The Role of Arbitrarily Primed PCR in Identifying the Source
of an Outbreak of Legionnaires’ Disease
CYNTHIA G. WHITNEY,
1JO HOFMANN,
1‡ JANET M. PRUCKLER,
1ROBERT F. BENSON,
1BARRY S. FIELDS,
1UTPALA BANDYOPADHYAY,
2EDWARD F. DONNALLY,
2CHRISTINA GIORGIO-ALMONTE,
3§ LEONARD A. MERMEL,
3SARA BOLAND,
1\
BELA T. MATYAS,
2#
ANDROBERT F. BREIMAN
1*
Childhood and Respiratory Diseases Branch, Division of Bacterial and Mycotic Diseases, National Center for
Infectious Diseases, Centers for Disease Control and Prevention, Atlanta, Georgia,
1and Disease Control,
Rhode Island Department of Health,
2and Rhode Island Hospital and Brown University School of Medicine,
3Providence, Rhode Island
Received 8 January 1997/Returned for modification 7 March 1997/Accepted 16 April 1997
An outbreak of community-acquired Legionnaires’ disease (LD) occurred in Providence, R.I., in fall 1993. To
find the outbreak source, exposures of 17 case patients were compared to those of 33 matched controls. Case
patients were more likely than controls to have visited a section of downtown (area A) during the 2 weeks before
illness (11 [65%] versus 9 [27%]; matched odds ratio, 6.5; P
5
0.01). Water samples were cultured from 27
aerosol-producing devices within area A. Legionella pneumophila serogroup 1 isolates underwent monoclonal
antibody (MAb) subtyping and arbitrarily primed PCR (AP-PCR). All four L. pneumophila serogroup 1 isolates
available from case patients who visited area A had identical MAb and AP-PCR patterns. Among 14
environ-mental isolates, 5 had MAb patterns that matched the case patient isolates, but only 1 had a matching AP-PCR
pattern. This investigation implicates a cooling tower in area A as the outbreak source and illustrates the
usefulness of AP-PCR for identifying sources of LD outbreaks.
Although over 40 species of Legionella have been identified
(3a, 31), most cases of Legionnaires’ disease and most
out-breaks of Legionnaires’ disease are due to Legionella
pneumo-phila serogroup 1 (24). Since L. pneumopneumo-phila serogroup 1 may
be isolated in up to 50% of building water supplies and cooling
towers (17), molecular epidemiologic testing is often a critical
component of outbreak investigations, particularly when an
epidemiologic investigation has identified more than one
po-tential source of transmission.
Monoclonal antibody (MAb) subtyping has been extremely
useful for targeting and confirming outbreak sources. For
out-break investigations in which transmission may be ongoing and
public health decisions must be made rapidly, crucial criteria
for a useful molecular epidemiologic test include its ability to
reliably discriminate among isolates of the same species and
serogroup as well as its speed and simplicity.
We applied a new technique, arbitrarily primed PCR
(AP-PCR), during a communitywide outbreak of Legionnaires’
dis-ease in Providence, R.I. AP-PCR, a relatively rapid, simple,
and inexpensive test, discriminated environmental isolates with
like MAb subtyping patterns and played a key role in
identi-fying the source of the outbreak.
The outbreak.
Between 12 August and 30 September 1993,
nine cases of Legionnaires’ disease were reported among
Rhode Island residents; two persons died. The Rhode Island
Department of Health (RIDH) received the reports from four
Providence hospitals; all patients had onset of symptoms prior
to their hospital admission. In the previous year, only one
unconfirmed case had been reported to the RIDH during a
similar time period. No common exposures among case
pa-tients were initially apparent, although many of those ill lived
or worked in downtown Providence. The RIDH and the
Cen-ters for Disease Control and Prevention (CDC) began an
in-vestigation to identify the source of the outbreak and
imple-ment an intervention strategy.
(The results of this investigation were presented in part at
the 34th Interscience Conference on Antimicrobial Agents and
Chemotherapy, October 1994, Orlando, Fla. [35a], and in
ref-erence 8a.)
MATERIALS AND METHODS
We defined a case as community-acquired pneumonia with onset after 1 August 1993 and laboratory confirmation of Legionnaires’ disease. Laboratory confirmation included isolation of Legionella from respiratory secretions by hos-pital microbiology laboratories (7, 12), detection of L. pneumophila serogroup 1 antigens in urine by radioimmunoassay (RIA) (performed at Miriam Hospital in Providence or by a reference laboratory) (2, 21), or demonstration of a fourfold rise in reciprocal titer of antibodies to L. pneumophila serogroup 1 (to$128) by indirect immunofluorescent antibody assay (performed at CDC or a reference laboratory) (7). Patients were excluded if they had not been in Providence or the adjacent suburbs in the 2 weeks before the onset of symptoms, an interval approximating the incubation period for Legionnaires’ disease.
We notified laboratory directors and hospital infection control practitioners at 17 hospitals serving the Providence area and adjacent areas of Massachusetts that an outbreak of Legionnaires’ disease was occurring. Infection control prac-titioners were then contacted twice weekly during the investigation to identify new cases. The RIDH also sent letters providing information on the outbreak and diagnostic testing for Legionnaires’ disease to all primary care physicians and to all emergency room and urgent care directors in Rhode Island and adjacent areas of Massachusetts reminding them to report all patients with Legionnaires’ disease.
We conducted a matched case control study to identify exposures associated with Legionnaires’ disease. Controls were matched for sex, age within 10 years, and the presence of other specific known risk factors for Legionnaires’ disease, including cigarette smoking, renal failure requiring dialysis, alcohol abuse, dia-betes mellitus, immunosuppressive therapy, organ transplantation, congestive heart failure, or lung disease. Patients with more than one risk factor were
* Corresponding author. Mailing address: CDC Mailstop C-23, 1600
Clifton Road NE, Atlanta, GA 30333. Phone: (404) 639-2215. Fax:
(404) 639-3970.
‡ Present address: Philadelphia Department of Public Health,
Phil-adelphia, PA 19146.
§ Present address: Cranston, RI 02905.
\
Present address: U.S. Naval Hospital, FPOAE 09619-0700.
# Present address: Division of Epidemiology and Immunizations,
State Laboratory Institute, Jamaica Plain, MA 02130.
1800
on May 15, 2020 by guest
http://jcm.asm.org/
matched on the condition placing them at highest risk for illness (immunosup-pressive therapy.diabetes mellitus or renal failure.heart or lung disease.
smoking or alcohol abuse). Controls were selected from among those persons attending the same clinic or doctor’s office as the case patient. If the case patient did not have a primary physician, controls were selected from the outpatient clinic that the patient was scheduled to attend following discharge. Two controls were selected for 16 of 17 case patients; only one suitable control could be found for the remaining patient.
We interviewed case patients and controls in person using a standardized questionnaire which addressed activities and exposures (identified by open-ended interviews of 10 case patients earlier in the investigation) during the 2 weeks before the case patient’s illness. Family members served as surrogates for deceased patients and patients requiring mechanical ventilation. An exposure for indoor sites such as businesses or restaurants was defined as entering the build-ing; for outdoor sites such as parks, plazas, or construction areas, an exposure was defined as walking through or next to the site. Participants who recalled driving through an area without stopping were considered unexposed for the analysis; those who could not recall whether they were exposed were excluded from the analysis for that variable.
Matched odds ratios (OR) and 95% confidence intervals (CI) were computed by exact methods (26) on Epi-Info software (10).
Aerosol-producing devices in and near a part of town frequented by most case patients were identified by visual survey from the tallest buildings in downtown Providence and by door-to-door questioning of building managers in the area. Between 8 and 28 October, we collected three 250-ml water samples from each of 24 cooling towers and three outdoor decorative fountains in downtown Prov-idence; there were no functioning outdoor drinking fountains identified in the downtown area that we investigated. During 22 October to 8 November, we collected 1-liter potable water samples and swabs from water heaters, showers, and kitchen sink faucets in the homes of six of the seven case patients from whom
Legionella was isolated (one patient was homeless) and from an apartment
building where two other case patients lived (3). Water samples were concen-trated by filtration, treated with acid, or cultured directly according to CDC protocols (8). Plates were examined for bacterial colonies typical of legionellae at 4 and 7 days. Four colonies from each positive sample were selected for identification and subtyping.
Isolates from case patients and water samples were subtyped during the in-vestigation at the CDC with a panel of MAbs to L. pneumophila serogroup 1 (19) by dot immunoblot (32) and by AP-PCR (15, 30). AP-PCRs were performed with 1mM primer (M13 Forward, 21 bp; 59TTA TGT AAA ACG ACG GCC AGT 39), 5ml of boiled cell lysate, and 0.25 U of Taq DNA polymerase (Perkin-Elmer Cetus). Amplification was performed in a DNA thermal cycler (Perkin-Elmer Cetus) programmed for 45 cycles of 1 min at 94°C, 1 min at 36°C, and 2 min at 72°C. Results were confirmed in a blinded fashion by pulsed-field gel electro-phoresis (PFGE) at Rhode Island Hospital (30). For PFGE, restriction digestion of chromosomal DNA was performed with 20 U of SfiI (New England Biolabs, Inc., Beverly, Mass.).
Research was conducted in compliance with guidelines of the U.S. Depart-ment of Health and Human Services as they apply to epidemic investigations by the U.S. Public Health Service, CDC.
RESULTS
Case finding detected eight additional case patients, for a
total of 17. All patients were hospitalized, and two (12%) died.
Seven case patients required mechanical ventilation. All had
illness onset dates after 29 August 1993, and eight had an onset
during the week of 12 September 1993 (Fig. 1). Eleven (65%)
were men. Ages ranged from 28 to 86 years (median, 49 years).
Sixteen (94%) patients had at least one medical risk factor for
Legionnaires’ disease, such as smoking (n
5
12) or diabetes
mellitus (n
5
1). Four patients had a documented history of
alcohol abuse; no other patients had medical conditions that
are known risk factors for aspiration. The diagnosis of
Legion-naires’ disease was made for three patients by isolation of
Legionella from respiratory secretions, for 10 patients by
de-tection of L. pneumophila serogroup 1 antigens in urine by
RIA, and for four case patients by both isolation of the
organ-ism and detection of L. pneumophila serogroup 1 antigens in
urine. Acute- and convalescent-phase sera were available for
three case patients, all of whom had greater than fourfold rises
in antibody titers.
Two case patients lived in the same apartment building,
building A, in downtown Providence; otherwise, no two
pa-tients lived or worked in the same building. No more than 4 of
17 case patients visited any single building in Providence,
sug-gesting that transmission for most case patients occurred
out-doors. Case patients were significantly more likely than
con-trols to report being in the northeast section of downtown
Providence (area A), a 0.75-square-km area including the
fi-nancial district (65 versus 27%; matched OR, 6.5; 95% CI, 1.5
to 45.2; P
5
0.01) (Table 1). Exposure to Kennedy Plaza,
within area A, was also associated with disease (matched OR,
5.9; 95% CI, 1.3 to 45.2; P
5
0.02). Case patients were no more
likely than controls to visit other sections of the Providence
area.
All seven patient isolates were L. pneumophila serogroup 1.
Four of these isolates were identical by MAb subtyping
(pat-tern 1, 2, 5, 6) and by AP-PCR (pat(pat-tern A) (Table 2). The four
case patients infected with strains with this pattern all reported
exposures to area A in the 2 weeks before the onset of illness.
All four had onset of symptoms during the week of 12 August.
The other three patient isolates, from case patients who did
not recall any exposure to area A during the 2 weeks before
their illness, differed by either MAb subtype or AP-PCR
pat-tern.
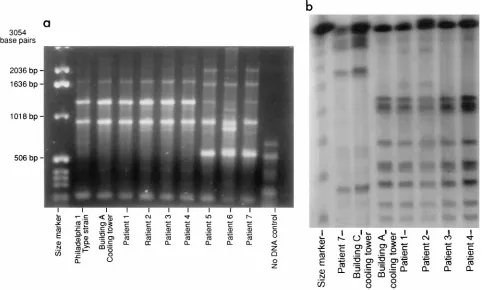
[image:2.612.319.555.70.228.2]Samples from 9 (37.5%) of 24 cooling towers and one
(33.3%) decorative fountain grew legionellae on culture (Fig.
2); all isolates were L. pneumophila serogroup 1. Four (28.6%)
of 14 isolates from environmental sources were MAb subtype
1, 2, 5, 6, matching the four identical patient strains (Table 2).
However, only one cooling tower isolate, obtained from a
building in area A (building A), was identical by AP-PCR and
MAb subtyping to the four identical case patient isolates (Fig.
3a). All samples from case patient homes were culture
nega-tive. PFGE results mirrored the AP-PCR findings in regard to
similarity between clinical specimens and the cooling tower at
building A (Table 2; Fig. 3b).
FIG. 1. Number of cases by week of onset (month/day).
TABLE 1. Summary of case control study results
Exposure No. of casesexposed/ totala(%)
No. of controls exposed/ totala(%)
Matched OR (95% CI)b
Downtown 11/17 (64.7) 15/32 (46.9) 2.7 (0.7–13.7)
Area A 11/17 (64.7) 9/33 (27.3) 6.5 (1.5–45.2)
Kennedy Plaza 8/17 (47.1) 5/32 (15.6) 5.9 (1.3–42.1) Suburban shopping center 0/16 (0) 9/32 (28.1) 0.0 (0–0.6)
aDenominators vary because of exclusion of those unable to recall their
exposure to a site.
bMatched OR and 95% CI were computed by exact methods (4).
on May 15, 2020 by guest
http://jcm.asm.org/
[image:2.612.317.557.620.702.2]Visiting any location within 200 m of the source tower at
building A was associated with disease (matched OR, 6.3; CI,
1.4 to 44.8; P
5
0.02). All four case patients with isolates
matching the source isolate recalled visiting the area within
200 m of the tower in the 2 weeks before the onset of illness
(OR
`
versus their matched controls; mid-P exact confidence
limits, 1.4 to
`; P
5
0.03). These four case patients were also
more likely to have taken walks in downtown Providence than
were their matched controls (matched OR
`; mid-P exact
confidence limits, 1.2 to
`; P
5
0.04). Patient 4 lived out of
state but visited downtown Providence one afternoon 3 days
before the onset of symptoms; that afternoon he worked on the
rooftop of a building adjacent to building A. He denied other
exposures within downtown Providence during the 2 weeks
before his illness began.
In response to these results, building A management
ar-ranged for cleaning of the cooling tower in accordance with
guidelines published by the Wisconsin Department of Health
and Human Services (37) and is monitoring the cooling tower
for recurring colonization with legionellae. No further cases of
Legionnaires’ disease with exposure to area A have been
iden-tified on continued surveillance.
DISCUSSION
The case control study targeted a section of downtown
Prov-idence (area A) as the source of the outbreak and indicated
where additional environmental studies were needed. The
study also found no specific building of residence or
employ-ment in common, suggesting that transmission occurred
out-doors. Among a variety of contaminated aerosol-producing
devices sampled, MAb subtyping narrowed the list of potential
outbreak sources but could not distinguish between isolates
from four separate devices. AP-PCR, a new method enabling
subtyping of strains in 8 h by a single laboratory technician,
helped pinpoint the source and was completed rapidly enough
to be of use in a public health intervention. PFGE would have
identified the outbreak strain as well and was better at
discrim-inating between nonoutbreak strains, as has been noted
previ-ously (30, 33, 35). PFGE, however, is more time-consuming (3
days generally required) than AP-PCR and may not be
ade-quate when a rapid response is needed for outbreak control.
Subtyping methods for Legionella are complementary, and
multiple tests may be necessary for some outbreak settings,
such as those involving common serogroups (e.g., L.
pneumo-phila serogroup 1).
The diagnosis of Legionnaires’ disease can be problematic.
Serologic testing is cumbersome and may be of little use
clin-ically because a single acute-phase titer has low positive
pre-dictive value (28, 29) and paired sera must be collected 3 to 6
weeks apart (36), too late for an impact on clinical
manage-ment. In this outbreak, however, all reported case patients
were diagnosed in a timely manner by isolation of the organism
from respiratory secretions or by RIA detection of L.
pneumo-phila serogroup 1 antigen in urine. The latter test, which is
[image:3.612.320.549.73.434.2]commercially available through a number of reference
labora-tories, can be completed in a few hours. Increasing physician
FIG. 2. Downtown Providence; dotted line encompasses area A. Lp1, L.
pneumophila serogroup 1.
TABLE 2. Results of MAb subtyping, AP-PCR, and PFGE for
L. pneumophila serogroup 1 isolates from patient and
environmental samples
Isolate source MAb subtype AP-PCRpattern patternPFGE
Patient 1
a1, 2, 5, 6
A
B
Patient 2
a1, 2, 5, 6
A
B
Patient 3
a1, 2, 5, 6
A
B
Patient 4
a1, 2, 5, 6
A
B
Patient 5
1, 2, 5, 6
B
C3
Patient 6
1, 2, 5, 6
C
G
Patient 7
1, 6
B
A
Building A CT
a,b1, 2, 5, 6
A
B
1, 6 (second isolate)
B
A
Building B CT
1, 2, 5, 6
B
A
1, 6 (second isolate)
B
C2
Building C CT
1, 6
B
A
Building D CT
1, 2, 5, 6
B
A
1, 6 (second isolate)
B
C
Building E CT
1, 2, 5, 6
B
A
1, 6 (second isolate)
B
C
Building F CT
1, 6
B
A
Building G CT
1, 6
B
A
Building H CT
1, 6
B
A
Building I CT
1, 6, 7
B
C4
Outdoor
fountain
1, 6
B
A
Philadelphia 1
type strain
c1, 2, 5, 6
A
F
aThese isolates are identical by MAb subtyping, AP-PCR, and PFGE. bCT, cooling tower.
cATCC 33152.
on May 15, 2020 by guest
http://jcm.asm.org/
[image:3.612.57.299.98.347.2]awareness and use of the urinary antigen RIA may assist in
patient management and in detecting outbreaks of
Legion-naires’ disease. Since diagnostic tests for LegionLegion-naires’ disease
are underutilized, Legionella may have caused many
pneumo-nias in Providence in addition to the 17 that were identified
and confirmed to be Legionnaires’ disease.
Some cases identified during active surveillance after initial
recognition of the outbreak were likely unrelated to the
out-break and may have occurred sporadically. Six (35%) case
patients did not recall being in the vicinity of building A and
had no other common exposures. Isolates available from
re-spiratory secretions from three of these persons were different
from each other and from the epidemic strain by PFGE,
sug-gesting that the patients were infected from different sources.
A recent prospective population-based study in Ohio
sug-gested that the incidence of sporadically occurring
Legion-naires’ disease is about 6/100,000 adult population per year
(25). Based on this rate, 60 cases of Legionnaires’ disease
would be expected among Rhode Island residents (1990
pop-ulation
5
1,003,464) per year, or approximately five cases per
month. It is likely that increased surveillance instituted during
this investigation optimized identification of sporadically
oc-curring (background) disease. The inclusion of sporadically
occurring cases in the case control study biased the results
toward the null, reducing the possibility for identifying a
sta-tistically significant association of disease with specific
expo-sure.
Transmission of Legionella organisms can occur following
inhalation of aerosolized water droplets containing the
bacte-rium. Aerosols from cooling towers and evaporative
condens-ers (5, 9, 11, 14, 20), decorative fountains (13), humidificondens-ers
(22), whirlpool baths (18, 23, 27, 34), and showers (6, 16) have
been shown to transmit disease in previous outbreaks.
Epide-miologic and laboratory data strongly suggest that outdoor
transmission of aerosols from a cooling tower in area A was the
source of this outbreak. Outdoor transmission of Legionella
from cooling towers has been noted in other outbreaks,
espe-cially within 200 m of the tower (17), and perhaps as far as 1 or
2 miles from the source (1). Area A includes sites as far as
500 m from the cooling tower on building A.
Although aspiration may be another mechanism for
Legio-nella transmission for patients with sporadic nosocomial
Le-gionnaires’ disease (4, 38), several factors exclude aspiration as
the primary mode of transmission for the case patients
iden-tified during this community outbreak. The shape of the
epi-demic curve (many cases over a brief period) indicates that the
outbreak is likely due to a point source. Patients did not,
however, report visiting a single building or institution where
coincident aspiration of potable water could have occurred.
Massive contamination of the city’s water supply with
Legio-nella would be required to produce such a community outbreak
from aspiration. None of the samples of potable water from
case patient homes tested (including building A) grew
Legio-nella on culture, making this consideration highly unlikely.
[image:4.612.67.553.73.363.2]The results of this investigation obtained through the use of
AP-PCR highlight the role of cooling tower aerosols in
trans-mitting Legionnaires’ disease. Legionellae were cultured from
37.5% of cooling towers in area A, a percentage similar to that
in previous reports (17), although only one cooling tower was
associated with this outbreak of Legionnaires’ disease. To
pre-vent further illness in Providence, health officials
recom-mended that all contaminated towers be cleaned according to
previously published guidelines (37) and that follow-up
cul-tures be performed on the implicated cooling tower. Effective
FIG. 3. AP-PCR analysis of patient isolates compared with isolate from cooling tower of building A (a) and PFGE analysis of matching patient and building A isolates and two comparison strains (b). Bacteriophage lambda concatemers (48.5 kb; New England Biolabs) were used as molecular size standards for PFGE.
on May 15, 2020 by guest
http://jcm.asm.org/
strategies are needed to minimize the potential of cooling
towers to transmit Legionnaires’ disease. Research should be
conducted to determine how often cooling towers transmit
Legionnaires’ disease (attributable risk) and to identify factors
that increase the attributable risk so that cost-effective
inter-ventions can be designed.
ACKNOWLEDGMENTS
We acknowledge the following people for their contributions to this
investigation: Marilyn Rittman, Linda D’Agostino, Richard Scott,
Marie Stoeckel, Cynthia Vanner, Edmond A. Arcand, Jr., and Barbara
A. DeBuono, RIDH; Harvey Lipman, CDC; and John Boyce, Charles
Carpenter, and Gail Potter-Bynoe, Miriam Hospital, Providence.
The RIDH and the CDC did not receive any outside funding for this
project.
REFERENCES
1. Addiss, D. G., J. P. Davis, M. LaVenture, P. J. Wand, M. A. Hutchinson, and
R. M. McKinney.1989. Community-acquired Legionnaires’ disease associ-ated with a cooling tower: evidence for longer-distance transport of
Legio-nella pneumophila. Am. J. Epidemiol. 130:557–568.
2. Aguero-Rosenfeld, M. E., and P. H. Edelstein. 1988. Retrospective evaluation of the DuPont radioimmunoassay kit for detection of Legionella pneumophila se-rogroup 1 antigenuria in humans. J. Clin. Microbiol. 26:1775–1778. 3. Barbaree, J. M., G. W. Gorman, W. T. Martin, B. S. Fields, and W. E.
Morrill.1987. Protocol for sampling environmental sites for legionellae. Appl. Environ. Microbiol. 53:1454–1458.
3a.Benson, R. F., W. L. Thacker, M. I. Daneshvar, and D. J. Brenner. 1996.
Legionella waltersii sp. nov. and an unnamed Legionella genomospecies
iso-lated from water in Australia. Int. J. Syst. Bacteriol. 46:631–634. 4. Blatt, S. P., M. D. Parkinson, E. Pace, P. Hoffman, D. Dolan, P. Lauderdale,
R. A. Zajac, and G. P. Melcher.1993. Nosocomial Legionnaires’ disease: aspiration as a primary mode of disease acquisition. Am. J. Med. 95:16–22. 5. Breiman, R. F., W. Cozen, B. S. Fields, T. D. Mastro, S. J. Carr, J. S. Spika,
and L. Mascola.1990. Role of air sampling in investigation of an outbreak of Legionnaires’ disease associated with exposure to aerosols from an evap-orative condenser. J. Infect. Dis. 161:1257–1261.
6. Breiman, R. F., B. S. Fields, J. S. Spika, G. N. Sanden, L. Volmer, A. Meier,
and J. S. Spika.1990. Association of shower use with Legionnaires’ disease: possible role of amoebae. JAMA 263:2924–2926.
7. Centers for Disease Control. 1987. Hospital-laboratory diagnosis of
Legio-nella infections. Centers for Disease Control, Atlanta, Ga.
8. Centers for Disease Control. 1992. Procedures for the recovery of Legionella from the environment. Centers for Disease Control, Atlanta, Ga. 8a.Centers for Disease Control and Prevention. 1994. Legionnaires’ disease
associated with cooling towers in Massachusetts, Michigan, and Rhode Is-land, 1993. Morbid. Mortal. Weekly Rep. 43:491–493, 499.
9. Cordes, L. G., D. W. Fraser, P. Skaliy, C. A. Perlino, W. R. Elsea, G. F.
Mallison, and P. S. Hayes.1980. Legionnaires’ disease outbreak at an At-lanta, Georgia, country club: evidence for spread from an evaporative con-denser. Am. J. Epidemiol. 111:425–431.
10. Dean, A. G., J. A. Dean, D. Coulombier, A. H. Burton, K. A. Brendel, D. C.
Smith, R. C. Dicker, D. M. Sullivan, and R. F. Fagan.1994. Epi Info, version 6: a word processing, database, and statistics program for epidemiology on microcomputers. Centers for Disease Control and Prevention, Atlanta, Ga. 11. Dondero, T. J., Jr., R. C. Rendtorff, G. F. Mallison, R. M. Weeks, J. S. Levy,
E. W. Wong, and W. Schaffner.1980. An outbreak of Legionnaires’ disease associated with a contaminated air-conditioning cooling tower. N. Engl. J. Med. 302:365–370.
12. Edelstein, P. H. 1993. Laboratory diagnosis of Legionnaires’ disease: an update from 1984, p. 7–11. In J. Barbaree, R. F. Breiman, and A. P. Dufour (ed.), Legionella: current status and emerging perspectives. American Soci-ety for Microbiology, Washington, D.C.
13. Fenstershieb, M. D., M. Miller, C. Diggins, S. Liska, L. Detwiler, S. B.
Werner, D. Lindquist, W. L. Thacker, and R. F. Benson.1990. Outbreak of Pontiac fever due to Legionella anisa. Lancet 2:35–37.
14. Garbe, P. L., B. J. Davis, J. S. Weisfeld, L. Markowitz, P. Miner, F. Garrity,
J. M. Barbaree, and A. L. Reingold.1985. Nosocomial Legionnaires’ disease: epidemiologic demonstration of cooling towers as a source. JAMA 254:521–524. 15. Gomez-Luz, P., B. S. Fields, R. F. Benson, W. T. Martin, S. P. O’Connor, and
C. M. Black.1993. Comparison of arbitrarily primed PCR, ribotyping and monoclonal antibody analysis for subtyping Legionella pneumophila sero-group 1. J. Clin. Microbiol. 31:1940–1942.
16. Hanrahan, J. P., D. L. Morse, V. B. Scharf, J. G. Debbie, G. P. Schmid, R. M.
McKinney, and M. Shayegani.1987. A community hospital outbreak of legio-nellosis: transmission by potable hot water. Am. J. Epidemiol. 125:639–649. 17. Hoge, C. W., and R. F. Breiman. 1991. Advances in the epidemiology and
control of Legionella infections. Epidemiol. Rev. 13:329–340.
18. Jernigan, D. B., J. Hofmann, M. S. Cetron, C. A. Genese, J. P. Nuorti, B. S.
Fields, R. F. Benson, R. J. Carter, P. H. Edelstein, I. C. Guerrero, S. M. Paul, H. B. Lipman, and R. Breiman.1996. Outbreak of Legionnaires’ disease among cruise ship passengers exposed to a contaminated whirlpool spa. Lancet 347:494–499.
19. Joly, J. R., R. M. McKinney, J. O. Tobin, W. F. Bibb, I. D. Watkins, and D.
Ramsay.1986. Development of a standardized subgrouping scheme for
Le-gionella pneumophila serogroup 1 using monoclonal antibodies. J. Clin.
Mi-crobiol. 23:768–771.
20. Keller, D. W., R. Hajjeh, A. Demaria, Jr., B. S. Fields, J. M. Pruckler, R. S.
Benson, P. E. Klutt, S. M. Lett, L. A. Mermel, C. Giorgio, and R. F. Breiman.
1996. Community outbreak of Legionnaires’ disease: an investigation con-firming the potential for cooling towers to transmit Legionella. Clin. Infect. Dis. 22:257–261.
21. Kohler, T. B., L. J. Wheat, M. L. V. French, P. L. Meenhorst, W. C. Winn,
and P. H. Edelstein.1985. Cross-reactive urinary antigens among patients infected with Legionella pneumophila serogroups 1 and 4 and the Leiden 1 strain. J. Infect. Dis. 152:1007–1012.
22. Mahoney, F. J., C. W. Hoge, T. A. Farley, J. M. Barbaree, and R. F. Breiman. 1992. Communitywide outbreak of Legionnaires’ disease associated with a grocery store mist machine. J. Infect. Dis. 165:736–739.
23. Mangione, E. J., R. S. Remis, K. A. Tait, H. B. McGee, G. W. German, B. B.
Wentworth, P. A. Baron, A. W. Hightower, J. M. Barbaree, and C. V. Broome.1985. An outbreak of Pontiac fever related to whirlpool use, Mich-igan 1982. JAMA 253:535–539.
24. Marston, B. J., H. B. Lipman, and R. F. Breiman. 1994. Surveillance for Legionnaires’ disease: risk factors for morbidity and mortality. Arch. Intern. Med. 154:2417–2422.
25. Marston, B. J., J. F. Plouffe, T. M. File, B. Hackman, S. J. Salstrom, H. B.
Lipman, and R. F. Breiman.Incidence of community-acquired pneumonia requiring hospitalization: population-based active surveillance in Ohio. Arch. Intern. Med., in press.
26. Martin, D., and H. Austin. 1991. An efficient program for computing con-ditional maximum likelihood estimates and exact confidence limits for a common odds ratio. Epidemiology 2:359–362.
27. Miller, L. A., J. L. Beebe, J. C. Butler, W. Martin, R. Benson, R. W. Hoffman,
and B. S. Fields.1993. Use of polymerase chain reaction in a epidemiologic investigation of Pontiac fever. J. Infect. Dis. 168:769–772.
28. Nichol, K. L., C. M. Parenti, and J. E. Johnson. 1991. High prevalence of positive antibodies to Legionella pneumophila among outpatients. Chest 100: 663–666.
29. Plouffe, J. F., T. M. File, Jr., R. F. Breiman, B. A. Hackman, S. J. Salstrom,
B. J. Marston, B. S. Fields, and the Community-Based Pneumonia Incidence Study Group.1995. Reevaluation of the definition of Legionnaires’ disease: use of the urinary antigen assay. Clin. Infect. Dis. 20:1286–1291. 30. Pruckler, J. M., L. A. Mermel, R. F. Benson, C. Giorgio, P. K. Cassiday, R. F.
Breiman, C. G. Whitney, and B. S. Fields.1995. Comparison of Legionella
pneumophila isolates by arbitrarily primed PCR and pulsed-field gel
electro-phoresis: analysis from seven epidemic investigations. J. Clin. Microbiol.
33:2872–2875.
31. Reingold, A. L., B. M. Thomason, B. J. Brake, L. Thacker, H. A. Wilkinson, and
J. N. Kuritsky.1984. Legionella pneumonia in the United States: the distribution of serogroups and species causing human illness. J. Infect. Dis. 149:819. 32. Sanden, G. N., P. K. Cassiday, and J. M. Barbaree. 1993. Rapid immunodot
technique for identifying Bordetella pertussis. J. Clin. Microbiol. 31:170–172. 33. Schoonmaker, D., T. Heimberger, and G. Birkhead. 1992. Comparison of ribotyping and restriction enzyme analysis using pulsed-field gel electro-phoresis for distinguishing Legionella pneumophila isolates obtained during a nosocomial outbreak. J. Clin. Microbiol. 20:1491–1498.
34. Spitalny, K. C., R. L. Vogt, L. A. Orciari, L. E. Witherell, P. Etkind, and L. F.
Novick.1984. Pontiac fever associated with a whirlpool spa. Am. J. Epide-miol. 120:809–817.
35. Van Belkum, A., M. Struelens, and W. Quint. 1993. Typing of Legionella
pneumophila strains by polymerase chain reaction-mediated DNA
finger-printing. J. Clin. Microbiol. 31:2198–2200.
35a.Whitney, C. G., J. Hofmann, J. Pruckler, B. Matyas, R. Benson, B. Fields, L.
Mermel, C. Giorgio, and R. Breiman.1994. A novel subtyping method to identify the source of an outbreak of Legionnaires’ disease, abstr. J192, p. 193.
In Abstracts of the 34th Interscience Conference on Antimicrobial Agents and
Chemotherapy. American Society for Microbiology, Washington, D.C. 36. Wilkinson, H. W., A. L. Reingold, B. J. Brake, D. L. McGiboney, G. W. Gorman,
and C. V. Broome.1983. Reactivity of serum from patients with suspected legionellosis against 29 antigens of legionellaceae and Legionella-like organisms by indirect immunofluorescence assay. J. Infect. Dis. 147:23–31.
37. Wise, M., D. Addiss, M. LaVenture, et al. 1987. Control of Legionella in cooling towers: summary guidelines. Wisconsin Department of Health and Social Services, Madison.
38. Yu, V. L. 1993. Could aspiration be the major mode of transmission for
Legionella? Am. J. Med. 95:13–15.