clearly, medicine as an art must continue to exist; how-ever, we believe our work illustrates a viable and durable method of delivering health care through standardiza-tion. It is this standardization combined with multiple “plan-do-check-act” cycles that provides the basis for future improvement.
REFERENCES
1. Thiagarajan RR, Ramamoorthy C, Gettmann T, Bratton SL. Survey of the use of peripherally inserted central venous cath-eters in children. Pediatrics. 1997;99(2). Available at: www.pediatrics.org/cgi/content/full/99/2/e4
2. Cardella JF, Fox PS, Lawler JB. Interventional radiologic place-ment of peripherally inserted central catheters. J Vasc Interv Radiol.1993;4(5):653– 660
3. Chow J, Friedman C, MacArthur R, et al. Peripherally inserted central catheter (PICC) fracture and embolization in the pedi-atric population.J Pediatr.2003;142(2):141–144
4. Forauer AR, Alonzo M. Change in peripherally inserted central catheter tip position with abduction and adduction of the up-per extremity.J Vasc Interv Radiol.2000;11(10):1315–1318 5. Fong NI, Holtzman SR, Bettmann MA, Bettis SJ. Peripherally
inserted central catheters: outcome as a function of the oper-ator.J Vasc Interv Radiol.2001;12(6):723–729
6. Tolomeo C, Mackey W. Peripherally inserted central catheters (PICCs) in the CF population: one center’s experience.Pediatr Nurs.2003;29(5):355–359
7. Walshe LJ, Malak SF, Eagan J, Sepkowitz KA. Complication rates among cancer patients with peripherally inserted central catheters.J Clin Oncol.2002;20(15):3276 –3281
8. Centers for Disease Control and Prevention. Guidelines for the prevention of intravascular catheter-related infections.MMWR Recomm Rep.2002;51(RR-10):1–29
9. Collignon PJ, Dreimanis DE, Beckingham WD, Roberts JL, Gardner A. Intravascular catheter bloodstream infections: an effective and sustained hospital-wide prevention program over 8 years.Med J Aust.2007;187(10):551–554
10. Mermel LA, Farr BM, Sherertz RJ, et al. Guidelines for the management of intravascular catheter-related infections.Clin Infect Dis.2001;32(9):1249 –1272
11. Racadio JM, Doellman DA, Johnson ND, Bean JA, Jacobs BR. Pediatric peripherally inserted central catheter: complication rates related to catheter tip location. Pediatrics.2001;107(2). Available at: www.pediatrics.org/cgi/content/full/107/2/e28 12. Allen AW, Megargell JL, Brown DB, et al. Venous thrombosis
associated with the placement of peripherally inserted central catheters.J Vasc Interv Radiol.2000;11(10):1309 –1314 13. Bivins MH, Callahan MJ. Position-dependent ventricular
tachycardia related to a peripherally inserted central catheter.
DOI: 10.1542/peds.2007-3670
2009;123;1155
Pediatrics
Darren S. Migita, Liz Postetter, Susan Heath, Patrick Hagan and Mark Del Beccaro
Entry
Continuous Performance Improvement and Computerized Physician Order
Governing Peripherally Inserted Central Venous Catheters by Combining
Services
Updated Information &
http://pediatrics.aappublications.org/content/123/4/1155 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/123/4/1155#BIBL This article cites 11 articles, 1 of which you can access for free at:
Subspecialty Collections
_management_sub
http://www.aappublications.org/cgi/collection/administration:practice
Administration/Practice Management
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2007-3670
2009;123;1155
Pediatrics
Darren S. Migita, Liz Postetter, Susan Heath, Patrick Hagan and Mark Del Beccaro
Entry
Continuous Performance Improvement and Computerized Physician Order
Governing Peripherally Inserted Central Venous Catheters by Combining
http://pediatrics.aappublications.org/content/123/4/1155
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.