Renal Function After Pediatric Cardiac Transplantation:
The Effect of Early Cyclosporin Dosage
Tim S. Hornung, MRCP*; Christian G.E.L. de Goede, MRCP*; Chris O’Brien, MRCP‡; Nadeem E. Moghal, MRCP§; John H. Dark, FRCS储; John J. O’Sullivan, MRCP*
ABSTRACT. Background. There is little data on renal function in pediatric heart transplant recipients. Early rejection is a major concern and most units run high cyclosporin A (CyA) levels during the 2 to 3 months after transplantation. We sought to document long-term renal function after transplantation and to assess influence of early CyA levels.
Methods. We reviewed all of our pediatric trans-plants between June 1985 and August 1998 who survived longer than 6 months (nⴝ54). Glomerular filtration rate (GFR) was estimated at 1, 2, 4, and 8 years posttransplan-tation using the Schwartz formula:
GFR (mL/min/1.73m2)ⴝ[Ht(cm)/creatinine(mol/
L)]ⴛX
We also analyzed whether change in renal function correlated with trough CyA levels.
Results. Median age at transplant was 4 years and median follow-up was 5 years. Survival rates were 87% at 1 year and 80% at 5 years. Mean GFR pretransplant was 79ⴞ19 mL/min/1.73 m2, reflecting prerenal impairment.
One year later, mean GFR was 72 mL/min/1.73 m2; after 2
years it was 65 mL/min/1.73 m2, after 4 years (nⴝ35) it
was 60 mL/min/1.73 m2, and after 8 years (nⴝ14) it was
57 mL/min/1.73 m2. CyA levels during the first 2 months
correlated with the change in GFR during the first year (r2ⴝ0.21).
Conclusions. This study demonstrates for the first time that decline in renal function after heart transplan-tation correlates with early CyA exposure; this dysfunc-tion persists even when CyA doses are subsequently reduced.Pediatrics2001;107:1346 –1350;heart transplant, kidney function, cyclosporin A.
ABBREVIATIONS. GFR, glomerular filtration rate; CyA, cyclo-sporin A.
D
espite widespread recognition of the nephro-toxic effects of cyclosporin therapy,1– 4 there is little data available regarding long-term renal function in pediatric cardiac transplant recipi-ents. Because of concerns about early cardiac rejec-tion, most units run high cyclosporin levels duringthe first months after transplantation, and these lev-els are often considerably higher than the levlev-els used after renal transplantation. The glomerular filtration rate (GFR) is often reduced before transplantation in this population because of low cardiac output and poor renal perfusion. Restoration of renal perfusion after transplantation should improve GFR; however, in many patients this is not the case. The purpose of this study was to document the progression of renal dysfunction in survivors of pediatric heart transplan-tation and to assess the influence of cyclosporin ex-posure.
PATIENTS AND METHODS
We retrospectively reviewed all patients who underwent car-diac transplantation at⬍16 years of age at our center between June 1985 and August 1998 who had structurally normal kidneys by ultrasound and who survived for⬎6 months after transplan-tation. Height and plasma creatinine was documented before transplantation and at 1 month, 1 year, 2 years, 4 years, and 8 years posttransplantation. Height was measured using a Harpenden wall-mounted stadiometer, and creatinine was measured from whole blood using a homogeneous enzyme immunoassay tech-nique (Emit 2000, Syva.Company, Cupertino, CA). GFR was esti-mated using the modified Schwartz formula5,6:
GFR (mL/min/1.73m2)
⫽[Height (cm)/creatinine (mol/L)]⫻X
Immunosuppression Regime
Patients initially receive combination immunotherapy with cy-closporin, azathioprine (2 mg/kg/d), and prednisolone (0.2 mg/ kg/d). Children⬍5 years old do not receive steroids after the first 24 hours. Cyclosporin dosage is adjusted aiming to achieve 12-hour trough levels between 300 to 400 ng/mL during the first 6 weeks after transplantation and 100 to 200 ng/mL thereafter. Antithymocyte globulin is also routinely given during the first week after transplantation, with the dosage being adjusted to keep the T-cell count below 50 000/mL. Prednisolone is routinely stopped 6 weeks after transplantation to minimize effects on growth7; very few patients required maintenance steroids.
There-after, patients are maintained on cyclosporin⫾azathioprine (de-pending on the white cell count). The cyclosporin preparation used was changed from Sandimmun to Neoral for all of our patients in July 1995, therefore, 17 patients received only Neoral. Neoral is a preconcentrate formulation of cyclosporin that under-goes a microemulsification process in the presence of gastrointes-tinal fluid and has less patient-to-patient pharmacokinetic vari-ability. Patients who were previously taking Sandimmun were prescribed an initial Neoral dose 20% lower than their Sandim-mun dose, and this was retitrated according to 12-hour trough levels.
Cyclosporin exposure was assessed in terms of mean serum cyclosporin trough levels and was divided into 3 periods: 1) the first 2 months after transplantation; 2) the next 10 months, ie, the remainder of the 1st year; and 3) the period from the end of the 1st year onward. The calculation of mean cyclosporin A (CyA) trough
From the *Department of Paediatric Cardiology, Freeman Hospital, ‡De-partment of Paediatrics, Royal Victoria Infirmary, §De‡De-partment of Paediat-ric Nephrology, Royal Victoria Infirmary, and储Department of Cardiotho-racic Surgery, Freeman Hospital, Newcastle upon Tyne, United Kingdom. Received for publication Jan 6, 2000; accepted Oct 12, 2000.
Reprint requests to (T.S.H.) Adult Congenital Cardiac Centre, Toronto General Hospital, Elizabeth St, Toronto, Canada, M5A 2C4. E-mail: tim.hornung@uhn.on.ca
level was performed using all available cyclosporin levels to de-termine the average trough level during a particular period, as follows:
(trough level 1⫻number of days at this level)
⫹(trough level 2⫻number of days at this level), etc. total number of days in the period under consideration
We assessed whether there was a correlation between cyclo-sporin exposure and decline in renal function, and also between decline in renal function and the use of other drugs. Blood pres-sure meapres-surements were compared with age-matched population figures to determine whether uncontrolled hypertension (defined as blood pressure⬎95th percentile for age and height) correlated with decline in renal function.
Statistical Analysis
Estimated GFR values are expressed as group mean⫾standard deviation. Group mean values were analyzed using analysis of variance and by comparing 95% confidence limits of group means. Correlation was assessed using linear regression analysis.
RESULTS
During the study period, 62 patients underwent cardiac transplantation, of whom 54 (27 boys) sur-vived beyond 6 months after transplantation and were included in the study. Median age at transplan-tation of study patients was 4 years (range: 0.3–15 years), median length of follow-up was 5.2 (range: 0.8 –11 years). Overall survival rates were 87% at 1 year and 80% at 5 years. Cardiac function was good in all cases except 2, both of whom developed left ventricular dysfunction at a late stage secondary to hypertension associated with severe renal impair-ment.
Height range for the whole group was reduced slightly compared with the normal population (Fig 1); however, the 12 patients who have reached 16 years of age show a normal range of heights. Al-though numbers are small, this suggests a normal spread of final heights and raises the possibility that the lower percentiles seen in the population as a whole represent growth delay rather than reduced growth potential.
Renal Function
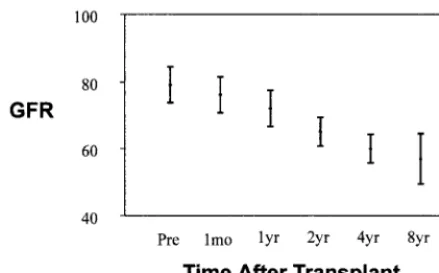
Mean GFR before transplantation was 79 ⫾ 19 mL/min/1.73 m2, the low value partly reflecting the
subgroup with low cardiac output and reduced renal perfusion. At 1 month after transplantation, the mean GFR had fallen slightly to 76 ⫾ 19 mL/min/ 1.73 m2.
Figure 2 shows that 1 year after transplantation, there was a fall in mean GFR to 72 ⫾ 20 mL/min/ 1.73 m2(P ⫽ .05 of 0 years vs 1 years) and after 2 years an additional fall to a mean of 65 ⫾ 15 mL/ min/1.73 m2(P⫽.03 of 2 years vs 1 years); there was no correlation between pretransplant GFR and post-transplant GFR. After this, the decline in renal func-tion then seemed to slow down somewhat, such that after 4 years (35 patients), the mean GFR is 60⫾ 14 mL/min/1.73 m2, and after 8 years (14 patients) the mean GFR is 57 ⫾ 14 mL/min/1.73 m2. Figure 3 shows this data in terms of the number of patients with varying degrees of renal impairment at each time point. At the most recent follow-up, 1 patient with severe renal failure had died having declined dialysis; another is expected to start dialysis immi-nently, and 2 more have severely impaired renal function (GFR⬍30 mL/min/1.73 m2).
Cyclosporin Levels
Mean trough cyclosporin levels were 345 ⫾ 52 ng/mL (range: 232– 454 ng/mL) during the first 2 months after transplantation. For the remainder of the first year, the mean levels were 215⫾64 ng/mL (137– 497 ng/mL), and after the first year 159 ⫾ 27 ng/mL (113–254 ng/mL). Cyclosporin levels during the first 2 months showed a significant correlation with change in GFR during the first year after trans-plantation (P ⫽ .0007, r2⫽ 0.21; Fig 4). There is an additional correlation between cyclosporin levels during the remainder of the first year and reduction in GFR during the second year after transplantation (P ⫽ .03, r2⫽ 0.13). The additional decline in GFR after the second year was not significantly correlated with cyclosporin levels, although numbers were small and there was less variation in cyclosporin levels between patients.
The rate of decline of renal function did not differ significantly between the group initially treated with Sandimmun (n⫽37, mean CyA trough level in first
2 months⫽349 ng/mL, mean change in GFR during the first year⫽ 7 mL/min/1.73 m2) and the group initially treated with Neoral (n ⫽ 17, mean CyA trough level in first 2 months ⫽ 345 ng/mL, mean change in GFR during first year ⫽ 9 mL/min/1.73 m2), although median length of follow-up was only 2.4 years in the neoral group. We found no correla-tion between deterioracorrela-tion in renal funccorrela-tion and use of other drugs, age at transplantation, or sex. De-tailed blood pressure data were available for 49 of 52 patients and showed that hypertension was frequent in this population, 82% of patients having been pertensive at some stage. The mean number of hy-pertensive days during the first year was 50 ⫾ 81 days; there was no correlation between decline in renal function and number of hypertensive days (P⫽.91). Hypertension after the first year was rare, although the 2 patients with the most severe renal dysfunction developed significant late hypertension requiring treatment with⬎1 antihypertensive agent.
DISCUSSION
Although cyclosporin is known to adversely effect renal function,1– 4 there is very little data regarding its effects after heart transplantation in children. We now present data from our complete population of pediatric transplant survivors which shows that moderate renal dysfunction is a near universal prob-lem in this population, and that in a minority, the degree of renal impairment is severe. We also dem-onstrate a correlation between early cyclosporin lev-els and rate of decline of renal function, allowing us to suggest safe cyclosporin trough levels for this population.
Prevalence of Renal Impairment
Our pediatric transplant population is maintained on a combination of cyclosporin ⫾ azathioprine, without the use of steroids. It has been our expecta-tion that this regimen would maximize growth po-tential, while allowing adequate immunosuppres-sion.7–9The dosage of cyclosporin required to avoid rejection is, however, higher with such a regimen. Although overall survival figures are very good (80% 5-year survival), 2 of our 54 transplant survivors have developed end-stage renal disease, and an ad-ditional 2 have severe impairment of renal function with expected progress to end-stage renal disease;
this represents 7% of our population with severe renal impairment. This data differs from the most recent report of pediatric heart transplant results from the International Society for Heart and Lung Transplantation,10 which shows 5-year survival of 65% but no patients with severe renal impairment (defined as a creatinine⬎2.5 mg/mL). Although it is possible that this discrepancy is attributable to un-derreporting to a voluntary registry or to differing definitions of severe renal impairment, it is also pos-sible that, particularly earlier on in our experience, we have been running cyclosporin levels higher than many other centers. When compared with Interna-tional Society for Heart and Lung Treatment registry figures, the results of our protocol seem to be better overall survival, but higher rates of renal impair-ment. Studies of adult heart transplant recipients are comparable to our experience, with a prevalence of end-stage renal disease of 3% to 10%.11–17
Influence of Cyclosporin Level
This study demonstrates a correlation between cy-closporin exposure during the first year and decline in GFR. This suggests that the maintenance of high early cyclosporin levels is an important factor in the renal damage seen in this group and that lower levels may result in less renal damage. Previous studies in adult populations have found no such correlation, but have often studied isolated trough levels taken at, for example, 3 or 12 months. In our study, we have used all available cyclosporin levels to determine the average trough level during a par-ticular period; we believe this has enabled us to give a more accurate estimation of the total cyclosporin exposure. Despite this, our results provide only a relatively weak correlation (r2⫽0.21), which is likely to be attributable to the remaining inaccuracies asso-ciated with the use of 12-hour trough cyclosporin levels. It is recognized that cyclosporin trough levels are an imperfect way of controlling dosage and, like-wise, estimation of total cyclosporin load. It is pos-sible that a more detailed cyclosporin profile would allow more accurate delineation of the renal effects of cyclosporin; however, in a retrospective study such as this, the only consistent measure available to us, as in most transplant centers, is the trough cyclosporin level. Furthermore, a detailed cyclosporin profile would require more blood samples to be taken and more time to be spent in hospital, raising ethical dilemmas particularly in the pediatric population.
Although it is likely that genetic influences have some influence on renal prognosis in this group,11 we believe that cyclosporin load is important and that maintenance of the lowest possible cyclosporin levels will be beneficial in terms of long-term renal function. These data suggest that an early mean cy-closporin trough level of 300 ng/mL is not associated with development of renal impairment; in fact most patients with mean levels⬍300 ng/mL showed an improvement in renal function as would be expected with restoration of normal cardiac output and renal perfusion. Trough cyclosporin levels ⬎300 ng/mL are associated with progressively greater risk of re-nal impairment in this population. We, therefore,
suggest that the target trough cyclosporin level dur-ing the aggressive period of early immunosuppres-sion should be 300 ng/mL or less.
Progression of Renal Impairment
Our data would suggest that although our immu-nosuppression regime results in excellent survival figures, there is a price to pay in terms of progressive impairment of renal function. The data demonstrate an early and rapid decline in renal function in the first 2 years after transplantation, with an additional, slower decline in subsequent years, despite lower maintenance cyclosporin levels. This differs from the pattern reported by several other groups in adult transplant recipients, in whom there is an early de-cline in renal function, but a subsequent pla-teau.13,18,19
It is too early to predict with confidence the num-ber of children in this group that will eventually develop severe renal impairment. The observed con-tinuing decline in renal function suggests that the early cyclosporin toxicity has caused a significant renal insult, such that progressive ongoing damage may develop as a result of hyperfiltration injury.20
Study Limitations
This study is a retrospective study that uses an indirect estimate of renal function and relies on
12-hour trough cyclosporin levels for estimation of total cyclosporin load. The accuracy of the study and the statistical power could potentially be improved by the direct measurement of glomerular filtration rate and by more detailed cyclosporin profiles. This sort of monitoring would, however, be both expensive and time-consuming and would result in an ever greater amount of time spent in hospital for a group of children who are already frequent visitors to the outpatient department.
CONCLUSION
This study is important because it demonstrates for the first time that decline in renal function after heart transplantation is correlated with early cyclo-sporin exposure.
These long-term data have had a significant im-pact on our overall immunosuppressive strategy in the pediatric age group, with individualization of immunosuppressive regimes to achieve the lowest cyclosporin level that will prevent rejection for each patient. We have also established a joint cardiac– renal clinic to improve the renal monitoring and outcome of this population. The use of alternative immunosuppressive agents may, in the future, result in an improved renal outlook for this patient group.
Fig 3. Change in GFR with time, expressed as group values.
ACKNOWLEDGMENT
We thank Dr Malcolm Coulthard for his assistance with review-ing the manuscript.
REFERENCES
1. Humes HD, Coffman T, Halderman H, Mihatsch M, Henry M, Wait RB. Cyclosporin nephrotoxicity: a workshop to discuss mechanisms, diag-nosis and treatment.Transplant Proc. 1988;20(suppl 3):833– 840 2. Youngleman DF, Kahng KU, Rosen BD, Dresner LS, Wait RB. Effects of
chronic cyclosporin administration on renal blood flow and intrarenal blood flow distribution.Transplantation. 1991;51:503–509
3. Bennett WM, DeMattos A, Meyer MM, Andoh T, Barry JM. Chronic cyclosporin nephropathy: the Achilles’ heel of immunosuppressive therapy.Kidney Int. 1996;50:554 –574
4. Mason J. The pathophysiology of Sandimmune (cyclosporine) in man and animals.Paediatr Nephrol. 1990;4:554 –574
5. Schwartz GJ, Haycock GB, Edelman CM, Spitzer A. A simple estimate of glomerular filtration rate in children derived from body length and plasma creatinine.Pediatrics.1976;58:259 –263
6. Schwartz A, Brion LP, Spitzer A. The use of plasma creatinine concen-tration for estimating glomerular filconcen-tration rate in infants, children and adolescents.Pediatr Clin North Am.1987;34:571–590
7. Au J, Gregory JW, Colquhoun IW, et al. Paediatric cardiac transplanta-tion with steroid-sparing maintenance immunosuppression.Arch Dis Child. 1992;67:1262–1266
8. Superina RA, Zangari A, Acal L, DeLuca E, Zaki A, Kimmel S. Growth in children following liver transplantation.Pediatr Transplant. 1998;2: 70 –75
9. Birkeland SA, Larsen KE, Rohr N. Pediatric renal transplantation with-out steroids.Pediatr Nephrol. 1998;12:87–92
10. Boucek MM, Novick RJ, Bennett LE, Fiol B, Keck BM, Hosenpud JD. The
registry of the international society of heart and lung transplantation: second official pediatric report–1998.J Heart Lung Transplant.1998;17: 1141–1160
11. Woolfson RG, Neild GH. Cyclosporin nephrotoxicity following cardiac transplantation.Nephrol Dial Transplant. 1997;12:2054 –2056
12. Greenberg A, Thompson ME, Griffith BJ, et al. Cyclosporine nephro-toxicity in cardiac allograft patients—a seven year follow-up. Transplan-tation. 1990;50:589 –593
13. Van Gelder T, Balk AH, Zietse R, Hesse C, Mochtar B, Weimar W. Renal insufficiency after heart transplantation: a case control study.Nephrol Dial Transplant. 1998;13:2322–2326
14. Parameshwar J, Schofield P, Large S. Long-term complications of car-diac transplantation.Br Heart J. 1995;74:341–342
15. Myers BD, Newton L. Cyclosporine-induced chronic nephropathy: an obliterative microvascular renal injury.J Am Soc Nephrol. 1991;2(suppl 1):S45–S52
16. Goldstein DJ, Zuech N, Sehgal V, Weinberg AD, Drusin R, Cohen D. Cyclosporin-associated end-stage nephropathy after cardiac transplantation: incidence and progression. Transplantation. 1997;63: 664 – 668
17. Myers BD, Ross J, Newton L, Luetscher J, Perloth M. Cyclosporin associated chronic nephropathy.N Engl J Med. 1984;311:699 –705 18. Ruggenenti P, Perico N, Amuchastegui CS, Ferrazzi P, Mamprin F,
Remuzzi G. Following an initial decline, glomerular filtration rate sta-bilizes in heart transplant patients on chronic cyclosporin.Am J Kidney Dis. 194;24:549 –553
19. Hartmann A, Andereassen AK, Holdaas H, Simonsen S, Geiran O, Berg KJ. Five years’ follow-up of renal glomerular and tubular functions in heart transplant recipients.J Heart Lung Transplant. 1996;15:972–979 20. Brenner BM. Nephron adaptation to renal injury or ablation.Am J
Physiol. 1985;249:F324 –F337
THE ACQUISITIVE SPIRIT
The consumption ethic may have started in the 1900s, but the desire is ancient. Kings and princes once thought they could solve problems by amassing things; we now join them.
Twitchell JB.Adcult USA.New York, NY: Columbia University Press; 1996
DOI: 10.1542/peds.107.6.1346
2001;107;1346
Pediatrics
H. Dark and John J. O'Sullivan
Tim S. Hornung, Christian G.E.L. de Goede, Chris O'Brien, Nadeem E. Moghal, John
Cyclosporin Dosage
Renal Function After Pediatric Cardiac Transplantation: The Effect of Early
Services
Updated Information &
http://pediatrics.aappublications.org/content/107/6/1346
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/107/6/1346#BIBL
This article cites 19 articles, 4 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/urology_sub Urology
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.107.6.1346
2001;107;1346
Pediatrics
H. Dark and John J. O'Sullivan
Tim S. Hornung, Christian G.E.L. de Goede, Chris O'Brien, Nadeem E. Moghal, John
Cyclosporin Dosage
Renal Function After Pediatric Cardiac Transplantation: The Effect of Early
http://pediatrics.aappublications.org/content/107/6/1346
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.