Cite as: Can Urol Assoc J 2015;9(1-2):E5-9. http://dx.doi.org/10.5489/cuaj.2113 Published online January 12, 2015.
Abstract
Introduction: There are several studies on the relationship between increased mean platelet volume (MPV) and varicocele. �e inves��e inves� tigated the relationship between preoperative and 6�month post� operative MPV values in patients whose varicocele was corrected with surgery.
Methods: A total of 282 patients underwent surgery at our urology clinic between December 2011 and December 2013 for primary varicocele. �e retrospectively examined the records of 61 patients who came to the 6�month postoperative follow�up. The preop� erative varicocele diagnosis was made with physical examination findings and supported with colour Doppler ultrasonography. Results: The varicocele was grade I in 12 patients, grade II in 34 patients and grade III in 11 patients. �hen the preoperative and 6�month postoperative haemoglobin (Hb), MPV, mean corpuscular volume, platelet, and platelet distribution width (PD�) values were compared, there was a significant decrease in MPV (p = 0.019), and a significant increase in Hb (p < 0.001). A noticeable increase was also present in PD�, but it was not statistically significant (p = 0.058).
Conclusion: �e found that MPV increased in patients with varic� ocele and tended to decrease again after the varicocele was sur� gically corrected. However, we feel larger prospective series are needed.
Introduction
Varicocele is defined as the dilatation of the pampiniform plexus of veins surrounding the testis.1 Clinical varicoceles
are present in about 15% of the general male population, and in up to 35% of men with primary infertility and 75% of men with secondary infertility.2 Varicoceles that are diag�
nosed primarily via physical examination are referred to as clinical varicoceles, whereas those that are <3 mm in diam�
eter and observed only via colour Doppler ultrasonography (CDU) with the Valsalva maneuver are considered subclini� cal varicoceles.3 Varicoceles are associated with other vas�
cular pathologies.4 Kılıç and colleagues also reported that
peripheral varicose veins share a pathological mechanism with varicocele.5
Mean platelet volume (MPV) is a parameter provided by the automatic blood count device during a routine blood count, but clinicians do not usually pay it much attention. It has been associated with thrombocyte volume, function, and activation.6 MPV and platelet distribution width (PD�)
are markers of platelet activation.7�9 It is generally accepted
that thrombocyte volume is determined during the produc� tion of thrombocytes from megakaryocytes.10 It is believed
that large thrombocytes are younger11 and less reactive.12
Increased MPV is associated with the presence and progno� sis of vascular disease, including peripheral, cerebrovascular, and coronary artery disease.13
Although there are studies on the relationship between MPV and vascular diseases, only a few investigate the rela� tionship between MPV and varicocele. Coban and colleagues found that MPV values were higher in varicocele group than in the control group.14 Therefore, we designed this study
to compare preoperative and postoperative MPV values in varicocele patients. �e investigated the relationship between preoperative and 6�month postoperative MPV values in patients whose varicocele was corrected with surgery.
Methods
Of the 282 patients who underwent surgery at our Şevket Yılmaz Training and Research Hospital’s Department of Urology between December 2011 and December 2013 due to primary varicocele, we retrospectively investigat� ed the records of 61 patients at their 6�month follow�up. All patients underwent varicocelectomy with a standard inguinal approach. This study was approved by our insti�
Soner Coban, MD;
*Ibrahim Keles, MD;
†İ
smail Biyik, MD;
§Muhammet Guzelsoy, MD;
*Ali Rıza Turkoglu, MD;
*Nihal Ocak, MD
¥*Department of Urology, Şevket Yılmaz Training and Research Hospital, Bursa, Turkey; †Department of Urology, School of Medicine, Afyon Kocatepe University, Afyonkarahisar, Turkey; §Department of Obstetrics and Gynecology, Karacabey State Hospital, Bursa, Turkey; ¥Department of Biochemistry, Şevket Yılmaz Training and Research Hospital, Bursa, Turkey.
tutional review board. Only 1 patient had bilateral varic� ocele, while the others had a unilateral left varicocele. The indication for surgery was infertility (primary in 38 patients, secondary in 16 patients) in 54 patients and other factors (pain, cosmetic reasons, etc.) in 3 patients. �e obtained the following information from patients: medical history, physi� cal examination, CDU, platelet, MPV, PD�, hemoglobin, white blood cell (�BC), and mean corpuscular volume (MCV) values. The preoperative varicocele diagnosis was made by physical examination and supported with CDU. Varicocele was grouped as mild (grade I: varicose veins are palpable only during the Valsalva maneuver), moderate (grade II: varicose veins may be palpable during rest but not visible), or severe (grade III: visible varicose veins).
Cases with non�varicocele scrotal pathologies (e.g., unde� scended testis, testicular torsion, epididymitis, orchitis, epi� dimo�orchitis, inguinal hernia, testicular mass) or systemic disease (e.g., hematological disorder, hypertension, diabetes mellitus, chronic renal failure, collagen vascular disease) were excluded from the study.
The full blood count test was performed with an automat� ic blood count test device (Abbott Cell�Dyn 3700 hematol� ogy analyzer) using blood with K�EDTA (Potassium�ethylene diamine tetraacetic acid) anticoagulation at our hospital. �e compared the preoperative and 6�month postoperative hemogram results.
Statistical tests were performed using software for �indows. Compliance of variables with a normal distribu�Compliance of variables with a normal distribu� tion was analyzed with visual (histogram and probability plots) and analytical methods (the Kolmogorov�Smirnov test). Descriptive analyses were provided as mean and standard deviation. Since the MPV and hemoglobin values showed normal distribution, the paired�t test was used in the preop� erative and postoperative comparison of these parameters, while the �ilcoxon test was used for the other parameters that did not comply with the normal distribution. Statistical significance was set at p < 0.05.
Results
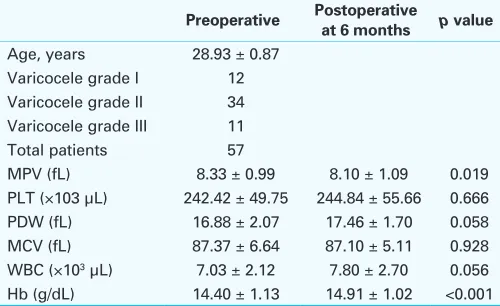
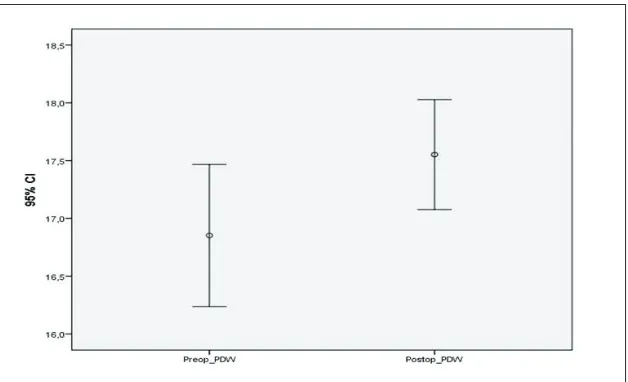
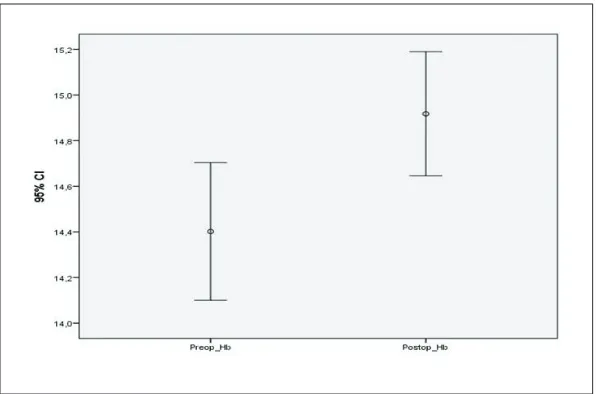
The mean age of the patients was 28.93 ± 0.87 (range: 16�45) (Table 1). The varicocele was grade I in 12 patients, grade II in 34 patients and grade III in 11 patients, while the bilateral case was grade III on the left and grade I on the right. �e excluded 4 patients with recurrence on CDU postoperative� postoperative� ly. �hen the preoperative and 6�month postoperative hemo�. �hen the preoperative and 6�month postoperative hemo� globin, MPV, MCV, platelet, and PD� values were com� pared, there was a significant decrease in MPV (p = 0.019), and a significant increase in hemoglobin (p < 0.001). A noticeable increase was also present in PD�, but it was not statistically significant (p = 0.058). Preoperatively and postoperatively mean MPV, PD�, and hemoglobin values are illustrated (Fig. 1, Fig. 2, Fig. 3).
Discussion
A varicocele is the most common correctable cause of male infertility and is defined as the abnormal dilatation of the veins creating the pampiniform plexus due to venous reflux. The usual etiological factors include hydrostatic pressure increase in the venous structures and venous reflux develop� ment due to anatomical features. The most important fac� tors that can cause such a hydrostatic pressure increase is the compression of the left renal vein between the superior mesenteric artery and the aorta (nutcracker phenomenon), inadequate gonadal vein valves, and direct opening of the left testicular vein to the left renal vein.15
Although it is not known how a varicocele creates dam� age in the testis, there are many theories. The two common accepted theories in varicocele pathophysiology are testicu� lar temperature increase and reflux of adrenal metabolits. Consequently varicocele can cause infertility via testicular damage, decrease of testicular volume, decrease of leydig cell functions, and impairment of spermatogenesis.16
A varicocele is a vascular problem. The cause is not definitely known although there are many theories on the physiopathogenesis. Vascular pathologies are associated with increased thrombocyte activity and increased throm� bocyte volume. The increased thromboxan, serotonin,
β�thromboglobulin, P�selectin, glycoprotein IIIa secretion and the decreased prostacyclin secretion from these activat� ed thrombocytes facilitate vasoconstriction and thrombocyte aggregation, leading to a high thrombotic potential.17�19 The
changes in the thrombocyte volume indicators can therefore have prophylactic and diagnostic value in thrombotic and prethrombotic events.19
Elevated MPV values have been shown in atherothrombotic disorders, such as acute myocardial ischemia, acute myocar� dial infarction, coronary atherosclerosis, and cerebrovascu�
Table 1. Demographic and clinical characteristics of the patients
Preoperative Postoperative at 6 months p value
Age, years 28.93 ± 0.87
Varicocele grade I 12
lar events. An increase in MPV has also been reported in conditions closely associated with insulin resistance, such as metabolic syndrome, obesity, diabetes mellitus, and hyperten� sion.9 Çoban and colleagues found significantly higher MPV
in obese patients with a body mass index of ≥30 kg/m2 than
in non�obese patients.20 They also reported that weight loss in
obese people led to a significant decrease in MPV; this in turn decreased cardiovascular disease risk by an antiatherogenic effect and by suppressing thrombocyte activation.21 Kario and
colleagues similarly found the thrombocyte count and MPV much higher in smoking patients and those with atheroscle� rotic lesions than in non�smoking patients and those with no atherosclerotic lesions and suggested that increased MPV accelerated atherosclerosis development. They also noticed a 10% decrease in MPV 1 to 3 months after quitting smoking in the atherosclerotic group.22
There are only a few studies investigating the relation� ship between MPV and varicocele. Bozkurt and colleagues reported the MPV values in a varicocele group were signifi� cantly higher than in the control group; their study included 60 patients with varicocele and 57 control group patients. They also found a significant correlation between MPV and varicocele grade and left spermatic vein diameter.23 �e simi�
larly evaluated the relationship between MPV and varic� ocele in 264 varicocele patients and 220 control subjects in another study and found MPV high in the patient group. However, we did not find a positive correlation between varicocele grade and left spermatic vein diameter.14 In the
current continuation study, we investigated the relationship between preoperative and 6�month postoperative MPV val� ues in patients whose varicoceles had been corrected with surgery. �hile a significant decrease was found in MPV
Fig. 1. The mean platelet volume (MPV) preoperative and 6-month postoperative values.
in the postoperative period, a noticeable rise was seen in PD�. However, we did not find a statistical significance. Studies evaluating the relationship between MPV and chron� ic inflammatory disease have shown high MPV values in patients with rheumatoid arthritis in the active period of the disease with high inflammatory marker levels.24 Similarly,
MPV values decreased after treatment of active disease in patients with ankylosing spondylitis.25
Furthermore, higher MPV values were shown in patients with severe obstructive sleep apnea leading to cardiovas� cular complications compared to a control group in a study with 95 subjects.26 A significant decrease was found in MPV
after continuous positive airway pressure (CPAP) treatment for 6 months in a similar group of patients.27
�e found lower hemoglobin levels in the varicocele group compared to controls. Some studies have reported lower testosterone levels in varicocele patients.28 Ferrucci
and colleagues reported that men in the lowest quartile of total and bioavailable testosterone were more likely to have anemia.29 Although we did not study serum testosterone lev�
els in this study, the lower hemoglobin in the varicocele group could be associated with low testosterone levels.
Conclusion
MPV is widely used to measure platelets. It increases in patients with varicocele and tends to decrease again in patients whose varicocele is corrected with surgery. Although we found that varicocele surgery corrected preoperatively increased MPV levels in this study, further larger series are need to support to this finding.
Competing interests: Authors declare no competing financial or personal interests.
This paper has been peer-reviewed.
References
1. Jarow JP, Espeland MA, Lipshultz LI. Evaluation of the azoospermic patient. J Urol 1989;142:62-5. 2. Goldstein M. Surgical management of male infertility. In: PCBs: Campbell-Walsh Urology. 10th edition.
Wein A, Kavoussi LR, Novick AC, Partin AW, Peters CA, editors. Philadelphia, PA: Elsevier Saunders; 2012:648-87. http://dx.doi.org/10.1016/B978-1-4160-6911-9.00022-0
3. Inci K, Gunay LM. The role of varicocele treatment in the management of non-obstructive azoospermia. Clinics 2013;68:89-98. http://dx.doi.org/10.6061/clinics/2013(Sup01)10
4. Yetkin E, Kilic S, Acikgoz N, et al. Increased prevalence of varicocele in patients with coronary artery ectasia. Coron Artery Dis 2005;16:261-4. http://dx.doi.org/10.1097/00019501-200508000-00001 5. Kilic S, Aksoy Y, Sincer I, et al. Cardiovascular evaluation of young patients with varicocele. Fertil Steril
2007;88:369-73. http://dx.doi.org/10.1016/j.fertnstert.2006.11.119
6. Bath PM, Butterworth RJ. Platelet size: Measurement, physiology and vascular disease. Blood Coagul Fibrinolysis 1996;7:157-61. http://dx.doi.org/10.1097/00001721-199603000-00011 7. Jagroop IA, Clatworthy I, Lewin J, et al. Shape change in human platelets: Measurement with a
channelyzer and visualisation by electron microscopy. Platelets 2000;11:28-32. http://dx.doi. org/10.1080/09537100075760
8. Park Y, Schoene N, Harris W. Mean platelet volume as an indicator of platelet activation: Methodological issues. Platelets 2002;13:301-6. http://dx.doi.org/10.1080/095371002220148332 9. Gasparyan AY, Ayvazyan L, Mikhailidis DP, et al. Mean platelet volume: A link between thrombosis and
inflammation? Curr Pharm Des 2011;17:47-58. http://dx.doi.org/10.2174/138161211795049804 10. Martin J. The relationship between megakaryocyte ploidy and platelet volume. Blood Cells
1989;15:108-17.
11. Chatterji AK, Lynch EC, Garg SK, et al. Circulating large platelets. N Engl J Med 1971;284:1440-1. http://dx.doi.org/10.1056/NEJM197106242842517
12. Van der Loo B, Martin JF. Megakaryocytes and platelets in vascular disease. Baillieres Clin Haematol 1997;10:109-23. http://dx.doi.org/10.1016/S0950-3536(97)80053-4
13. Vizioli L, Muscari S, Muscari A. The relationship of mean platelet volume with the risk and prognosis of cardiovascular diseases. Int J Clin Pract 2009;63:1509-15. http://dx.doi.org/10.1111/j.1742-1241.2009.02070.x
14. Coban S, Keleş I, Bıyık I, et al. Is there any relationship between mean platelet volume and varicocele? Andrologia Jan 6. 2014. http://dx.doi.org/10.1111/and.12220
15. Kendirci M, Miroğlu C. Erkek Reprodüktif Sistem Hastalıkları ve Tedavisi. Varikosel Patofizyolojisi, ed. Türk Androloji Derneği Yayınları, İstanbul; 2004:427-46.
16. World Health Organization. The influence of varicocele on parameters of fertility in a large group of men presenting to infertility clinics. Fertil Steril 1992;57:1289-93.
18. Mathur A, Robinson MS, Cotton J, et al. Platelet reactivity in acute coronary syndromes. Evidence for differences in platelet behaviour between unstble angina and myocardial infarction. Thromb Haemost 2001;85:989-94.
19. Martin JF, Bath PM, Burr ML. Influence of platelet size on out-come after myocardial infarction. Lancet 1991;338:1409-11. http://dx.doi.org/10.1016/0140-6736(91)92719-I
20. Çoban E, Özdoğan M, Yazıcıoğlu G, et al. The mean platelet volume in patients with obesity. Int J Clin Prac 2005;59:981-2. http://dx.doi.org/10.1111/j.1742-1241.2005.00500.x
21. Çoban E, Yılmaz A, Sarı R. The effect of weight loss on the mean platelet volume in obese patients. Platelets 2007;18:212-6. http://dx.doi.org/10.1080/09537100600975362
22. Kario K, Matsuo T, Nakao K. Cigarette smoking increases the mean platelet volume in elderly patients with risk factors for atherosclerosis. Clin Lab Haematol 1992;14:281-7. http://dx.doi. org/10.1111/j.1365-2257.1992.tb00103.x
23. Bozkurt Y, Soylemez H, Sancaktutar AA, et al. Relationship between mean platelet volume and varicocele: A preliminary study. Urology 2012;79:1048-51. http://dx.doi.org/10.1016/j.urology.2012.01.019 24. Milovanovic M, Nilsson E, Järemo P. Relationships between platelets and inflammatory markers in rheu-matoid arthritis. Clin Chim Acta 2010;343:237-40. http://dx.doi.org/10.1016/j.cccn.2003.12.030
25. Yazici S, Yazici M, Erer B, et al. The platelet functions in patients with ankylosing spondylitis: anti-TNF-alpha therapy decreases the mean platelet volume and platelet mass. Platelets 2010;21:126-31. http:// dx.doi.org/10.3109/09537100903470306
26. Varol E, Ozturk O, Gonca T, et al. Mean platelet volume is increased in patients with severe obstructive sleep apnea. Scand J Clin Lab Invest 2010;70:497-502. http://dx.doi.org/10.3109/00365513.2 010.520733
27. Varol E, Ozturk O, Yucel H, et al. The effects of continuous positive airway pressure therapy on mean platelet volume in patients with obstructive sleep apnea. Platelets 2011;22:552-6. http://dx.doi.org/ 10.3109/09537104.2011.578182
28. Tanrikut C, Goldstein M, Rosoff JS, et al. Varicocele as a risk factor for androgen deficiency and effect of repair. BJU Int 2011;108:1480-4. http://dx.doi.org/10.1111/j.1464-410X.2010.10030.x 29. Ferrucci L, Maggio M, Bandinelli S, et al. Low testosterone levels and the risk of anemia in older men
and women. Arch Intern Med 2006;166:1380-8. http://dx.doi.org/10.1001/archinte.166.13.1380